

The Effectiveness of Calcium Phosphates in the Treatment of Dentinal Hypersensitivity: A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Screening and Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Synthesis of Results
3. Results
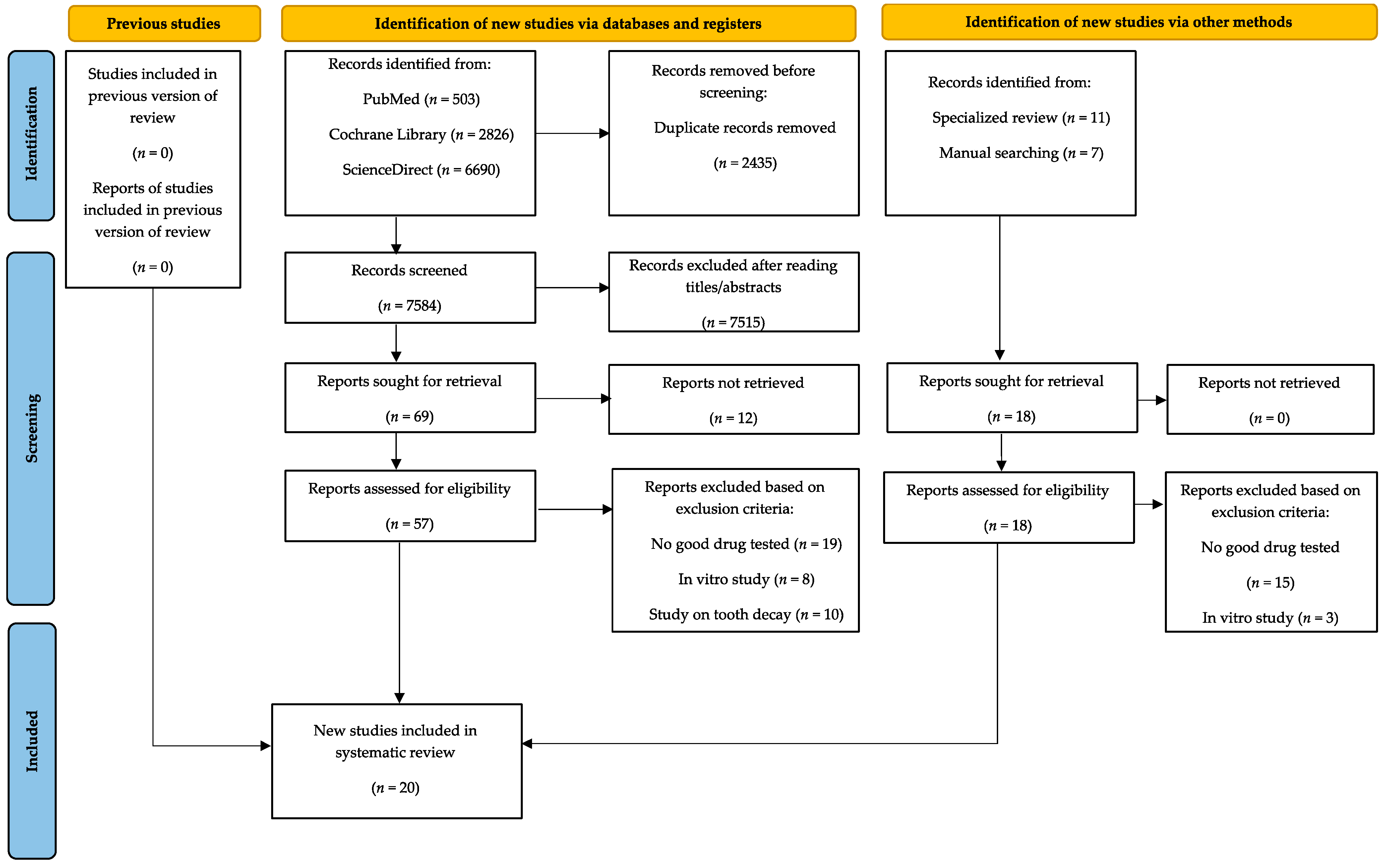
3.1. Study Selection
3.2. Description of Included Studies
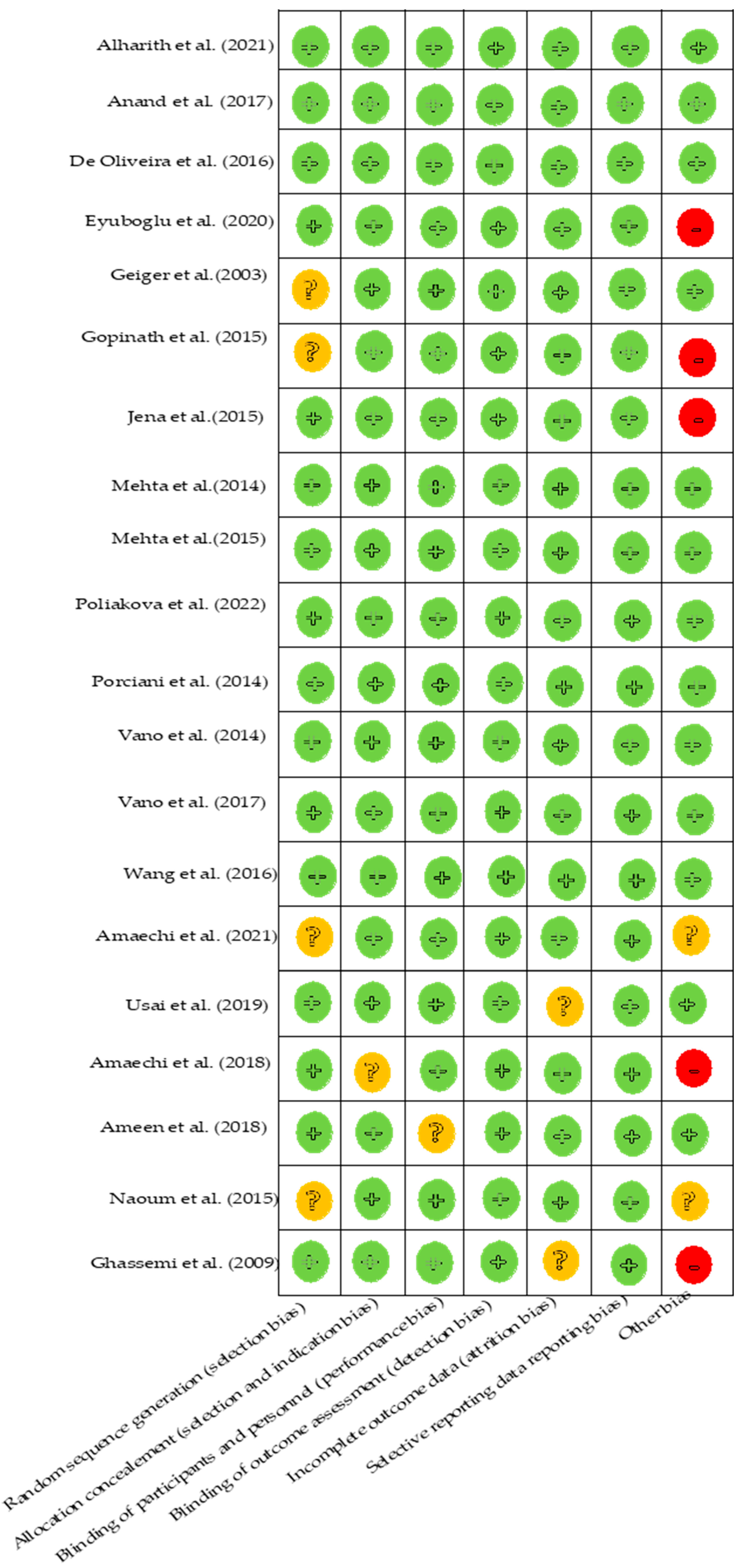
3.3. Analysis of the Risks of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Addy, M. Etiology and clinical implications of dentine hypersensitivity. Dent. Clin. N. Am. 1990, 34, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Holland, G.R.; Narhi, M.N.; Addy, M.; Gangarosa, L.; Orchardson, R. Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J. Clin. Periodontol. 1997, 24, 808–813. [Google Scholar] [CrossRef]
- Mantzourani, M.; Sharma, D. Dentine sensitivity: Past, present and future. J. Dent. 2013, 41, S3–S17. [Google Scholar] [CrossRef]
- Bekes, K.; Hirsch, C. What is known about the influence of dentine hypersensitivity on oral health-related quality of life? Clin. Oral Investig. 2013, 17 (Suppl. 1), S45–S51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapp, R.; Avery, J.K.; Strachan, D.S. Possible Role of the Acetylcholinesterase in Neural Conduction within the Dental Pulp; University of Alabama Press: Birmingham, UK, 1968. [Google Scholar]
- West, N.; Lussi, A.; Seong, J.; Hellwig, E. Dentin hypersensitivity: Pain mechanisms and aetiology of exposed cervical dentin. Clin. Oral Investig. 2013, 17, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Brannstrom, M. A hydrodynamic mechanism in the transmission of pain-producing stimuli through the dentin. In Sensory Mechanisms in Dentine; Pergamon Press: Oxford, UK, 1963; pp. 73–79. [Google Scholar]
- Brannstrom, M. The surface of sensitive dentine. An experimental study using replication. Odontol. Rev. 1965, 16, 293–299. [Google Scholar]
- Brannstrom, M. Sensitivity of dentine. Oral Surg. Oral Med. Oral Pathol. 1966, 21, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Martins, C.C.; Firmino, R.T.; Riva, J.J.; Ge, L.; Carrasco-Labra, A.; Brignardello-Petersen, R.; Colunga-Lozano, L.E.; Granville-Garcia, A.F.; Costa, F.O.; Yepes-Nunez, J.J.; et al. Desensitizing Toothpastes for Dentin Hypersensitivity: A Network Meta-analysis. J. Dent. Res. 2020, 99, 514–522. [Google Scholar] [CrossRef]
- Shiau, H.J. Dentin hypersensitivity. J. Evid.-Based Dent. Pract. 2012, 12, 220–228. [Google Scholar] [CrossRef]
- Karim, B.F.; Gillam, D.G. The efficacy of strontium and potassium toothpastes in treating dentine hypersensitivity: A systematic review. Int. J. Dent. 2013, 2013, 573258. [Google Scholar] [CrossRef] [Green Version]
- Sharif, M.O.; Iram, S.; Brunton, P.A. Effectiveness of arginine-containing toothpastes in treating dentine hypersensitivity: A systematic review. J. Dent. 2013, 41, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Cruz, J.; Stout, J.R.; Heaton, L.J.; Wataha, J.C.; Northwest, P. Dentin hypersensitivity and oxalates: A systematic review. J. Dent. Res. 2011, 90, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Magno, M.B.; Nascimento, G.C.R.; Da Penha, N.K.S.; Pessoa, O.F.; Loretto, S.C.; Maia, L.C. Difference in effectiveness between strontium acetate and arginine-based toothpastes to relieve dentin hypersensitivity. A systematic review. Am. J. Dent. 2015, 28, 40–44. [Google Scholar] [PubMed]
