
Carbon Fiber-Reinforced PolyEtherEtherKetone (CFR-PEEK) Instrumentation in Degenerative Disease of Lumbar Spine: A Pilot Study

 , , ,
, , ,
Abstract
:1. Introduction
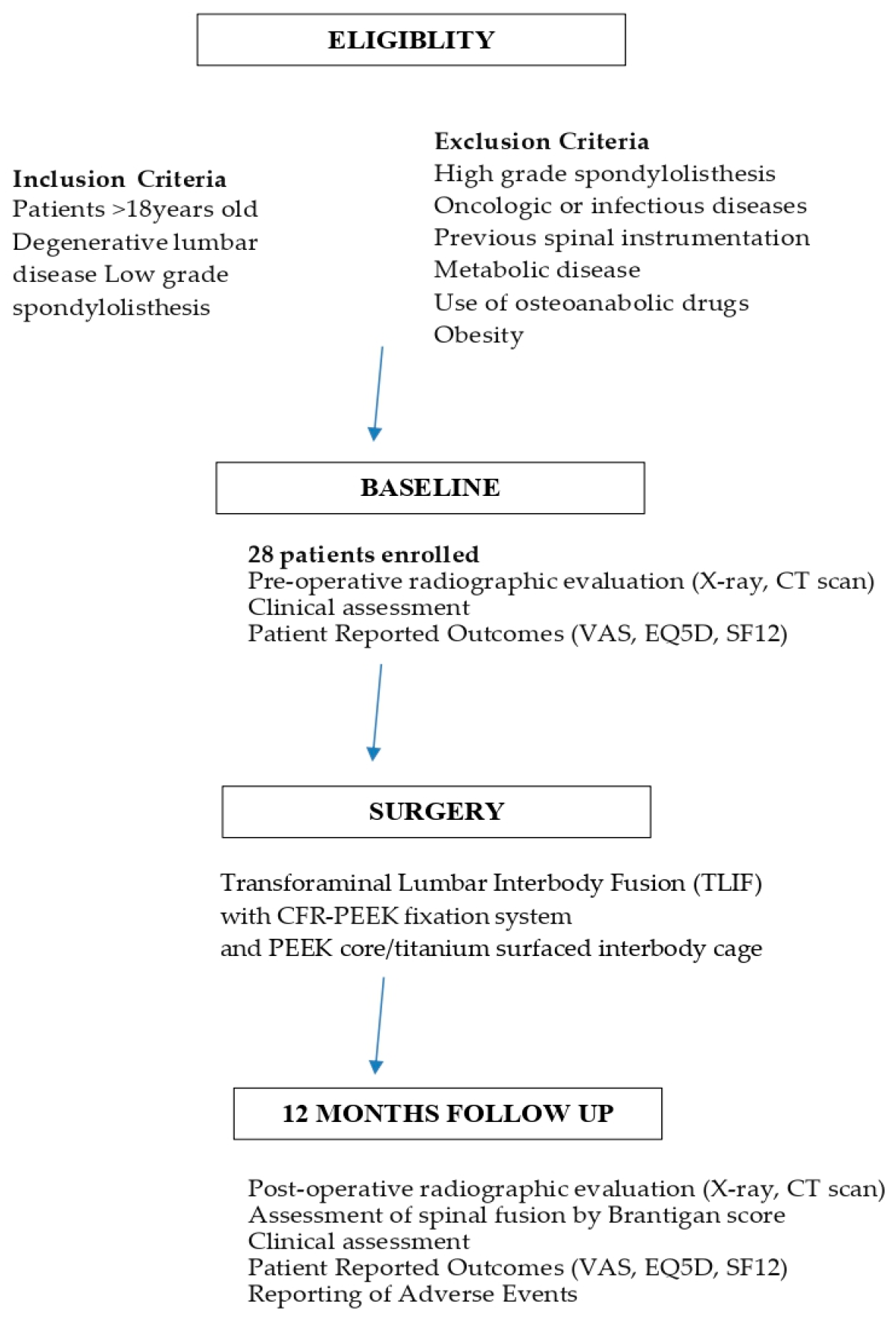
2. Materials and Methods
Statistical Analysis
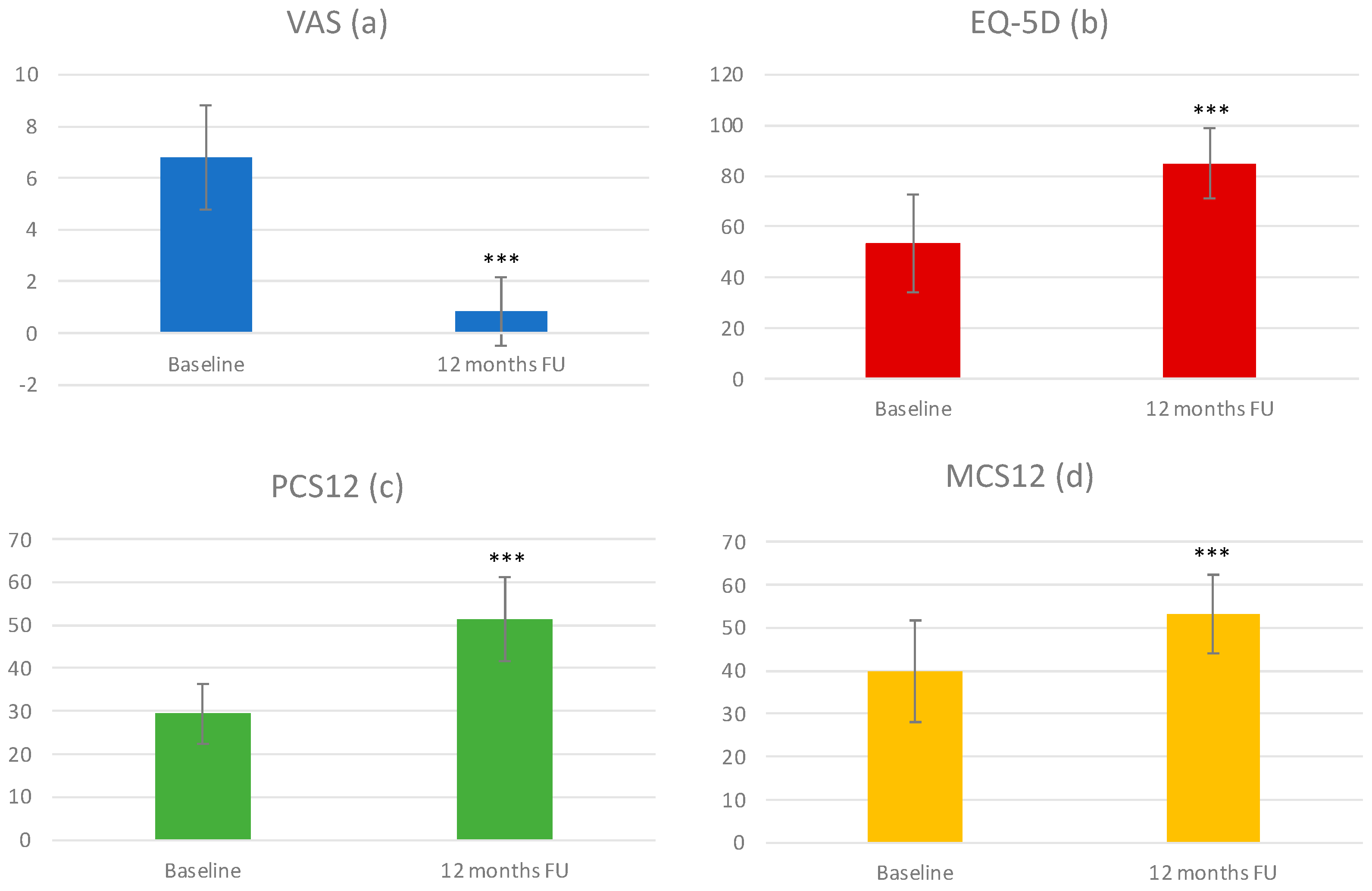
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taal, D.; Madhavan, K.; Chieng, L.O.; Ghobrial, G.M.; Wang, M.Y. Metals in Spine. World Neurosurg. 2017, 100, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Singh, K. Review on titanium and titanium based alloys as biomaterials for orthopaedic applications. Mater. Sci. Eng. C 2019, 102, 844–862. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.R.; Kwon, J.W.; Suk, K.S.; Kim, H.S.; Moon, S.H.; Park, S.Y.; Lee, B.H. The Clinical Use of Osteobiologic and Metallic Biomaterials in Orthopedic Surgery: The Present and the Future. Materials 2023, 16, 3633. [Google Scholar] [CrossRef]
- Rajak, D.K.; Wagh, P.H.; Linul, E. Manufacturing Technologies of Carbon/Glass Fiber-Reinforced Polymer Composites and Their Properties: A Review. Polymers 2021, 13, 3721. [Google Scholar] [CrossRef] [PubMed]
- Nugraha, A.D.; Nuryanta, M.I.; Sean, L.; Budiman, K.; Kusni, M.; Muflikhun, M.A. Recent Progress on Natural Fibers Mixed with CFRP and GFRP: Properties, Characteristics, and Failure Behaviour. Polymers 2022, 14, 5138. [Google Scholar] [CrossRef] [PubMed]
- Avanzini, A.; Battini, D.; Petrogalli, C.; Pandini, S.; Donzella, G. Anisotropic Behaviour of Extruded Short Carbon Fibre Reinforced PEEK Under Static and Fatigue Loading. Appl. Compos. Mater. 2022, 29, 1041–1060. [Google Scholar] [CrossRef]
- Li, C.S.; Vannabouathong, C.; Sprague, S.; Bhandari, M. The Use of Carbon-Fiber-Reinforced (CFR) PEEK Material in Orthopedic Implants: A Systematic Review. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2015, 8, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Long, J.R.; Kalani, M.A.; Goulding, K.A.; Ashman, J.B.; Flug, J.A. Carbon-fiber-reinforced polyetheretherketone orthopedic implants in musculoskeletal and spinal tumors: Imaging and clinical features. Skeletal Radiol. 2023, 52, 393–404. [Google Scholar] [CrossRef]
