


Infrared Thermography Imaging for Assessment of Peripheral Perfusion in Patients with Septic Shock
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fleischmann-Struzek, C.; Mellhammar, L.; Rose, N.; Cassini, A.; Rudd, K.E.; Schlattmann, P.; Allegranzi, B.; Reinhart, K. Incidence and Mortality of Hospital- and ICU-Treated Sepsis: Results from an Updated and Expanded Systematic Review and Meta-Analysis. Intensive Care Med. 2020, 46, 1552–1562. [Google Scholar] [CrossRef] [PubMed]
- Ince, C. Hemodynamic Coherence and the Rationale for Monitoring the Microcirculation. Crit. Care 2015, 19, S8. [Google Scholar] [CrossRef] [Green Version]
- Ait-Oufella, H.; Bourcier, S.; Lehoux, S.; Guidet, B. Microcirculatory Disorders during Septic Shock. Curr. Opin. Crit. Care 2015, 21, 271–275. [Google Scholar] [CrossRef]
- Hariri, G.; Joffre, J.; Leblanc, G.; Bonsey, M.; Lavillegrand, J.-R.; Urbina, T.; Guidet, B.; Maury, E.; Bakker, J.; Ait-Oufella, H. Narrative Review: Clinical Assessment of Peripheral Tissue Perfusion in Septic Shock. Ann. Intensive Care 2019, 9, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, A.; Jansen, T.C.; van Bommel, J.; Ince, C.; Bakker, J. The Prognostic Value of the Subjective Assessment of Peripheral Perfusion in Critically Ill Patients. Crit. Care Med. 2009, 37, 934–938. [Google Scholar] [CrossRef] [Green Version]
- Alegría, L.; Vera, M.; Dreyse, J.; Castro, R.; Carpio, D.; Henriquez, C.; Gajardo, D.; Bravo, S.; Araneda, F.; Kattan, E.; et al. A Hypoperfusion Context May Aid to Interpret Hyperlactatemia in Sepsis-3 Septic Shock Patients: A Proof-of-Concept Study. Ann. Intensive Care 2017, 7, 29. [Google Scholar] [CrossRef] [Green Version]
