


Optimized Solutions of Electrocardiogram Lead and Segment Selection for Cardiovascular Disease Diagnostics
 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Datasets
2.1.1. The SH Database
2.1.2. The PTB Database
2.2. The Genetic Algorithm-Based ECG Leads and Segment Length Optimization Framework
2.2.1. Raw ECG Data Preprocessing
2.2.2. Feature Extraction at Different Fragment Lengths
2.2.3. Generating Optimal Combination by Genetic Algorithm
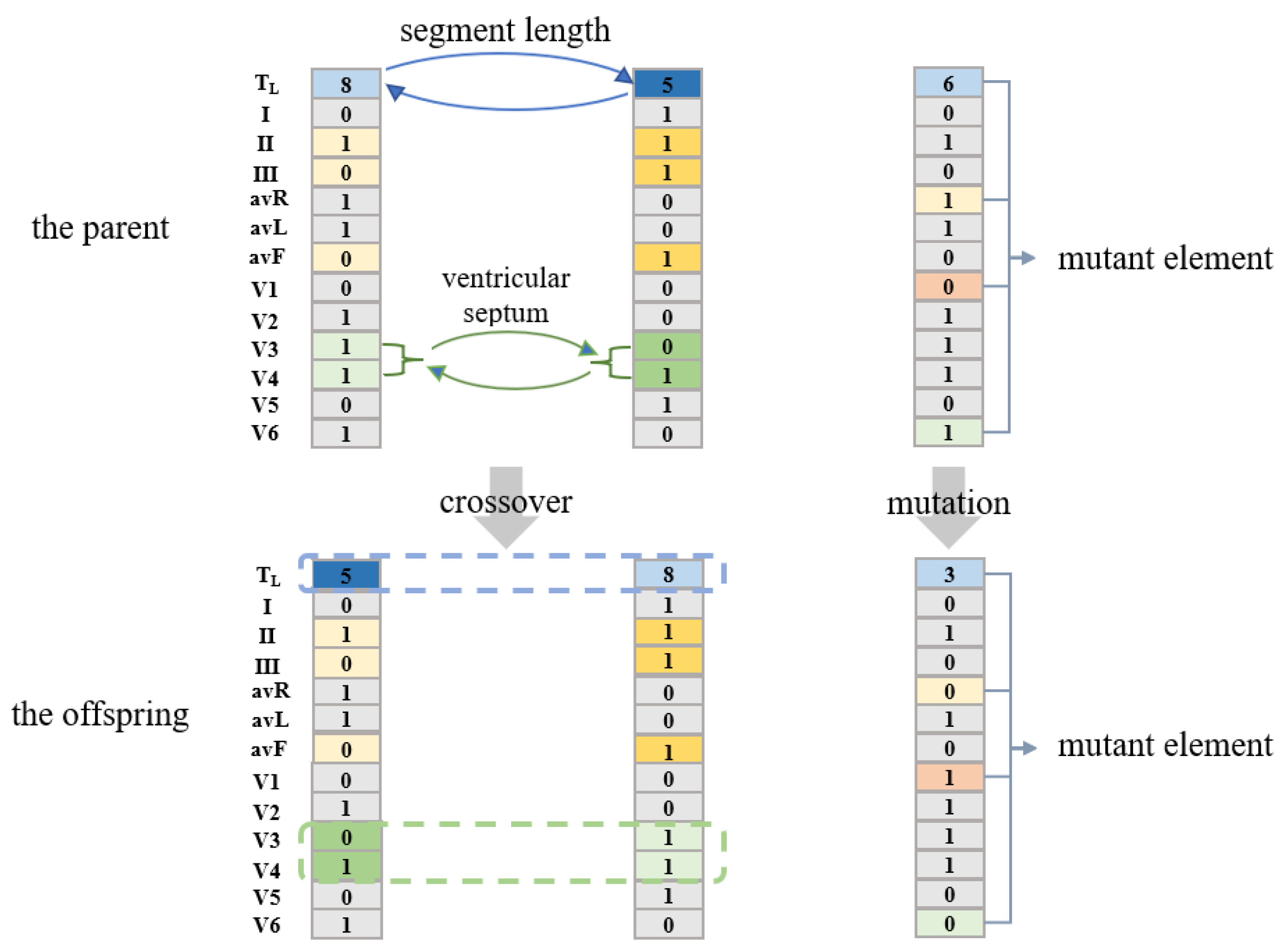
The Proposed Encoding Strategy
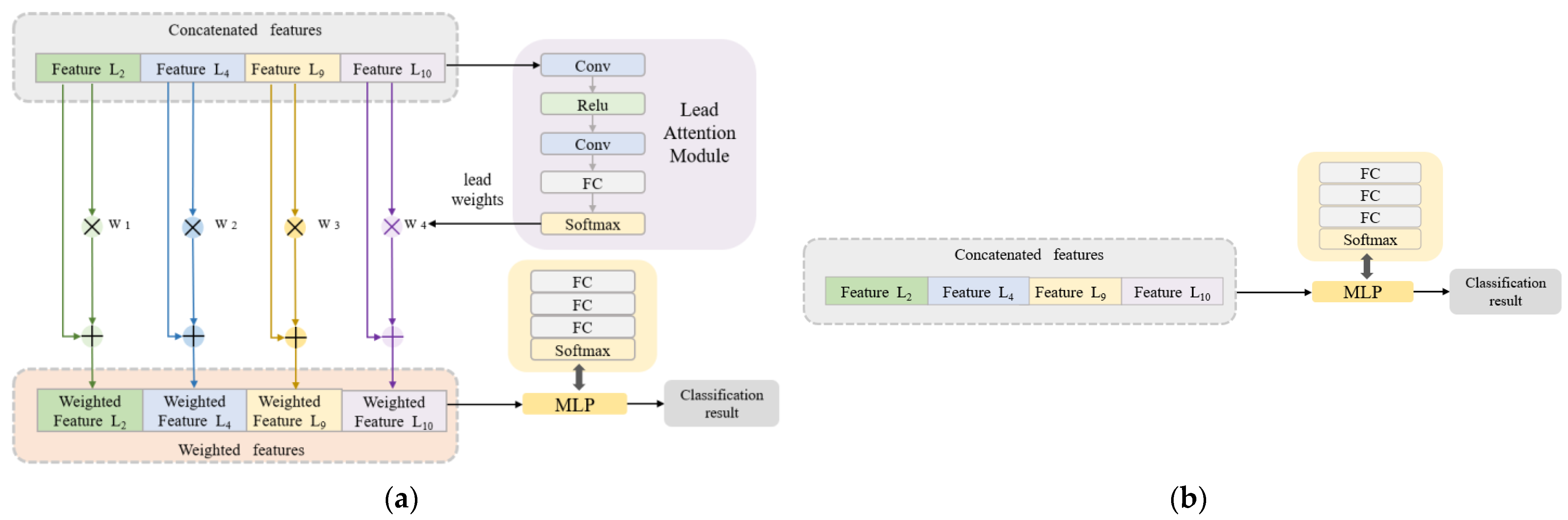
Classification Algorithm Combined with the Lead Attention Module
Generating the Optimal Solutions
| Algorithm 1 Generation of optimal ECG lengths and lead combinations based on GA |