- Gendreau, L.; Barlow, A.P.; Mason, S.C. Overview of the clinical evidence for the use of NovaMin in providing relief from the pain of dentin hypersensitivity. J. Clin. Dent. 2011, 22, 90–95. [Google Scholar]
- Zhu, M.; Li, J.; Chen, B.; Mei, L.; Yao, L.; Tian, J.; Li, H. The Effect of Calcium Sodium Phosphosilicate on Dentin Hypersensitivity: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0140176. [Google Scholar] [CrossRef] [PubMed]
- de Melo Alencar, C.; de Paula, B.L.F.; Guanipa Ortiz, M.I.; Barauna Magno, M.; Martins Silva, C.; Cople Maia, L. Clinical efficacy of nano-hydroxyapatite in dentin hypersensitivity: A systematic review and meta-analysis. J. Dent. 2019, 82, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Marto, C.M.; Baptista Paula, A.; Nunes, T.; Pimenta, M.; Abrantes, A.M.; Pires, A.S.; Laranjo, M.; Coelho, A.; Donato, H.; Botelho, M.F.; et al. Evaluation of the efficacy of dentin hypersensitivity treatments—A systematic review and follow-up analysis. J. Oral Rehabil. 2019, 46, 952–990. [Google Scholar] [CrossRef]
- Lee, B.S.; Chang, C.W.; Chen, W.P.; Lan, W.H.; Lin, C.P. In vitro study of dentin hypersensitivity treated by Nd:YAP laser and bioglass. Dent. Mater. 2005, 21, 511–519. [Google Scholar] [CrossRef]
- Miglani, S.; Aggarwal, V.; Ahuja, B. Dentin hypersensitivity: Recent trends in management. J. Conserv. Dent. 2010, 13, 218–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moraschini, V.; da Costa, L.S.; Dos Santos, G.O. Effectiveness for dentin hypersensitivity treatment of non-carious cervical lesions: A meta-analysis. Clin. Oral Investig. 2018, 22, 617–631. [Google Scholar] [CrossRef]
- Ray, R.D.; Ward, A.A., Jr. A preliminary report on studies of basic calcium phosphate in bone replacement. Surg. Forum 1951, 429–434. [Google Scholar]
- Chow, L.C. Next generation calcium phosphate-based biomaterials. Dent. Mater. J. 2009, 28, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daculsi, G.; Laboux, O.; Malard, O.; Weiss, P. Current state of the art of biphasic calcium phosphate bioceramics. J. Mater. Sci. Mater. Med. 2003, 14, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Rajula, M.P.B.; Narayanan, V.; Venkatasubbu, G.D.; Mani, R.C.; Sujana, A. Nano-hydroxyapatite: A Driving Force for Bone Tissue Engineering. J. Pharm. Bioallied Sci. 2021, 13, S11–S14. [Google Scholar] [CrossRef]
- Martins, C.C.; Riva, J.J.; Firmino, R.T.; Schunemann, H.J. Formulations of desensitizing toothpastes for dentin hypersensitivity: A scoping review. J. Appl. Oral Sci. 2022, 30, e20210410. [Google Scholar] [CrossRef]
- Zhou, J.; Chiba, A.; Scheffel, D.L.; Hebling, J.; Agee, K.; Niu, L.N.; Tay, F.R.; Pashley, D.H. Effects of a Dicalcium and Tetracalcium Phosphate-Based Desensitizer on In Vitro Dentin Permeability. PLoS ONE 2016, 11, e0158400. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Polyakova, M.; Sokhova, I.; Doroshina, V.; Arakelyan, M.; Novozhilova, N.; Babina, K. The Effect of Toothpastes Containing Hydroxyapatite, Fluoroapatite, and Zn-Mg-hydroxyapatite Nanocrystals on Dentin Hypersensitivity: A Randomized Clinical Trial. J. Int. Soc. Prev. Community Dent. 2022, 12, 252–259. [Google Scholar] [CrossRef]
