

OculusGraphy: Signal Analysis of the Electroretinogram in a Rabbit Model of Endophthalmitis Using Discrete and Continuous Wavelet Transforms
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
1.1. Electroretinogram
1.2. Analysis of the Electroretinogram Waveform
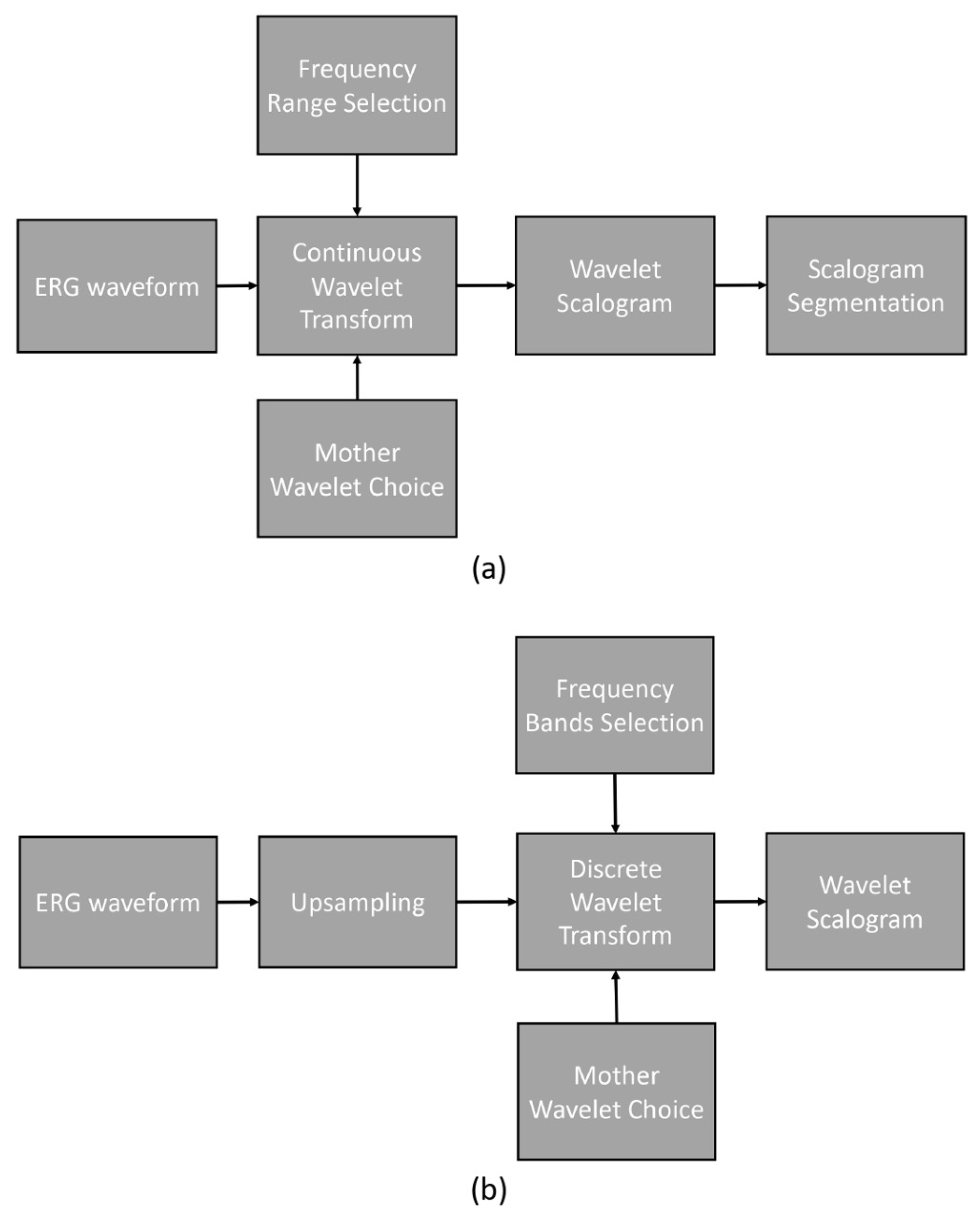
2. Materials and Methods
2.1. Study Protocol and Signals
- 1.
- Daubechies wavelet;
- 2.
- Ricker wavelet;
- 3.
- Wavelet Biorthogonal 3.1 (bior3.1);
- 4.
- Morlet wavelet;
- 5.
- Haar wavelet;
- 6.
- Gaussian wavelet.
2.2. Endophthalmitis Treatment in Rabbit
3. Results
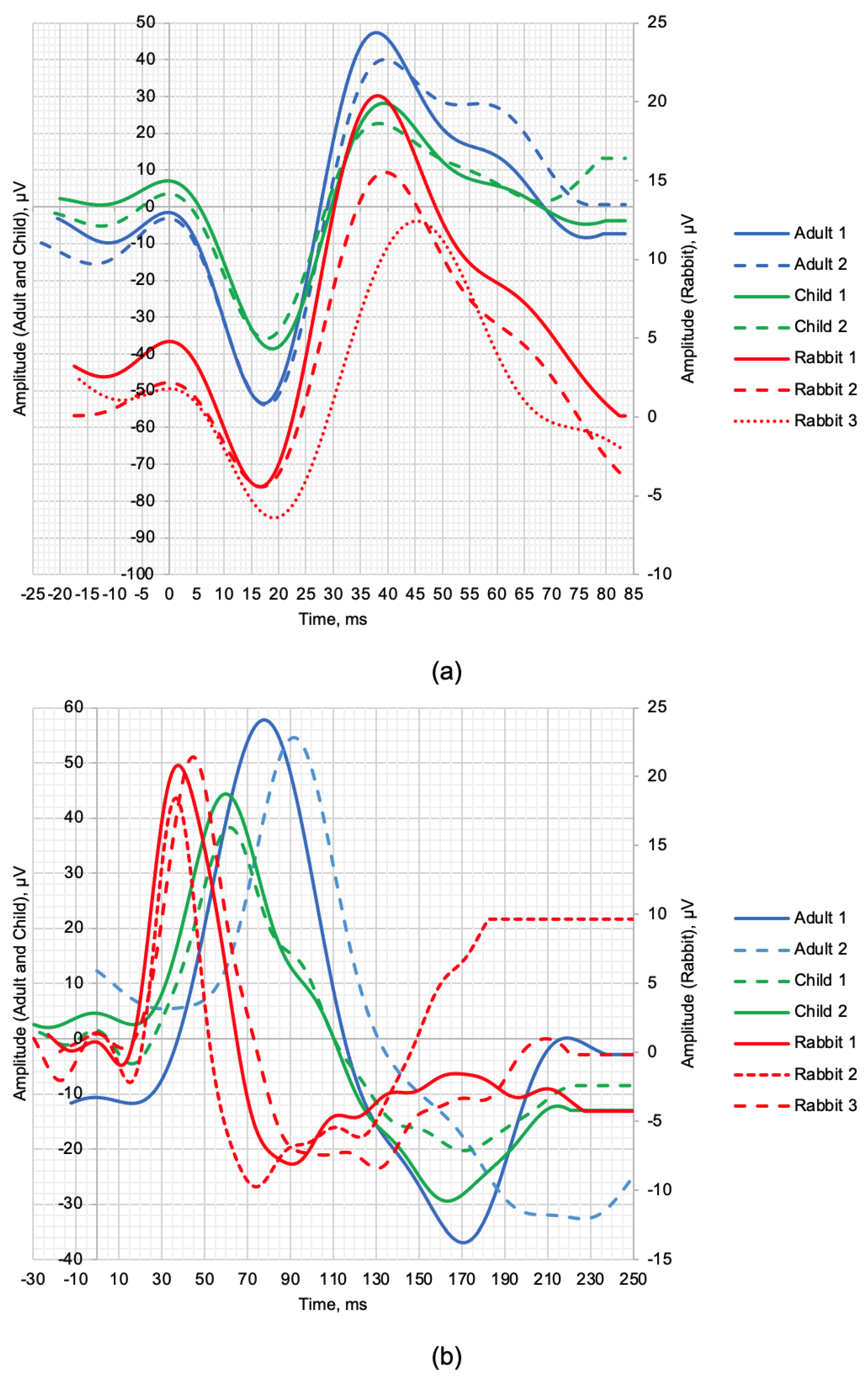
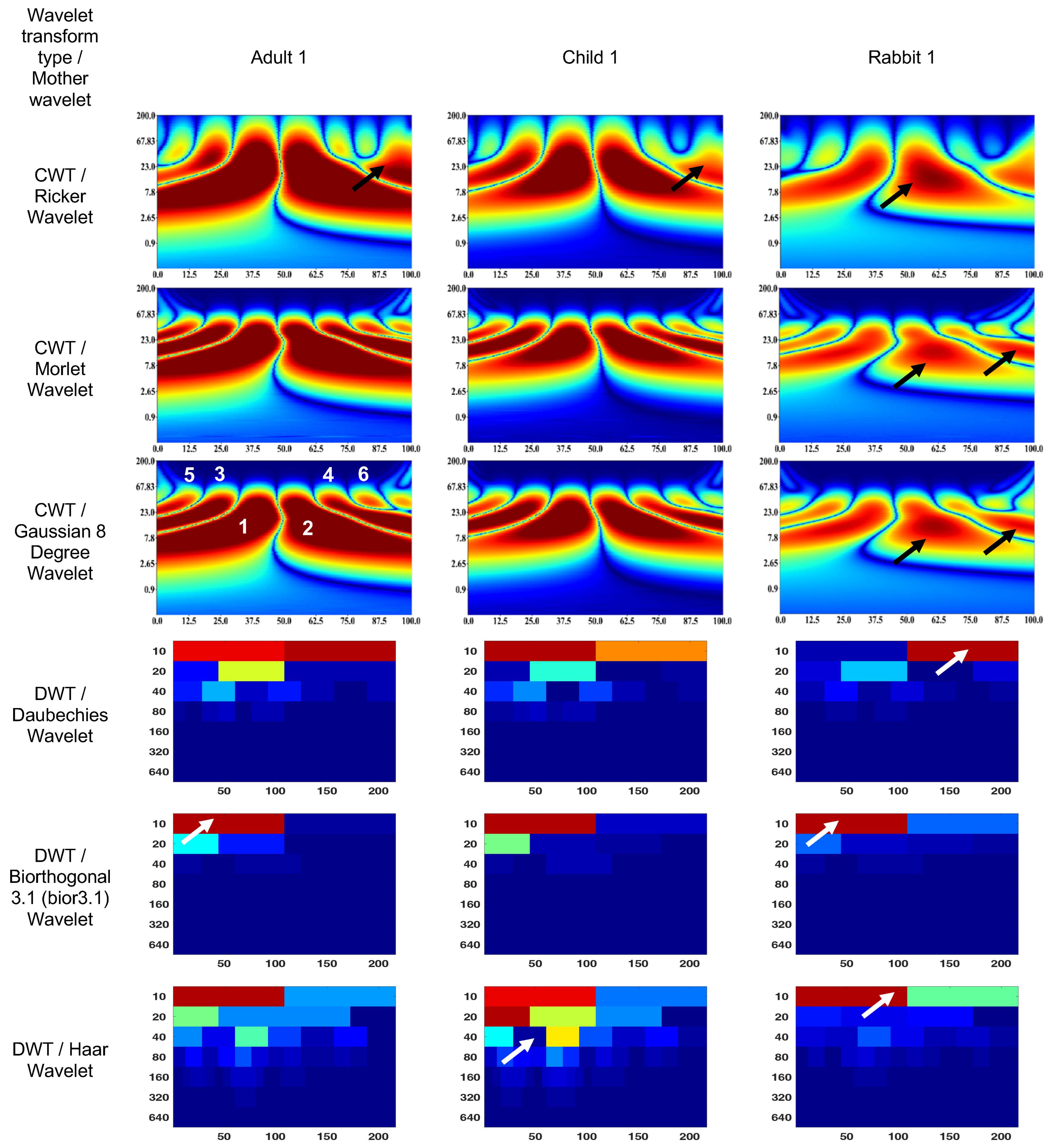
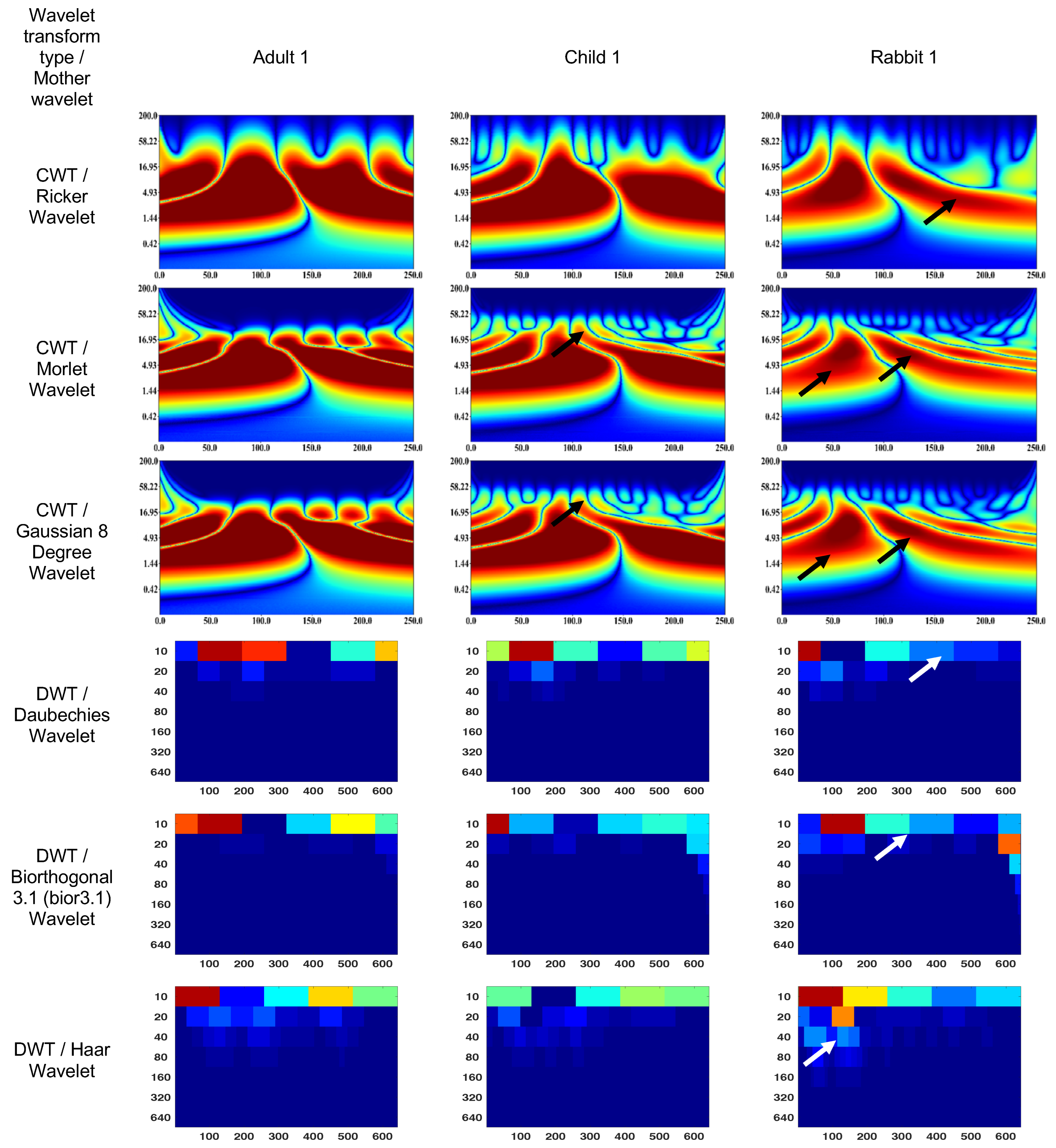
3.1. Wavelet Scalograms of Human and Rabbit ERGs
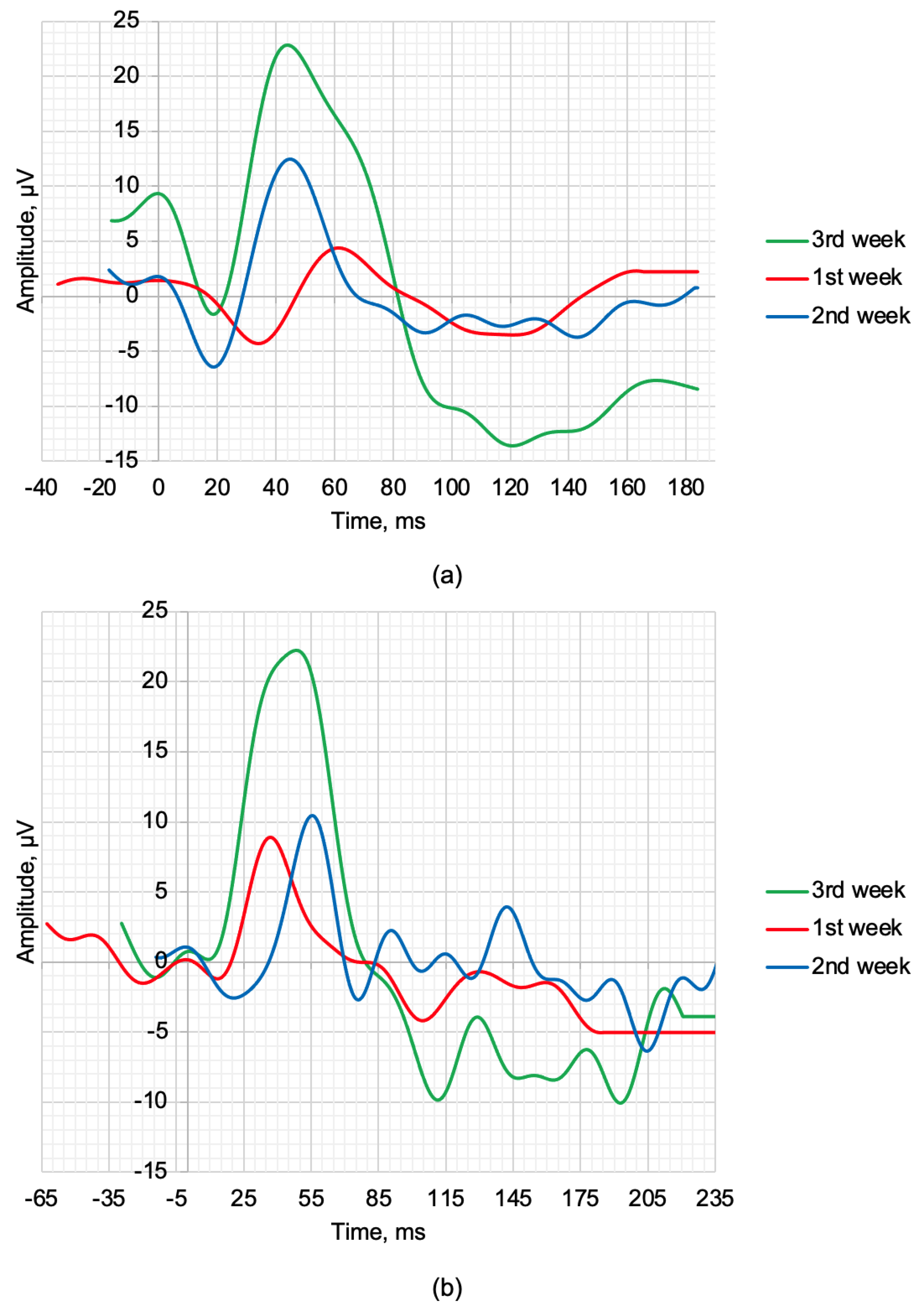
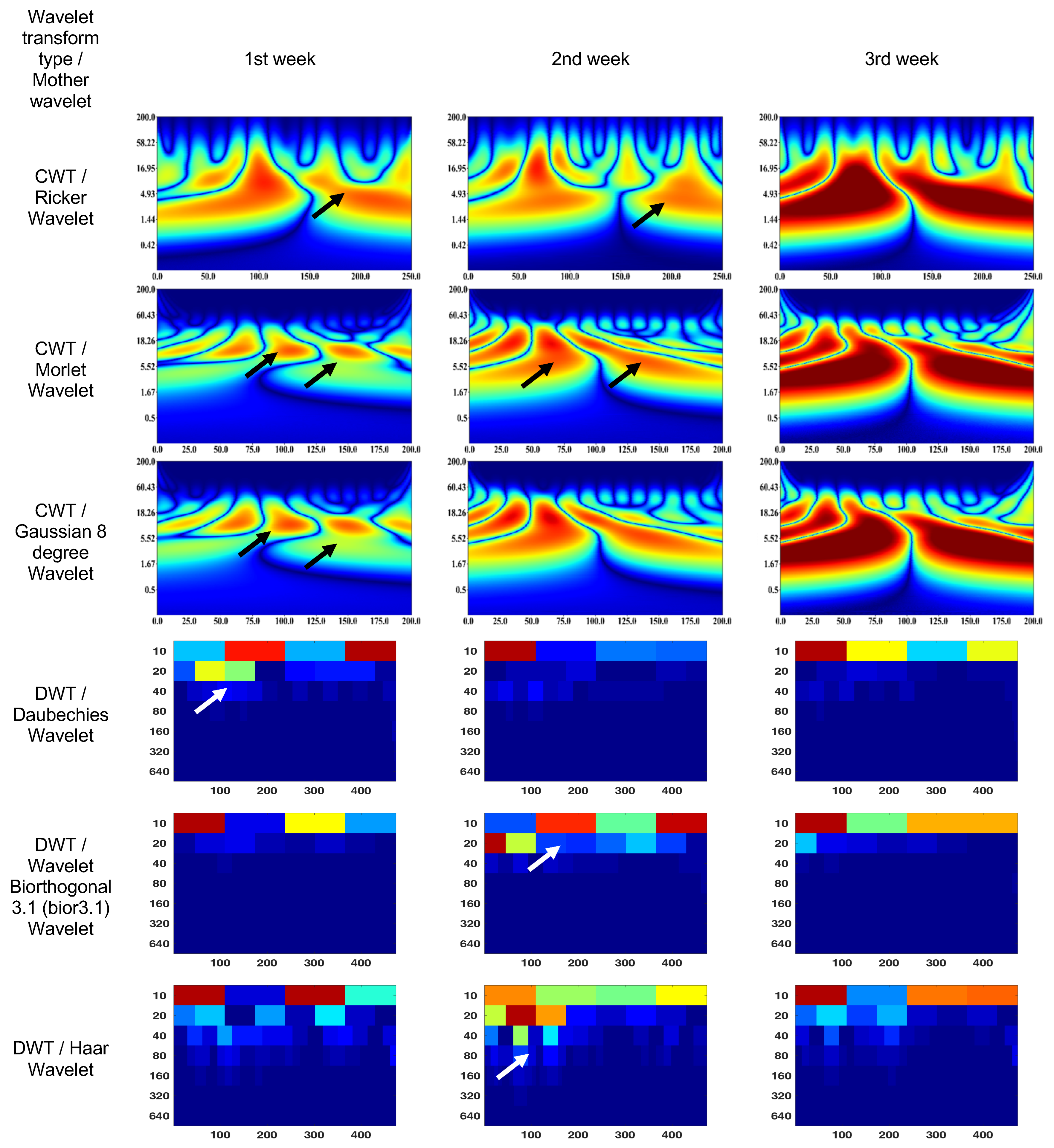
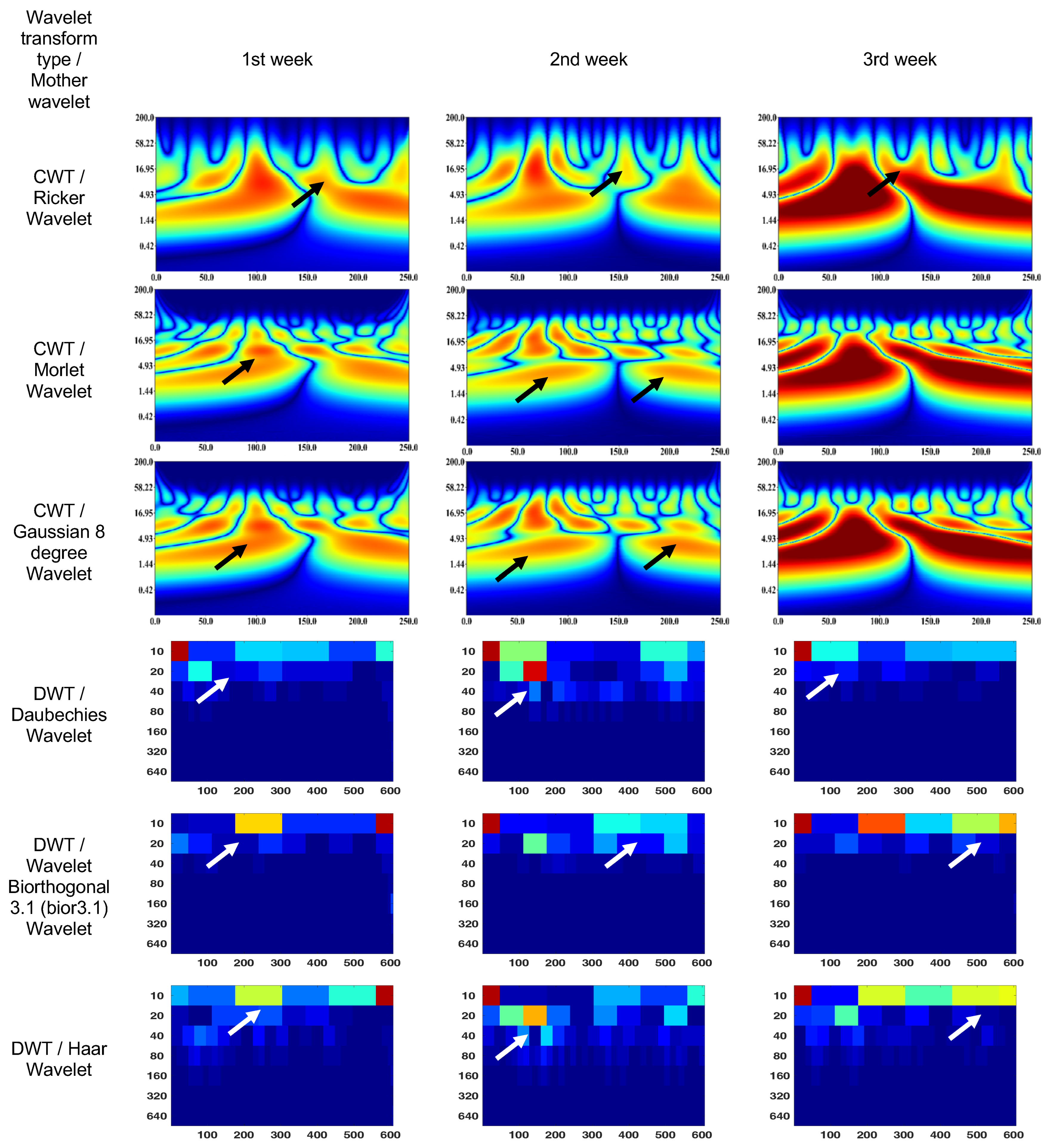
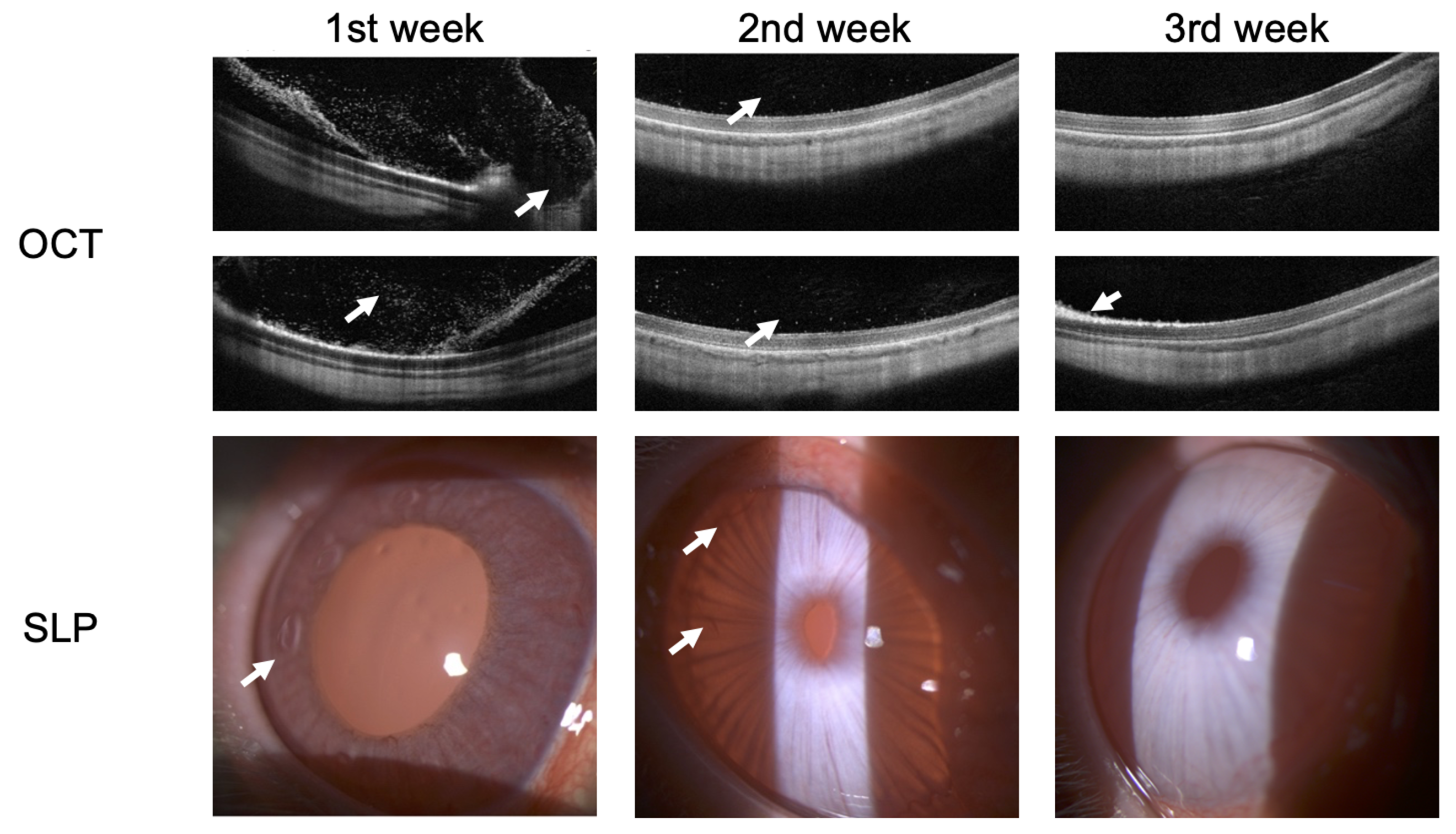
3.2. Endophthalmitis Treatment in Rabbit
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LA | Light Adapted |
| OPs | Oscillatory Potentials |
| DWT | Discrete Wavelet Transform |
| CWT | Continuous Wavelet Transform |
| SLP | Slit-lamp Photography |
| OCT | Optical Coherence Tomography |
References
- Robson, A.G.; Frishman, L.J.; Grigg, J.; Hamilton, R.; Jeffrey, B.G.; Kondo, M.; Li, S.; McCulloch, D.L. ISCEV Standard for full-field clinical electroretinography (2022 update). Doc. Ophthalmol. 2022, 144, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Robson, A.G.; Nilsson, J.; Li, S.; Jalali, S.; Fulton, A.B.; Tormene, A.P.; Holder, G.E.; Brodie, S.E. ISCEV guide to visual electrodiagnostic procedures. Doc. Ophthalmol. 2018, 136, 1–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granit, R. Physiology of Vision. Annu. Rev. Physiol. 1950, 12, 485–502. [Google Scholar] [CrossRef] [PubMed]
- Baylor, D.A.; Lamb, T.D.; Yau, K.W. The membrane current of single rod outer segments. J. Physiol. 1979, 288, 589–611. [Google Scholar] [CrossRef]
- Robson, J.G.; Saszik, S.M.; Ahmed, J.; Frishman, L.J. Rod and cone contributions to the a-wave of the electroretinogram of the macaque. J. Physiol. 2003, 547, 509–530. [Google Scholar] [CrossRef]
- Robson, J.G.; Frishman, L.J. The rod-driven a-wave of the dark-adapted mammalian electroretinogram. Prog. Retin. Eye Res. 2014, 39, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Knapp, A.G.; Schiller, P.H. The contribution of on-bipolar cells to the electroretinogram of rabbits and monkeys. A study using 2-amino-4-phosphonobutyrate (APB). Vis. Res. 1984, 24, 1841–1846. [Google Scholar] [CrossRef]