- Bourcier, S.; Pichereau, C.; Boelle, P.-Y.; Nemlaghi, S.; Dubée, V.; Lejour, G.; Baudel, J.-L.; Galbois, A.; Lavillegrand, J.-R.; Bigé, N.; et al. Toe-to-Room Temperature Gradient Correlates with Tissue Perfusion and Predicts Outcome in Selected Critically Ill Patients with Severe Infections. Ann. Intensive Care 2016, 6, 63. [Google Scholar] [CrossRef] [Green Version]
- Amson, H.; Vacheron, C.-H.; Thiolliere, F.; Piriou, V.; Magnin, M.; Allaouchiche, B. Core-to-Skin Temperature Gradient Measured by Thermography Predicts Day-8 Mortality in Septic Shock: A Prospective Observational Study. J. Crit. Care 2020, 60, 294–299. [Google Scholar] [CrossRef]
- Ferraris, A.; Bouisse, C.; Mottard, N.; Thiollière, F.; Anselin, S.; Piriou, V.; Allaouchiche, B. Mottling Score and Skin Temperature in Septic Shock: Relation and Impact on Prognosis in ICU. PLoS ONE 2018, 13, e0202329. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Ait-Oufella, H.; Lemoinne, S.; Boelle, P.Y.; Galbois, A.; Baudel, J.L.; Lemant, J.; Joffre, J.; Margetis, D.; Guidet, B.; Maury, E.; et al. Mottling Score Predicts Survival in Septic Shock. Intensive Care Med. 2011, 37, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A Severity of Disease Classification System. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-Related Organ Failure Assessment) Score to Describe Organ Dysfunction/Failure. On Behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.A.S.; Machado-Moreira, C.A.; van den Heuvel, A.M.J.; Caldwell, J.N. Hands and Feet: Physiological Insulators, Radiators and Evaporators. Eur. J. Appl. Physiol. 2014, 114, 2037–2060. [Google Scholar] [CrossRef] [PubMed]
- Schey, B.M.; Williams, D.Y.; Bucknall, T. Skin Temperature and Core-Peripheral Temperature Gradient as Markers of Hemodynamic Status in Critically Ill Patients: A Review. Heart Lung 2010, 39, 27–40. [Google Scholar] [CrossRef]