- Alharith, D.N.; Al-Omari, M.; Almnea, R.; Basri, R.; Alshehri, A.H.; Al-Nufiee, A.A. Clinical efficacy of single application of plain nano-hydroxyapatite paste in reducing dentine hypersensitivity—A randomized clinical trial. Saudi Endod. J. 2021, 11, 24. [Google Scholar]
- Amaechi, B.T.; Lemke, K.C.; Saha, S.; Luong, M.N.; Gelfond, J. Clinical efficacy of nanohydroxyapatite-containing toothpaste at relieving dentin hypersensitivity: An 8 weeks randomized control trial. BDJ Open 2021, 7, 23. [Google Scholar] [CrossRef]
- Eyüboğlu, G.; Naiboğlu, P. Clinical efficacy of different dentin desensitizers. Oper. Dent. 2020, 45, E317–E333. [Google Scholar] [CrossRef]
- Usai, P.; Campanella, V.; Sotgiu, G.; Spano, G.; Pinna, R.; Eramo, S.; Saderi, L.; Garcia-Godoy, F.; Derchi, G.; Mastandrea, G.; et al. Effectiveness of Calcium Phosphate Desensitising Agents in Dental Hypersensitivity Over 24 Weeks of Clinical Evaluation. Nanomaterials 2019, 9, 1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amaechi, B.T.; Lemke, K.C.; Saha, S.; Gelfond, J. Clinical Efficacy in Relieving Dentin Hypersensitivity of Nanohydroxyapatite-containing Cream: A Randomized Controlled Trial. Open Dent. J. 2018, 12, 572–585. [Google Scholar] [CrossRef]
- Ameen, S.; Niazy, M.; El-yassaky, M.; Jamil, W.; Attia, M. Clinical Evaluation of Nano-Hydroxyapatite as Dentin Desensitizer. Al-Azhar Dent. J. Girls 2018, 5, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Anand, S.; Rejula, F.; Sam, J.V.G.; Christaline, R.; Nair, M.G.; Dinakaran, S. Comparative Evaluation of Effect of Nano-hydroxyapatite and 8% Arginine Containing Toothpastes in Managing Dentin Hypersensitivity: Double Blind Randomized Clinical Trial. Acta Med. (Hradec Kral.) 2017, 60, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Vano, M.; Derchi, G.; Barone, A.; Pinna, R.; Usai, P.; Covani, U. Reducing dentine hypersensitivity with nano-hydroxyapatite toothpaste: A double-blind randomized controlled trial. Clin. Oral Investig. 2018, 22, 313–320. [Google Scholar] [CrossRef]
- Douglas de Oliveira, D.W.; Oliveira, E.S.; Mota, A.F.; Pereira, V.H.; Bastos, V.O.; Gloria, J.C.; Goncalves, P.F.; Flecha, O.D. Effectiveness of Three Desensitizing Dentifrices on Cervical Dentin Hypersensitivity: A Pilot Clinical Trial. J. Int. Acad. Periodontol. 2016, 18, 57–65. [Google Scholar] [PubMed]
- Wang, L.; Magalhaes, A.C.; Francisconi-Dos-Rios, L.F.; Calabria, M.P.; Araujo, D.; Buzalaf, M.; Lauris, J.; Pereira, J.C. Treatment of Dentin Hypersensitivity Using Nano-Hydroxyapatite Pastes: A Randomized Three-Month Clinical Trial. Oper. Dent. 2016, 41, E93–E101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopinath, N.M.; John, J.; Nagappan, N.; Prabhu, S.; Kumar, E.S. Evaluation of Dentifrice Containing Nano-hydroxyapatite for Dentinal Hypersensitivity: A Randomized Controlled Trial. J. Int. Oral Health 2015, 7, 118–122. [Google Scholar] [PubMed]
