
Upper-Limb Kinematic Behavior and Performance Fatigability of Elderly Participants Performing an Isometric Task: A Quasi-Experimental Study

 , ,
, ,  ,
,  , , , ,
, , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
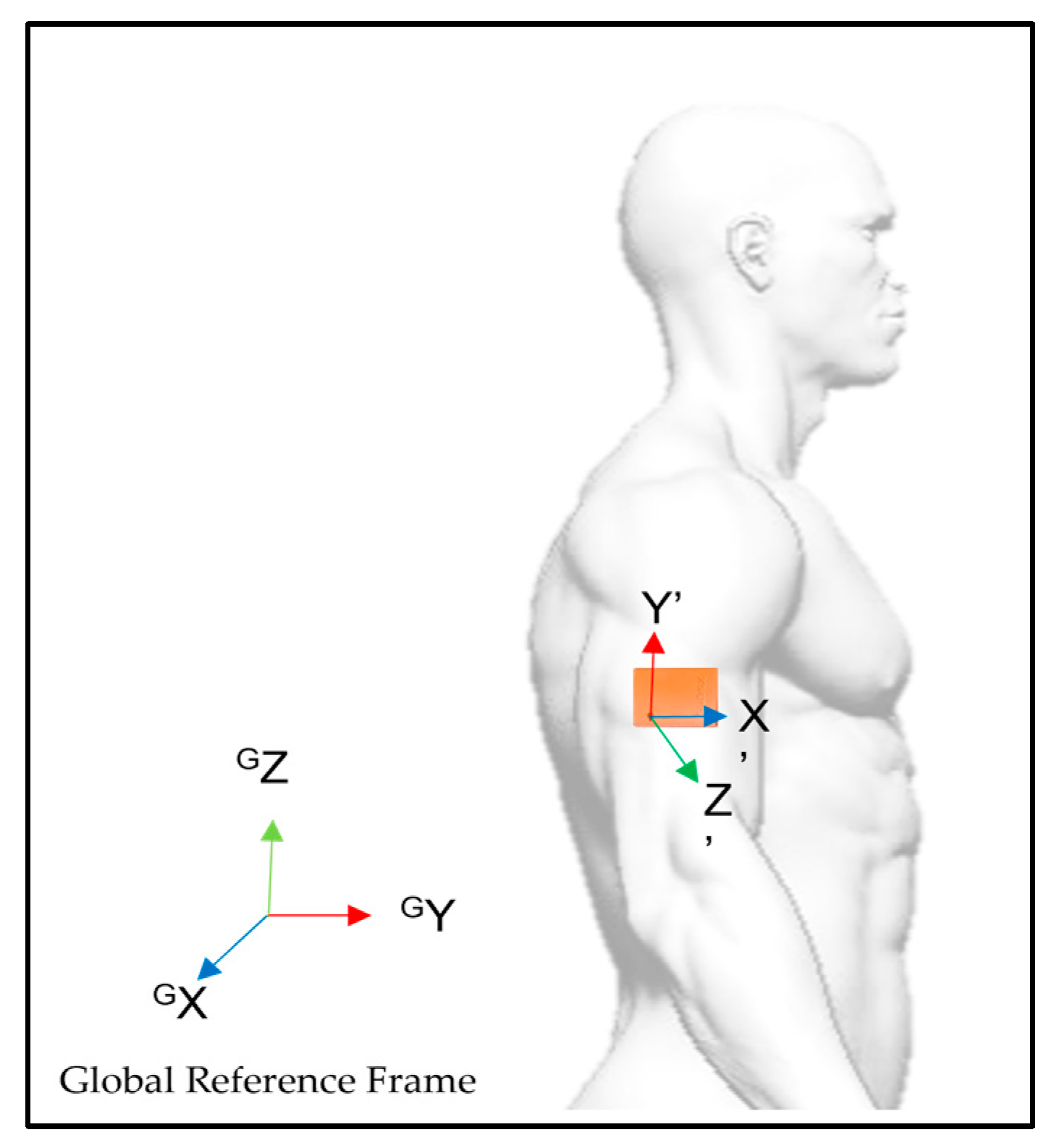
2.2. Inertial Measurement Unit (IMU) and Time-to-Task Failure (TTF)
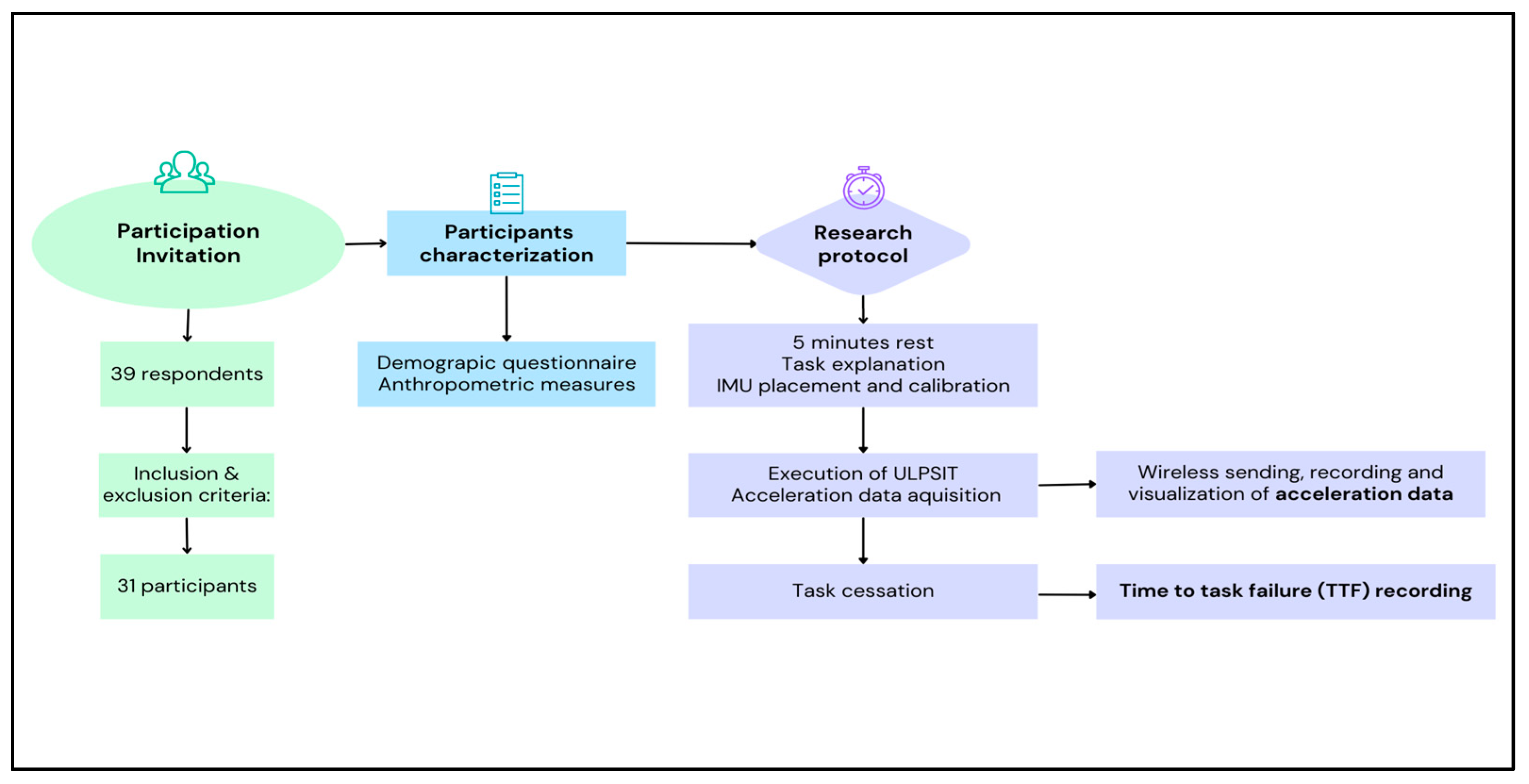
2.3. Research Procedure
2.4. Data Processing and Statistical Analysis
3. Results
3.1. Sample Demographic and Anthropometric Characteristics
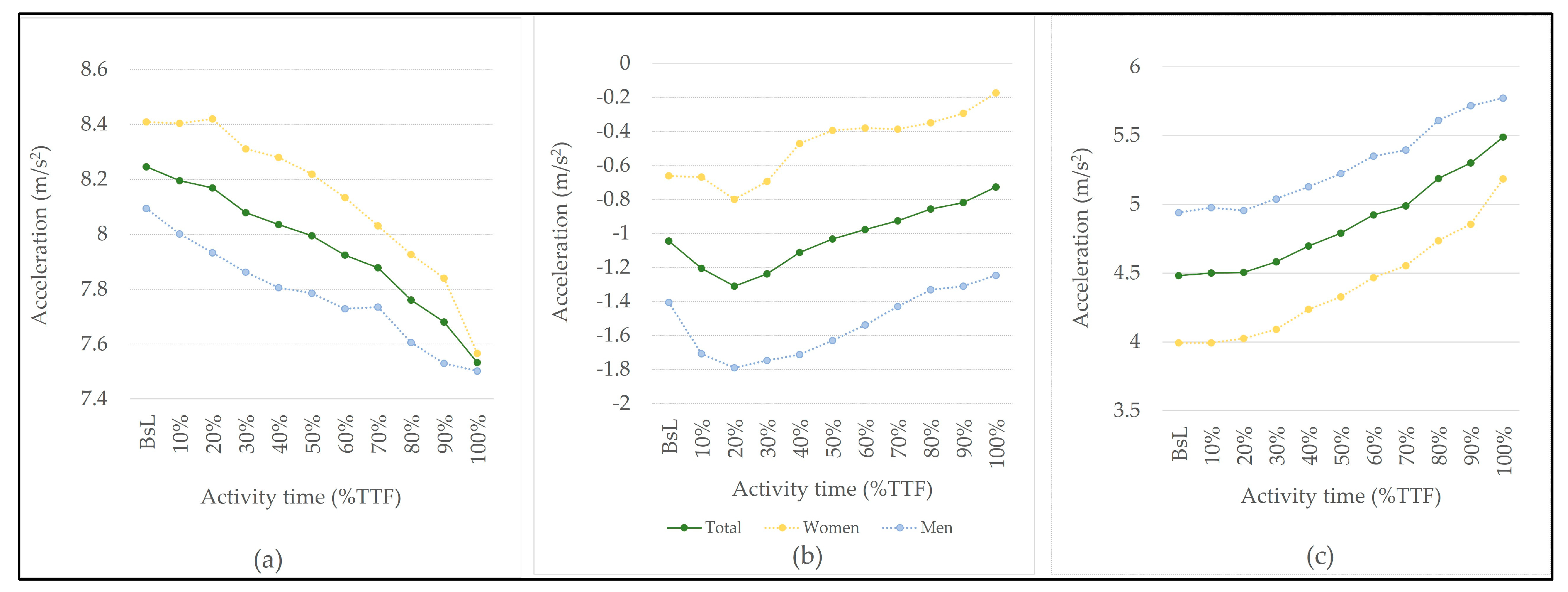
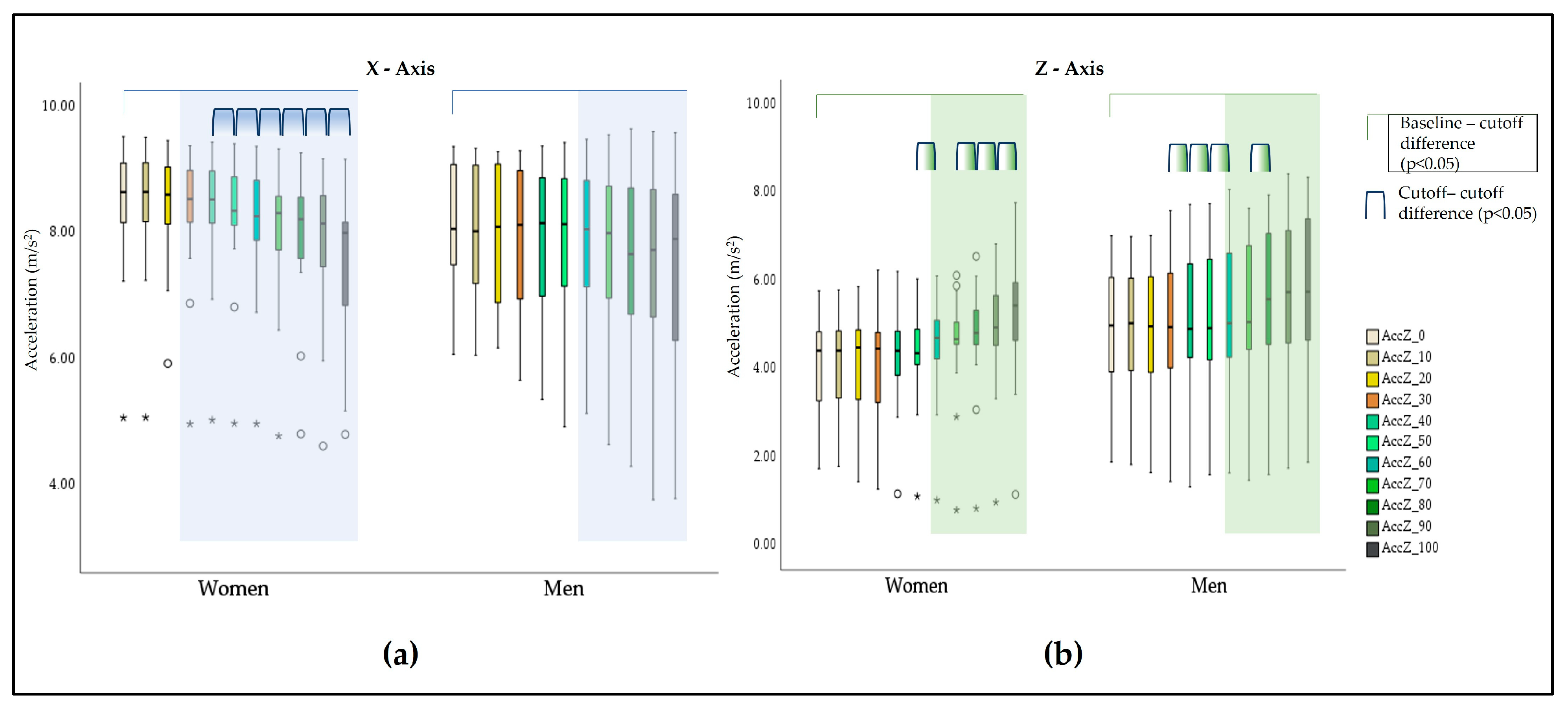
3.2. Acceleration Behavior of the Upper Limb during Isometric Activity
3.3. Time-to-task Failure
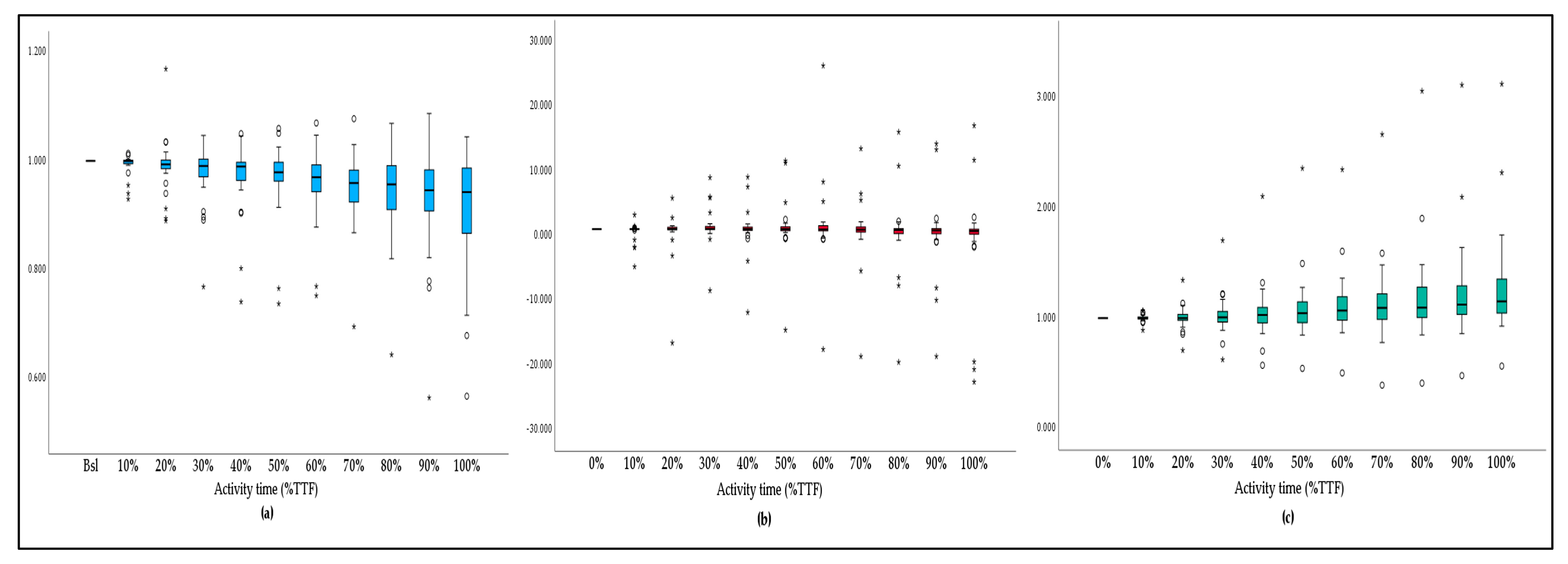
3.4. Acceleration Variation and TTF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murofushi, K.; Yamaguchi, D.; Hirohata, K.; Furuya, H.; Mitomo, S. Variations in Upper Limb and Trunk Muscles Activation during Isometric Exercises with or without Exertion of Control. Isokinet. Exerc. Sci. 2022, 30, 251–258. [Google Scholar] [CrossRef]
- Sarmento, A.O.; Santos, A.d.C.; Trombetta, I.C.; Dantas, M.M.; Oliveira Marques, A.C.; do Nascimento, L.S.; Barbosa, B.T.; dos Santos, M.R.; Andrade, M.d.A.; Jaguaribe-Lima, A.M.; et al. Regular Physical Exercise Improves Cardiac Autonomic and Muscle Vasodilatory Responses to Isometric Exercise in Healthy Elderly. Clin. Interv. Aging 2017, 12, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Lemley, K.J.; Drewek, B.; Hunter, S.K.; Hoeger Bement, M.K. Pain Relief after Isometric Exercise Is Not Task-Dependent in Older Men and Women. Med. Sci. Sports Exerc. 2014, 46, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Enoka, R.M.; Baudry, S.; Rudroff, T.; Farina, D.; Klass, M.; Duchateau, J. Unraveling the Neurophysiology of Muscle Fatigue. J. Electromyogr. Kinesiol. 2011, 21, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Velloso, M.; do Nascimento, N.H.; Gazzotti, M.R.; Jardim, J.R. Evaluation of Effects of Shoulder Girdle Training on Strength and Performance of Activities of Daily Living in Patients with Chronic Obstructive Pulmonary Disease. Int. J. COPD 2013, 8, 187–192. [Google Scholar] [CrossRef]
- Panka, G.F.L.; Oliveira, M.M.; França, D.C.; Parreira, V.F.; Britto, R.R.; Velloso, M. Ventilatory and Muscular Assessment in Healthy Subjects during an Activity of Daily Living with Unsupported Arm Elevation. Rev. Bras. Fisioter. 2010, 14, 337–343. [Google Scholar] [CrossRef]
- Frykholm, E.; Lima, V.P.; Selander, H.V.; Nyberg, A.; Janaudis-Ferreira, T. Physiological and Symptomatic Responses to Arm versus Leg Activities in People with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. COPD: J. Chronic Obstr. Pulm. Dis. 2019, 16, 390–405. [Google Scholar] [CrossRef]
- Tiller, N.B.; Campbell, I.G.; Romer, L.M. Influence of Upper-Body Exercise on the Fatigability of Human Respiratory Muscles. Med. Sci. Sports Exerc. 2017, 49, 1461–1472. [Google Scholar] [CrossRef]
- Dupuis, F.; Sole, G.; Mercier, C.; Roy, J.S. Impact of Fatigue at the Shoulder on the Contralateral Upper Limb Kinematics and Performance. PLoS ONE 2022, 17, e0266370. [Google Scholar] [CrossRef]
- Cowley, J.C.; Gates, D.H. Proximal and Distal Muscle Fatigue Differentially Affect Movement Coordination. PLoS ONE 2017, 12, e0712835. [Google Scholar] [CrossRef]