- Heynen, H.; van Norren, D. Origin of the electroretinogram in the intact macaque eye–II. Current source-density analysis. Vis. Res. 1985, 25, 709–715. [Google Scholar] [CrossRef]
- Thompson, D.A.; Feather, S.; Stanescu, H.C.; Freudenthal, B.; Zdebik, A.A.; Warth, R.; Ognjanovic, M.; Hulton, S.A.; Wassmer, E.; van′t Hoff, W.; et al. Altered electroretinograms in patients with KCNJ10 mutations and EAST syndrome. J. Physiol. 2011, 589, 1681–1689. [Google Scholar] [CrossRef]
- Diamond, J.S. Inhibitory Interneurons in the Retina: Types, Circuitry, and Function. Annu. Rev. Vis. Sci. 2017, 3, 1–24. [Google Scholar] [CrossRef]
- Barnes, S.; Grove, J.C.R.; McHugh, C.F.; Hirano, A.A.; Brecha, N.C. Horizontal Cell Feedback to Cone Photoreceptors in Mammalian Retina: Novel Insights From the GABA-pH Hybrid Model. Front. Cell. Neurosci. 2020, 14, 595064. [Google Scholar] [CrossRef]
- Bush, R.A.; Sieving, P.A. A proximal retinal component in the primate photopic ERG a-wave. Investig. Ophthalmol. Vis. Sci. 1994, 35, 635–645. [Google Scholar]
- Gouras, P.; MacKay, C. A new component in the a-wave of the human cone electroretinogram. Doc. Ophthalmol. 2000, 101, 19–24. [Google Scholar] [CrossRef]
- Dang, T.M.; Tsai, T.I.; Vingrys, A.J.; Bui, B.V. Post-receptoral contributions to the rat scotopic electroretinogram a-wave. Doc. Ophthalmol. 2011, 122, 149–156. [Google Scholar] [CrossRef]
- Hirano, A.A.; Vuong, H.E.; Kornmann, H.L.; Schietroma, C.; Stella, S.L., Jr.; Barnes, S.; Brecha, N.C. Vesicular Release of GABA by Mammalian Horizontal Cells Mediates Inhibitory Output to Photoreceptors. Front. Cell. Neurosci. 2020, 14, 600777. [Google Scholar] [CrossRef]
- Viswanathan, S.; Frishman, L.J.; Robson, J.G.; Walters, J.W. The photopic negative response of the flash electroretinogram in primary open angle glaucoma. Investig. Ophthalmol. Vis. Sci. 2001, 42, 514–522. [Google Scholar]
- Wachtmeister, L.; Dowling, J.E. The oscillatory potentials of the mudpuppy retina. Investig. Ophthalmol. Vis. Sci. 1978, 17, 1176–1188. [Google Scholar]
- Wachtmeister, L. Further studies of the chemical sensitivity of the oscillatory potentials of the electroretinogram (ERG) I. GABA- and glycine antagonists. Acta Ophthalmol. 1980, 58, 712–725. [Google Scholar] [CrossRef]
- Wachtmeister, L. Further studies of the chemical sensitivity of the oscillatory potentials of the electroretinogram (ERG). II. Glutamate-aspartate-and dopamine antagonists. Acta Ophthalmol. 1981, 59, 247–258. [Google Scholar] [CrossRef]
