
CT Imaging of Eustachian Tube Balloon Dilation: Method Development on Cadaver Heads
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Specimen Preparation
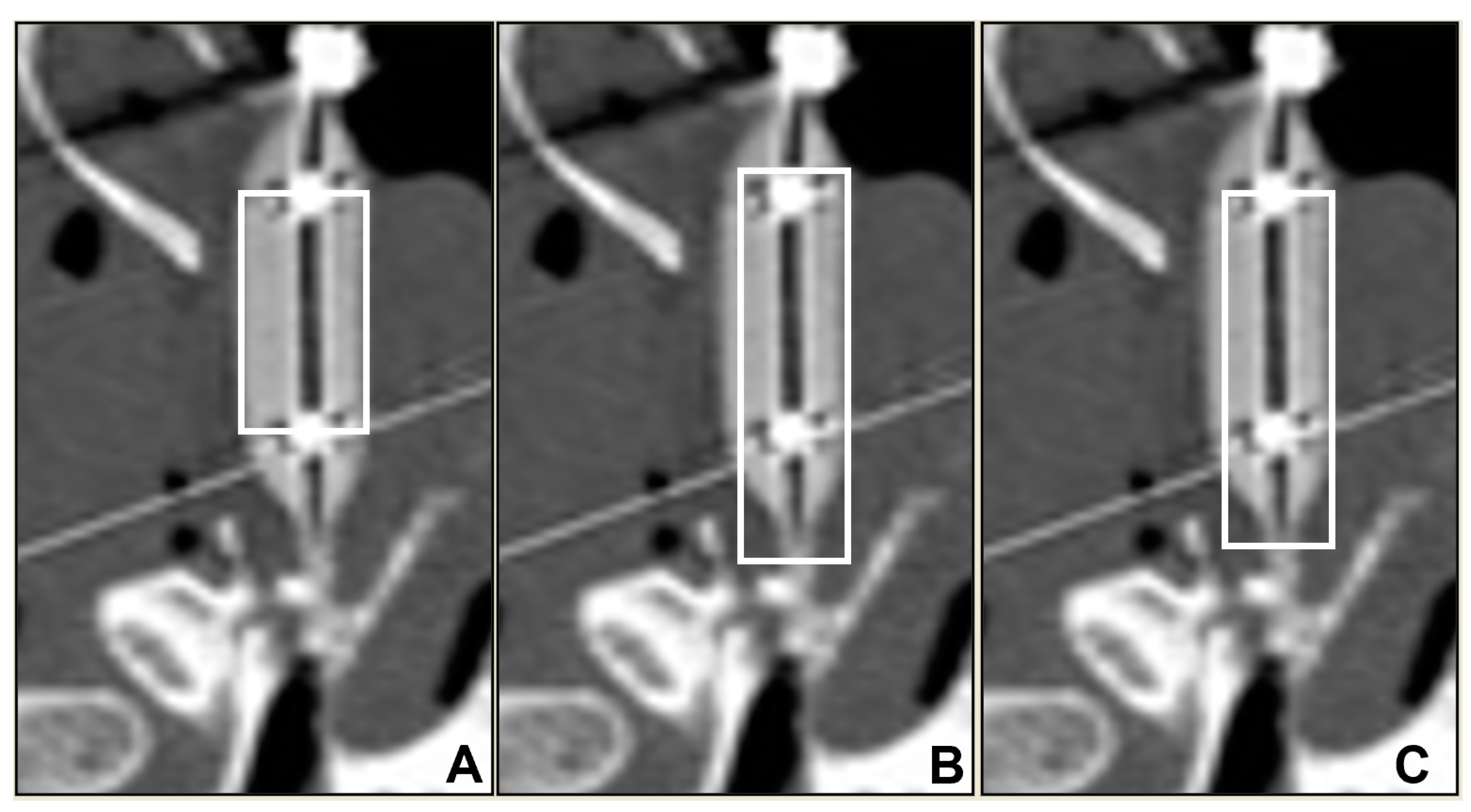
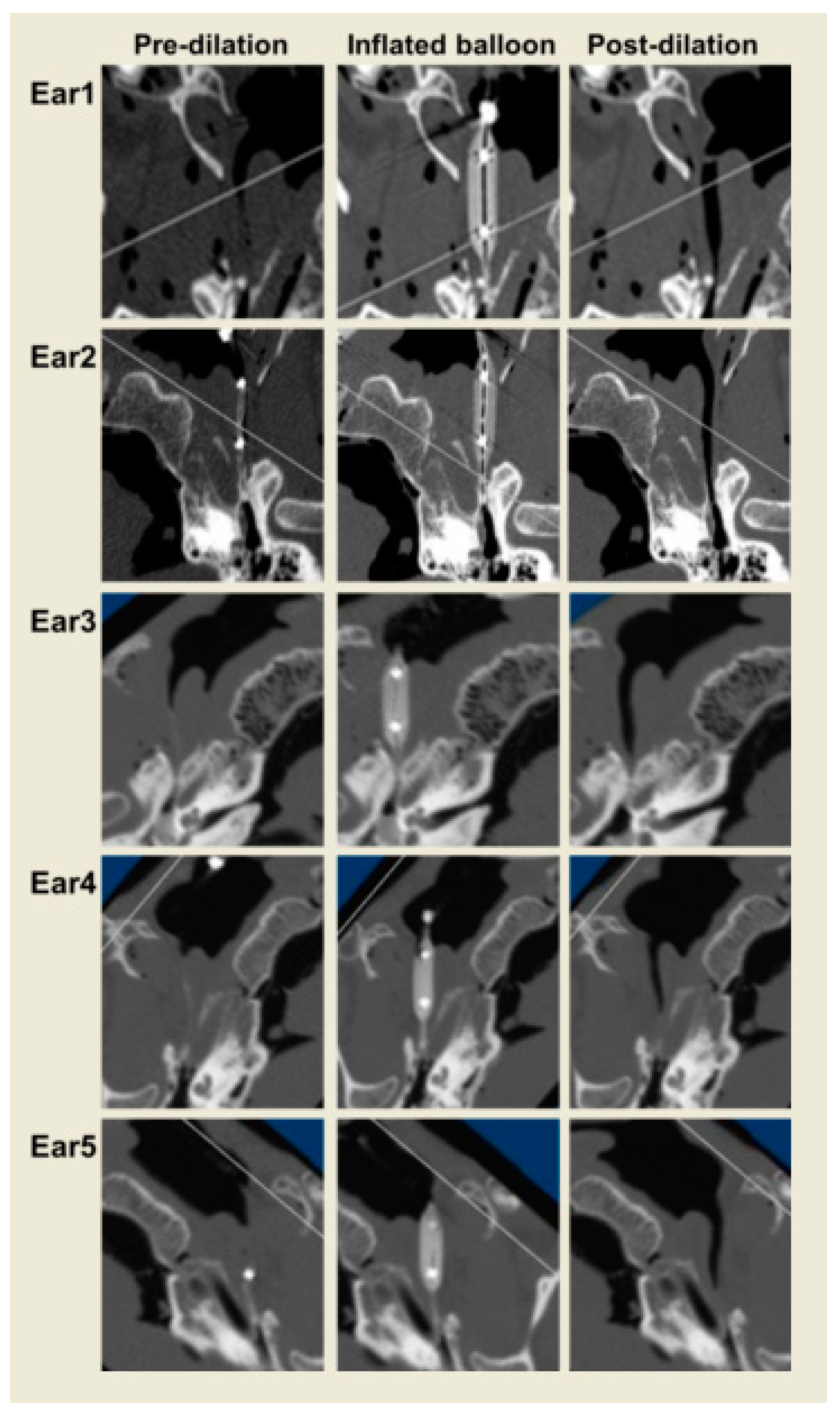
2.2. Experimental Protocol
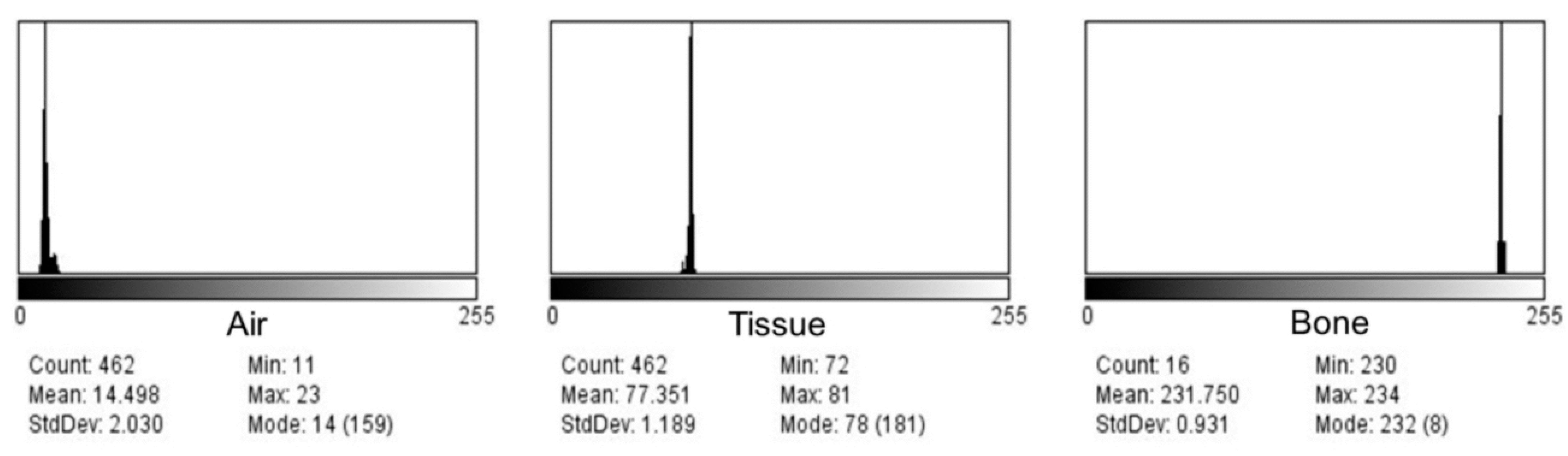
2.3. Image Analysis
3. Results
4. Discussion
5. Study Limitations
- The main limitation of this study is the small sample size. Even for method development, a larger sample size would have been better;
- The ImageJ image analysis software may have limitations compared to other newer software that may eliminate some of the labor-intensive steps in standardizing ROIs and generating outcome images and reports;
- Utilizing a cadaver head in the study has inherent limitations due to tissue elasticity and recoil properties similar to those in live human subjects. On the other hand, it was possible to have six consecutive CT scans as per the protocol on cadaver heads for the purpose of method development, while this would not be justified in live human subjects;
- The effects of balloon shape and length, as well as different durations of balloon inflation, have not been explored in this study. Future studies incorporating and controlling the biomechanics of the balloons and their effects on tissues may provide a better understanding of the role of this treatment and its long-term outcomes and consequences.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bluestone, C.D.; Bluestone, M.B. Eustachian Tube: Structure, Function, and Role in Middle-Ear Disease, 2nd ed.; Peoples Medical Publishing House: Raleigh, NC, USA, 2017. [Google Scholar]
- Doyle, W.J. A formal description of middle ear pressure-regulation. Hear Res. 2017, 354, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Bluestone, C.D.; Klein, J.O. Otitis Media in Infant and Children, 5th ed.; B. C. Decker, Inc.: Hamilton, OT, Canada, 2007. [Google Scholar]