- Wu, R.; Ditroilo, M.; Delahunt, E.; de Vito, G. Age Related Changes in Motor Function (II)Decline in Motor Performance Outcomes. International Journal of Sports Medicine. Int. J. Sport Med. 2021, 42, 215–226. [Google Scholar] [CrossRef]
- Hassan, A.S.; Fajardo, M.E.; Cummings, M.; Mcpherson, L.M.; Negro, F.; Dewald, J.P.A.; Heckman, C.J.; Pearcey, G.E.P. Estimates of Persistent Inward Currents Are Reduced in Upper Limb Motor Units of Older Adults. J. Physiol. 2021, 599, 4865–4882. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; de Vito, G.; Delahunt, E.; Ditroilo, M. Age-Related Changes in Motor Function (I)Mechanical and Neuromuscular Factors. International Journal of Sports Medicine. Int. J. Sport Med. 2020, 41, 709–719. [Google Scholar] [CrossRef]
- Enoka, R.M.; Duchateau, J. Translating Fatigue to Human Performance. Med. Sci. Sports Exerc. 2016, 48, 2228–2238. [Google Scholar] [CrossRef] [PubMed]
- Gruet, M. Fatigue in Chronic Respiratory Diseases: Theoretical Framework and Implications for Real-Life Performance and Rehabilitation. Front. Physiol. 2018, 9, 1285. [Google Scholar] [CrossRef]
- Loy, B.D.; Taylor, R.L.; Fling, B.W.; Horak, F.B. Relationship between Perceived Fatigue and Performance Fatigability in People with Multiple Sclerosis: A Systematic Review and Meta-Analysis. J. Psychosom. Res. 2017, 100, 1–7. [Google Scholar] [CrossRef]
- Hunter, S.K. Performance Fatigability: Mechanisms and Task Specificity. Cold Spring Harb. Perspect. Med. 2018, 8, a029728. [Google Scholar] [CrossRef]
- Missenard, O.; Mottet, D.; Perrey, S. The Role of Cocontraction in the Impairment of Movement Accuracy with Fatigue. Exp. Brain Res. 2008, 185, 151–156. [Google Scholar] [CrossRef]
- Dupuis, F.; Sole, G.; Wassinger, C.; Bielmann, M.; Bouyer, L.J.; Roy, J.S. Fatigue, Induced via Repetitive Upper-Limb Motor Tasks, Influences Trunk and Shoulder Kinematics during an Upper Limb Reaching Task in a Virtual Reality Environment. PLoS ONE 2021, 16, e0249403. [Google Scholar] [CrossRef]
- Forman, D.A.; Forman, G.N.; Mugnosso, M.; Zenzeri, J.; Murphy, B.; Holmes, M.W.R. Sustained Isometric Wrist Flexion and Extension Maximal Voluntary Contractions Similarly Impair Hand-Tracking Accuracy in Young Adults Using a Wrist Robot. Front. Sports Act. Living 2020, 2, 53. [Google Scholar] [CrossRef]
- Pedersen, J.; Lönn, J.; Hellström, F.; Djupsjöbacka, M.; Johansson, H. Localized Muscle Fatigue Decreases the Acuity of the Movement Sense in the Human Shoulder. Med. Sci. Sports Exerc. 1999, 31, 1047–1052. [Google Scholar] [CrossRef]
- Gribble, P.L.; Mullin, L.I.; Cothros, N.; Mattar, A. Role of Cocontraction in Arm Movement Accuracy. J. Neurophysiol. 2003, 89, 2396–2405. [Google Scholar] [CrossRef] [PubMed]
- Taniai, Y.; Naniwa, T.; Nishii, J. Optimal Reaching Trajectories Based on Feedforward Control. Biol. Cybern. 2022, 116, 517–526. [Google Scholar] [CrossRef]
- Jiang, Y.; Hernandez, V.; Venture, G.; Kulić, D.; Chen, B.K. A Data-Driven Approach to Predict Fatigue in Exercise Based on Motion Data from Wearable Sensors or Force Plate. Sensors 2021, 21, 1499. [Google Scholar] [CrossRef]
- Lebel, K.; Boissy, P.; Hamel, M.; Duval, C. Inertial Measures of Motion for Clinical Biomechanics: Comparative Assessment of Accuracy under Controlled Conditions—Effect of Velocity. PLoS ONE 2013, 8, e79945. [Google Scholar] [CrossRef]