| Input: Feature data of each lead with different segment lengths extracted in Section 2.2.2. Algorithm settings, population size = 100, maximum number of iterations = 20 Output: Optimal combination of ECG leads and segment length |
| 1 G0: number of iterations: i = 0. Initialize the population with the given population size using the proposed encoding strategy. 2 for i = 0, 1, 2, …, 20 do 3 Calculate the fitness of each individual in the population Gi 4 Select the individuals with the top 50 fitness as the parent |
| 5 Generate Gi by the selected parents using crossover and mutation operations |
| 6 i = i + 1 |
| 7 if the maximum fitness in the population remains unchanged for three generations |
| 8 break from step 2 |
| 9 else 10 continue the iteration |
| 11 end |
| 12 Return the individual with the maximum fitness in the iterative process |
2.2.4. Performance Metrics
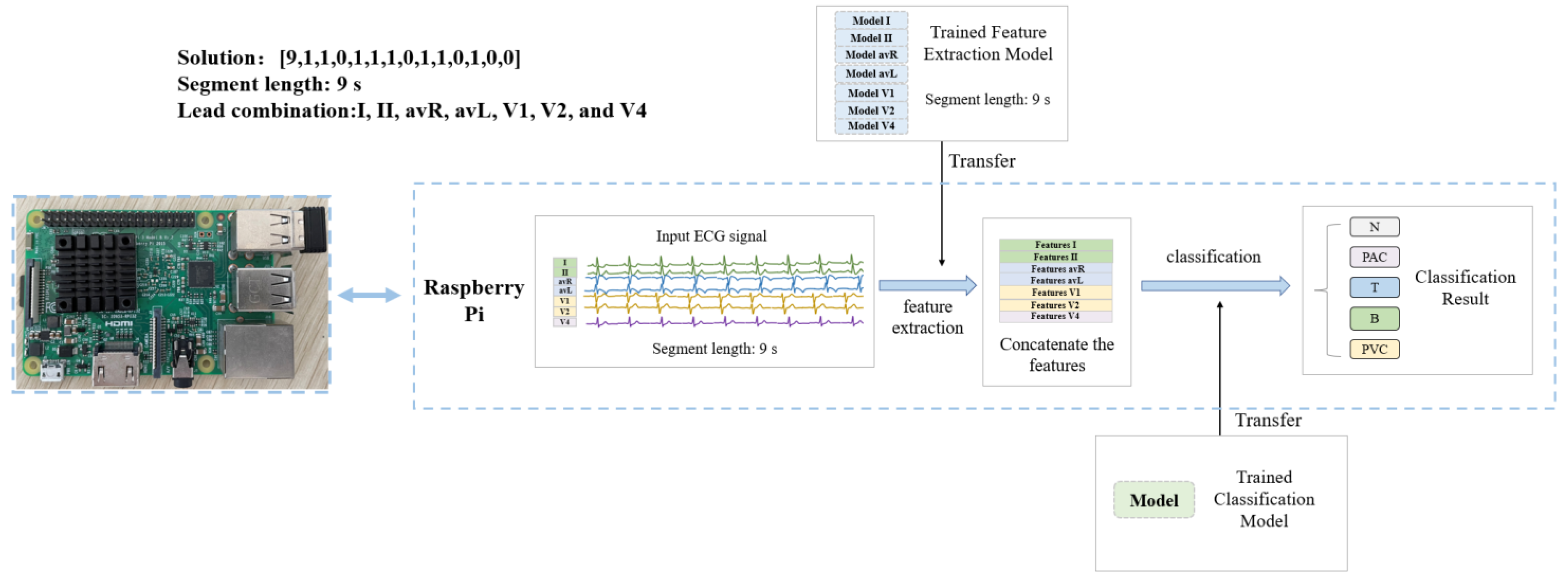