- Poe, D.S.; Silvola, J.; Pyykko, I. Balloon dilation of the cartilaginous eustachian tube. Otolaryngol. Head Neck Surg. 2011, 144, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Schroder, S.; Lehmann, M.; Ebmeyer, J.; Upile, T.; Sudhoff, H. Balloon Eustachian tuboplasty: A retrospective cohort study. Clin. Otolaryngol. 2015, 40, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Poe, D.; Anand, V.; Dean, M.; Roberts, W.H.; Stolovitzky, J.P.; Hoffmann, K.; Nachlas, N.E.; Light, J.P.; Widick, M.H.; Sugrue, J.P.; et al. Balloon dilation of the eustachian tube for dilatory dysfunction: A randomized controlled trial. Laryngoscope 2018, 128, 1200–1206. [Google Scholar] [CrossRef] [PubMed]
- Meyer, T.A.; O’Malley, E.M.; Schlosser, R.J.; Soler, Z.M.; Cai, J.; Hoy, M.J.; Slater, P.W.; Cutler, J.L.; Simpson, R.J.; Clark, M.J.; et al. A Randomized Controlled Trial of Balloon Dilation as a Treatment for Persistent Eustachian Tube Dysfunction With 1-Year Follow-Up. Otol. Neurotol. 2018, 39, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.Y.; Kok, S.; Walton, J. Balloon dilation for eustachian tube dysfunction: Systematic review. J. Laryngol. Otol. 2016, 130 (Suppl. 4), S2–S6. [Google Scholar] [CrossRef] [PubMed]
- Huisman, J.M.L.; Verdam, F.J.; Stegeman, I.; de Ru, J.A. Treatment of Eustachian tube dysfunction with balloon dilation: A systematic review. Laryngoscope 2018, 128, 237–247. [Google Scholar] [CrossRef]
- Alper, C.M.; Rath, T.J.; Teixeira, M.S.; Swarts, J.D. A Novel Imaging Method for the Cartilaginous Eustachian Tube Lumen: Computerized Tomography During the Forced Response Test. Ann. Otol. Rhinol. Laryngol. 2018, 127, 13–20. [Google Scholar] [CrossRef]
- Catalano, P.J.; Jonnalagadda, S.; Yu, V.M. Balloon catheter dilatation of Eustachian tube: A preliminary study. Otol. Neurotol. 2012, 33, 1549–1552. [Google Scholar] [CrossRef]
- McCoul, E.D.; Anand, V.K. Eustachian tube balloon dilation surgery. Int. Forum Allergy Rhinol. 2012, 2, 191–198. [Google Scholar] [CrossRef]
- Tisch, M.; Maier, H.; Sudhoff, H. Balloon dilation of the Eustachian tube: Clinical experience in the management of 126 children. Acta Otorhinolaryngol. Ital. 2017, 37, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Alper, C.M.; Teixeira, M.S.; Rath, T.J.; Hall-Burton, D.; Swarts, J.D. Change in Eustachian Tube Function With Balloon Dilation in Adults With Ventilation Tubes. Otol. Neurotol. 2020, 41, 482–488. [Google Scholar] [CrossRef] [PubMed]