- Gupta, A.; Puliyel, J.; Garg, B.; Upadhyay, P. Mean Core to Peripheral Temperature Difference and Mean Lactate Levels in First 6 Hours of Hospitalisation as Two Indicators of Prognosis: An Observational Cohort Study. BMC Pediatr. 2020, 20, 515. [Google Scholar] [CrossRef]
- Ring, E.F.J.; Ammer, K. Infrared Thermal Imaging in Medicine. Physiol. Meas. 2012, 33, R33–R46. [Google Scholar] [CrossRef]
- Zaproudina, N.; Varmavuo, V.; Airaksinen, O.; Närhi, M. Reproducibility of Infrared Thermography Measurements in Healthy Individuals. Physiol. Meas. 2008, 29, 515–524. [Google Scholar] [CrossRef]
- Zhu, W.P.; Xin, X.R. Study on the Distribution Pattern of Skin Temperature in Normal Chinese and Detection of the Depth of Early Burn Wound by Infrared Thermography. Ann. N. Y. Acad. Sci. 1999, 888, 300–313. [Google Scholar] [CrossRef]
- Rubinstein, E.H.; Sessler, D.I. Skin-Surface Temperature Gradients Correlate with Fingertip Blood Flow in Humans. Anesthesiology 1990, 73, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Taylor, N.A.S.; Tipton, M.J.; Kenny, G.P. Considerations for the Measurement of Core, Skin and Mean Body Temperatures. J. Therm. Biol. 2014, 46, 72–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ait-Oufella, H.; Bourcier, S.; Alves, M.; Galbois, A.; Baudel, J.-L.; Margetis, D.; Bige, N.; Offenstadt, G.; Maury, E.; Guidet, B. Alteration of Skin Perfusion in Mottling Area during Septic Shock. Ann. Intensive Care 2013, 3, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joly, H.R.; Weil, M.H. Temperature of the Great Toe as an Indication of the Severity of Shock. Circulation 1969, 39, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, G.; Pedreros, C.; Veas, E.; Bruhn, A.; Romero, C.; Rovegno, M.; Neira, R.; Bravo, S.; Castro, R.; Kattan, E.; et al. Evolution of Peripheral vs Metabolic Perfusion Parameters during Septic Shock Resuscitation. A Clinical-Physiologic Study. J. Crit. Care 2012, 27, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moraine, J.J.; van der Linden, P. Toe Temperature versus Transcutaneous Oxygen Tension Monitoring during Acute Circulatory Failure. Intensive Care Med. 1988, 14, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Hirtler, L.; Lübbers, A.; Rath, C. Vascular Coverage of the Anterior Knee Region—An Anatomical Study. J. Anat. 2019, 235, 289–298. [Google Scholar] [CrossRef]
- Westcott, S.; Wung, W.; Schelegle, A.; Ganaga, S.; Schaefer, S. “Cool Knees” as a Measure of Systemic Vascular Resistance in Cardiac Patients. Cureus 2020, 12, e11304. [Google Scholar] [CrossRef]
- Kimura, S.; Butt, W. Core-Peripheral Temperature Gradient and Skin Temperature as Predictors of Major Adverse Events Among Postoperative Pediatric Cardiac Patients. J. Cardiothorac. Vasc. Anesth. 2022, 36, 690–698. [Google Scholar] [CrossRef]
- Saxena, A.; Ng, E.Y.K.; Canchi, T.; Lim, J.L.; Beruvar, A.S. A Method to Produce High Contrast Vein Visualization in Active Dynamic Thermography (ADT). Comput. Biol. Med. 2021, 132, 104309. [Google Scholar] [CrossRef]
- Saxena, A.; Ng, E.Y.K.; Lim, S.T. Active Dynamic Thermography to Detect the Presence of Stenosis in the Carotid Artery. Comput. Biol. Med. 2020, 120, 103718. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Age (years) | 72 (62, 79) |
| Female (n (%)) | 33 (40.7%) |
| APACHE II | 23 (18, 27) |
| SOFA | 9 (7, 12) |
| Mean arterial pressure (mm Hg) | 75.0 (67, 85) |
| Norepinephrine dose (mcg/kg/min) | 0.11 (0.08, 0.17) |
| Serum lactate (mmol/L) | 2.6 (1.9, 4.9) |
| Temperature of the big toe (°C) | 26.4 (23.6, 32.3) |
| Core to knee temperature difference (°C) | 3.3 (2.2, 4.4) |
| Core to toe temperature difference (°C) | 6.2 (2.8, 9.5) |
| 28-day mortality | 22 (27.2%) |
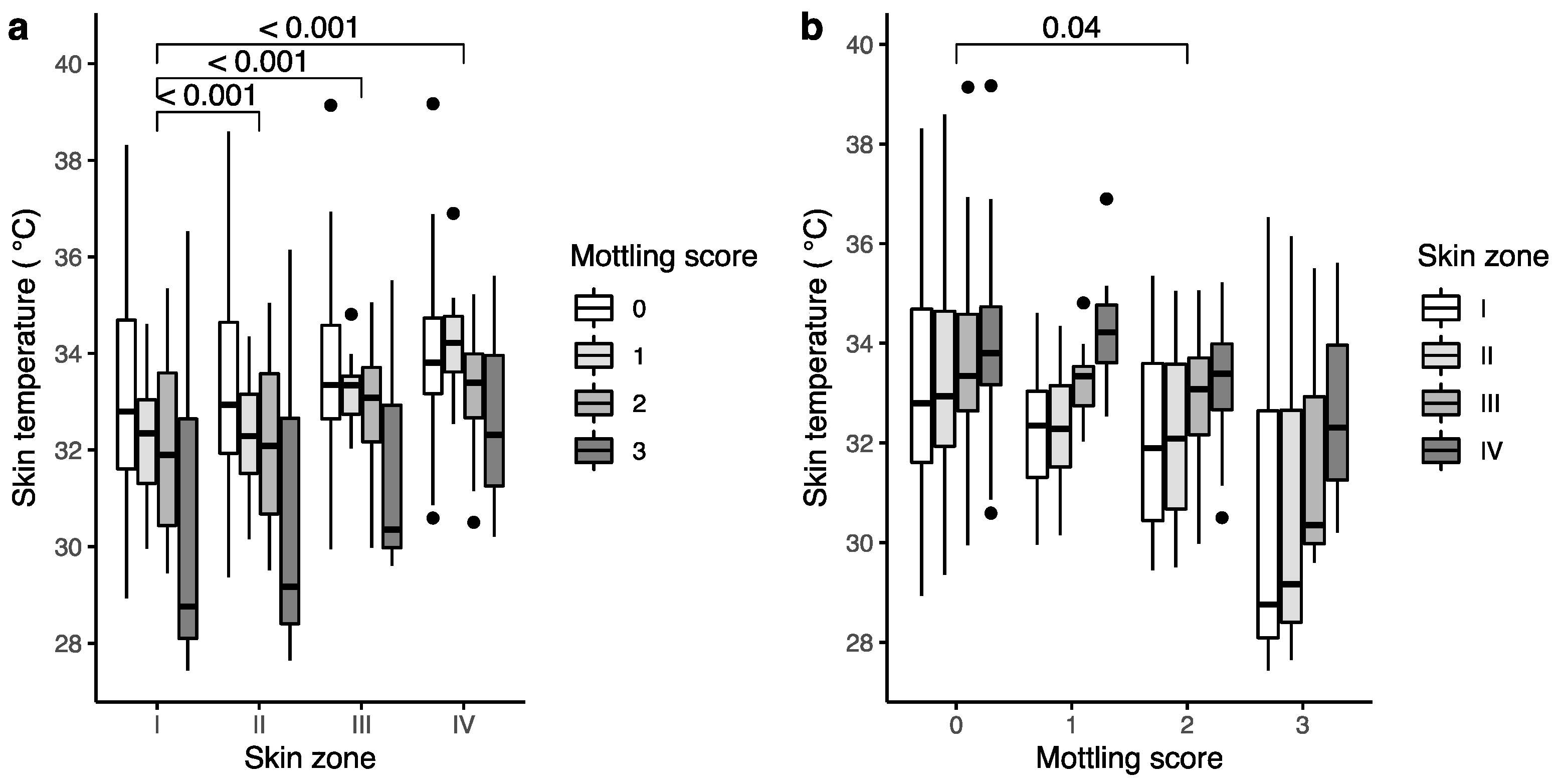