- Wachtmeister, L. Oscillatory potentials in the retina: What do they reveal. Prog. Retin. Eye Res. 1998, 17, 485–521. [Google Scholar] [CrossRef]
- Dong, C.J.; Agey, P.; Hare, W.A. Origins of the electroretinogram oscillatory potentials in the rabbit retina. Vis. Neurosci. 2004, 21, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Myers, A.C.; Bruun, A.; Ghosh, F.; Adrian, M.L.; Andreasson, S.; Ponjavic, V. Intravitreal injection of triamcinolone acetonide into healthy rabbit eyes alters retinal function and morphology. Curr. Eye Res. 2013, 38, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Pochop, P.; Darsova, D.; Uhlik, J.; Lestak, J.; Kukaka, J.; Kodetova, D.; Klapkova, E.; Malis, J.; Vajner, L. Retinal toxicity after repeated intravitreal carboplatin injection into rabbit eyes. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2014, 158, 552–556. [Google Scholar] [CrossRef]
- Smith, N.P.; Lamb, T.D. The a-wave of the human electroretinogram recorded with a minimally invasive technique. Vis. Res. 1997, 37, 2943–2952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedburg, C.; Allen, C.P.; Mason, P.J.; Lamb, T.D. Contribution of cone photoreceptors and post-receptor mechanisms to the human photopic electroretinogram. J. Physiol. 2004, 556, 819–834. [Google Scholar] [CrossRef]
- Mahroo, O.A.; Ban, V.S.; Bussmann, B.M.; Copley, H.C.; Hammond, C.J.; Lamb, T.D. Modeling the initial phase of the human rod photoreceptor response to the onset of steady illumination. Doc. Ophthalmol. 2012, 124, 125–131. [Google Scholar] [CrossRef]
- Forte, J.D.; Bui, B.V.; Vingrys, A.J. Wavelet analysis reveals dynamics of rat oscillatory potentials. J. Neurosci. Methods 2008, 169, 191–200. [Google Scholar] [CrossRef]
- Gauvin, M.; Dorfman, A.L.; Trang, N.; Gauthier, M.; Little, J.M.; Lina, J.M.; Lachapelle, P. Assessing the Contribution of the Oscillatory Potentials to the Genesis of the Photopic ERG with the Discrete Wavelet Transform. BioMed Res. Int. 2016, 2016, 2790194. [Google Scholar] [CrossRef] [Green Version]
- Rufiange, M.; Dassa, J.; Dembinska, O.; Koenekoop, R.K.; Little, J.M.; Polomeno, R.C.; Dumont, M.; Chemtob, S.; Lachapelle, P. The photopic ERG luminance-response function (photopic hill): Method of analysis and clinical application. Vis. Res. 2003, 43, 1405–1412. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, R.; Bees, M.A.; Chaplin, C.A.; McCulloch, D.L. The luminance-response function of the human photopic electroretinogram: A mathematical model. Vis. Res. 2007, 47, 2968–2972. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.A.; Jeffrey, B.G.; Messias, A.M.V.; Robson, A.G. ISCEV extended protocol for the stimulus–response series for the dark-adapted full-field ERG b-wave. Doc. Ophthalmol. 2019, 138, 217–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garon, M.L.; Dorfman, A.L.; Racine, J.; Koenekoop, R.K.; Little, J.M.; Lachapelle, P. Estimating ON and OFF contributions to the photopic hill: Normative data and clinical applications. Doc. Ophthalmol. 2014, 129, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Constable, P.A.; Gaigg, S.B.; Bowler, D.M.; Jagle, H.; Thompson, D.A. Full-field electroretinogram in autism spectrum disorder. Doc. Ophthalmol. 2016, 132, 83–99. [Google Scholar] [CrossRef]
- Constable, P.A.; Marmolejo-Ramos, F.; Gauthier, M.; Lee, I.O.; Skuse, D.H.; Thompson, D.A. Discrete Wavelet Transform Analysis of the Electroretinogram in Autism Spectrum Disorder and Attention Deficit Hyperactivity Disorder. Front. Neurosci. 2022, 16, 890461. [Google Scholar] [CrossRef]
- Gauvin, M.; Sustar, M.; Little, J.M.; Brecelj, J.; Lina, J.M.; Lachapelle, P. Quantifying the ON and OFF Contributions to the Flash ERG with the Discrete Wavelet Transform. Transl. Vis. Sci. Technol. 2017, 6, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penkala, K.; Jaskuła, M.; Lubiński, W. Improvement of the PERG parameters measurement accuracy in the continuous wavelet transform coefficients domain. Ann. Acad. Med. Stetin. 2007, 53, 58–60. [Google Scholar]
- Penkala, K. Analysis of bioelectrical signals of the human retina (PERG) and visual cortex (PVEP) evoked by pattern stimuli. Bull. Pol. Acad. Sci. Tech. Sci. 2005, 53, 223–229. [Google Scholar]
- Ahmadieh, H.; Behbahani, S.; Safi, S. Continuous wavelet transform analysis of ERG in patients with diabetic retinopathy. Doc. Ophthalmol. 2021, 142, 305–314. [Google Scholar] [CrossRef]
- Barraco, R.; Persano Adorno, D.; Brai, M. Wavelet analysis of human photoreceptoral response. In Proceedings of the 2010 3rd International Symposium on Applied Sciences in Biomedical and Communication Technologies (ISABEL 2010), Rome, Italy, 7–10 November 2010. [Google Scholar]
- Barraco, R.; Persano Adorno, D.; Brai, M. An approach based on wavelet analysis for feature extraction in the a-wave of the electroretinogram. Comput. Methods Programs Biomed. 2011, 104, 316–324. [Google Scholar] [CrossRef]
- Barraco, R.; Persano Adorno, D.; Brai, M. ERG signal analysis using wavelet transform. Theory Biosci. 2011, 130, 155–163. [Google Scholar] [CrossRef]