- McCoul, E.D.; Anand, V.K.; Christos, P.J. Validating the clinical assessment of eustachian tube dysfunction: The Eustachian Tube Dysfunction Questionnaire (ETDQ-7). Laryngoscope 2012, 122, 1137–1141. [Google Scholar] [CrossRef]
- Schroder, S.; Lehmann, M.; Sauzet, O.; Ebmeyer, J.; Sudhoff, H. A novel diagnostic tool for chronic obstructive eustachian tube dysfunction-the eustachian tube score. Laryngoscope 2015, 125, 703–708. [Google Scholar] [CrossRef]
- Schroder, S.; Lehmann, M.; Korbmacher, D.; Sauzet, O.; Sudhoff, H.; Ebmeyer, J. Evaluation of tubomanometry as a routine diagnostic tool for chronic obstructive Eustachian tube dysfunction. Clin. Otolaryngol. 2015, 40, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Alper, C.M.; Teixeira, M.S.; Kim, J.H.; Douglas Swarts, J. Diagnostic accuracy of tubomanometry R value in detecting the Eustachian tube pressure equalizing function. Eur. Arch. Otorhinolaryngol. 2017, 274, 1865–1872. [Google Scholar] [CrossRef]
- Teixeira, M.S.; Swarts, J.D.; Alper, C.M. Accuracy of the ETDQ-7 for Identifying Persons with Eustachian Tube Dysfunction. Otolaryngol. Head Neck Surg. 2018, 158, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Niwa, H.; Takahashi, M.; Yanagita, N.; Naganawa, S. Evaluation of clearance function of the Eustachian tube by sequential contrast CT. Acta Otolaryngol. Suppl. 1990, 471, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.J.; Choi, A.Y.; Yoon, S.W.; Kwon, K.H.; Yeo, S.G. The Value of Measuring Eustachian Tube Aeration on Temporal Bone CT in Patients with Chronic Otitis Media. Clin. Exp. Otorhinolaryngol. 2010, 3, 59–64. [Google Scholar] [CrossRef]
- Poe, D.S.; Hanna, B.M. Balloon dilation of the cartilaginous portion of the eustachian tube: Initial safety and feasibility analysis in a cadaver model. Evaluation Studies. Am. J. Otolaryngol. 2011, 32, 115–123. [Google Scholar] [CrossRef]