- Wang, H.; Refai, M.I.M.; van Beijnum, B.J.F. Measuring Upper-Extremity Use with One IMU. In Proceedings of the 12th International Joint Conference on Biomedical Engineering Systems and Technologies—BIOSIGNALS, Prague, Czech Republic, 22–24 February 2019; pp. 93–100. [Google Scholar] [CrossRef]
- Marotta, L.; Scheltinga, B.L.; van Middelaar, R.; Bramer, W.M.; van Beijnum, B.J.F.; Reenalda, J.; Buurke, J.H. Accelerometer-Based Identification of Fatigue in the Lower Limbs during Cyclical Physical Exercise: A Systematic Review. Sensors 2022, 22, 3008. [Google Scholar] [CrossRef]
- Rudigkeit, N.; Paulich, M.; Schepers, M.; Bellusci, G. Xsens MTw Awinda: Miniature Wireless Inertial-Magnetic Motion Tracker for Highly Accurate 3D Kinematic Applications; Xsens: Enschede, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Zhang, G.; Wong, I.K.K.; Chen, T.L.W.; Hong, T.T.H.; Wong, D.W.C.; Peng, Y.; Yan, F.; Wang, Y.; Tan, Q.; Zhang, M. Identifying Fatigue Indicators Using Gait Variability Measures: A Longitudinal Study on Elderly Brisk Walking. Sensors 2020, 20, 6983. [Google Scholar] [CrossRef] [PubMed]
- Henschke, J.; Kaplick, H.; Wochatz, M.; Engel, T. Assessing the Validity of Inertial Measurement Units for Shoulder Kinematics Using a Commercial Sensor-Software System: A Validation Study. Health Sci. Rep. 2022, 5, e772. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J.M. Systematic Review on Kinematic Assessments of Upper Limb Movements after Stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef]
- Hughes, C.M.L.; Tran, B.; Modan, A.; Zhang, X. Accuracy and Validity of a Single Inertial Measurement Unit-Based System to Determine Upper Limb Kinematics for Medically Underserved Populations. Front. Bioeng. Biotechnol. 2022, 10, 918617. [Google Scholar] [CrossRef]
- Morrow, M.M.B.; Lowndes, B.; Fortune, E.; Kaufman, K.R.; Hallbeck, M.S. Validation of Inertial Measurement Units for Upper Body Kinematics. J. Appl. Biomech. 2017, 33, 227–232. [Google Scholar] [CrossRef]
- Höglund, G.; Grip, H.; Öhberg, F. The Importance of Inertial Measurement Unit Placement in Assessing Upper Limb Motion. Med. Eng. Phys. 2021, 92, 1–9. [Google Scholar] [CrossRef]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.S. Validity and Reliability of wearable Sensors for Joint Angle Estimation: A Systematic Review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef]
- Guo, C.C.; Chiesa, P.A.; de Moor, C.; Fazeli, M.S.; Schofield, T.; Hofer, K.; Belachew, S.; Scotland, A. Digital Devices for Assessing Motor Functions in Mobility Impaired and Healthy Populations: A Systematic Literature Review. J. Med. Internet Res. 2022, 24, e37683. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.W.; Li, Z.G.; Du, H.; Yan, B.Y.; Lu, P.D. Recognition of Upper Limb Action Intention Based on IMU. Sensors 2022, 22, 1954. [Google Scholar] [CrossRef] [PubMed]
- Moyen-Sylvestre, B.; Goubault, É.; Begon, M.; Côté, J.N.; Bouffard, J.; Dal Maso, F. Power Spectrum of Acceleration and Angular Velocity Signals as Indicators of Muscle Fatigue during Upper Limb Low-Load Repetitive Tasks. Sensors 2022, 22, 8008. [Google Scholar] [CrossRef]
