
Enhancing Skin Cancer Detection and Classification in Dermoscopic Images through Concatenated MobileNetV2 and Xception Models
 , and
, and 
Abstract
:1. Introduction
- Improved accuracy and robustness in skin cancer detection and classification
- Enhanced generalization capabilities, enabling accurate identification of skin cancer
- A comparative examination indicating the superiority of the suggested concatenated model over individual MobileNetV2 and Xception models, as well as other existing approaches
- Real-world application with a user-friendly interface for efficient and reliable skin cancer screening
2. Related Works
3. Materials and Methods
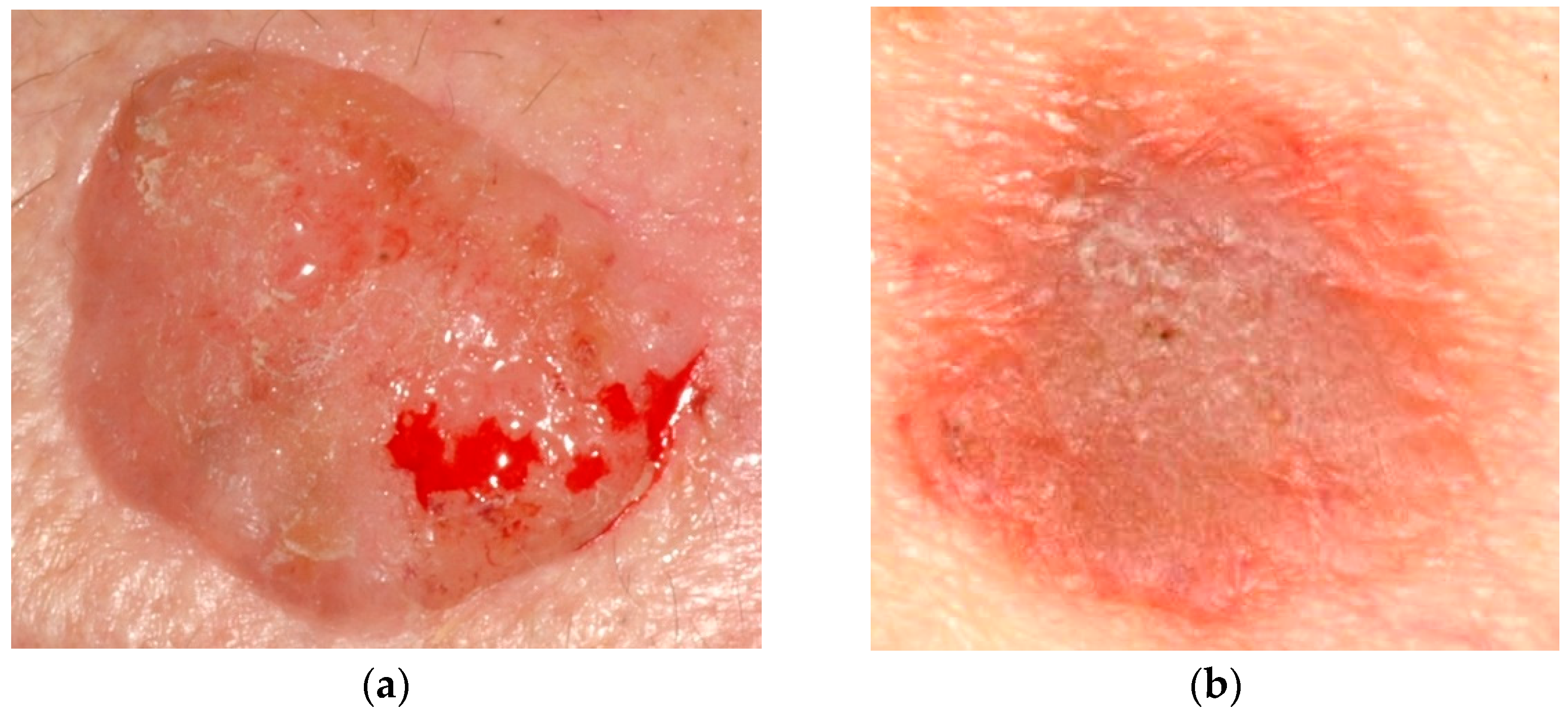
3.1. Dataset Description
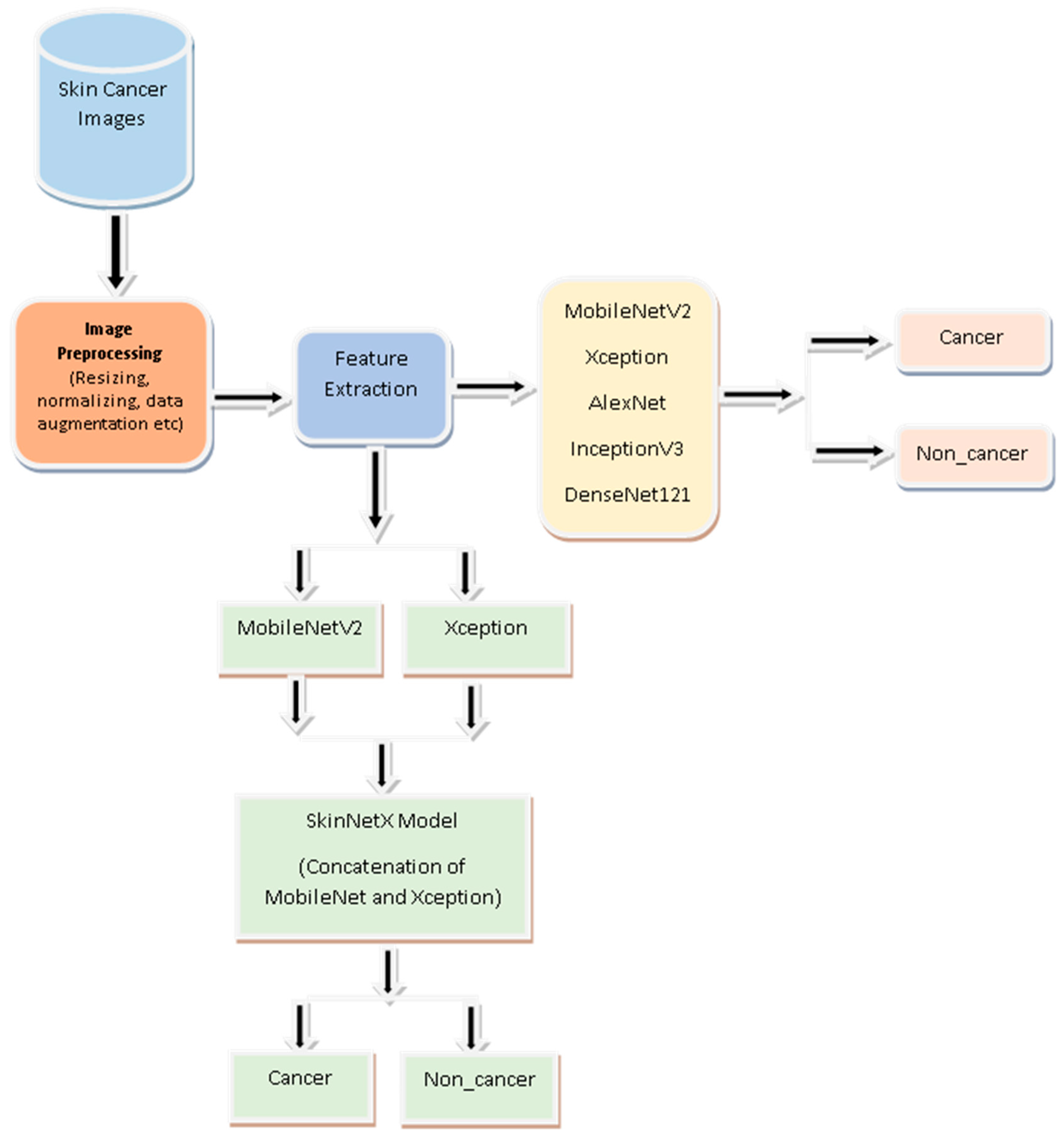
3.2. Methodology
3.2.1. Motivation
3.2.2. Image Augmentation and Preprocessing
3.2.3. Deep Learning (DL)
3.2.4. SkinNetX Model
3.3. Transfer Learning (TL)
3.3.1. Xception Model
3.3.2. MobileNetV2
3.3.3. AlexNet Model
3.3.4. DenseNet121 Model
3.3.5. InceptionV3 Model
3.4. Hyperparameter Setting
3.5. Performance Evaluation Metrics
4. Results and Discussion
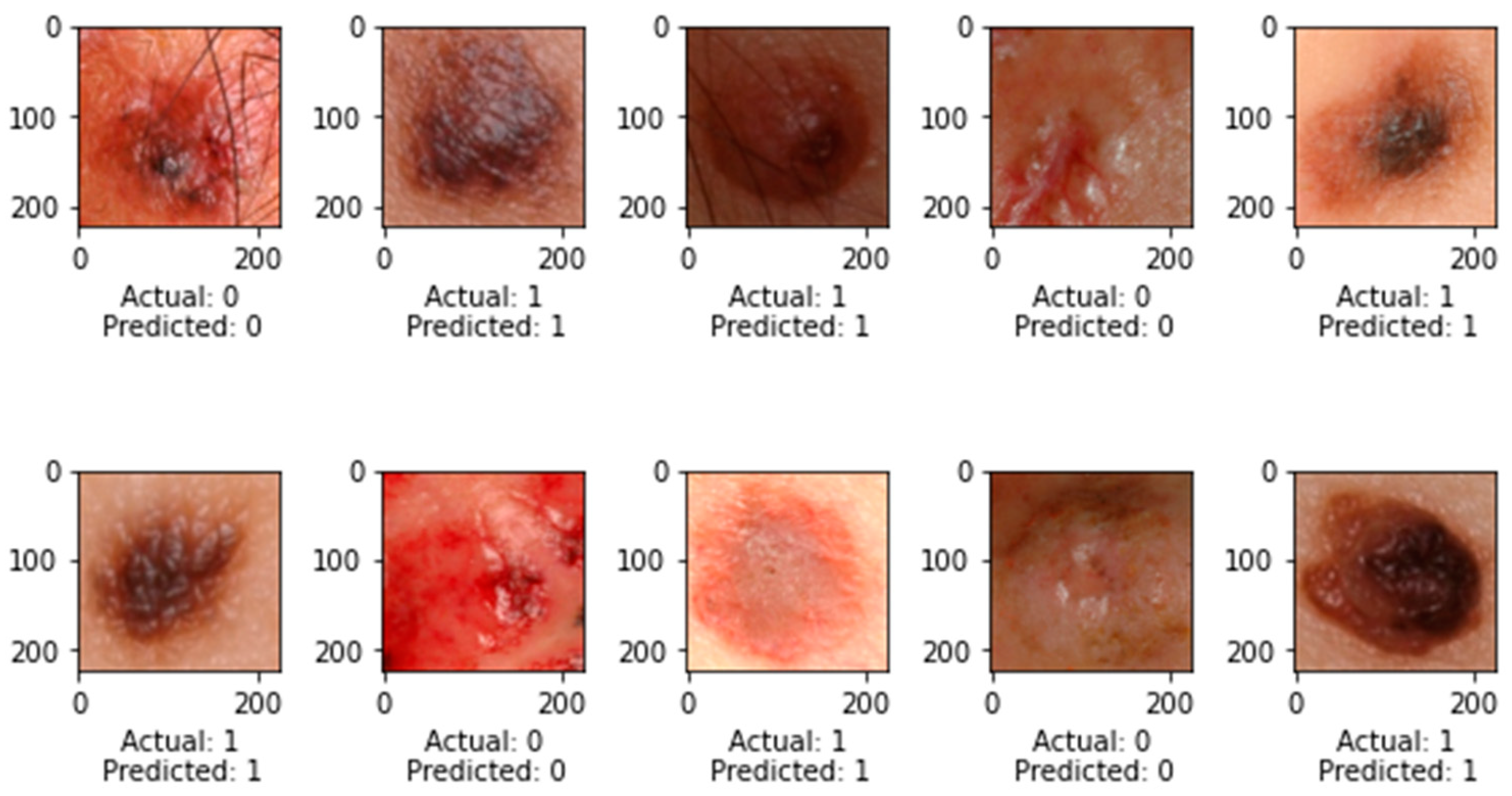
4.1. Performance Evaluation of SkinNetX Model
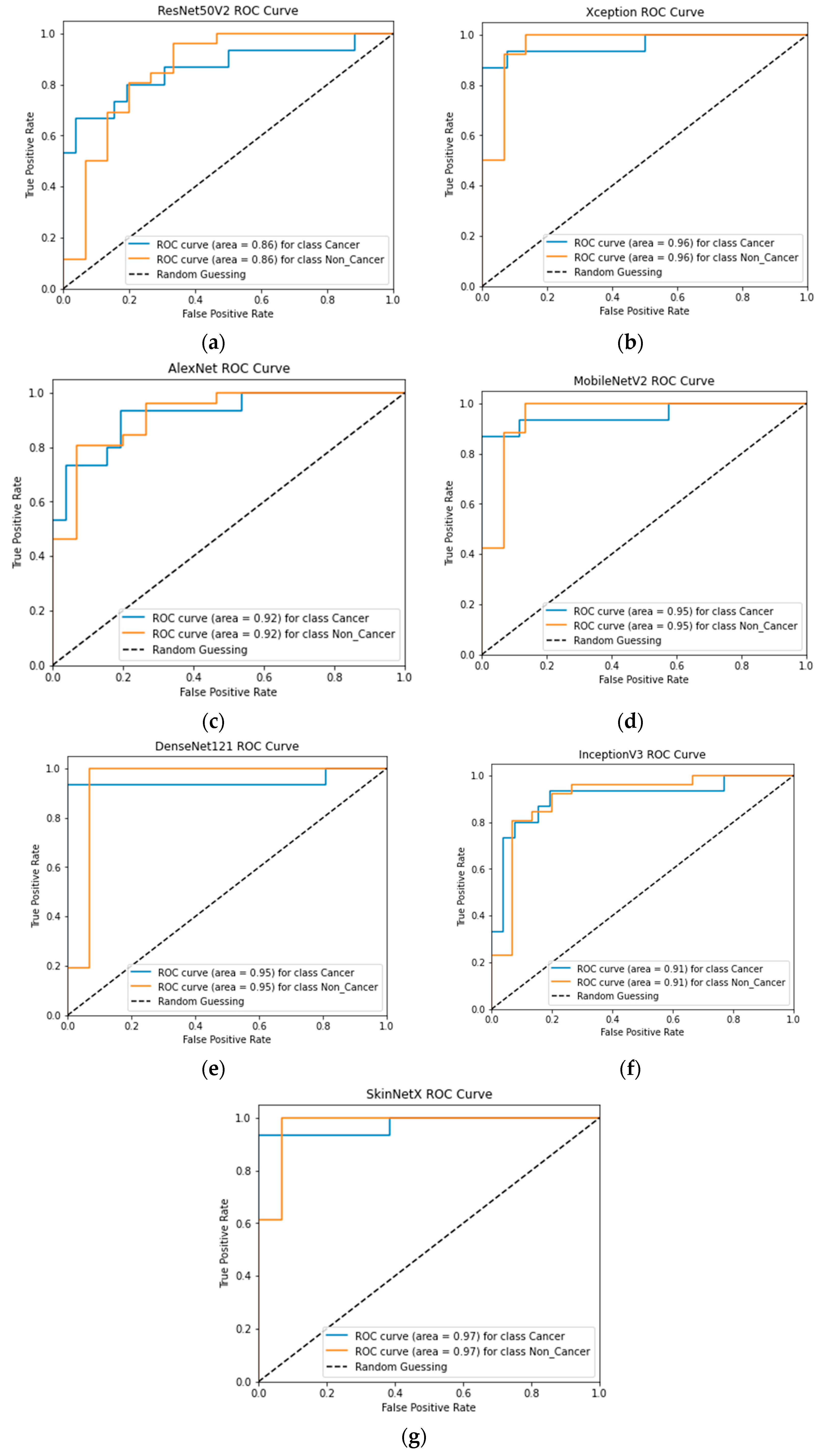
4.2. Comparative Evaluation Using Cutting-Edge Pre-Trained DL Models
4.3. Comparative Studies with Recent Research
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rembielak, A.; Ajithkumar, T. Non-Melanoma Skin Cancer—An Underestimated Global Health Threat? Clin. Oncol. 2019, 31, 735–737. [Google Scholar] [CrossRef]
- Hopkins, Z.H.; Secrest, A.M. Public health implications of Google searches for sunscreen, sunburn, skin cancer, and melanoma in the United States. Am. J. Health Promot. 2019, 33, 611–615. [Google Scholar] [CrossRef]
- Santos, M.O. Estimate 2018: Cancer incidence in Brazil. Rev. Bras. Cancerol. 2018, 64, 119–120. [Google Scholar] [CrossRef]
- Adegun, A.A.; Viriri, S.; Ogundokun, R.O. Deep Learning Approach for Medical Image Analysis. Comput. Intell. Neurosci. 2021, 2021, 6215281. [Google Scholar] [CrossRef]
- Adegun, A.A.; Ogundokun, R.O.; Adebiyi, M.O.; Asani, E.O. CAD-based machine learning project for reducing human-factor-related errors in medical image analysis. In Handbook of Research on the Role of Human Factors in IT Project Management; IGI Global: Hershey, Pennsylvania, 2020; pp. 164–172. [Google Scholar]
- Ayo, F.E.; Ogundokun, R.O.; Awotunde, J.B.; Adebiyi, M.O.; Adeniyi, A.E. Severe acne skin disease: A fuzzy-based method for diagnosis. In Proceedings of the Computational Science and Its Applications–ICCSA 2020: 20th International Conference, Cagliari, Italy, 1–4 July 2020; Springer: Berlin/Heidelberg, Germany, 2020. Part VI 20. pp. 320–334. [Google Scholar]
- Li, Q.-K.; Lin, H.; Tan, X.; Du, S. H∞ Consensus for Multiagent-Based Supply Chain Systems Under Switching Topology and Uncertain Demands. IEEE Trans. Syst. Man Cybern. Syst. 2020, 50, 4905–4918. [Google Scholar] [CrossRef]