- Abdel-Aziz, T.; Schroder, S.; Lehmann, M.; Gehl, H.B.; Ebmeyer, J.; Sudhoff, H. Computed tomography before balloon Eustachian tuboplasty—A true necessity? Otol. Neurotol. 2014, 35, 635–638. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, R.; Kobayashi, T.; Yoshida, M.; Yoshida, N.; Kikuchi, T.; Oshima, T.; Kawase, T.; Katori, Y. Patulous Eustachian Tube and Otitis Media With Effusion as Complications After Trigeminal Nerve Injury. Otol. Neurotol. 2017, 38, 1125–1128. [Google Scholar] [CrossRef] [PubMed]
- Buytaert, J.A.; Salih, W.H.; Dierick, M.; Jacobs, P.; Dirckx, J.J. Realistic 3D computer model of the gerbil middle ear, featuring accurate morphology of bone and soft tissue structures. J. Assoc. Res. Otolaryngol. 2011, 12, 681–696. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, H.; Kobayashi, T.; Takasaki, K.; Takahashi, H.; Ishimaru, H.; Morikawa, M.; Hayashi, K. Imaging of the patulous Eustachian tube: High-resolution CT evaluation with multiplanar reconstruction technique. Acta Otolaryngol. 2004, 124, 918–923. [Google Scholar] [CrossRef]
- Sheer, F.J.; Swarts, J.D.; Ghadiali, S.N. Three-dimensional finite element analysis of Eustachian tube function under normal and pathological conditions. Med. Eng. Phys. 2012, 34, 605–616. [Google Scholar] [CrossRef]
- Tarabichi, M.; Najmi, M. Visualization of the eustachian tube lumen with Valsalva computed tomography. Laryngoscope 2015, 125, 724–729. [Google Scholar] [CrossRef]
- Ikeda, R.; Kikuchi, T.; Oshima, H.; Miyazaki, H.; Hidaka, H.; Kawase, T.; Katori, Y.; Kobayashi, T. Computed tomography findings of the bony portion of the Eustachian tube with or without patulous Eustachian tube patients. Eur. Arch. Otorhinolaryngol. 2017, 274, 781–786. [Google Scholar] [CrossRef]
- Smith, M.E.; Scoffings, D.J.; Tysome, J.R. Imaging of the Eustachian tube and its function: A systematic review. Neuroradiology 2016, 58, 543–556. [Google Scholar] [CrossRef]
- Randrup, T.S.; Ovesen, T. Balloon eustachian tuboplasty: A systematic review. Otolaryngol. Head Neck Surg. 2015, 152, 383–392. [Google Scholar] [CrossRef]