- Perez-Roman, R.J.; Boddu, J.V.; Bashti, M.; Bryant, J.-P.; Amadasu, E.; Gyedu, J.S.; Wang, M.Y. The Use of Carbon Fiber-Reinforced Instrumentation in Patients with Spinal Oncologic Tumors: A Systematic Review of Literature and Future Directions. World Neurosurg. 2023, 173, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Boriani, S.; Tedesco, G.; Ming, L.; Ghermandi, R.; Amichetti, M.; Fossati, P.; Krengli, M.; Mavilla, L.; Gasbarrini, A. Carbon-fiber-reinforced PEEK fixation system in the treatment of spine tumors: A preliminary report. Eur. Spine J. 2018, 27, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, G.; Gasbarrini, A.; Bandiera, S.; Ghermandi, R.; Boriani, S. Composite PEEK/Carbon fiber implants can increase the effectiveness of radiotherapy in the management of spine tumors. J. Spine Surg. 2017, 3, 323–329, Erratum in J. Spine Surg. 2018, 4, 167. [Google Scholar] [CrossRef] [Green Version]
- Boriani, S.; Pipola, V.; Cecchinato, R.; Ghermandi, R.; Tedesco, G.; Fiore, M.R.; Dionisi, F.; Gasbarrini, A. Composite PEEK/carbon fiber rods in the treatment for bone tumors of the cervical spine: A case series. Eur. Spine J. 2020, 29, 3229–3236. [Google Scholar] [CrossRef] [PubMed]
- Ringel, F.; Ryang, Y.-M.; Kirschke, J.S.; Müller, B.S.; Wilkens, J.J.; Brodard, J.; Combs, S.E.; Meyer, B. Radiolucent Carbon Fiber-Reinforced Pedicle Screws for Treatment of Spinal Tumors: Advantages for Radiation Planning and Follow-Up Imaging. World Neurosurg. 2017, 105, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Qin, W.; Li, Y.; Ma, J.; Liang, Q.; Tang, B. Mechanical properties and cytotoxicity of hierarchical carbon fiber-reinforced poly (ether-ether-ketone) composites used as implant materials. J. Mech. Behav. Biomed. Mater. 2019, 89, 227–233. [Google Scholar] [CrossRef]