- Tan, X.; Lin, J.; Xu, K.; Chen, P.; Ma, L.; Lau, R.W. Mirror Detection with the Visual Chirality Cue. IEEE Trans. Pattern Anal. Mach. Intell. 2023, 45, 3492–3504. [Google Scholar] [CrossRef]
- Zhang, X.; Lu, Z.; Yuan, X.; Wang, Y.; Shen, X. L2-Gain Adaptive Robust Control for Hybrid Energy Storage System in Electric Vehicles. IEEE Trans. Power Electron. 2021, 36, 7319–7332. [Google Scholar] [CrossRef]
- Liu, N.; Liang, G.; Li, L.; Zhou, H.; Zhang, L.; Song, X. An eyelid parameters auto-measuring method based on 3D scanning. Displays 2021, 69, 102063. [Google Scholar] [CrossRef]
- Raza, K.; Singh, N.K. A tour of unsupervised deep learning for medical image analysis. Curr. Med. Imaging 2021, 17, 1059–1077. [Google Scholar]
- Cheng, L.; Yin, F.; Theodoridis, S.; Chatzis, S.; Chang, T.-H. Rethinking Bayesian Learning for Data Analysis: The art of prior and inference in sparsity-aware modeling. IEEE Signal Process. Mag. 2022, 39, 18–52. [Google Scholar] [CrossRef]
- Li, C.; Lin, L.; Zhang, L.; Xu, R.; Chen, X.; Ji, J.; Li, Y. Long noncoding RNA p21 enhances autophagy to alleviate endothelial progenitor cells damage and promote endothelial repair in hypertension through SESN2/AMPK/TSC2 pathway. Pharmacol. Res. 2021, 173, 105920. [Google Scholar] [CrossRef] [PubMed]
- Jin, K.; Gao, Z.; Jiang, X.; Wang, Y.; Ma, X.; Li, Y.; Ye, J. MSHF: A Multi-Source Heterogeneous Fundus (MSHF) Dataset for Image Quality Assessment. Sci. Data 2023, 10, 286. [Google Scholar] [CrossRef]
- Xiong, S.; Li, B.; Zhu, S. DCGNN: A single-stage 3D object detection network based on density clustering and graph neural network. Complex Intell. Syst. 2022, 9, 3399–3408. [Google Scholar] [CrossRef]
- Deng, X.; Liu, E.; Li, S.; Duan, Y.; Xu, M. Interpretable Multi-Modal Image Registration Network Based on Disentangled Convolutional Sparse Coding. IEEE Trans. Image Process. 2023, 32, 1078–1091. [Google Scholar] [CrossRef]
- Dang, W.; Xiang, L.; Liu, S.; Yang, B.; Liu, M.; Yin, Z.; Yin, L.; Zheng, W. A Feature Matching Method based on the Convolutional Neural Network. J. Imaging Sci. Technol. 2023, 67, 030402. [Google Scholar] [CrossRef]
- Lu, S.; Yang, B.; Xiao, Y.; Liu, S.; Liu, M.; Yin, L.; Zheng, W. Iterative reconstruction of low-dose CT based on differential sparse. Biomed. Signal Process. Control. 2023, 79, 104204. [Google Scholar] [CrossRef]
- Xu, H.; Van der Jeught, K.; Zhou, Z.; Zhang, L.; Yu, T.; Sun, Y.; Li, Y.; Wan, C.; So, K.M.; Liu, D.; et al. Atractylenolide I enhances responsiveness to immune checkpoint blockade therapy by activating tumor antigen presentation. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Brinker, T.J.; Hekler, A.; Utikal, J.S.; Grabe, N.; Schadendorf, D.; Klode, J.; Berking, C.; Steeb, T.; Enk, A.H.; von Kalle, C. Skin cancer classification using convolutional neural networks: Systematic review. J. Med. Internet Res. 2018, 20, e11936. [Google Scholar] [CrossRef]
- Lv, Z.; Qiao, L.; Li, J.; Song, H. Deep-Learning-Enabled Security Issues in the Internet of Things. IEEE Internet Things J. 2020, 8, 9531–9538. [Google Scholar] [CrossRef]