- Gauvin, M.; Lina, J.M.; Lachapelle, P. Advance in ERG analysis: From peak time and amplitude to frequency, power, and energy. BioMed Res. Int. 2014, 2014, 246096. [Google Scholar] [CrossRef] [Green Version]
- Dimopoulos, I.S.; Freund, P.R.; Redel, T.; Dornstauder, B.; Gilmour, G.; Sauvé, Y. Changes in rod and cone-driven oscillatory potentials in the aging human retina. Investig. Ophthalmol. Vis. Sci. 2014, 55, 5058–5073. [Google Scholar] [CrossRef] [Green Version]
- Miguel-Jiménez, J.M.; Blanco, R.; De-Santiago, L.; Fernández, A.; Rodríguez-Ascariz, J.M.; Barea, R.; Martín-Sánchez, J.L.; Amo, C.; Sánchez-Morla, E.; Boquete, L. Continuous-wavelet-transform analysis of the multifocal ERG waveform in glaucoma diagnosis. Med. Biol. Eng. Comput. 2015, 53, 771–780. [Google Scholar] [CrossRef]
- Brandao, L.M.; Monhart, M.; Schötzau, A.; Ledolter, A.A.; Palmowski-Wolfe, A.M. Wavelet decomposition analysis in the two-flash multifocal ERG in early glaucoma: A comparison to ganglion cell analysis and visual field. Doc. Ophthalmol. 2017, 135, 29–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassankarimi, H.; Noori, S.M.R.; Jafarzadehpour, E.; Yazdani, S.; Radinmehr, F. Analysis of pattern electroretinogram signals of early primary open-angle glaucoma in discrete wavelet transform coefficients domain. Int. Ophthalmol. 2019, 39, 2373–2383. [Google Scholar] [CrossRef] [PubMed]
- Zhdanov, A.; Dolganov, A.; Zanca, D.; Borisov, V.; Ronkin, M. Advanced Analysis of Electroretinograms Based on Wavelet Scalogram Processing. Appl. Sci. 2022, 12, 12365. [Google Scholar] [CrossRef]
- Sarossy, M.; Crowston, J.; Kumar, D.; Weymouth, A.; Wu, Z. Time–Frequency Analysis of ERG With Discrete Wavelet Transform and Matching Pursuits for Glaucoma. Transl. Vis. Sci. Technol. 2022, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Gauvin, M.; Little, J.M.; Lina, J.M.; Lachapelle, P. Functional decomposition of the human ERG based on the discrete wavelet transform. J. Vis. 2015, 15, 14. [Google Scholar] [CrossRef]
- Dorfman, A.L.; Gauvin, M.; Vatcher, D.; Little, J.M.; Polomeno, R.C.; Lachapelle, P. Ring analysis of multifocal oscillatory potentials (mfOPs) in cCSNB suggests near-normal ON-OFF pathways at the fovea only. Doc. Ophthalmol. 2020, 141, 99–109. [Google Scholar] [CrossRef]
- Mohammad-Manjur, S.; Hossain, M.-B.; Constable, P.A.; Thompson, D.A.; Marmolejo-Ramos, F.; Lee, I.O.; Skuse, D.H.; Posada-Quintero, H.F. Detecting Autism Spectrum Disorder Using Spectral Analysis of Electroretinogram and Machine Learning: Preliminary results. IEEE Trans. Biomed. Eng. 2022, 2022, 3435–3438. [Google Scholar]