- Goubault, E.; Verdugo, F.; Bailly, F.; Begon, M.; Dal Maso, F. Inertial Measurement Units and Partial Least Square Regression to Predict Perceived 1 Exertion during Repetitive Fatiguing Piano Tasks; Elseiver: Amsterdam, The Netherlands, 2022. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef]
- Review, C.; Communication, S.; Principles, G. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar] [CrossRef]
- Silva-Migueis, H.; Martínez-Jiménez, E.M.; Casado-Hernández, I.; Dias, A.; Monteiro, A.J.; Martins, R.B.; Romero-Morales, C.; López-López, D.; Gómez-Salgado, J. Influence of an Upper Limb Isometric Task in Perceived and Performance Fatigability of Elderly Subjects: A Quasi-Experimental Study. Biology 2022, 11, 1175. [Google Scholar] [CrossRef] [PubMed]
- Schepers, M.; Giuberti, M.; Bellusci, G. Xsens MVN: Consistent Tracking of Human Motion Using Inertial Sensing; Xsens: Enschede, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Roetenberg, D.; Luinge, H.; Slycke, P. Xsens MVN: Full 6DOF Human Motion Tracking Using Miniature Inertial Sensors; Xsens: Enschede, The Netherlands, 2013; Volume 3. [Google Scholar]
- Provot, T.; Najdem, A.; Valdes-Tamayo, L.; Chiementin, X. Impact of Exhaustion Level on Tibial Acceleration Signature of Amateur Runners. Comput. Methods Biomech. Biomed. Eng. 2020, 23, S241–S243. [Google Scholar] [CrossRef]
- Yang, C.; Bouffard, J.; Srinivasan, D.; Ghayourmanesh, S.; Cantú, H.; Begon, M.; Côté, J.N. Changes in Movement Variability and Task Performance during a Fatiguing Repetitive Pointing Task. J. Biomech. 2018, 76, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Gao, G.; Li, Z.; Huan, Z.; Chen, Y.; Liang, J.; Zhou, B.; Dong, C. Human Behavior Recognition Model Based on Feature and Classifier Selection. Sensors 2021, 21, 7791. [Google Scholar] [CrossRef] [PubMed]
- Cowley, J.C.; Gates, D.H. Inter-Joint Coordination Changes during and after Muscle Fatigue. Hum. Mov. Sci. 2017, 56, 109–118. [Google Scholar] [CrossRef]
- Monjo, F.; Terrier, R.; Forestier, N. Muscle Fatigue as an Investigative Tool in Motor Control: A Review with New Insights on Internal Models and Posture-Movement Coordination. Hum. Mov. Sci. 2015, 44, 225–233. [Google Scholar] [CrossRef] [PubMed]
- McDonald, A.C.; Mulla, D.M.; Keir, P.J. Muscular and Kinematic Adaptations to Fatiguing Repetitive Upper Extremity Work. Appl. Ergon. 2019, 75, 250–256. [Google Scholar] [CrossRef]
- Tse, C.T.F.; McDonald, A.C.; Keir, P.J. Adaptations to Isolated Shoulder Fatigue during Simulated Repetitive Work. Part I: Fatigue. J. Electromyogr. Kinesiol. 2016, 29, 34–41. [Google Scholar] [CrossRef]
- Pethick, J.; Tallent, J. The Neuromuscular Fatigue-Induced Loss of Muscle Force Control. Sports 2022, 10, 184. [Google Scholar] [CrossRef]
- Thomas, S.J.; Castillo, G.C.; Topley, M.; Paul, R.W. The Effects of Fatigue on Muscle Synergies in the Shoulders of Baseball Players. Sports Health 2022, 15, 282–289. [Google Scholar] [CrossRef]
- Ortega-Auriol, P.A.; Besier, T.F.; Byblow, W.D.; McMorland, A.J.C. Fatigue Influences the Recruitment, but Not Structure, of Muscle Synergies. Front. Hum. Neurosci. 2018, 12, 217. [Google Scholar] [CrossRef]
- Palomino, D.P.; Torres Pareja, M.; Mateos, L.M.; Mendoza Láiz, N. The Isometric Muscle Contraction Tasks or Repetitive Movements to Evaluate the Effects of Fatigue. A Systematic Review. Arch. Med. Deporte 2018, 35, 326–332. [Google Scholar]