- Uri, O.; Folman, Y.; Laufer, G.; Behrbalk, E. A Novel Spine Fixation System Made Entirely of Carbon-Fiber-Reinforced PEEK Composite: An In Vitro Mechanical Evaluation. Adv. Orthop. 2020, 2020, 4796136. [Google Scholar] [CrossRef] [PubMed]
- Bruner, H.J.; Guan, Y.; Yoganandan, N.; Pintar, F.A.; Maiman, D.J.; Slivka, M.A. Biomechanics of polyaryletherketone rod composites and titanium rods for posterior lumbosacral instrumentation. Presented at the 2010 Joint Spine Section Meeting. Laboratory investigation. J. Neurosurg. Spine 2010, 13, 766–772. [Google Scholar] [CrossRef]
- Lindtner, R.A.; Schmid, R.; Nydegger, T.; Konschake, M.; Schmoelz, W. Pedicle screw anchorage of carbon fiber-reinforced PEEK screws under cyclic loading. Eur. Spine J. 2018, 27, 1775–1784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oikonomidis, S.; Greven, J.; Bredow, J.; Eh, M.; Prescher, A.; Fischer, H.; Thüring, J.; Eysel, P.; Hildebrand, F.; Kobbe, P.; et al. Biomechanical effects of posterior pedicle screw-based instrumentation using titanium versus carbon fiber reinforced PEEK in an osteoporotic spine human cadaver model. Clin. Biomech. 2020, 80, 105153. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Yang, D.; Yang, C.; Spintzyk, S.; Scheideler, L.; Li, P.; Li, D.; Geis-Gerstorfer, J.; Rupp, F. Carbon Fiber Reinforced PEEK Composites Based on 3D-Printing Technology for Orthopedic and Dental Applications. J. Clin. Med. 2019, 8, 240. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Zhang, H.; Lan, A.; Yang, S.; Zhang, J.; Wang, H.; Zhou, Z.; Zhou, Y.; Zhao, J.; Jiang, Z. Enhanced bioactivity and osteogenic property of carbon fiber reinforced polyetheretherketone composites modified with amino groups. Colloids Surf. B Biointerfaces 2020, 193, 111098. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Devine, J.N. PEEK biomaterials in trauma, orthopedic, and spinal implants. Biomaterials 2007, 28, 4845–4869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleege, C.; Makowski, M.; Rauschmann, M.; Fraunhoffer, K.L.; Fennema, P.; Arabmotlagh, M.; Rickert, M. Carbon fiber-reinforced pedicle screws reduce artifacts in magnetic resonance imaging of patients with lumbar spondylodesis. Sci. Rep. 2020, 10, 16094. [Google Scholar] [CrossRef] [PubMed]
