
Retrospective Analysis of Responders and Impaired Patients with Knee Osteoarthritis Treated with Two Consecutive Injections of Very Pure Platelet-Rich Plasma (PRP)
 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PRP Preparation and Infiltration
2.3. Clinical Data Assessment
2.4. Radiographic Assessment
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Demographic Assessment: Comparison of Responders, Non-Responders and Impaired Patients
3.3. Biological Characteristics of PRP Injected
3.4. Clinical Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PRP | Platelet-rich plasma |
| VAS | Visual Analogue Scale |
| WOMAC | Western Ontario, McMaster Universities Osteoarthritis Index |
| KOA | Knee osteoarthritis |
| MPCI | Minimal perceptible clinical improvement |
References
- Kobayashi, S.; Pappas, E.; Fransen, M.; Refshauge, K.; Simic, M. The prevalence of patellofemoral osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2016, 24, 1697–1707. [Google Scholar] [CrossRef] [Green Version]
- van Jonbergen, H.-P.W.; Poolman, R.W.; van Kampen, A. Isolated patellofemoral osteoarthritis. Acta Orthop. 2010, 81, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [Green Version]
- Primorac, D.; Molnar, V.; Rod, E.; Jeleč, Ž.; Čukelj, F.; Matišić, V.; Vrdoljak, T.; Hudetz, D.; Hajsok, H.; Borić, I. Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic Considerations. Genes 2020, 11, 854. [Google Scholar] [CrossRef]
- Kim, Y.-M.; Joo, Y.-B. Patellofemoral osteoarthritis. Knee Surg. Relat. Res. 2012, 24, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Lonner, J.H.; Bloomfield, M.R. The clinical outcome of patellofemoral arthroplasty. Orthop. Clin. N. Am. 2013, 44, 271–280. [Google Scholar] [CrossRef]
- Mont, M.A.; Haas, S.; Mullick, T.; Hungerford, D.S. Total knee arthroplasty for patellofemoral arthritis. J. Bone Jt. Surg. Am. 2002, 84, 1977–1981. [Google Scholar] [CrossRef]
- Laskin, R.S.; van Steijn, M. Total knee replacement for patients with patellofemoral arthritis. Clin. Orthop. Relat. Res. 1999, 367, 89–95. [Google Scholar]
- Hohmann, E.; Tetsworth, K.; Glatt, V. Is platelet-rich plasma effective for the treatment of knee osteoarthritis? A systematic review and meta-analysis of level 1 and 2 randomized controlled trials. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 955–967. [Google Scholar] [CrossRef]
- Tang, J.Z.; Nie, M.J.; Zhao, J.Z.; Zhang, G.C.; Zhang, Q.; Wang, B. Platelet-rich plasma versus hyaluronic acid in the treatment of knee osteoarthritis: A meta-analysis. J. Orthop. Surg. Res. 2020, 15, 403. [Google Scholar] [CrossRef]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2021, 49, 249–260. [Google Scholar] [CrossRef]