- Hunter, S.K. Sex Differences in Human Fatigability: Mechanisms and Insight to Physiological Responses. Acta Physiol. 2014, 210, 768–789. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.K. The Relevance of Sex Differences in Performance Fatigability. Med. Sci. Sports Exerc. 2016, 48, 2247–2256. [Google Scholar] [CrossRef] [PubMed]
- Hunter, S.K.; Enoka, R.M. Sex Differences in the Fatigability of Arm Muscles Depends on Absolute Force during Isometric Contractions. J. Appl. Physiol. 2001, 91, 2686–2694. [Google Scholar] [CrossRef]
- Bouffard, J.; Yang, C.; Begon, M.; Côté, J. Sex Differences in Kinematic Adaptations to Muscle Fatigue Induced by Repetitive Upper Limb Movements. Biol. Sex Differ. 2018, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Zijdewind, I.; Hyngstrom, A.; Hunter, S. Editorial: Fatigability and Motor Performance in Special and Clinical Populations. Front. Physiol. 2021, 11, 2020–2022. [Google Scholar] [CrossRef]
- Ansdell, P.; Brownstein, C.G.; Škarabot, J.; Hicks, K.M.; Howatson, G.; Thomas, K.; Hunter, S.K.; Goodall, S. Sex Differences in Fatigability and Recovery Relative to the Intensity–Duration Relationship. J. Physiol. 2019, 597, 5577–5595. [Google Scholar] [CrossRef]
- Budhota, A.; Tommasino, P.; Hussain, A.; Campolo, D. Identification of Shoulder Muscle Synergies in Healthy Subjects during an Isometric Task. IEEE Int. Conf. Rehabil. Robot 2017, 2017, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Avin, K.G.; Naughton, M.R.; Ford, B.W.; Moore, H.E.; Monitto-Webber, M.N.; Stark, A.M.; Gentile, A.J.; Law, L.A.F. Sex Differences in Fatigue Resistance Are Muscle Group Dependent. Med. Sci. Sports Exerc. 2010, 42, 1943–1950. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Characteristics | Total Sample Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p Value 1 | Effect Size Cohen’s d |
|---|---|---|---|---|---|
| Age (years) | 72.61 ± 5.23 | 72.27 ± 6.05 | 72.94 ± 4.49 | 0.727 | 0.126 |
| (65–85) | (65–85) | (65–82) | |||
| Weight (kg) | 73.18 ± 13.01 | 67.57 ± 12.37 | 78.44 ± 11.61 | 0.009 | 0.907 |
| (48–100) | (48–86.5) | (57.90–100) | |||
| Height (m) | 1.60 ± 0.08 | 1.54 ± 0.43 | 1.65 ± 0.06 | <0.001 | 2.116 |
| (1.48–1.76) | (1.48–1.64) | (1.57–1.76) | |||
| BMI (kg/m2) | 28.71 ± 4.66 | 28.69 ± 5.30 | 28.74 ± 4.15 | 0.490 | 0.695 |
| (21.57–37.94) | (21.57–37.94) | (23.42–35.61) |
| Activity Time (TTF) | X-axis | Y-axis | Z-axis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p Value 1 | Effect Size r | Total Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p value 1 | Effect Size r | Total Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p Value 2 | Effect Size Cohen´s d | |
| Baseline | −8.25 ± 1.04 (5.07–9.53) | 8.41 ± 1.11 (9.53–5.07) | 8.09 ± 0.97 (9.37–6.08) | 0.264 | 0.206 | −1.05 ± 2.47 (−4.14–6.74) | −0.66 ± 2.94 (6.74–−3.62) | −1.40 ± 1.96 (−4.14–1.97) | 0.740 | 0.064 | 4.48 ± 1.35 (1.74–7.02) | 3.99 ± 1.18 (5.77–1.74) | 4.94 ± 1.37 (7.02–1.90) | 0.048 | 0.742 |
| 10% | 8.20 ± 1.07 (5.08–9.52) | 8.40 ± 1.10 (9.52–5.08) | 8.00 ± 1.04 (9.34–6.06) | 0.202 | 0.234 | −1.20 ± 2.48 (−4.72–6.74) | −0.67 ± 2.95 (6.74–−3.61) | −1.71 ± 1.90 (−4.72–0.96) | 0.599 | 0.099 | 4.50 ± 1.37 (1.80–7.00) | 3.99 ± 1.19 (5.79–1.80) | 4.98 ± 1.40 (7.00–1.84) | 0.045 | 0.754 |