- Jena, A.; Shashirekha, G. Comparison of efficacy of three different desensitizing agents for in-office relief of dentin hypersensitivity: A 4 weeks clinical study. J. Conserv. Dent. 2015, 18, 389–393. [Google Scholar] [CrossRef] [Green Version]
- Mehta, D.; Gowda, V.; Finger, W.J.; Sasaki, K. Randomized, placebo-controlled study of the efficacy of a calcium phosphate containing paste on dentin hypersensitivity. Dent. Mater. 2015, 31, 1298–1303. [Google Scholar] [CrossRef] [PubMed]
- Naoum, S.J.; Lenard, A.; Martin, F.E.; Ellakwa, A. Enhancing Fluoride Mediated Dentine Sensitivity Relief through Functionalised Tricalcium Phosphate Activity. Int. Sch. Res. Not. 2015, 2015, 905019. [Google Scholar] [CrossRef]
- Mehta, D.; Gowda, V.S.; Santosh, A.; Finger, W.J.; Sasaki, K. Randomized controlled clinical trial on the efficacy of dentin desensitizing agents. Acta Odontol. Scand. 2014, 72, 936–941. [Google Scholar] [CrossRef]
- Porciani, P.F.; Chazine, M.; Grandini, S. A clinical study of the efficacy of a new chewing gum containing calcium hydroxyapatite in reducing dentin hypersensitivity. J. Clin. Dent. 2014, 25, 32–36. [Google Scholar] [PubMed]
- Vano, M.; Derchi, G.; Barone, A.; Covani, U. Effectiveness of nano-hydroxyapatite toothpaste in reducing dentin hypersensitivity: A double-blind randomized controlled trial. Quintessence Int. 2014, 45, 703–711. [Google Scholar] [CrossRef]
- Ghassemi, A.; Hooper, W.; Winston, A.E.; Sowinski, J.; Bowman, J.; Sharma, N. Effectiveness of a baking soda toothpaste delivering calcium and phosphate in reducing dentinal hypersensitivity. J. Clin. Dent. 2009, 20, 203–210. [Google Scholar]
- Geiger, S.; Matalon, S.; Blasbalg, J.; Tung, M.; Eichmiller, F.C. The clinical effect of amorphous calcium phosphate (ACP) on root surface hypersensitivity. Oper. Dent. 2003, 28, 496–500. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behzadi, S.; Mohammadi, Y.; Rezaei-Soufi, L.; Farmany, A. Occlusion effects of bioactive glass and hydroxyapatite on dentinal tubules: A systematic review. Clin. Oral. Investig. 2022, 26, 6061–6078. [Google Scholar] [CrossRef]
- Gul, H.; Ghaffar, M.A.; Kaleem, M.; Khan, A.S. Hydroxyapatite, a potent agent to reduce dentin hypersensitivity. J. Pak. Med. Assoc. 2021, 71, 2604–2610. [Google Scholar] [CrossRef]
- Limeback, H.; Enax, J.; Meyer, F. Clinical Evidence of Biomimetic Hydroxyapatite in Oral Care Products for Reducing Dentin Hypersensitivity: An Updated Systematic Review and Meta-Analysis. Biomimetics 2023, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.H.; Kim, Y.K.; Myung, S.K. Desensitizing toothpaste versus placebo for dentin hypersensitivity: A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 131–141. [Google Scholar] [CrossRef]
- Yang, Z.Y.; Wang, F.; Lu, K.; Li, Y.H.; Zhou, Z. Arginine-containing desensitizing toothpaste for the treatment of dentin hypersensitivity: A meta-analysis. Clin. Cosmet. Investig. Dent. 2016, 8, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Hu, M.L.; Zheng, G.; Zhang, Y.D.; Yan, X.; Li, X.C.; Lin, H. Effect of desensitizing toothpastes on dentine hypersensitivity: A systematic review and meta-analysis. J. Dent. 2018, 75, 12–21. [Google Scholar] [CrossRef]