2.3. The Hardware Implementation of the Algorithm
3. Results
3.1. Arrhythmia Detection in SH Database
3.2. MI Detection in PTB Database
3.3. The Comparison of Lead Selection Methods
3.4. The Performance of the Algorithm with a Fixed Lead Number
3.5. The Results of Ablation Experiments
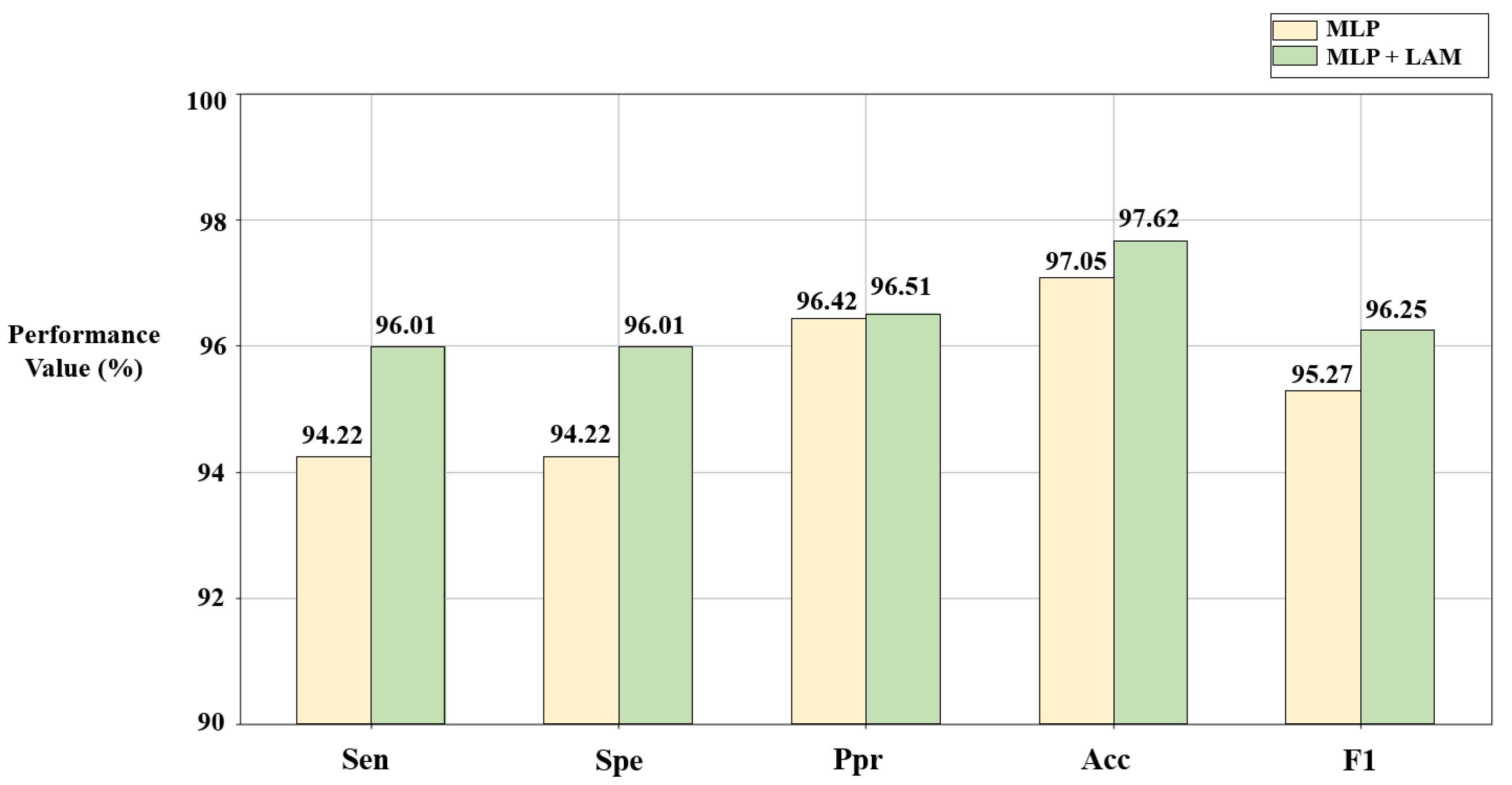
3.5.1. The Effect of the Lead Attention Module
3.5.2. The Effect of the Weighted Cross-Entropy Loss Function on PTB Database
3.6. The Results of Model Cross-Checking
3.7. The Results of Hardware Implementation of the Algorithm
4. Discussion
4.1. The Analysis of the Results
4.2. The Comparison with Existing Works
4.3. The Contributions
4.4. The Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardiovascular Diseases (CVDs). 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 23 June 2022).