| 20% | 8.17 ± 1.05 (5.93–9.47) | 8.42 ± 0.93 (9.47–5.93) | 7.93 ± 1.12 (9.29–6.18) | 0.202 | 0.234 | −1.31 ± 2.48 (−5.48–5.83) | −0.80 ± 2.82 (5.83–−3.64) | −1.79 ± 2.07 (−5.48–1.27) | 0.654 | 0.085 | 4.51 ± 1.41 (1.45–7.03) | 4.02 ± 1.20 (5.87–1.45) | 4.96 ± 1.47 (7.03–1.66) | 0.064 | 0.691 |
| 30% | 8.08 ± 1.20 (4.97–9.38) | 8.31 ± 1.14 (9.38–4.97) | 7.86 ± 1.24 (9.30–5.67) | 0.338 | 0.177 | −1.24 ± 2.58 (−5.41–6.85) | −0.70 ± 3.04 (6.85–−3.60) | −1.75 ± 2.04 (−5.41–1.39) | 0.626 | 0.092 | 4.58 ± 1.47 (1.28–7.59) | 4.09 ± 1.23 (6.24–1.28) | 5.04 ± 1.57 (7.59–1.45) | 0.073 | 0.669 |
| 40% | 8.04 ± 1.23 (5.04–9.44) | 8.28 ± 1.10 (9.44–5.04) | 7.81 ± 1.33 (9.38–5.36) | 0.423 | 0.149 | −1.11 ± 2.56 (−5.31–6.80) | −0.47 ± 3.00 (6.80–−3.56) | −1.71 ± 1.97 (−5.31–1.38) | 0.520 | 0.121 | 4.70 ± 1.47 (1.17–7.73) | 4.24 ± 1.18 (6.21 – 1.17) | 5.13 ± 1.61 (7.73–1.33) | 0.091 | 0.629 |
| 50% | 7.99 ± 1.24 (4.93–9.43) | 8.22 ± 1.10 (9.41–4.98) | 7.78 ± 1.35 (9.43–4.93) | 0.520 | 0.121 | −1.03 ± 2.55 (−5.09–6.92) | −0.40 ± 3.06 (6.92–−3.62) | −1.63 ± 1.85 (−5.09–1.13) | 0.446 | 0.142 | 4.79 ± 1.45 (1.12–7.75) | 4.33 ± 1.16 (6.04–1.12) | 5.22 ± 1.59 (7.75–1.61) | 0.085 | 0.640 |
| 60% | 7.92 ± 1.25 (4.98–9.49) | 8.13 ± 1.09 (9.37–4.98) | 7.73 ± 1.38 (9.49–5.14) | 0.572 | 0.107 | −0.98 ± 2.49 (−4.87–6.80) | −0.38 ± 3.06 (6.80–−3.61) | −1.54 ± 1.72 (−4.87–0.81) | 0.545 | 0.114 | 4.92 ± 1.51 (1.03–8.07) | 4.47 ± 1.23 (6.11–1.03) | 5.35 ± 1.66 (8.07–1.65) | 0.105 | 0.602 |
| 70% | 7.88 ± 1.21 (4.65–9.56) | 8.03 ± 1.13 (9.33–4.78) | 7.73 ± 1.31 (9.56–4.65) | 0.599 | 0.099 | −0.93 ± 2.53 (−4.53–7.14) | −0.39 ± 3.16 (7.14–−3.70) | −1.43 ± 1.72 (−4.53–0.75) | 0.682 | 0.078 | 4.99 ± 1.51 (0.80–7.64) | 4.56 ± 1.30 (6.12–0.80) | 5.39 ± 1.61 (7.64–1.48) | 0.123 | 0.571 |
| 80% | 7.76 ± 1.27 (4.30–9.65) | 7.93 ± 1.17 (9.27–4.81) | 7.61 ± 1.38 (9.65–4.30) | 0.599 | 0.099 | −0.86 ± 2.45 (−4.13–7.01) | −0.35 ± 3.10 (7.10–−3.71) | −1.33 ± 1.57 (−4.13–0.89) | 0.861 | 0.036 | 5.19 ± 1.58 (0.84–7.94) | 4.74 ± 1.37 (6.56–0.84) | 5.61 ± 1.68 (7.94–1.61) | 0.125 | 0.568 |
| 90% | 7.68 ± 1.36 (3.77–9.61) | 7.84 ± 1.23 (9.18–4.62) | 7.53 ± 1.50 (9.61–3.77) | 0.682 | 0.078 | −0.82 ± 2.39 (−3.85–7.25) | −0.29 ± 3.11 (7.25–−3.85) | −1.31 ± 1.36 (−3.77–0.74) | 0.922 | 0.021 | 5.30 ± 1.63 (0.98–8.42) | 4.86 ± 1.40 (6.84–0.98) | 5.72 ± 1.75 (8.42–1.75) | 0.143 | 0.541 |
| 100% | 7.53 ± 1.37 (3.79–9.59) | 7.57 ± 1.28 (9.17–4.81) | 7.50 ± 1.49 (9.59–3.79) | 0.984 | 0.007 | −0.73 ± 2.28 (−3.83–6.68) | −0.17 ± 2.98 (6.68–−3.83) | −1.25 ± 1.21 (−3.54–0.65) | 0.654 | 0.085 | 5.49 ± 1.64 (1.16–8.35) | 5.19 ± 1.54 (7.77–1.16) | 5.77 ± 1.73 (8.35–1.89) | 0.328 | 0.357 |
| X-Axis | Y-Axis | Z-Axis | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample p Value 1 | Effect Size r | Women p Value 1 | Effect Size r | Men p Value 1 | Effect Size r | Total Sample p Value 1 | Effect Size r | Women p Value 1 | Effect Size r | Men p Value 1 | Effect Size r | Total Sample p Value 2 | Effect Size Cohen’s d | Women p Value 2 | Effect Size Cohen’s d | Men p Value 2 | Effect Size Cohen’s d | |
| Baseline-10%TTF | 0.100 | 0.209 | 0.691 | 0.073 | 0.079 | 0.311 | 0.183 | 0.169 | 0.820 | 0.041 | 0.148 | 0.256 | 0.416 | 0.148 | 0.968 | 0.011 | 0.378 | 0.227 |