- Cunha-Cruz, J.; Zeola, L.F. Limited Evidence Suggests That Many Types of Desensitizing Toothpaste May Reduce Dentin Hypersensitivity, but Not the Ones With Strontium or Amorphous Calcium Phosphate. J. Evid.-Based Dent. Pract. 2019, 19, 101337. [Google Scholar] [CrossRef] [PubMed]
- Zang, P.; Parkinson, C.; Hall, C.; Wang, N.; Jiang, H.; Zhang, J.; Du, M. A Randomized Clinical Trial Investigating the Effect of Particle Size of Calcium Sodium Phosphosilicate (CSPS) on the Efficacy of CSPS-containing Dentifrices for the Relief of Dentin Hypersensitivity. J. Clin. Dent. 2016, 27, 54–60. [Google Scholar]
- Machado, A.C.; Maximiano, V.; Yoshida, M.L.; Freitas, J.G.; Mendes, F.M.; Aranha, A.C.C.; Scaramucci, T. Efficacy of a calcium-phosphate/fluoride varnish and ionomeric sealant on cervical dentin hypersensitivity: A randomized, double-blind, placebo-controlled clinical study. J. Oral Rehabil. 2022, 49, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Alencar, C.D.; Ortiz, M.I.; Silva, F.A.; Alves, E.B.; Araujo, J.L.; Silva, C.M. Effect of nanohydroxyapatite associated with photobiomodulation in the control of dentin hypersensitivity: A randomized, double-blind, placebo-controlled clinical trial. Am. J. Dent. 2020, 33, 138–144. [Google Scholar]
- Shetty, S.; Kohad, R.; Yeltiwar, R. Hydroxyapatite as an in-office agent for tooth hypersensitivity: A clinical and scanning electron microscopic study. J. Periodontol. 2010, 81, 1781–1789. [Google Scholar] [CrossRef]
- Demetriou, C.; Hu, L.; Smith, T.O.; Hing, C.B. Hawthorne effect on surgical studies. ANZ J. Surg. 2019, 89, 1567–1576. [Google Scholar] [CrossRef]
- Colloca, L. The Placebo Effect in Pain Therapies. Ann. Rev. Pharmacol. Toxicol. 2019, 59, 191–211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pubmed (filters applied: Randomized Control Trial, Human) | (“Dentin Sensitivity” [Mesh] OR Sensitivities, Dentin OR Sensitivity, Dentin OR Dentine Hypersensitivity OR Dentine Hypersensitivities OR Hypersensitivities, Dentine OR Hypersensitivity, Dentine OR Dentine Sensitivity OR Dentine Sensitivities OR Sensitivities, Dentine OR Sensitivity, Dentine OR Tooth Sensitivity OR Sensitivities, Tooth OR Sensitivity, Tooth OR Tooth Sensitivities OR Dentin Hypersensitivity OR Dentin Hypersensitivities OR Hypersensitivities, Dentin OR Hypersensitivity, Dentin) AND (“Dentin Desensitizing Agents” [Mesh] OR Agents, Dentin Desensitizing OR Desensitizing Agents, Dentin OR “Tooth Remineralization” [Mesh]) AND (“Calcium Phosphates” [Mesh] OR dicalcium phosphate OR calcium monohydrogen phosphate dihydrate OR dicalcium phosphate dihydrate OR dibasic calcium phosphate dihydrate OR calcium phosphate, dihydrate OR calcium phosphate, dibasic OR dicalcium phosphate anhydrous OR brushite OR morphous calcium phosphate OR nHAC composite OR “Hydroxyapatites” [MeSH Terms] OR Hydroxyapatite Derivatives) |