- Shi, H.; Wang, H.; Huang, Y.; Zhao, L.; Qin, C.; Liu, C. A hierarchical method based on weighted extreme gradient boosting in ECG heartbeat classification. Comput. Methods Programs Biomed. 2019, 171, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alim, A.; Islam, M.K. Application of Machine Learning on Ecg Signal Classification Using Morphological Features. In Proceedings of the 2020 IEEE Region 10 Symposium (TENSYMP), Dhaka, Bangladesh, 5–7 June 2020; pp. 1632–1635. [Google Scholar]
- Shen, M.; Wang, L.; Zhu, K.; Zhu, J. Multi-lead ECG classification based on independent component analysis and support vector machine. In Proceedings of the 2010 3rd International Conference on Biomedical Engineering and Informatics, Yantai, China, 16–18 October 2010; Volume 3, pp. 960–964. [Google Scholar]
- Khorrami, H.; Moavenian, M. A comparative study of DWT, CWT and DCT transformations in ECG arrhythmias classification. Expert Syst. Appl. 2010, 37, 5751–5757. [Google Scholar] [CrossRef]
- Desai, U.; Martis, R.J.; Gurudas Nayak, C.; Seshikala, G.; Sarika, K.; Shetty, K. Decision support system for arrhythmia beats using ECG signals with DCT, DWT and EMD methods: A comparative study. J. Mech. Med. Biol. 2016, 16, 1640012. [Google Scholar] [CrossRef]
- Raj, S.; Ray, K.C. ECG signal analysis using DCT-based DOST and PSO optimized SVM. IEEE Trans. Instrum. Meas. 2017, 66, 470–478. [Google Scholar] [CrossRef]
- Zhao, L.; Li, J.; Ren, H. Multi domain fusion feature extraction and classification of ECG based on PCA-ICA. In Proceedings of the 2020 IEEE 4th Information Technology, Networking, Electronic and Automation Control Conference (ITNEC), Chongqing, China, 12–14 June 2020; Volume 1, pp. 2593–2597. [Google Scholar]
- Martis, R.J.; Acharya, U.R.; Min, L.C. ECG beat classification using PCA, LDA, ICA and discrete wavelet transform. Biomed. Signal Process. Control 2013, 8, 437–448. [Google Scholar] [CrossRef]
- Kanaan, L.; Merheb, D.; Kallas, M.; Francis, C.; Amoud, H.; Honeine, P. PCA and KPCA of ECG signals with binary SVM classification. In Proceedings of the 2011 IEEE Workshop on Signal Processing Systems (SiPS), Beirut, Lebanon, 4–7 October 2011; pp. 344–348. [Google Scholar]
- Uyar, A.; Gurgen, F. Arrhythmia classification using serial fusion of support vector machines and logistic regression. In Proceedings of the 2007 4th IEEE Workshop on Intelligent Data Acquisition and Advanced Computing Systems: Technology and Applications, Dortmund, Germany, 6–8 September 2007; pp. 560–565. [Google Scholar]
- Chauhan, S.; Vig, L.; Ahmad, S. ECG anomaly class identification using LSTM and error profile modeling. Comput. Biol. Med. 2019, 109, 14–21. [Google Scholar] [CrossRef]
- Padhy, S.; Dandapat, S. Third-order tensor based analysis of multilead ECG for classification of myocardial infarction. Biomed. Signal Process. Control 2017, 31, 71–78. [Google Scholar] [CrossRef]
- Han, C.; Shi, L. Automated interpretable detection of myocardial infarction fusing energy entropy and morphological features. Comput. Methods Programs Biomed. 2019, 175, 9–23. [Google Scholar] [CrossRef]
- Sahoo, S.; Subudhi, A.; Dash, M.; Sabut, S. Automatic classification of cardiac arrhythmias based on hybrid features and decision tree algorithm. Int. J. Autom. Comput. 2020, 17, 551–561. [Google Scholar] [CrossRef]
- Park, J.; Kang, K. PcHD: Personalized classification of heartbeat types using a decision tree. Comput. Biol. Med. 2014, 54, 79–88. [Google Scholar] [CrossRef]
- Yang, H.; Wei, Z. Arrhythmia recognition and classification using combined parametric and visual pattern features of ECG morphology. IEEE Access 2020, 8, 47103–47117. [Google Scholar] [CrossRef]
- Dilmac, S.; Ölmezz, Z.; Ölmez, T. Comparative analysis of MABC with KNN, SOM, and ACO algorithms for ECG heartbeat classification. Turk. J. Electr. Eng. Comput. Sci. 2018, 26, 2819–2830. [Google Scholar]
- Sun, L.; Lu, Y.; Yang, K.; Li, S. ECG analysis using multiple instance learning for myocardial infarction detection. IEEE Trans. Biomed. Eng. 2012, 59, 3348–3356. [Google Scholar] [CrossRef] [PubMed]