| Baseline-20%TTF | 0.068 | 0.231 | 0.061 | 0.342 | 0.179 | 0.238 | 0.117 | 0.199 | 0.609 | 0.093 | 0.121 | 0.274 | 0.679 | 0.075 | 0.622 | 0.130 | 0.872 | 0.041 |
| Baseline-30%TTF | 0.018 | 0.301 | 0.041 | 0.373 | 0.098 | 0.293 | 0.389 | 0.109 | 0.865 | 0.031 | 0.234 | 0.210 | 0.252 | 0.210 | 0.399 | 0.225 | 0.453 | 0.192 |
| Baseline-40%TTF | 0.006 | 0.348 | 0.015 | 0.446 | 0.070 | 0.320 | 0.969 | 0.005 | 0.281 | 0.197 | 0.352 | 0.165 | 0.062 | 0.349 | 0.171 | 0.373 | 0.229 | 0.313 |
| Baseline-50%TTF | 0.003 | 0.383 | 0.005 | 0.508 | 0.070 | 0.320 | 0.597 | 0.067 | 0.307 | 0.187 | 0.717 | 0.064 | 0.020 | 0.441 | 0.111 | 0.439 | 0.105 | 0.432 |
| Baseline-60%TTF | <0.001 | 0.431 | 0.004 | 0.529 | 0.039 | 0.366 | 0.570 | 0.072 | 0.334 | 0.176 | 0.959 | 0.009 | 0.003 | 0.580 | 0.039 | 0.589 | 0.043 | 0.552 |
| Baseline-70%TTF | <0.001 | 0.465 | 0.003 | 0.550 | 0.034 | 0.375 | 0.505 | 0.085 | 0.427 | 0.145 | 0.796 | 0.046 | 0.002 | 0.606 | 0.047 | 0.561 | 0.017 | 0.673 |
| Baseline-80%TTF | <0.001 | 0.478 | 0.002 | 0.570 | 0.023 | 0.402 | 0.410 | 0.105 | 0.460 | 0.135 | 0.569 | 0.101 | <0.001 | 0.704 | 0.025 | 0.649 | 0.008 | 0.757 |
| Baseline-90%TTF | <0.001 | 0.500 | 0.001 | 0.591 | 0.020 | 0.411 | 0.367 | 0.114 | 0.460 | 0.135 | 0.501 | 0.119 | <0.001 | 0.746 | 0.014 | 0.726 | 0.009 | 0.746 |
| Baseline-100%TTF | <0.001 | 0.498 | 0.001 | 0.591 | 0.044 | 0.357 | 0.299 | 0.132 | 0.427 | 0.145 | 0.501 | 0.119 | <0.001 | 0.851 | 0.002 | 0.954 | 0.010 | 0.737 |
| X-Axis | Y-Axis | Z-Axis | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample p Value 1 | Effect Size r | Women p Value 1 | Effect Size r | Men p Value 1 | Effect Size r | Total Sample p Value 1 | Effect Size r | Women p Value 1 | Effect Size r | Men p Value 1 | Effect Size r | Total Sample p Value2 | Effect Size Cohen´s d | Women p Value 2 | Effect Size Cohen´s d | Men p Value 2 | Effect Size Cohen´s d | |
| 10–20%TTF | 0.117 | 0.199 | 0.156 | 0.259 | 0.278 | 0.192 | 0.256 | 0.144 | 0.496 | 0.125 | 0.379 | 0.155 | 0.902 | 0.022 | 0.546 | 0.160 | 0.721 | 0.091 |
| 20–30%TTF | 0.085 | 0.219 | 0.088 | 0.311 | 0.438 | 0.137 | 0.272 | 0.139 | 0.460 | 0.135 | 0.438 | 0.137 | 0.082 | 0.323 | 0.303 | 0.276 | 0.172 | 0.359 |
| 30–40%TTF | 0.256 | 0.144 | 0.394 | 0.156 | 0.379 | 0.155 | 0.153 | 0.182 | 0.211 | 0.228 | 0.535 | 0.110 | 0.007 | 0.524 | 0.066 | 0.515 | 0.033 | 0.587 |
| 40–50%TTF | 0.104 | 0.207 | 0.031 | 0.394 | 0.836 | 0.037 | 0.033 | 0.271 | 0.140 | 0.270 | 0.134 | 0.265 | 0.004 | 0.558 | 0.051 | 0.552 | 0.045 | 0.546 |
| 50–60%TTF | 0.005 | 0.358 | 0.002 | 0.570 | 0.255 | 0.201 | 0.108 | 0.204 | 0.691 | 0.073 | 0.063 | 0.329 | <0.001 | 0.917 | 0.001 | 1.053 | 0.006 | 0.794 |
| 60–70%TTF | 0.030 | 0.276 | 0.017 | 0.435 | 0.501 | 0.119 | 0.117 | 0.199 | 0.776 | 0.052 | 0.070 | 0.320 | 0.239 | 0.216 | 0.164 | 0.380 | 0.637 | 0.120 |
| 70–80%TTF | 0.002 | 0.403 | 0.009 | 0.477 | 0.063 | 0.329 | 0.126 | 0.194 | 0.570 | 0.104 | 0.179 | 0.238 | <0.001 | 0.806 | 0.007 | 0.809 | 0.006 | 0.790 |
| 80–90%TTF | 0.075 | 0.226 | 0.041 | 0.373 | 0.605 | 0.091 | 0.308 | 0.129 | 0.281 | 0.197 | 0.796 | 0.046 | 0.007 | 0.523 | 0.036 | 0.598 | 0.091 | 0.451 |