| Cochrane library (All text) | Dentine Hypersensitivity OR Tooth Sensitivities OR Agents Dentin Desensitizing OR Remineralization tooth AND dicalcium phosphate OR calcium monohydrogen phosphate dihydrate OR dicalcium phosphate dihydrate OR dibasic calcium phosphate dihydrate OR calcium phosphates OR dihydrate calcium phosphate OR brushite OR Hydroxyapatite Derivatives OR Amorphous calcium phosphate OR nHAC composite |
| Embase (filters applied: Human, controlled study) | (‘dentine hypersensitivity’/exp OR ‘dentine hypersensitivity’ OR ((‘dentine’/exp OR dentine) AND (‘hypersensitivity’/exp OR hypersensitivity)) OR ‘tooth sensitivities’ OR ((‘tooth’/exp OR tooth) AND sensitivities) OR ‘agents dentin desensitizing’ OR (agents AND (‘dentin’/exp OR dentin) AND desensitizing) OR ‘remineralization tooth and dicalcium phosphate or calcium monohydrogen phosphate dihydrate‘ OR ((‘remineralization’/exp OR remineralization) AND tooth and dicalcium AND phosphate or AND calcium AND monohydrogen AND (‘phosphate’/exp OR phosphate) AND dihydrate) OR ‘dicalcium phosphate dihydrate‘ OR (dicalcium AND (‘phosphate’/exp OR phosphate) AND dihydrate) OR ‘dibasic calcium phosphate dihydrate‘ OR (dibasic AND (‘calcium’/exp OR calcium) AND (‘phosphate’/exp OR phosphate) AND dihydrate) OR ‘calcium phosphates’/exp OR ‘calcium phosphates’ OR ((‘calcium’/exp OR calcium) AND (‘phosphates’/exp OR phosphates)) OR ‘dihydrate calcium phosphate ‘ OR (dihydrate AND (‘calcium’/exp OR calcium) AND phosphate) OR ‘brushite’/exp OR brushite OR ‘hydroxyapatite derivatives’ OR ((‘hydroxyapatite’/exp OR hydroxyapatite) AND derivatives) OR ‘amorphous calcium phosphate‘ OR (amorphous AND (‘calcium’/exp OR calcium) AND phosphate) OR ‘nhac composite’ OR (nhac AND (‘composite’/exp OR composite))) AND ([controlled clinical trial]/lim OR [randomized controlled trial]/lim) |
| Author, Year, Country | Participants (ST) | Age Range Mean Age (SD) | Study Design | Study Group (n) | Evaluation Method | Results |
|---|---|---|---|---|---|---|
| Poliakova et al., 2022, Russia [30] | 30 (NR) | 35–45 years 37.5 (2) | RCT, DB | G1(n = 10): 20% n-HA paste; G2 (n = 10): nZnMgHA paste; G3 (n = 10): nFAP paste Toothbrushes twice daily for a month | Schiff Index values of CAS at baseline (T0) and after 2 (T1) and 4 (T2) weeks | At 4 weeks the Schiff Index score of 20% n-HA decreased significantly compared to baseline. |
| Alharith et al., 2021, Saudi Arabie [31] | 63 (126) | 18–60 years 39 (NR) | RCT, DB | G1 (n = 21): 15% n-HA paste; G2 (n = 21): fluoride paste; G3 (n = 21): placebo Single application of the paste at the baseline visit and 1 week follow up visit | VAS scores of TS and CAS evaluated at baseline (T0), immediately after paste application (T1), and after 1 week (T2) | A statistically significant reduction in VAS scores of TS and CAS tests from T0–T1 and T0–T2. Single application of n-HA paste significantly reduces DH. |
| Amaechi et al., 2021, USA [32] | 85 (NR) | 18–80 years 50.8 (11.4) | RCT, DB | G1 (n = 22): 10% n-HA; G2 (n = 19): 15% n-HA; G3 (n = 24): 10% n-HA + 5% Potassium Nitrate; G4 (n = 20): 15% SCPS Toothbrush during 2 min twice a day for 8 weeks | VAS scores of CAS and cold test at baseline (T0), 2 weeks (T1), 4 weeks (T2), 6 weeks (T3), and 8 weeks (T4). | All concentrations of n-HA showed a significant decrease in VAS scores at each time point. |