- Hannun, A.Y.; Rajpurkar, P.; Haghpanahi, M.; Tison, G.H.; Bourn, C.; Turakhia, M.P.; Ng, A.Y. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nat. Med. 2019, 25, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Kharshid, A.; Alhichri, H.S.; Ouni, R.; Bazi, Y. Classification of short-time single-lead ECG recordings using deep residual CNN. In Proceedings of the 2019 2nd International Conference on New Trends in Computing Sciences (ICTCS), Amman, Jordan, 9–11 October 2019; pp. 1–6. [Google Scholar]
- Acharya, U.R.; Fujita, H.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adam, M. Application of deep convolutional neural network for automated detection of myocardial infarction using ECG signals. Inf. Sci. 2017, 415, 190–198. [Google Scholar] [CrossRef]
- Xiaolin, L.; Cardiff, B.; John, D. A 1d convolutional neural network for heartbeat classification from single lead ecg. In Proceedings of the 2020 27th IEEE International Conference on Electronics, Circuits and Systems (ICECS), Glasgow, UK, 23–25 November 2020; pp. 1–2. [Google Scholar]
- Reasat, T.; Shahnaz, C. Detection of inferior myocardial infarction using shallow convolutional neural networks. In Proceedings of the 2017 IEEE Region 10 Humanitarian Technology Conference (R10-HTC), Dhaka, Bangladesh, 21–23 December 2017; pp. 718–721. [Google Scholar]
- Liu, W.; Zhang, M.; Zhang, Y.; Liao, Y.; Huang, Q.; Chang, S.; Wang, H.; He, J. Real-time multilead convolutional neural network for myocardial infarction detection. IEEE J. Biomed. Health Inform. 2017, 22, 1434–1444. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liang, D.; Liu, A.; Gao, M.; Chen, X.; Zhang, X.; Chen, X. MLBF-Net: A multi-lead-branch fusion network for multi-class arrhythmia classification using 12-Lead ECG. IEEE J. Transl. Eng. Health Med. 2021, 9, 1–11. [Google Scholar] [CrossRef]
- Ye, X.; Lu, Q. Automatic Classification of 12-lead ECG Based on Model Fusion. In Proceedings of the 2020 13th International Congress on Image and Signal Processing, BioMedical Engineering and Informatics (CISP-BMEI), Chengdu, China, 17–19 October 2020; pp. 733–738. [Google Scholar]
- Yang, X.; Zhang, X.; Yang, M.; Zhang, L. 12-Lead ECG arrhythmia classification using cascaded convolutional neural network and expert feature. J. Electrocardiol. 2021, 67, 56–62. [Google Scholar] [CrossRef]
- Baloglu, U.B.; Talo, M.; Yildirim, O.; San Tan, R.; Acharya, U.R. Classification of myocardial infarction with multi-lead ECG signals and deep CNN. Pattern Recognit. Lett. 2019, 122, 23–30. [Google Scholar] [CrossRef]
- Jekova, I.; Christov, I.; Krasteva, V. Atrioventricular Synchronization for Detection of Atrial Fibrillation and Flutter in One to Twelve ECG Leads Using a Dense Neural Network Classifier. Sensors 2022, 22, 6071. [Google Scholar] [CrossRef]
- Hussein, A.F.; Hashim, S.J.; Rokhani, F.Z.; Wan Adnan, W.A. An automated high-accuracy detection scheme for myocardial ischemia based on multi-lead long-interval ECG and Choi-Williams time-frequency analysis incorporating a multi-class SVM classifier. Sensors 2021, 21, 2311. [Google Scholar] [CrossRef] [PubMed]
- Krasteva, V.; Ménétré, S.; Didon, J.P.; Jekova, I. Fully convolutional deep neural networks with optimized hyperparameters for detection of shockable and non-shockable rhythms. Sensors 2020, 20, 2875. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Zhou, Q.; Lei, L.; Zheng, K.; Xiang, W. An IoT-cloud based wearable ECG monitoring system for smart healthcare. J. Med. Syst. 2016, 40, 286. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Yi, C.; Li, W.; Li, Y. A wearable H-shirt for exercise ECG monitoring and individual lactate threshold computing. Comput. Ind. 2017, 92, 1–11. [Google Scholar] [CrossRef]
- Liu, C.; Zhang, X.; Zhao, L.; Liu, F.; Chen, X.; Yao, Y.; Li, J. Signal quality assessment and lightweight QRS detection for wearable ECG SmartVest system. IEEE Internet Things J. 2018, 6, 1363–1374. [Google Scholar] [CrossRef]
- Mitchell, M. An Introduction to Genetic Algorithms; MIT Press: Cambridge, MA, USA, 1998. [Google Scholar]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.-K.; Stanley, H.E. Physiobank, physiotoolkit, and physionet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef]
- Available online: https://www.physionet.org/content/ptbdb/1.0.0/ (accessed on 20 June 2022).