| Estimate | Lower 95% CI | Upper 95% CI | p Value | |
|---|---|---|---|---|
| (Intercept) | 32.99 | 32.47 | 33.52 | >0.001 |
| Skin zone | ||||
| I (ref) | ||||
| II | 0.12 | 0.07 | 0.17 | >0.001 |
| III | 0.64 | 0.42 | 0.87 | >0.001 |
| IV | 1.04 | 0.72 | 1.37 | >0.001 |
| Mottling score | ||||
| 0 (ref) | ||||
| 1 | 0.19 | −0.87 | 1.24 | 0.73 |
| 2 | −0.86 | −1.69 | −0.02 | 0.04 |
| 3 | −1.39 | −3.05 | 0.26 | 0.10 |
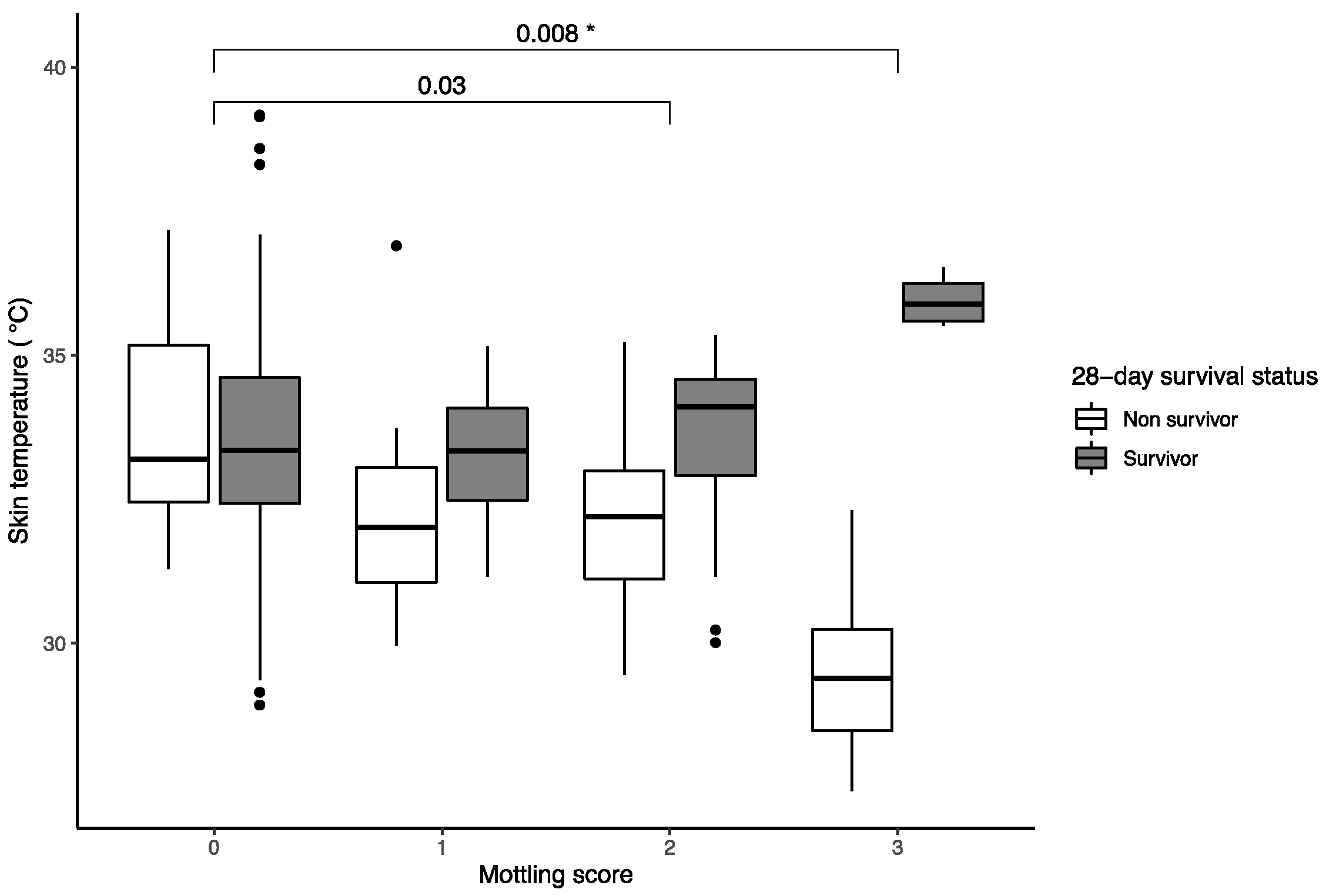
| Estimate | Lower 95% CI | Upper 95% CI | p Value | |
|---|---|---|---|---|
| (Intercept) | 34.77 | 32.58 | 34.53 | >0.001 |
| Survivor | −0.67 | −1.65 | 0.31 | 0.18 |
| Mottling score | ||||
| 0 (ref) | ||||
| 1 | 1.05 | –1.06 | 3.16 | 0.33 |
| 2 | −1.89 | −3.17 | −0.62 | >0.001 |
| 3 | −3.03 | −5.14 | −0.92 | >0.001 |
| Survival status and mottling score interaction | ||||
| Survivor: MS0 (ref) | ||||
| Survivor: MS1 | −1.11 | −3.52 | 1.30 | 0.37 |
| Survivor: MS2 | 1.84 | 0.04 | 3.64 | 0.04 |
| Survivor: MS3 | 4.09 | 0.65 | 7.54 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kazune, S.; Vasiljevs, E.; Caica-Rinca, A.; Marcinkevics, Z.; Grabovskis, A. Infrared Thermography Imaging for Assessment of Peripheral Perfusion in Patients with Septic Shock. Bioengineering 2023, 10, 729. https://doi.org/10.3390/bioengineering10060729
Kazune S, Vasiljevs E, Caica-Rinca A, Marcinkevics Z, Grabovskis A. Infrared Thermography Imaging for Assessment of Peripheral Perfusion in Patients with Septic Shock. Bioengineering. 2023; 10(6):729. https://doi.org/10.3390/bioengineering10060729
Chicago/Turabian StyleKazune, Sigita, Edgars Vasiljevs, Anastasija Caica-Rinca, Zbignevs Marcinkevics, and Andris Grabovskis. 2023. "Infrared Thermography Imaging for Assessment of Peripheral Perfusion in Patients with Septic Shock" Bioengineering 10, no. 6: 729. https://doi.org/10.3390/bioengineering10060729