- Pan, S.J.; Yang, Q. A survey on transfer learning. IEEE Trans. Knowl. Data Eng. 2010, 22, 1345–1359. [Google Scholar] [CrossRef]
- Shorten, C.; Khoshgoftaar, T.M. A survey on Image Data Augmentation for Deep Learning. J. Big Data 2019, 6, 60. [Google Scholar] [CrossRef]
- Nath, R.P.; Balaji, V.N. Artificial intelligence in power systems. In IOSR Journal of Computer Engineering (IOSR-JCE); Jeppiaar Engineering College: Chennai, India, 2014; ISSN 2278-0661. [Google Scholar]
- Rashid, J.; Ishfaq, M.; Ali, G.; Saeed, M.R.; Hussain, M.; Alkhalifah, T.; Alturise, F.; Samand, N. Skin Cancer Disease Detection Using Transfer Learning Technique. Appl. Sci. 2022, 12, 5714. [Google Scholar] [CrossRef]
- Xu, Y.; Ahokangas, P.; Louis, J.N.; Pongrácz, E. Electricity market empowered by artificial intelligence: A platform approach. Energies 2019, 12, 4128. [Google Scholar] [CrossRef]
- Kourou, K.; Exarchos, T.P.; Exarchos, K.P.; Karamouzis, M.V.; Fotiadis, D.I. Machine learning applications in cancer prognosis and prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef]
- Cruz, J.A.; Wishart, D.S. Applications of Machine Learning in Cancer Prediction and Prognosis. Cancer Informatics 2006, 2, 59–77. [Google Scholar] [CrossRef]
- Sohail, M.; Ali, G.; Rashid, J.; Ahmad, I.; Almotiri, S.H.; AlGhamdi, M.A.; Nagra, A.A.; Masood, K. Racial Identity-Aware Facial Expression Recognition Using Deep Convolutional Neural Networks. Appl. Sci. 2021, 12, 88. [Google Scholar] [CrossRef]
- Rashid, J.; Khan, I.; Ali, G.; Almotiri, S.H.; AlGhamdi, M.A.; Masood, K. Multi-Level Deep Learning Model for Potato Leaf Disease Recognition. Electronics 2021, 10, 2064. [Google Scholar] [CrossRef]
- Arowolo, M.O.; Ogundokun, R.O.; Misra, S.; Agboola, B.D.; Gupta, B. Machine learning-based IoT system for COVID-19 epidemics. Computing 2023, 105, 831–847. [Google Scholar] [CrossRef]
- Hordri, N.F.; Yuhaniz, S.S.; Shamsuddin, S.M. Deep learning and its applications: A review. In Proceedings of the Conference on Postgraduate Annual Research on Informatics Seminar, Kuala Lumpur, Malaysia, 26 October 2016; pp. 1–5. [Google Scholar]
- Zeng, Q.; Bie, B.; Guo, Q.; Yuan, Y.; Han, Q.; Han, X.; Chen, M.; Zhang, X.; Yang, Y.; Liu, M.; et al. Hyperpolarized Xe NMR signal advancement by metal-organic framework entrapment in aqueous solution. Proc. Natl. Acad. Sci. USA 2020, 117, 17558–17563. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Omotosho, A.; Asani, E.O.; Ogundokun, R.O.; Ananti, E.C.; Adegun, A. A neuro-fuzzy based system for the classification of cells as cancerous or non-cancerous. Int. J. Med. Res. Health Sci. 2018, 7, 155–166. [Google Scholar]
- Fujisawa, Y.; Inoue, S.; Nakamura, Y. The possibility of deep learning-based, computer-aided skin tumor classifiers. Front. Med. 2019, 6, 191. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Yao, H.; Zhang, S. An efficient way to refine DenseNet. Signal Image Video Process. 2019, 13, 959–965. [Google Scholar] [CrossRef]
- Shin, H.-C.; Roth, H.R.; Gao, M.; Lu, L.; Xu, Z.; Nogues, I.; Yao, J.; Mollura, D.; Summers, R.M. Deep convolutional neural networks for computer-aided detection: CNN architectures, dataset characteristics and transfer learning. IEEE Trans. Med. Imaging 2016, 35, 1285–1298. [Google Scholar] [CrossRef]