| Eyuboglu et al., 2020, Turkey [33] | 40 (121) | 18–65 years 41.35 (NR) | RCT, DB | G1 (n = 10; n * = 21): TTCP/DCPA; G2 (n = 10; n * = 36): Sodium Fluoride 5%, TCP Xylitol; G3 (n = 10; n * = 33): SR Monomer Matrix + 2-hydroxyethyl methacrylate; G4 (n = 10; n * = 31): 2-hydroxyethyl methacrylate + glutaraldehyde. One application according to manufacturer’s instruction | VAS score of TS and CAS evaluated at baseline (T0), immediately after application (T1), after 1 day (T2), after 2 weeks (T3) and after 4 weeks (T4) | TTCP/DCPA showed a significant difference between T0 and T1 and a significantly lower CAS score at T4 than T2 and T3. |
| Usai et al., 2019, Italy [34] | 105 (210–420) | 20–50 years 43–50 (NR) | RCT, DB | G1 (n = 35): TTCP/DCPA 30 s application; G2 (n = 35): DD (premixed n-HAP alcohol-based gel) 45 s application; G3 (n = 35): BWE (premixed n-HAP water-based gel) 10 min application | VAS scores of TS and CAS were recorded at baseline (T0), immediately after (T1), at 1 week (T2), 4 weeks (T2), 12 weeks (T3) and 24 weeks (T4). | TTCP/DCPA paste showed a statistically significant decrease in DH after 24 weeks in comparison to T0. |
| Amaechi et al., 2018, USA [35] | 50 (NR) | 18–80 years 45.47 (13) | RCT, DB | G1 (n = 25): 20%n-HA; G2 (n = 25): 20% Silica. One application during 5 min after the 2 min before-bed brushing teeth and water rinsing. | VAS scores of CAS and cold stimulation at baseline (T0), 2 weeks (T1), 4 weeks (T2), 6 weeks (T3) and 8 weeks (T4) | VAS score of CAS indicated significant reduction in DH at each time point with either n-HAP. |
| Ameen et al., 2018, Egypt [36] | 10 (40) | 20–45 years (NR) | RCT, DB | G1 (n * = 10): 15%n-HA + 1%NaF; G2 (n * = 10): 15%n-HA; G3 (n * = 10): 25%n-HA + 1%NaF; G4 (n * = 10): 25%n-HA. Four applications during 1 min at T0, 1 day, 1 week, 2 weeks and 4 weeks | Schiff index values for TS, CAS and Cold stimulation were evaluated at baseline (T0), 1 day (T1), 1 week (T2), 2 weeks (T3) and 4 weeks (T4) | n-HA molecules showed significant effects on DH at T1 compared to T0. The level of the Schiff index was back to 0 for all groups after 2 weeks. |
| Anand et al., 2018, India [37] | 60 (60) | 18–50 years 42.33 (7.58) | RCT, DB | G1 (n = 30): 8% arginine paste; G2 (n = 30): 1% n-HA paste. One application of 1 cm of toothpaste directly to the sensitive site of the selected tooth, then brushing for two minutes twice a day for 4 weeks | Amperage values were recorded at baseline, 5 min, 1 and 4 weeks with Digitest II (PARKELL, Inc., New York, NY. USA) | n-HA containing toothpastes provided a statistically significant reduction in DH, 5 min, 1 and 4 weeks after application. |
| Vano et al., 2017, Italy [38] | 105 (NR) | 20–70 years (NR) | RCT, DB | G1 (n = 35): 2% n-HA gel paste; G2 (n = 35): fluoride gel paste; G3 (n = 35): placebo, 10 min application twice a day during 4 weeks | VAS scores for TS and CAS were evaluated at baseline (T0) and after 2(T1) and 4(T2) weeks | n-HA in gel toothpaste significantly reduced the DH between baseline and 4 weeks |