- Galbusera, F.; Bellini, C.M.; Anasetti, F.; Ciavarro, C.; Lovi, A.; Brayda-Bruno, M. Rigid and flexible spinal stabilization devices: A biomechanical comparison. Med. Eng. Phys. 2011, 33, 490–496. [Google Scholar] [CrossRef]
- Kang, K.-T.; Koh, Y.-G.; Son, J.; Yeom, J.S.; Park, J.-H.; Kim, H.-J. Biomechanical evaluation of pedicle screw fixation system in spinal adjacent levels using polyetheretherketone, carbon-fiber-reinforced polyetheretherketone, and traditional titanium as rod materials. Compos. Part B Eng. 2017, 130, 248–256. [Google Scholar] [CrossRef]
- Rampersaud, Y.R.; Anderson, P.A.; Dimar, J.R., 2nd; Fisher, C.G. Spine Trauma Study Group and Degenerative Spine Study Group. Spinal Adverse Events Severity System, version 2 (SAVES-V2): Inter- and intraobserver reliability assessment. J. Neurosurg. Spine 2016, 25, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Brantigan, J.W.; Steffee, A.D. A carbon fiber implant to aid interbody lumbar fusion: Two-year clinical results in the first 26 patients. Spine 1993, 18, 2106–2117. [Google Scholar] [CrossRef] [PubMed]
- Brantigan, J.W.; Steffee, A.D.; Geiger, J.M. A carbon fiber implant to aid interbody lumbar fusion. Mechanical testing. Spine 1991, 16 (Suppl. S6), S277–S282. [Google Scholar] [CrossRef] [PubMed]
- Disch, A.; Luzzati, A.; Melcher, I.; Schaser, K.; Feraboli, F.; Schmoelz, W. Three-dimensional stiffness in a thoracolumbar en-bloc spondylectomy model: A biomechanical in vitro study. Clin. Biomech. 2007, 22, 957–964. [Google Scholar] [CrossRef]
- Disch, A.C.; Schaser, K.D.; Melcher, I.; Luzzati, A.; Feraboli, F.; Schmoelz, W. En bloc spondylectomy reconstructions in a biomechanical in-vitro study. Eur. Spine J. 2008, 17, 715–725. [Google Scholar] [CrossRef] [Green Version]