- Pham, B.T.; Jaafari, A.; Prakash, I.; Bui, D.T. A novel hybrid intelligent model of support vector machines and the MultiBoost ensemble for landslide susceptibility modeling. Bull. Eng. Geol. Environ. 2019, 78, 2865–2886. [Google Scholar] [CrossRef]
- Salamon, J.; Bello, J.P. Deep Convolutional Neural Networks and Data Augmentation for Environmental Sound Classification. IEEE Signal Process. Lett. 2017, 24, 279–283. [Google Scholar] [CrossRef]
- Matsunaga, K.; Hamada, A.; Minagawa, A.; Koga, H. Image classification of melanoma, nevus and seborrheic keratosis by deep neural network ensemble. arXiv 2017, arXiv:1703.03108. [Google Scholar]
- Albahar, M.A. Skin Lesion Classification Using Convolutional Neural Network With Novel Regularizer. IEEE Access 2019, 7, 38306–38313. [Google Scholar] [CrossRef]
- Ao, J.; Shao, X.; Liu, Z.; Liu, Q.; Xia, J.; Shi, Y.; Qi, L.; Pan, J.; Ji, M. Stimulated Raman Scattering Microscopy Enables Gleason Scoring of Prostate Core Needle Biopsy by a Convolutional Neural Network. Cancer Res. 2023, 83, 641–651. [Google Scholar] [CrossRef]
- Zhuang, Y.; Chen, S.; Jiang, N.; Hu, H. An Effective WSSENet-Based Similarity Retrieval Method of Large Lung CT Image Databases. KSII Trans. Internet Inf. Syst. 2022, 16, 2359–2376. [Google Scholar] [CrossRef]
- Zhuang, Y.; Jiang, N.; Xu, Y. Progressive Distributed and Parallel Similarity Retrieval of Large CT Image Sequences in Mobile Telemedicine Networks. Wirel. Commun. Mob. Comput. 2022, 2022, 6458350. [Google Scholar] [CrossRef]
- Lu, S.; Yang, J.; Yang, B.; Yin, Z.; Liu, M.; Yin, L.; Zheng, W. Analysis and Design of Surgical Instrument Localization Algorithm. Comput. Model. Eng. Sci. 2023, 137, 669–685. [Google Scholar] [CrossRef]
- Wang, Q.; Sun, L.; Wang, Y.; Zhou, M.; Hu, M.; Chen, J.; Wen, Y.; Li, Q. Identification of melanoma from hyperspectral pathology image using 3D convolutional networks. IEEE Trans. Med. Imaging 2020, 40, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Li, D.; Zhu, X. Cancer immunotherapy: Pros, cons and beyond. Biomed. Pharmacother. 2020, 124, 109821. [Google Scholar] [CrossRef] [PubMed]
- Sinikumpu, S.-P.; Jokelainen, J.; Keinänen-Kiukaanniemi, S.; Huilaja, L. Skin cancers and their risk factors in older persons: A population-based study. BMC Geriatr. 2022, 22, 269. [Google Scholar] [CrossRef] [PubMed]
- Jinnai, S.; Yamazaki, N.; Hirano, Y.; Sugawara, Y.; Ohe, Y.; Hamamoto, R. The Development of a Skin Cancer Classification System for Pigmented Skin Lesions Using Deep Learning. Biomolecules 2020, 10, 1123. [Google Scholar] [CrossRef] [PubMed]
- Parker, E.R. The influence of climate change on skin cancer incidence—A review of the evidence. Int. J. Women’s Dermatol. 2020, 7, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Efimenko, M.; Ignatev, A.; Koshechkin, K. Review of medical image recognition technologies to detect melanomas using neural networks. BMC Bioinform. 2020, 21, 270. [Google Scholar] [CrossRef]