- Saraf, A.; Hussain, A.; Bishnoi, S.; Azam, G.; Habib, H. Serial Platelet-Rich Plasma Intra-articular Injections in Kellgren and Lawrence Grade IV Knee Joint Osteoarthritis: A Prospective Blinded Placebo-Controlled Interventional Study. Indian. J. Orthop. 2022, 56, 1722–1728. [Google Scholar] [CrossRef]
- Huda, N.; Islam, M.S.U.; Bishnoi, S.; Kumar, H.; Aggarwal, S.; Ganai, A.A. Role of Triple Injection Platelet-Rich Plasma for Osteoarthritis Knees: A 2 Years Follow-Up Study. Indian. J. Orthop. 2022, 56, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Dhillon, M.S.; Aggarwal, S.; Marwaha, N.; Jain, A. Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: A prospective, double-blind, randomized trial. Am. J. Sports Med. 2013, 41, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Filardo, G.; Kon, E.; Pereira Ruiz, M.T.; Vaccaro, F.; Guitaldi, R.; Di Martino, A.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Leukocyte-poor PRP application for the treatment of knee osteoarthritis. Joints 2013, 1, 112–120. [Google Scholar] [PubMed]
- Vaquerizo, V.; Padilla, S.; Aguirre, J.J.; Begona, L.; Orive, G.; Anitua, E. Two cycles of plasma rich in growth factors (PRGF-Endoret) intra-articular injections improve stiffness and activities of daily living but not pain compared to one cycle on patients with symptomatic knee osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 2615–2621. [Google Scholar] [CrossRef] [PubMed]
- Ehrich, E.W.; Davies, G.M.; Watson, D.J.; Bolognese, J.A.; Seidenberg, B.C.; Bellamy, N. Minimal perceptible clinical improvement with the Western Ontario and McMaster Universities osteoarthritis index questionnaire and global assessments in patients with osteoarthritis. J. Rheumatol. 2000, 27, 2635–2641. [Google Scholar]
- Magalon, J.; Chateau, A.L.; Bertrand, B.; Louis, M.L.; Silvestre, A.; Giraudo, L.; Veran, J.; Sabatier, F. DEPA classification: A proposal for standardising PRP use and a retrospective application of available devices. BMJ Open Sport. Exerc. Med. 2016, 2, e000060. [Google Scholar] [CrossRef] [Green Version]
- Saita, Y.; Kobayashi, Y.; Nishio, H.; Wakayama, T.; Fukusato, S.; Uchino, S.; Momoi, Y.; Ikeda, H.; Kaneko, K. Predictors of Effectiveness of Platelet-Rich Plasma Therapy for Knee Osteoarthritis: A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 4514. [Google Scholar] [CrossRef]
- Chopin, C.; Geoffroy, M.; Kanagaratnam, L.; Dorilleau, C.; Ecarnot, F.; Siboni, R.; Salmon, J.H. Prognostic Factors Related to Clinical Response in 210 Knees Treated by Platelet-Rich Plasma for Osteoarthritis. Diagnostics 2023, 13, 760. [Google Scholar] [CrossRef]