- Hamilton, R. Clinical electrophysiology of vision-commentary on current status and future prospects. Eye 2021, 35, 2341–2343. [Google Scholar] [CrossRef]
- Mahroo, O.A. Visual electrophysiology and “the potential of the potentials”. Eye 2023, 1–10. [Google Scholar] [CrossRef]
- Dhyani, S.; Kumar, A.; Choudhury, S. Analysis of ECG-based arrhythmia detection system using machine learning. MethodsX 2023, 10, 102195. [Google Scholar] [CrossRef]
- Ji, N.; Ma, L.; Dong, H.; Zhang, X. EEG signals feature extraction based on DWT and EMD combined with approximate entropy. Brain Sci. 2019, 9, 201. [Google Scholar] [CrossRef] [Green Version]
- Zarei, A.; Asl, B.M. Automatic seizure detection using orthogonal matching pursuit, discrete wavelet transform, and entropy based features of EEG signals. Comput. Biol. Med. 2021, 131, 104250. [Google Scholar] [CrossRef]
- Yip, Y.W.Y.; Man, T.C.; Pang, C.P.; Brelen, M.E. Improving the quality of electroretinogram recordings using active electrodes. Exp. Eye Res. 2018, 176, 46–52. [Google Scholar] [CrossRef]
- Zhdanov, A.E.; Dolganov, A.Y.; Zanca, D.; Borisov, V.I.; Lucian, E.; Dorosinskiy, L.G. Evaluation of the effectiveness of the decision support algorithm for physicians in retinal dystrophy using machine learning methods. Comput. Opt. 2023, 47, 272–277. [Google Scholar] [CrossRef]
- Behbahani, S.; Ahmadieh, H.; Rajan, S. Feature Extraction Methods for Electroretinogram Signal Analysis: A Review. IEEE Access 2021, 9, 116879–116897. [Google Scholar] [CrossRef]
- Ponomarev, V.O.; Kazaykin, V.N.; Lizunov, A.V.; Vokhmintsev, A.S.; Vainshtein, I.A.; Dezhurov, S.V.; Marysheva, V.V. Evaluation of the Ophthalmotoxic Effect of Quantum Dots InP/ZnSe/ZnS 660 and Bioconjugates Based on Them in Terms of the Prospects for the Treatment of Resistant Endophthalmitis. experimental research. Part 2 (Stage 1). Ophthalmol. Russ. 2021, 18, 876–884. [Google Scholar] [CrossRef]
- Kondo, M.I.N.E.O. Animal models of human retinal and optic nerve diseases analyzed using electroretinography. Nippon Ganka Gakkai Zasshi 2010, 114, 248–278. [Google Scholar]
- Ciulla, T.A.; Criswell, M.H.; Danis, R.P.; Hill, T.E.; Introne, W.J. Endothelin-1-mediated retinal artery vasospasm and the rabbit electroretinogram. J. Ocul. Pharmacol. Ther. 2000, 16, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, J.; Majzoub, M.E.; Coroneo, M.; Thomas, T.; Willcox, M. Comparative analysis of ocular surface tissue microbiome in human, mouse, rabbit, and guinea pig. Exp. Eye Res. 2021, 207, 108609. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Pi, Y.L.; Zhang, M.N. The effect of Vaccinium uliginosum on rabbit retinal structure and light-induced function damage. Chin. J. Integr. Med. 2012, 18, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Famiglietti, E.V.; Sharpe, S.J. Regional topography of rod and immunocytochemically characterized “blue” and “green” cone photoreceptors in rabbit retina. Vis. Neurosci. 1995, 12, 1151–1175. [Google Scholar] [CrossRef]
- Williams, D.L. The rabbit eye. In Ophthalmology of Exotic Pets; Cooper, J.E., Thomas, M.R.L., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2012; pp. 15–55. [Google Scholar]
- Horio, N.; Terasaki, H.; Yamamoto, E.; Miyake, Y. Electroretinogram in the diagnosis of endophthalmitis after intraocular lens implantation. Am. J. Ophthalmol. 2001, 132, 258–259. [Google Scholar] [CrossRef]
- Kim, I.T.; Chung, K.H.; Koo, B.S. Efficacy of ciprofloxacin and dexamethasone in experimental pseudomonas endophthalmitis. Korean J. Ophthalmol. 1996, 10, 8–17. [Google Scholar] [CrossRef]
- Callegan, M.C.; Booth, M.C.; Jett, B.D.; Gilmore, M.S. Pathogenesis of gram-positive bacterial endophthalmitis. Infect. Immun. 1999, 67, 3348–3356. [Google Scholar] [CrossRef] [Green Version]
- Shahar, J.; Zemel, E.; Perlman, I.; Loewenstein, A. Physiological and toxicological effects of cefuroxime on the albino rabbit retina. Investig. Ophthalmol. Vis. Sci. 2012, 53, 906–914. [Google Scholar] [CrossRef]
- Cardoso, J.F.; Perasoli, F.B.; Almeida, T.C.; Marques, M.B.F.; Toledo, C.R.; Gil, P.O.; Tavares, H.D.S.; Da Paz, M.C.; Mussel, W.D.N.; Magalhães, J.T.; et al. Vancomycin-loaded N, N-dodecyl, methyl-polyethylenimine nanoparticles coated with hyaluronic acid to treat bacterial endophthalmitis: Development, characterization, and ocular biocompatibility. Int. J. Biol. Macromol. 2021, 169, 330–341. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Author | Transform Type (Mother Wavelet) | Signals (Subjects) |
|---|---|---|---|
| 2005 | Penkala [37] | CWT (Morlet, Ricker) | 120 (N/A) |
| 2007 | Penkala [36] | 102 (N/A) | |
| 2010 | Barraco [39] | CWT (Ricker) | 24 (N/A) |
| 2011 | Barraco [40] | N/A (10) | |
| 2011 | Barraco [41] | N/A (10) | |
| 2014 | Gauvin [42] | CWT (Morse), DWT (Haar) | N/A (40) |
| 2014 | Dimopoulos [43] | CWT (Morlet) | N/A (63) |
| 2015 | Miguel-Jiménez [44] | N/A (47) | |
| 2017 | Brandao [45] | DWT (Daubechies) | 60 (60) |
| 2019 | Hassankarimi [46] | DWT (Daubechies) | 60 (N/A) |
| 2020 | Ahmadieh [38] | CWT (Morlet) | N/A (36) |