- Zhuo, Z.; Du, L.; Lu, X.; Chen, J.; Cao, Z. Smoothed Lv Distribution Based Three-Dimensional Imaging for Spinning Space Debris. IEEE Trans. Geosci. Remote. Sens. 2022, 60, 1–13. [Google Scholar] [CrossRef]
- Ojukwu, C.E. Melanoma skin cancer detection using support vector machines and convolutional neural networks. Int. J. Sci. Res. Comput. Sci. Eng. 2021, 9, 9–12. [Google Scholar]
- Mohapatra, S.; Abhishek NV, S.; Bardhan, D.; Ghosh, A.A.; Mohanty, S. Skin cancer classification using convolution neural networks. In Advances in Distributed Computing and Machine Learning: Proceedings of ICADCML 2020; Springer: Singapore, 2020; pp. 433–442. [Google Scholar]
- Azghadi, M.R.; Lammie, C.; Eshraghian, J.K.; Payvand, M.; Donati, E.; Linares-Barranco, B.; Indiveri, G. Hardware implementation of deep network accelerators towards healthcare and biomedical applications. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 1138–1159. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Shen, Q.; Ma, Y.; Liu, L.; Jia, W.; Chen, L.; Xie, J. Calcium Homeostasis in Parkinson’s Disease: From Pathology to Treatment. Neurosci. Bull. 2022, 38, 1267–1270. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Hu, X.; Sun, J.; Liu, J. Hyperspectral anomaly detection using ensemble and robust collaborative representation. Inf. Sci. 2023, 624, 748–760. [Google Scholar] [CrossRef]
- Nie, W.; Bao, Y.; Zhao, Y.; Liu, A. Long Dialogue Emotion Detection Based on Commonsense Knowledge Graph Guidance. IEEE Trans. Multimed. 2023, 1–15. [Google Scholar] [CrossRef]
- Gao, Z.; Pan, X.; Shao, J.; Jiang, X.; Su, Z.; Jin, K.; Ye, J. Automatic interpretation and clinical evaluation for fundus fluorescein angiography images of diabetic retinopathy patients by deep learning. Br. J. Ophthalmol. 2022, 321472. [Google Scholar] [CrossRef] [PubMed]
- Giotis, I.; Molders, N.; Land, S.; Biehl, M.; Jonkman, M.F.; Petkov, N. MED-NODE: A computer-assisted melanoma diagnosis system using non-dermoscopic images. Expert Syst. Appl. 2015, 42, 6578–6585. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, N.; Liu, A.-A.; Li, W.; Zhang, Y. High-Order Interaction Learning for Image Captioning. IEEE Trans. Circuits Syst. Video Technol. 2022, 32, 4417–4430. [Google Scholar] [CrossRef]
- Yang, S.; Li, Q.; Li, W.; Li, X.; Liu, A.-A. Dual-Level Representation Enhancement on Characteristic and Context for Image-Text Retrieval. IEEE Trans. Circuits Syst. Video Technol. 2022, 32, 8037–8050. [Google Scholar] [CrossRef]
- Wang, W.; Chen, Z.; Yuan, X. Simple low-light image enhancement based on Weber–Fechner law in logarithmic space. Signal Process. Image Commun. 2022, 106, 116742. [Google Scholar] [CrossRef]
- Zhao, L.; Wang, L. A new lightweight network based on MobileNetV3. KSII Trans. Internet Inf. Syst. 2022, 16, 1–15. [Google Scholar] [CrossRef]
- Khan, M.Q.; Hussain, A.; Rehman, S.U.; Khan, U.; Maqsood, M.; Mehmood, K.; Khan, M.A. Classification of Melanoma and Nevus in Digital Images for Diagnosis of Skin Cancer. IEEE Access 2019, 7, 90132–90144. [Google Scholar] [CrossRef]