- Kumar, A.; Tomar, H.; Mehla, V.K.; Komaragiri, R.; Kumar, M. Stationary wavelet transform based ECG signal denoising method. ISA Trans. 2021, 114, 251–262. [Google Scholar] [CrossRef]
- Seena, V.; Yomas, J. A review on feature extraction and denoising of ECG signal using wavelet transform. In Proceedings of the 2014 2nd international conference on devices, circuits and systems (ICDCS), Coimbatore, India, 6–8 March 2014; pp. 1–6. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Gordon-Rodriguez, E.; Loaiza-Ganem, G.; Pleiss, G.; Cunningham, J.P. Uses and abuses of the cross-entropy loss: Case studies in modern deep learning. In Proceedings of the 2nd International Conference on Electronics, Biomedical Engineering, and Health Informatics, Surabaya, Indonesia, 3–4 November 2020; Volume 137, pp. 1–10. [Google Scholar]
- Fu, J.; Liu, J.; Tian, H.; Li, Y.; Bao, Y.; Fang, Z.; Lu, H. Dual attention network for scene segmentation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 16–17 June 2019; pp. 3146–3154. [Google Scholar]
- Available online: https://www.tsu.tw/heart/ecg/qsecg/jichu/39.html (accessed on 29 June 2022).
- Zimetbaum, P.J.; Josephson, M.E. Use of the electrocardiogram in acute myocardial infarction. N. Engl. J. Med. 2003, 348, 933–940. [Google Scholar] [CrossRef]
- Fu, L.; Lu, B.; Nie, B.; Peng, Z.; Liu, H.; Pi, X. Hybrid network with attention mechanism for detection and location of myocardial infarction based on 12-lead electrocardiogram signals. Sensors 2020, 20, 1020. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signal Type | Number of Patients in Training Set | Number of Patients in Test Set |
|---|---|---|
| Normal ECG (N) | 1336 | 334 |
| Premature atrial contractions (PAC) | 1024 | 260 |
| Premature ventricular contractions (PVC) | 328 | 82 |
| Tachycardia (T) | 532 | 137 |
| Bradycardia (B) | 606 | 147 |
| Signal Type | Number of Patients in Training Set | Number of Records in Training Set | Number of Patients in Test Set | Number of Records in Test Set |
|---|---|---|---|---|
| Healthy controls (HC) | 41 | 63 | 11 | 17 |
| Myocardial infarction (MI) | 118 | 294 | 30 | 74 |
| Fragment Length | The SH Database | The PTB Database | |||||
|---|---|---|---|---|---|---|---|
| Number of Fragments | Number of Fragments | ||||||
| N | PAC | PVC | T | B | HC | MI | |
| 1 s | 47,032 | 33,464 | 14,553 | 21,131 | 17,499 | 9515 | 41,455 |
| 2 s | 22,985 | 16,458 | 7169 | 10,418 | 8608 | 4783 | 20,748 |
| 3 s | 15,210 | 10,690 | 4736 | 6859 | 5548 | 3215 | 13,945 |
| 4 s | 11,069 | 7877 | 3484 | 5053 | 4074 | 2417 | 10,388 |
| 5 s | 8777 | 6156 | 2737 | 3982 | 3196 | 1966 | 8575 |
| 6 s | 7083 | 5042 | 2258 | 3248 | 2625 | 1647 | 7156 |
| 7 s | 6030 | 4139 | 1889 | 2732 | 2129 | 1407 | 6087 |
| 8 s | 5088 | 3644 | 1645 | 2350 | 1861 | 1248 | 5369 |
| 9 s | 4614 | 3213 | 1474 | 2118 | 1646 | 1089 | 4668 |
| Layer Name | Number of Filters × Kernel Size | Stride | Activation Function | |
|---|---|---|---|---|
| Input | Input size = 1000 (1 s)–9000 (9 s) | |||
| Conv1+BN | 64 × 13 | 1 | ReLU | |
| Max Pool1 | — | 2 | — | |
| Conv2_x | Conv2_1+BN | 64 × 3 | 1 | ReLU |
| Conv2_2+BN | 64 × 3 | 2 | ReLU | |
| Average Pool2 | — | 2 | — | |
| Conv3_x | Conv3_1+BN | 64 × 3 | 1 | ReLU |
| Conv3_2+BN | 64 × 3 | 2 | ReLU | |
| Average Pool3 | — | 2 | — | |
| Conv4_x | Conv4_1+BN | 128 × 3 | 1 | ReLU |
| Conv4_2+BN | 128 × 3 | 2 | ReLU | |
| Average Pool4 | — | 2 | — | |
| Conv5_x | Conv5_1+BN | 256 × 3 | 1 | ReLU |