- Shen, F.H.; Gasbarrini, A.; Lui, D.F.; Reynolds, J.; Capua, J.; Boriani, S. Integrated Custom Composite Polyetheretherketone/Carbon fiber (PEEK/CF) Vertebral Body Replacement (VBR) in the Treatment of Bone Tumors of the Spine: A Preliminary Report From a Multicenter Study. Spine 2022, 47, 252–260. [Google Scholar] [CrossRef]
- Laux, C.J.; Villefort, C.; Ehrbar, S.; Wilke, L.; Guckenberger, M.; Müller, D.A. Carbon Fiber/Polyether Ether Ketone (CF/PEEK) Implants Allow for More Effective Radiation in Long Bones. Materials 2020, 13, 1754. [Google Scholar] [CrossRef] [Green Version]
- Pipola, V.; Boriani, S.; Ghermandi, R.; Tedesco, G.; Evangelisti, G.; Girolami, M.; Ricci, A.; Gasbarrini, A. Composite peek/carbon fiber pre-shaped rods and sublaminar bands for posterior stabilization of cervico-thoracic junction: A novel technique. J. Clin. Neurosci. 2020, 72, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Mastella, E.; Molinelli, S.; Magro, G.; Mirandola, A.; Russo, S.; Vai, A.; Mairani, A.; Choi, K.; Fiore, M.; Fossati, P.; et al. Dosimetric characterization of carbon fiber stabilization devices for post-operative particle therapy. Phys. Med. 2017, 44, 18–25. [Google Scholar] [CrossRef]
- Lee, C.S.; Hwang, C.J.; Lee, D.-H.; Kim, Y.-T.; Lee, H.S. Fusion Rates of Instrumented Lumbar Spinal Arthrodesis according to Surgical Approach: A Systematic Review of Randomized Trials. Clin. Orthop. Surg. 2011, 3, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, K.; Aizawa, T.; Kanno, H.; Itoi, E. Adjacent segment degeneration after fusion spinal surgery—A systematic review. Int. Orthop. 2018, 43, 987–993. [Google Scholar] [CrossRef]
- Alakhras, J.; Alakhras, T.M. Effect of cold weather on patients with orthopedic implants. J. Taibah Univ. Med. Sci. 2020, 15, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Tecapeek CF30 Black Carbon Filled Peek. Available online: https://Www.Ensingerplastics.Com/En/Shapes/Peek-Tecapeek-Cf30-Black#/Product-Technical-Detail-Collapse-Item-1-Lvl-1 (accessed on 11 June 2023).
- Carbon-Fiber Reinforced Polyetheretherketone (PEEK). Available online: https://polymerdatabase.com/Commercial%20Polymers/PEEK-CF.html (accessed on 11 June 2023).