| 2022 | Zhdanov [47] | CWT (Gaussian) | 425 (N/A) |
| 2022 | Sarossy [48] | DWT (Fejer–Korovkin) | 103 (55) |
| Scotopic 2.0 ERG Response | Maximum 2.0 ERG Response | |
|---|---|---|
| Flash intensity, cd·s·m | 2 | 2 |
| Background light, cd·s·m | 0 | 0 |
| Flash duration, ms | 0.5 | 3 |
| Flash frequency, kHz | 20 | 20 |
| Stimulus interval, s (cps) | 2.5 (0.4) | 10 or 13 (0.1) |
| Flash color | white | white |
| Adult 1 | Adult 2 | Child 1 | Child 2 | Rabbit 1 | Rabbit 2 | Rabbit 3 | |
|---|---|---|---|---|---|---|---|
| Age | 20.5 y.o. | 27.8 y.o. | 10.9 y.o. | 7.5 y.o. | 2–3.5 mos. | ||
| Maximum 2.0 ERG Response | |||||||
| a, µV | 52.32 | 50.69 | 45.65 | 39.28 | 9.18 | 6.59 | 8.2 |
| b, µV | 101.22 | 93.78 | 66.74 | 58.35 | 24.75 | 19.92 | 18.86 |
| la, ms | 17.5 | 18 | 19 | 18 | 16.5 | 17 | 19.5 |
| lb, ms | 38 | 39.5 | 39.5 | 38.5 | 38 | 39.5 | 45.5 |
| Scotopic 2.0 ERG Response | |||||||
| a, µV | 1.04 | - | 6.05 | 2.03 | 1.82 | 3.47 | 1.04 |
| b, µV | 69.53 | 60.01 | 42.77 | 46.91 | 21.87 | 20.47 | 21.12 |
| la, ms | 17 | - | 16 | 16.5 | 10.5 | 14.5 | 12.5 |
| lb, ms | 78 | 92.5 | 62.5 | 60.5 | 38.5 | 37.5 | 44.5 |
| 1st Week | 2nd Week | 3rd Week | |
|---|---|---|---|
| Maximum 2.0 ERG Response | |||
| a, µV | 5.61 | 8.03 | 10.81 |
| b, µV | 16.48 | 18.6 | 24.14 |
| la, ms | 33 | 17.5 | 20 |
| lb, ms | 47 | 46.5 | 43 |
| Scotopic 2.0 ERG Response | |||
| a, µV | 1.81 | 3.43 | 0.75 |
| b, µV | 10.26 | 12.72 | 21.92 |
| la, ms | 13 | 22.5 | 8.5 |
| lb, ms | 39.5 | 57.5 | 50.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhdanov, A.; Constable, P.; Manjur, S.M.; Dolganov, A.; Posada-Quintero, H.F.; Lizunov, A. OculusGraphy: Signal Analysis of the Electroretinogram in a Rabbit Model of Endophthalmitis Using Discrete and Continuous Wavelet Transforms. Bioengineering 2023, 10, 708. https://doi.org/10.3390/bioengineering10060708
Zhdanov A, Constable P, Manjur SM, Dolganov A, Posada-Quintero HF, Lizunov A. OculusGraphy: Signal Analysis of the Electroretinogram in a Rabbit Model of Endophthalmitis Using Discrete and Continuous Wavelet Transforms. Bioengineering. 2023; 10(6):708. https://doi.org/10.3390/bioengineering10060708
Chicago/Turabian StyleZhdanov, Aleksei, Paul Constable, Sultan Mohammad Manjur, Anton Dolganov, Hugo F. Posada-Quintero, and Aleksander Lizunov. 2023. "OculusGraphy: Signal Analysis of the Electroretinogram in a Rabbit Model of Endophthalmitis Using Discrete and Continuous Wavelet Transforms" Bioengineering 10, no. 6: 708. https://doi.org/10.3390/bioengineering10060708