- Bec, C.; Rousset, A.; Brandin, T.; François, P.; Rabarimeriarijaona, S.; Dumoulin, C.; Heleu, G.; Grimaud, F.; Veran, J.; Magalon, G.; et al. A Retrospective Analysis of Characteristic Features of Responders and Impaired Patients to a Single Injection of Pure Platelet-Rich Plasma in Knee Osteoarthritis. J. Clin. Med. 2021, 10, 1748. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.; van der Heijde, D.; Altman, R.D.; Anderson, J.J.; Bellamy, N.; Hochberg, M.; Simon, L.; Strand, V.; Woodworth, T.; Dougados, M. OMERACT-OARSI initiative: Osteoarthritis Research Society International set of responder criteria for osteoarthritis clinical trials revisited. Osteoarthr. Cartil. 2004, 12, 389–399. [Google Scholar] [CrossRef] [Green Version]
- Guillibert, C.; Charpin, C.; Raffray, M.; Benmenni, A.; Dehaut, F.X.; El Ghobeira, G.; Giorgi, R.; Magalon, J.; Arniaud, D. Single Injection of High Volume of Autologous Pure PRP Provides a Significant Improvement in Knee Osteoarthritis: A Prospective Routine Care Study. Int. J. Mol. Sci. 2019, 20, 1327. [Google Scholar] [CrossRef] [Green Version]
- Rastogi, A.K.; Davis, K.W.; Ross, A.; Rosas, H.G. Fundamentals of Joint Injection. AJR Am. J. Roentgenol. 2016, 207, 484–494. [Google Scholar] [CrossRef]
- Huang, G.; Hua, S.; Yang, T.; Ma, J.; Yu, W.; Chen, X. Platelet-rich plasma shows beneficial effects for patients with knee osteoarthritis by suppressing inflammatory factors. Exp. Ther. Med. 2018, 15, 3096–3102. [Google Scholar] [CrossRef] [Green Version]
- Braun, H.J.; Kim, H.J.; Chu, C.R.; Dragoo, J.L. The effect of platelet-rich plasma formulations and blood products on human synoviocytes: Implications for intra-articular injury and therapy. Am. J. Sports Med. 2014, 42, 1204–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooiveld, M.J.; Roosendaal, G.; van den Berg, H.M.; Bijlsma, J.W.; Lafeber, F.P. Haemoglobin-derived iron-dependent hydroxyl radical formation in blood-induced joint damage: An in vitro study. Rheumatology 2003, 42, 784–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Park, Y.B.; Ha, C.W.; Roh, Y.J.; Park, J.G. Adverse Reactions and Clinical Outcomes for Leukocyte-Poor Versus Leukocyte-Rich Platelet-Rich Plasma in Knee Osteoarthritis: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2021, 9, 23259671211011948. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Pereira Ruiz, M.T.; Vaccaro, F.; Guitaldi, R.; Di Martino, A.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Platelet-rich plasma intra-articular injections for cartilage degeneration and osteoarthritis: Single-versus double-spinning approach. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2082–2091. [Google Scholar] [CrossRef]
- Joshi Jubert, N.; Rodriguez, L.; Reverte-Vinaixa, M.M.; Navarro, A. Platelet-Rich Plasma Injections for Advanced Knee Osteoarthritis: A Prospective, Randomized, Double-Blinded Clinical Trial. Orthop. J. Sports Med. 2017, 5, 2325967116689386. [Google Scholar] [CrossRef]