- Filali, Y.; ELKhoukhi, H.; Sabri, M.A.; Aarab, A. Efficient fusion of hand-crafted and pre-trained CNNs features to classify melanoma skin cancer. Multimed. Tools Appl. 2020, 79, 31219–31238. [Google Scholar] [CrossRef]
- Hu, K.; Niu, X.; Liu, S.; Zhang, Y.; Cao, C.; Xiao, F.; Yang, W.; Gao, X. Classification of melanoma based on feature similarity measurement for codebook learning in the bag-of-features model. Biomed. Signal Process. Control. 2019, 51, 200–209. [Google Scholar] [CrossRef]
- Abbas, Q.; Celebi, M.E. DermoDeep-A classification of melanoma-nevus skin lesions using multi-feature fusion of visual features and deep neural network. Multimed. Tools Appl. 2019, 78, 23559–23580. [Google Scholar] [CrossRef]
- Dalila, F.; Zohra, A.; Reda, K.; Hocine, C. Segmentation and classification of melanoma and benign skin lesions. Optik 2017, 140, 749–761. [Google Scholar] [CrossRef]
- Almansour, E.; Jaffar, M.A. Classification of Dermoscopic skin cancer images using color and hybrid texture features. IJCSNS 2016, 16, 135–139. [Google Scholar]
- Pham, T.C.; Luong, C.M.; Visani, M.; Hoang, V.D. Deep CNN and data augmentation for skin lesion classification. In Proceedings of the Intelligent Information and Database Systems: 10th Asian Conference, ACIIDS 2018, Dong Hoi City, Vietnam, 19–21 March 2018; Springer: Berlin/Heidelberg, Germany, 2018. Part II 10. pp. 573–582. [Google Scholar]
- Yu, L.; Chen, H.; Dou, Q.; Qin, J.; Heng, P.A. Automated Melanoma Recognition in Dermoscopy Images via Very Deep Residual Networks. IEEE Trans. Med. Imaging 2016, 36, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Rokhana, R.; Herulambang, W.; Indraswari, R. Deep convolutional neural network for melanoma image classification. In Proceedings of the 2020 International Electronics Symposium (IES), Marrakech, Morocco, 24–26 March 2020; pp. 481–486. [Google Scholar]
- Xie, F.-Y.; Fan, H.; Li, Y.; Jiang, Z.-G.; Meng, R.-S.; Bovik, A. Melanoma Classification on Dermoscopy Images Using a Neural Network Ensemble Model. IEEE Trans. Med. Imaging 2016, 36, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Liberman, G.; Acevedo, D.; Mejail, M. Classification of melanoma images with fisher vectors and deep learning. In Iberoamerican Congress on Pattern Recognition; Springer: Berlin/Heidelberg, Germany, 2018; pp. 732–739. [Google Scholar]
- Zhou, Q.; Shi, Y.; Xu, Z.; Qu, R.; Xu, G. Classifying melanoma skin lesions using convolutional spiking neural networks with unsupervised stdp learning rule. IEEE Access 2020, 8, 101309–101319. [Google Scholar] [CrossRef]
- Hosny, K.M.; Kassem, M.A.; Foaud, M.M. Skin melanoma classification using ROI and data augmentation with deep convolutional neural networks. Multimed. Tools Appl. 2020, 79, 24029–24055. [Google Scholar] [CrossRef]
- Mukherjee, S.; Adhikari, A.; Roy, M. Malignant melanoma classification using cross-platform dataset with deep learning CNN architecture. In Recent Trends in Signal and Image Processing; Springer: Berlin/Heidelberg, Germany, 2019; pp. 31–41. [Google Scholar]