| 90–100%TTF | 0.040 | 0.261 | 0.020 | 0.425 | 0.679 | 0.073 | 0.367 | 0.114 | 0.394 | 0.156 | 0.605 | 0.091 | 0.010 | 0.493 | 0.014 | 0.728 | 0.382 | 0.225 |
| %TTF | Total Sample | Women | Men |
|---|---|---|---|
| Baseline | −0.851 ** 95% CI [−0.926, −0.712] | −0.821 ** 95% CI [−0.938, −0.533] | −0.909 ** 95% CI [−0.968, −0.753] |
| 10% | −0.853 ** 95% CI [−0.927, −0.715] | −0.811 ** 95% CI [−0.934, −0.512] | −0.876 ** 95% CI [−0.956, −0.673] |
| 20% | −0.869 ** 95% CI [−0.935, −0.744] | −0.854 ** 95% CI [−0.950, −0.608] | −0.874 ** 95% CI [−0.955, −0.668] |
| 30% | −0.882 ** 95% CI [−0.941, −0.768] | −0.914 ** 95% CI [−0.971, −0.756] | −0.888 ** 95% CI [−0.960, −0.701] |
| 40% | −0.877 ** 95% CI [−0.939, −0.759] | −0.871 ** 95% CI [−0.956, −0.648] | −0.915 ** 95% CI [−0.970, −0.768] |
| 50% | −0.876 ** 95% CI [−0.938, −0.757] | −0.850 ** 95% CI [−0.949, −0.599] | −0.918 ** 95% CI [−0.971, −0.775] |
| 60% | −0.874 ** 95% CI [−0.937, −0.753] | −0.846 ** 95% CI [−0.946, −0.583] | −0.929 ** 95% CI [−0.975, −0.804] |
| 70% | −0.825 ** 95% CI [−0.912, −0.666] | −0.736 ** 95% CI [−0.906, −0.360] | −0.941 ** 95% CI [−0.979, −0.835] |
| 80% | −0.864 ** 95% CI [−0.932, −0.735] | −0.782 ** 95% CI [−0.924, −0.451] | −0.941 ** 95% CI [−0.979, −0.835] |
| 90% | −0.848 ** 95% CI [−0.924, −0.706] | −0.664 ** 95% CI [−0.877, −0.230] | −0.971 ** 95% CI [−0.990, −0.917] |
| 100% | −0.882 ** 95% CI [−0.941, −0.768] | −0.739 ** 95% CI [−0.907, −0.365] | −0.979 ** 95% CI [−0.992, −0.939] |
| Total Sample Mean ± SD (Range) | Women Mean ± SD (Range) | Men Mean ± SD (Range) | p Value 1 | Effect Size Cohen’s d | |
|---|---|---|---|---|---|
| TTF (sec) | 474.52 ± 301.41 | 369.60 ± 228.79 | 572.88 ± 333.95 | 0.037 | 0.706 |
| (128–1443) | (128-1012) | (286–1443) |
| Axis Cut-off | Men |
|---|---|
| X 10% | 0.524 * 95% CI [0.022, 0.815] |
| X 20% | 0.726 ** 95% CI [0.347, 0.902] |
| X 30% | 0.656 ** 95% CI [0.222, 0.873] |
| X 40% | 0.547 * 95% CI [0.054, 0.825] |
| X 50% | 0.635 ** 95% CI [0.188, 0.864] |
| X 60% | 0.503 * 95% CI [−0.006, 0.805] |
| Y 10% | −0.509 * 95% CI [−0.808, −0.001] |
| Y 30% | −0.603 * 95% CI [−0.850, −0.137] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Migueis, H.; Martínez-Jiménez, E.M.; Casado-Hernández, I.; Dias, A.; Monteiro, A.J.; Martins, R.B.; Bernardes, J.M.; López-López, D.; Gómez-Salgado, J. Upper-Limb Kinematic Behavior and Performance Fatigability of Elderly Participants Performing an Isometric Task: A Quasi-Experimental Study. Bioengineering 2023, 10, 526. https://doi.org/10.3390/bioengineering10050526
Silva-Migueis H, Martínez-Jiménez EM, Casado-Hernández I, Dias A, Monteiro AJ, Martins RB, Bernardes JM, López-López D, Gómez-Salgado J. Upper-Limb Kinematic Behavior and Performance Fatigability of Elderly Participants Performing an Isometric Task: A Quasi-Experimental Study. Bioengineering. 2023; 10(5):526. https://doi.org/10.3390/bioengineering10050526
Chicago/Turabian StyleSilva-Migueis, Helena, Eva María Martínez-Jiménez, Israel Casado-Hernández, Adriano Dias, Ana Júlia Monteiro, Rodrigo B. Martins, João Marcos Bernardes, Daniel López-López, and Juan Gómez-Salgado. 2023. "Upper-Limb Kinematic Behavior and Performance Fatigability of Elderly Participants Performing an Isometric Task: A Quasi-Experimental Study" Bioengineering 10, no. 5: 526. https://doi.org/10.3390/bioengineering10050526