| Conv5_2+BN | 256 × 3 | 2 | ReLU | |
| Average Pool5 | — | 2 | — | |
| Conv6_x | Conv6_1+BN | 512 × 3 | 1 | ReLU |
| Conv6_2+BN | 512 × 3 | 2 | ReLU | |
| Average Pool6 | — | 2 | — | |
| Conv7_x | Conv7_1+BN | 512 × 3 | 1 | ReLU |
| Conv7_2+BN | 512 × 3 | 2 | ReLU | |
| Average Pool7 | — | 2 | — | |
| GAP, FC (Units = 2 or units = 5), Softmax (Arrhythmia), or Sigmoid (Myocardial infarction) | ||||
| ECG Leads | Parts of the Heart |
|---|---|
| I (L1), avL (L5) | Anterior side wall of the left ventricle |
| II(L2), III(L3), avF (L6) | Ventricle posterior wall |
| avR (L4) | Inner chamber of ventricle |
| V1 (L7), V2 (L8) | Right ventricle |
| V3 (L9), V4 (L10) | Ventricular septum |
| V5 (L11), V6 (L12) | Left ventricle |
| Predicted Class | ||||||
|---|---|---|---|---|---|---|
| N | PAC | T | B | PVC | ||
| True Class | N | 998 | 0 | 0 | 0 | 0 |
| PAC | 1 | 655 | 0 | 0 | 5 | |
| T | 0 | 0 | 429 | 0 | 0 | |
| B | 0 | 1 | 0 | 332 | 0 | |
| PVC | 5 | 12 | 0 | 0 | 279 | |
| Class | Sen (%) | Spe (%) | Ppr (%) | Acc (%) | F1 (%) |
|---|---|---|---|---|---|
| N | 100.00 | 99.65 | 99.40 | 99.78 | 99.70 |
| PAC | 99.09 | 99.37 | 98.05 | 99.30 | 98.57 |
| T | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| B | 99.70 | 100.00 | 100.00 | 99.96 | 99.85 |
| PVC | 94.26 | 99.79 | 98.24 | 99.19 | 96.21 |
| Average | 98.61 | 99.76 | 99.14 | 99.65 | 98.87 |
| Predicted Class | |||
|---|---|---|---|
| HC | MI | ||
| True Class | HC | 391 | 28 |
| MI | 22 | 1663 | |
| Class | Sen (%) | Spe (%) | Ppr (%) | Acc (%) | F1 (%) |
|---|---|---|---|---|---|
| HC | 93.32 | 98.69 | 94.67 | 97.62 | 93.99 |
| MI | 98.69 | 93.32 | 98.34 | 97.62 | 98.52 |
| Average | 96.01 | 96.01 | 96.51 | 97.62 | 96.25 |
| Lead | Coding | Sen (%) | Spe (%) | Ppr (%) | Acc (%) | F1 (%) |
|---|---|---|---|---|---|---|
| I | [9,1,0,0,0,0,0,0,0,0,0,0,0] | 79.58 | 94.71 | 77.50 | 91.93 | 78.29 |
| II | [9,0,1,0,0,0,0,0,0,0,0,0,0] | 81.17 | 95.17 | 79.24 | 92.55 | 79.73 |
| III | [9,0,0,1,0,0,0,0,0,0,0,0,0] | 79.01 | 94.28 | 77.66 | 91.37 | 78.07 |
| avR | [9,0,0,0,1,0,0,0,0,0,0,0,0] | 80.23 | 95.06 | 79.55 | 92.52 | 79.73 |
| avL | [9,0,0,0,0,1,0,0,0,0,0,0,0] | 77.80 | 93.77 | 73.83 | 90.15 | 74.81 |
| avF | [9,0,0,0,0,0,1,0,0,0,0,0,0] | 79.75 | 94.36 | 76.37 | 91.06 | 77.45 |
| V1 | [9,0,0,0,0,0,0,1,0,0,0,0,0] | 76.66 | 93.97 | 75.84 | 90.87 | 76.05 |
| V2 | [9,0,0,0,0,0,0,0,1,0,0,0,0] | 78.83 | 94.48 | 79.40 | 91.87 | 78.54 |
| V3 | [9,0,0,0,0,0,0,0,0,1,0,0,0] | 78.41 | 94.63 | 79.38 | 91.96 | 78.11 |
| V4 | [9,0,0,0,0,0,0,0,0,0,1,0,0] | 79.56 | 94.64 | 77.45 | 91.59 | 77.98 |
| V5 | [9,0,0,0,0,0,0,0,0,0,0,1,0] | 80.57 | 94.93 | 77.63 | 92.11 | 78.85 |
| V6 | [9,0,0,0,0,0,0,0,0,0,0,0,1] | 77.10 | 94.10 | 75.19 | 90.74 | 75.80 |
| All 12 leads | [9,1,1,1,1,1,1,1,1,1,1,1,1] | 97.84 | 99.68 | 99.12 | 99.53 | 98.41 |
| Proposed | [9,1,1,0,1,1,0,1,1,0,1,0,0] | 98.61 | 99.76 | 99.14 | 99.65 | 98.87 |
| Lead | Coding | Sen (%) | Spe (%) | Ppr (%) | Acc (%) | F1 (%) |
|---|---|---|---|---|---|---|
| I | [5,1,0,0,0,0,0,0,0,0,0,0,0] | 89.41 | 89.41 | 93.47 | 94.68 | 91.26 |
| II | [5,0,1,0,0,0,0,0,0,0,0,0,0] | 82.15 | 82.15 | 81.37 | 88.21 | 81.75 |
| III | [5,0,0,1,0,0,0,0,0,0,0,0,0] | 76.24 | 76.24 | 82.78 | 87.79 | 78.82 |
| avR | [5,0,0,0,1,0,0,0,0,0,0,0,0] | 87.24 | 87.24 | 87.72 | 92.06 | 87.48 |
| avL | [5,0,0,0,0,1,0,0,0,0,0,0,0] | 73.82 | 73.82 | 78.25 | 85.65 | 75.65 |
| avF | [5,0,0,0,0,0,1,0,0,0,0,0,0] | 75.17 | 75.17 | 76.75 | 85.08 | 75.91 |