- Esteva, A.; Kuprel, B.; Thrun, S. Deep Networks for Early Stage Skin Disease and Skin Cancer Classification; Stanford University: Stanford, CA, USA, 2015. [Google Scholar]
- Çakmak, M.; Tenekecı, M.E. Melanoma detection from dermoscopy images using Nasnet Mobile with Transfer Learning. In Proceedings of the 2021 29th Signal Processing and Communications Applications Conference (SIU), Istanbul, Turkey, 9–11 June 2021; pp. 1–4. [Google Scholar]
- Han, S.S.; Kim, M.S.; Lim, W.; Park, G.H.; Park, I.; Chang, S.E. Classification of the clinical images for benign and malignant cutaneous tumors using a deep learning algorithm. J. Investig. Dermatol. 2018, 138, 1529–1538. [Google Scholar] [CrossRef]
- Hosny, K.M.; Kassem, M.A.; Foaud, M.M. Classification of skin lesions using transfer learning and augmentation with Alex-net. PLoS ONE 2019, 14, e0217293. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Ogundokun, R.O.; Misra, S.; Douglas, M.; Damaševičius, R.; Maskeliūnas, R. Medical Internet-of-Things Based Breast Cancer Diagnosis Using Hyperparameter-Optimized Neural Networks. Futur. Internet 2022, 14, 153. [Google Scholar] [CrossRef]
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Ogundokun, R.O.; Maskeliūnas, R.; Damaševičius, R. Human posture detection using image augmentation and hyperparameter-optimized transfer learning algorithms. Appl. Sci. 2022, 12, 10156. [Google Scholar] [CrossRef]
- Sharma, S.; Kumar, S. The Xception model: A potential feature extractor in breast cancer histology images classification. ICT Express 2022, 8, 101–108. [Google Scholar] [CrossRef]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Dong, K.; Zhou, C.; Ruan, Y.; Li, Y. MobileNetV2 model for image classification. In Proceedings of the 2020 2nd International Conference on Information Technology and Computer Application (ITCA), Guangzhou, China, 18–20 December 2020; pp. 476–480. [Google Scholar]
- Ahsan, M.; Nazim, R.; Siddique, Z.; Huebner, P. Detection of COVID-19 Patients from CT Scan and Chest X-ray Data Using Modified MobileNetV2 and LIME. Healthcare 2021, 9, 1099. [Google Scholar] [CrossRef]
- Xiao, L.; Yan, Q.; Deng, S. Scene classification with improved AlexNet model. In Proceedings of the 2017 12th International Conference on Intelligent Systems and Knowledge Engineering (ISKE), Nanjing, China, 24–26 November 2017; pp. 1–6. [Google Scholar]
- Nandhini, S.; Ashokkumar, K. An automatic plant leaf disease identification using DenseNet-121 architecture with a mutation-based henry gas solubility optimization algorithm. Neural Comput. Appl. 2022, 34, 5513–5534. [Google Scholar] [CrossRef]
- Zhou, Z.; Yang, X.; Ji, J.; Wang, Y.; Zhu, Z. Classifying fabric defects with evolving Inception v3 by improved L2, 1-norm regularized extreme learning machine. Text. Res. J. 2023, 93, 936–956. [Google Scholar] [CrossRef]
- Tembhurne, J.V.; Hebbar, N.; Patil, H.Y.; Diwan, T. Skin cancer detection using ensemble of machine learning and deep learning techniques. Multimed. Tools Appl. 2023, 82, 27501–27524. [Google Scholar] [CrossRef]