- Louis, M.L.; Magalon, J.; Jouve, E.; Bornet, C.E.; Mattei, J.C.; Chagnaud, C.; Rochwerger, A.; Veran, J.; Sabatier, F. Growth Factors Levels Determine Efficacy of Platelets Rich Plasma Injection in Knee Osteoarthritis: A Randomized Double Blind Noninferiority Trial Compared with Viscosupplementation. Arthroscopy 2018, 34, 1530–1540.e1532. [Google Scholar] [CrossRef] [PubMed]
- Jain, D.; Goyal, T.; Verma, N.; Paswan, A.K.; Dubey, R.K. Intradiscal Platelet-Rich Plasma Injection for Discogenic Low Back Pain and Correlation with Platelet Concentration: A Prospective Clinical Trial. Pain Med. 2020, 21, 2719–2725. [Google Scholar] [CrossRef] [PubMed]
- Bansal, H.; Leon, J.; Pont, J.L.; Wilson, D.A.; Bansal, A.; Agarwal, D.; Preoteasa, I. Platelet-rich plasma (PRP) in osteoarthritis (OA) knee: Correct dose critical for long term clinical efficacy. Sci. Rep. 2021, 11, 3971. [Google Scholar] [CrossRef]
- Vilchez-Cavazos, F.; Millán-Alanís, J.M.; Blázquez-Saldaña, J.; Álvarez-Villalobos, N.; Peña-Martínez, V.M.; Acosta-Olivo, C.A.; Simental-Mendía, M. Comparison of the Clinical Effectiveness of Single Versus Multiple Injections of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2019, 7, 2325967119887116. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, M.; Delgado, D.; Sanchez, P.; Muinos-Lopez, E.; Paiva, B.; Granero-Molto, F.; Prosper, F.; Pompei, O.; Perez, J.C.; Azofra, J.; et al. Combination of Intra-Articular and Intraosseous Injections of Platelet Rich Plasma for Severe Knee Osteoarthritis: A Pilot Study. Biomed. Res. Int. 2016, 2016, 4868613. [Google Scholar] [CrossRef]
- Ríos Luna, A.; Fahandezh-Saddi Díaz, H.; Villanueva Martinez, M.; Prado, R.; Padilla, S.; Anitua, E. Office-Based Intraosseous Infiltrations of PRGF in Knee Osteoarthritis: Description of Technique. Arthrosc. Tech. 2022, 11, e917–e921. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; Jorquera, C.; de Dicastillo, L.L.; Fiz, N.; Knörr, J.; Beitia, M.; Aizpurua, B.; Azofra, J.; Delgado, D. Real-world evidence to assess the effectiveness of platelet-rich plasma in the treatment of knee degenerative pathology: A prospective observational study. Ther. Adv. Musculoskelet. Dis. 2022, 14, 1759720x221100304. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| PRP Responders (N = 36) | PRP Impaired (N = 21) | p-Value | |
|---|---|---|---|
| Gender (M:F), n (%) | 17:19 (47:53) | 11:10 (52:48) | 0.787 |
| Age (years), mean/SD | 52.6 ± 14.0 | 53.9 ± 13.9 | 0.821 |
| BMI (Kg/m2), mean/SD | 25.6 ± 4.0 | 26.0 ± 2.8 | 0.541 |
| KL II-III, n (%) | 30 (83.0) | 11 (52.0) | 0.025 |
| KL IV, n (%) | 6 (16.6) | 10 (48.0) | |
| WOMAC baseline, mean/SD | 43.8 ± 19.65 | 32.5 ± 20.1 | 0.021 |
| VAS baseline, mean/SD | 5.8 ± 2.1 | 4.8 ± 2.2 | 0.076 |