- Ranu, H.S. The Thermal Properties of Human Cortical Bone: An in Vitro Study. Eng. Med. 1987, 16, 175–176. [Google Scholar] [CrossRef]
- Feldmann, A.; Wili, P.; Maquer, G.; Zysset, P. The thermal conductivity of cortical and cancellous bone. Eur. Cell Mater. 2018, 35, 25–33. [Google Scholar] [CrossRef]
- Fajardo, J.E.; Carlevaro, C.M.; Vericat, F.; Berjano, E.; Irastorza, R.M. Effect of the trabecular bone microstructure on measuring its thermal conductivity: A computer modeling-based study. J. Therm. Biol. 2018, 77, 131–136. [Google Scholar] [CrossRef]
- Calttenburg, R.; Cohen, J.; Conner, S.; Cook, N. Thermal properties of cancellous bone. J. Biomed. Mater. Res. 1975, 9, 169–182. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Sample (Total Number = 28 Patients) | |
|---|---|
| Age, year median (range) | 48 (20–75) |
| Sex, n (%) | |
| Male | 14 (50.0) |
| Female | 14 (50.0) |
| Number of instrumented levels a, n (%) | |
| 1 | 19 (67.9) |
| 2 | 7 (25) |
| 3 | 2 (7.1) |
| Levels instrumented b, n (%) | |
| L2 | 1 (1.5) |
| L3 | 3 (4.5) |
| L4 | 17 (25.4) |
| L5 | 28 (41.8) |
| S1 | 17 (25.4) |
| Total number of instrumented levels | 67 |
| Previous non-instrumented surgery c, n (%) | 6 (21.4) |
| Classification | Description | Number of Cases |
|---|---|---|
| Pseudoarthrosis, collapse of construct, loss of disc height, vertebral slip, broken screw, displacement of the cage, resorption of bone graft | 0 |
| Significant resorption of bone graft, major lucency, or gap visible in the fusion area > 2 mm | 0 |
| A small lucency or gap may be visible with at least half of the graft area showing no lucency between the graft bone and the vertebral bone | 4 |
| Bone bridges the entire fusion area with at least the density originally achieved at surgery. There should be no lucency between the graft bone and the vertebral bone. | 4 |
| The bone in the fusion area is more dense and more mature than originally achieved at surgery; there is no interface between the donor bone and the vertebral bone: a sclerotic line between the graft bone and the vertebral bone indicates solid fusion. Other indicators of solid fusion are fusion at the facet joints and anterior progression of the graft in the disc. | 20 |
| Answer | Number of Patients (%) |
|---|---|
| 20 |
| 6 |
| 1 |
| 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghermandi, R.; Tosini, G.; Lorenzi, A.; Griffoni, C.; La Barbera, L.; Girolami, M.; Pipola, V.; Barbanti Brodano, G.; Bandiera, S.; Terzi, S.; et al. Carbon Fiber-Reinforced PolyEtherEtherKetone (CFR-PEEK) Instrumentation in Degenerative Disease of Lumbar Spine: A Pilot Study. Bioengineering 2023, 10, 872. https://doi.org/10.3390/bioengineering10070872
Ghermandi R, Tosini G, Lorenzi A, Griffoni C, La Barbera L, Girolami M, Pipola V, Barbanti Brodano G, Bandiera S, Terzi S, et al. Carbon Fiber-Reinforced PolyEtherEtherKetone (CFR-PEEK) Instrumentation in Degenerative Disease of Lumbar Spine: A Pilot Study. Bioengineering. 2023; 10(7):872. https://doi.org/10.3390/bioengineering10070872
Chicago/Turabian StyleGhermandi, Riccardo, Giovanni Tosini, Alberto Lorenzi, Cristiana Griffoni, Luigi La Barbera, Marco Girolami, Valerio Pipola, Giovanni Barbanti Brodano, Stefano Bandiera, Silvia Terzi, and et al. 2023. "Carbon Fiber-Reinforced PolyEtherEtherKetone (CFR-PEEK) Instrumentation in Degenerative Disease of Lumbar Spine: A Pilot Study" Bioengineering 10, no. 7: 872. https://doi.org/10.3390/bioengineering10070872