- Schilder, A.G.; Bhutta, M.F.; Butler, C.C.; Holy, C.; Levine, L.H.; Kvaerner, K.J.; Norman, G.; Pennings, R.J.; Poe, D.; Silvola, J.T.; et al. Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clin. Otolaryngol. 2015, 40, 407–411. [Google Scholar] [CrossRef]
- Yoshida, H.; Kobayashi, T.; Morikawa, M.; Hayashi, K.; Tsujii, H.; Sasaki, Y. CT imaging of the patulous eustachian tube--comparison between sitting and recumbent positions. Auris Nasus Larynx 2003, 30, 135–140. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Small | Longest | Long | |
|---|---|---|---|
| Ear 1 | 20 | 6 | 8 |
| Ear 2 | 33 | 23 | 26 |
| Ear 3 | 68 | 50 | 62 |
| Ear 4 | 100 | 74 | 97 |
| Ear 5 | 98 | 68 | 88 |
| % Increase | 64 | 44 | 56 |
| Width 1 | Width 2 | Width 3 | Average | |
|---|---|---|---|---|
| Ear 1 | 3.5 | 57.8 | 31.6 | 31 |
| Ear 2 | 0 | 93.5 | 10 | 34.5 |
| Ear 3 | 9 | 75.6 | 100 | 61.5 |
| Ear 4 | 4.2 | 53.3 | 47.2 | 34.9 |
| Ear 5 | 25 | 78.9 | 0 | 34.6 |
| Average pixel | 8.3 | 71.8 | 37.8 | 39.3 |
| Distance 1 | Distance 2 | Distance 3 | |
|---|---|---|---|
| Ear 1 | 67.99 | 50.45 | 20.82 |
| Ear 2 | 87.74 | 56.01 | 34.41 |
| Ear 3 | 73.37 | 44.24 | 30.16 |
| Ear 4 | 75.41 | 37.79 | 38.09 |
| Ear 5 | 72.6 | 37.79 | 32.82 |
| Average (pixel) | 75.42 | 45.26 | 31.26 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cetin-Ferra, S.; Teixeira, M.S.; Swarts, J.D.; Rath, T.J.; Alper, C.M. CT Imaging of Eustachian Tube Balloon Dilation: Method Development on Cadaver Heads. Bioengineering 2023, 10, 592. https://doi.org/10.3390/bioengineering10050592
Cetin-Ferra S, Teixeira MS, Swarts JD, Rath TJ, Alper CM. CT Imaging of Eustachian Tube Balloon Dilation: Method Development on Cadaver Heads. Bioengineering. 2023; 10(5):592. https://doi.org/10.3390/bioengineering10050592
Chicago/Turabian StyleCetin-Ferra, Selma, Miriam S. Teixeira, J. Douglas Swarts, Tanya J. Rath, and Cuneyt M. Alper. 2023. "CT Imaging of Eustachian Tube Balloon Dilation: Method Development on Cadaver Heads" Bioengineering 10, no. 5: 592. https://doi.org/10.3390/bioengineering10050592