- Mehr, R.A.; Ameri, A. Skin Cancer Detection Based on Deep Learning. J. Biomed. Phys. Eng. 2022, 12, 559–568. [Google Scholar]
- Huang, H.; Hsu, B.W.; Lee, C.; Tseng, V.S. Development of a light-weight deep learning model for cloud applications and remote diagnosis of skin cancers. J. Dermatol. 2021, 48, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F. GitHub—Keras-Team/Keras: Deep Learning for Humans. 2015. Available online: https://github.com/keras-team/keras (accessed on 29 June 2023).
- FAQ—Keras Documentation. 2019. Available online: https://keras.io/getting-started/faq/#why-is-the-training-loss-much-higher-than-the-testing-loss (accessed on 29 June 2023).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer Type | Number of Filters |
|---|---|
| MobileNetV2 | |
| GlobalAveragePooling2D | |
| Dense | 256 |
| Dropout | 0.5 |
| Dense | 512 |
| Xception | |
| GlobalAveragePooling2D | |
| Dense | 256 |
| Dropout | 0.5 |
| Dense | 512 |
| Concatenate | |
| Dense | 2 |
| Model | Depth | Parameters (M) | Size (MB) |
|---|---|---|---|
| AlexNet | 11 | 60 | 227 |
| DenseNet121 | 242 | 8.1 | 33 |
| MobileNetV2 | 105 | 3.5 | 14 |
| Xception | 81 | 22.9 | 88 |
| InceptionV3 | 189 | 23.9 | 92 |
| ResNet50V2 | 103 | 25.6 | 98 |
| Parameter | Values |
|---|---|
| Learning rate | 0.0001 |
| Optimizer | SGD |
| Epochs | 100 |
| Verbose | 1 |
| Activation function | ReLU |
| Iteration per epoch | 12 |
| Early stopping | Patience = 80 |
| Model | Accuracy | Precision | Recall | F1-Score | Misclass | AUC |
|---|---|---|---|---|---|---|
| Proposed Model | 97.56 | 93.33 | 100 | 96.55 | 0.0244 | 97.00 |
| Xception | 85.37 | 93.33 | 73.68 | 82.35 | 0.1463 | 96.00 |
| MobileNetV2 | 90.24 | 93.33 | 82.35 | 87.50 | 0.0976 | 95.00 |
| AlexNet | 80.49 | 80.00 | 70.59 | 75.00 | 0.1951 | 92.00 |
| InceptionV3 | 82.93 | 70.00 | 93.33 | 80.00 | 0.1707 | 91.00 |
| DenseNet121 | 95.12 | 93.33 | 93.33 | 93.33 | 0.0488 | 95.00 |
| ResNet50V2 | 77.50 | 92.86 | 61.90 | 74.29 | 0.2250 | 86.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogundokun, R.O.; Li, A.; Babatunde, R.S.; Umezuruike, C.; Sadiku, P.O.; Abdulahi, A.T.; Babatunde, A.N. Enhancing Skin Cancer Detection and Classification in Dermoscopic Images through Concatenated MobileNetV2 and Xception Models. Bioengineering 2023, 10, 979. https://doi.org/10.3390/bioengineering10080979
Ogundokun RO, Li A, Babatunde RS, Umezuruike C, Sadiku PO, Abdulahi AT, Babatunde AN. Enhancing Skin Cancer Detection and Classification in Dermoscopic Images through Concatenated MobileNetV2 and Xception Models. Bioengineering. 2023; 10(8):979. https://doi.org/10.3390/bioengineering10080979
Chicago/Turabian StyleOgundokun, Roseline Oluwaseun, Aiman Li, Ronke Seyi Babatunde, Chinecherem Umezuruike, Peter O. Sadiku, AbdulRahman Tosho Abdulahi, and Akinbowale Nathaniel Babatunde. 2023. "Enhancing Skin Cancer Detection and Classification in Dermoscopic Images through Concatenated MobileNetV2 and Xception Models" Bioengineering 10, no. 8: 979. https://doi.org/10.3390/bioengineering10080979