| V1 | [5,0,0,0,0,0,0,1,0,0,0,0,0] | 74.28 | 74.28 | 75.54 | 84.36 | 74.87 |
| V2 | [5,0,0,0,0,0,0,0,1,0,0,0,0] | 73.90 | 73.90 | 87.18 | 88.36 | 78.07 |
| V3 | [5,0,0,0,0,0,0,0,0,1,0,0,0] | 68.42 | 68.42 | 76.02 | 84.03 | 70.94 |
| V4 | [5,0,0,0,0,0,0,0,0,0,1,0,0] | 77.70 | 77.70 | 84.08 | 88.55 | 80.26 |
| V5 | [5,0,0,0,0,0,0,0,0,0,0,1,0] | 86.23 | 86.23 | 89.78 | 92.59 | 87.84 |
| V6 | [5,0,0,0,0,0,0,0,0,0,0,0,1] | 86.20 | 86.20 | 90.09 | 92.68 | 87.95 |
| All 12 leads | [5,1,1,1,1,1,1,1,1,1,1,1,1] | 93.24 | 93.24 | 91.97 | 95.20 | 92.59 |
| Proposed | [5,1,0,1,0,0,1,0,1,0,1,0,1] | 96.01 | 96.01 | 96.51 | 97.62 | 96.25 |
| Solutions | SH Database | PTB Database | ||||
|---|---|---|---|---|---|---|
| Optimal Lead Combination | Acc (%) | F1 (%) | Optimal Lead Combination | Acc (%) | F1 (%) | |
| Optimal solution | I, II, avR, avL, V1, V2, V4 | 99.65 | 98.87 | I, III, avF, V2, V4, V6 | 97.62 | 96.25 |
| Optimal solution fixed with 2 leads | avR, V4 | 90.65 | 89.48 | I, V6 | 95.10 | 92.29 |
| Optimal solution fixed with 3 leads | I, avR, V4 | 94.63 | 93.89 | I, avF, V6 | 96.10 | 93.62 |
| Optimal solution fixed with 4 leads | I, II, avR, V4 | 96.95 | 96.12 | I, III, avF, V6 | 96.87 | 96.13 |
| Predicted Class | |||
|---|---|---|---|
| HC | MI | ||
| True Class | HC | 356 | 63 |
| MI | 19 | 1666 | |
| Loss Function | Sen (%) | Spe (%) | Ppr (%) | Acc (%) | F1 (%) |
|---|---|---|---|---|---|
| Cross-entropy | 91.92 | 91.92 | 95.64 | 96.10 | 93.64 |
| Weighted cross-entropy | 96.01 | 96.01 | 96.51 | 97.62 | 96.25 |
| Predicted Class | ||||||
|---|---|---|---|---|---|---|
| N | PAC | T | B | PVC | ||
| True Class | HC | 1081 | 8 | 0 | 0 | 0 |
| MI | 163 | 126 | 2222 | 0 | 2157 | |
| Predicted Class | |||
|---|---|---|---|
| HC | MI | ||
| True Class | N | 8754 | 23 |
| PAC | 5297 | 859 | |
| T | 27 | 3955 | |
| B | 3174 | 22 | |
| PVC | 146 | 2591 | |
| Disease Categories | Segment Length of the Input Signal (s) | Processing Time of Raspberry Pi (s) | Time Ratio | Accuracy of Hardware Implementation |
|---|---|---|---|---|
| Arrhythmia | 9.00 | 1.16 | 0.129 | 100% |
| MI | 5.00 | 0.64 | 0.128 | 100% |
| Research | Database | ECG Leads | Number of Categories | Method | ECG Length (s) | Acc (%) | F1 (%) |
|---|---|---|---|---|---|---|---|
| [22] 2017 | PTB | II | 2 | CNN | 0.651 | 95.22 | - |
| [24] 2017 | PTB | II, III, avF | 2 | Shallow CNN | 3.072 | 84.54 | - |
| [14] 2019 | PTB | All 12 leads | 2 | SVM | 0.8 | 92.69 | 83.26 |
| [46] 2020 | PTB | All 12 leads | 2 | MLA-CNN-BiGRU | 0.651 | 96.50 | - |
| Proposed | PTB | I, III, avF, V2, V4, V6 | 2 | GA-LSLO | 5 | 97.62 | 96.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, J.; Li, Z.; Liu, W.; Zhang, H.; Guo, Q.; Chang, S.; Wang, H.; He, J.; Huang, Q. Optimized Solutions of Electrocardiogram Lead and Segment Selection for Cardiovascular Disease Diagnostics. Bioengineering 2023, 10, 607. https://doi.org/10.3390/bioengineering10050607
Shi J, Li Z, Liu W, Zhang H, Guo Q, Chang S, Wang H, He J, Huang Q. Optimized Solutions of Electrocardiogram Lead and Segment Selection for Cardiovascular Disease Diagnostics. Bioengineering. 2023; 10(5):607. https://doi.org/10.3390/bioengineering10050607
Chicago/Turabian StyleShi, Jiguang, Zhoutong Li, Wenhan Liu, Huaicheng Zhang, Qianxi Guo, Sheng Chang, Hao Wang, Jin He, and Qijun Huang. 2023. "Optimized Solutions of Electrocardiogram Lead and Segment Selection for Cardiovascular Disease Diagnostics" Bioengineering 10, no. 5: 607. https://doi.org/10.3390/bioengineering10050607