| PRP Responders | PRP Impaired | ||||
|---|---|---|---|---|---|
| 1st PRP | 2nd PRP | 1st PRP | 2nd PRP | ||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | p Value | |
| Injected volume (mL) | 10.0 ± 0.0 | 10.0 ± 0.0 | 10.0 ± 0.0 | 10.0 ± 0.0 | - |
| Platelet concentration (106/mL) | 573 ± 134 | 559 ± 139 | 573 ± 134 | 573 ± 134 | - |
| Leukocyte concentration (106/mL) | 0.5 ± 0.2 | 0.5 ± 0.2 | 0.5 ± 0.2 | 0.5 ± 0.2 | - |
| Red blood cells concentration (109/mL) | 0.01 ± 0.00 | 0.01 ± 0.00 | 0.01 ± 0.01 | 0.01 ± 0.00 | - |
| Quantity of injected platelets (106) | 5724 ± 1344 | 5589 ± 1392 | 5553 ± 1363 | 5778 ± 1271 | 0.928 |
| Quantity of injected leucocytes (106) | 4.5 ± 2.2 | 4.8 ± 2.3 | 4.0 ± 3.3 | 6.0 ± 8.6 | 0.499 |
| Quantity of injected red blood cells (109) | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.467 |
| Relative composition | |||||
| Platelets (%) | 96.7 ± 1.6 | 96.1 ± 2.7 | 96.9 ± 1.6 | 96.5 ± 1.3 | - |
| Leukocytes (%) | 0.1 ± 0.0 | 0.1 ± 0.0 | 0.1 ± 0.1 | 0.1 ± 0.1 | - |
| Red blood cells (%) | 3.3 ± 1.6 | 3.8 ± 2.7 | 3.0 ± 1.6 | 3.4 ± 1.2 | - |
| Groups | ||||
|---|---|---|---|---|
| Variable | Responders | p-Value | Impaired | p-Value |
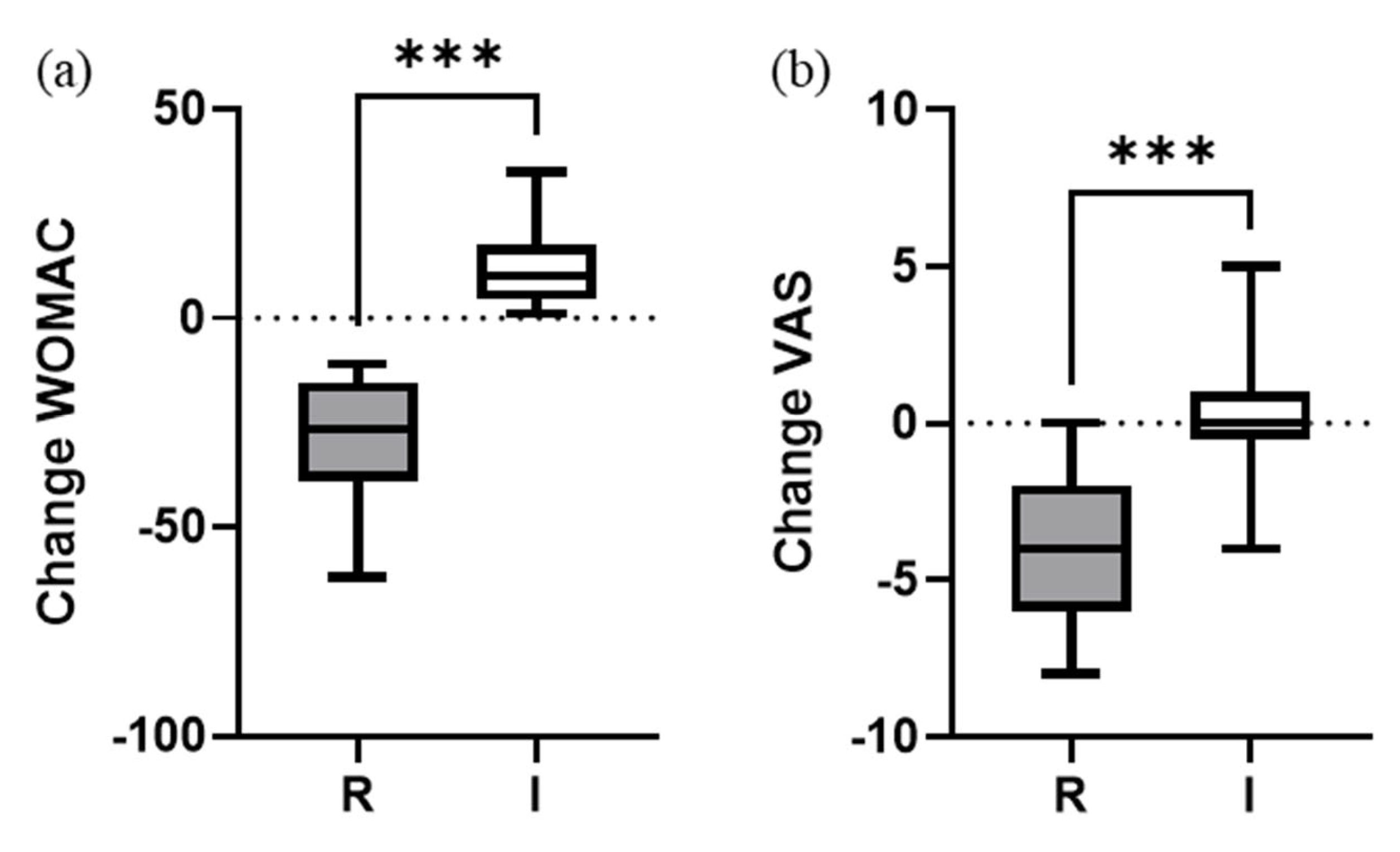
| WOMAC (global) | ||||
| Baseline | 43.8 ± 19.6 | <0.001 | 32.5 ± 20.1 | 0.027 |
| 1 year | 14.6 ± 12.7 | 44.7 ± 20.0 | ||
| Change | −29.2 ± 14.3 | −12.1 ± 9.1 | ||
| 95% CI | −34.1, −24.3 | 7.9, 16.4 | ||
| VAS | ||||
| Baseline | 5.8 ± 2.1 | <0.001 | 4.8 ± 2.2 | 0.843 |
| 1 year | 1.9 ± 1.4 | 4.9 ± 1.7 | ||
| Change | −3.9 ± 2.2 | 0.1 ± 1.9 | ||
| 95% CI | −4.6, −3.1 | −0.7, 1.0 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silvestre, A.; Lintingre, P.-F.; Pesquer, L.; Meyer, P.; Moreau-Durieux, M.-H.; Dallaudiére, B. Retrospective Analysis of Responders and Impaired Patients with Knee Osteoarthritis Treated with Two Consecutive Injections of Very Pure Platelet-Rich Plasma (PRP). Bioengineering 2023, 10, 922. https://doi.org/10.3390/bioengineering10080922
Silvestre A, Lintingre P-F, Pesquer L, Meyer P, Moreau-Durieux M-H, Dallaudiére B. Retrospective Analysis of Responders and Impaired Patients with Knee Osteoarthritis Treated with Two Consecutive Injections of Very Pure Platelet-Rich Plasma (PRP). Bioengineering. 2023; 10(8):922. https://doi.org/10.3390/bioengineering10080922
Chicago/Turabian StyleSilvestre, Alain, Pierre-Francois Lintingre, Lionel Pesquer, Philippe Meyer, Marie-Hélène Moreau-Durieux, and Benjamin Dallaudiére. 2023. "Retrospective Analysis of Responders and Impaired Patients with Knee Osteoarthritis Treated with Two Consecutive Injections of Very Pure Platelet-Rich Plasma (PRP)" Bioengineering 10, no. 8: 922. https://doi.org/10.3390/bioengineering10080922