| De Oliveira et al., 2016, Brazil [39] | 8 (138) | 22–48 years 29.5 (NR) | RCT, DB | G1 (n * = 33): Strontium acetate/calcium carbonate 60 s application; G2 (n * = 31): Calcium Carbonate/8% Arginine 3 s application by repeating 1 time the procedure; G3 (n * = 39): n-HA 10 s application with rest of 5 min; G4 (n * = 35): toothpaste without fluoride, 60 s application | VAS scores of CAS and cold stimulus with tetrafluoroethane were evaluated at baseline (T0), immediately after paste application (T1), after 24 h (T2) and after 30 days (T3). | n-HA showed significant difference for CAS and cold test between T0 and T3 days. |
| Wang et al., 2016, Brazil [40] | 28 (137) | 18–60 years (NR) | RCT, DB | G1 (n * = 31): 20%n-HA paste + NaF; 9000 ppm F; G2 (n * = 22): 20%n-HA + home-care pastes (10% HA, potassium nitrate, and NaF; 900 ppm F); G3 (n * = 28): 8% arginine + home-care toothpaste (8% arginine, sodium monofluorophosphate, 1450 ppm F); G4 (n * = 45): Duraphat. One application twice a day after toot brushing for 3 months | VAS scores of CAS was evaluated at baseline (T0) and after 1(T1) month and 3(T2) months | n-HA toothpaste was effective treatment for reducing DH over three months. |
| Gopinath et al., 2015, India [41] | 36 (NR) | 18–60 years (NR) | RCT, DB | G1 (n = 18): n-HA paste; G2 (n = 18): 5% SCPS. Brushing for two minutes and no more than twice a day in total during 4 weeks | VAS scores of TS, CAS and cold water tests were recorded at baseline (T0) and after 4 weeks (T1). | n-HA paste showed significant reduction in DH after 4 weeks |
| Jena et al., 2015, India [42] | 45 (122) | 18–50 years (NR) | RCT, DB | G1 (n * = 40): 5% Novamin paste; G2 (n * = 40): 8% arginine paste; G3 (n * = 42): 15% n-HA paste, 60 s application | VAS scores of TS and CAS at baseline (T0) immediately (T1), 1 (T2) and 4 (T3) weeks after treatment | n-HA showed significant reduction in VAS immediately, after 1 and 4 weeks. |
| Mehta et al., 2015, India [43] | 35 (70) | 18–42 years 33.3 (NR) | RCT, DB | G1 (n * = 35): TTCP/DCPA; G2 (n * = 35): Placebo, 30 s application | VAS scores to TS and CAS at baseline T0, 15 min after treatment (T1), 1 day (T2), 1 week (T3), 3 (T4) and 6 (T5) months | TTCP/DCPA toothpaste show a decrease in DH progressively from (T1) to (T5). |
| Naoum et al., 2015, Australia [44] | 71 (NR) | 39–45 years (NR) | RCT, DB | G1 (n = 20): Colgate Cavity Protection (1000 ppmF-MFP); G2 (n = 17): Sensodyne Total Care (1000 ppmF-NaF + 19,300 ppmK+ -KNO3); G3 (n = 16): Clinpro Tooth Creme (950 ppmF-NaF + f TCP); G4 (n = 18): Clinpro Tooth Creme (brushing + additional topical application). Toothbrush twice daily for 10 weeks | NRS-11 pain rating scale of TS, CAS and hypertonic solution were assessed at baseline (T0), 6 weeks (T1), and 10 weeks (T2) | fTCP (brushing + additional topical application) showed a significant reduction in DH. |
| Mehta et al., 2014, India [45] | 49 (200) | 18–50 years (NR) | RCT, DB | G1 (n * = 50): MSC 30 s application; G2 (n * = 50): NAN 20 s application; G3 (n * = 50): TTCP/DCPA (TMD) 30 s application; G4 (n * = 50): GLU, 60 s application | VAS scores to TS and CAS were recorded at baseline (T0) and immediately after application (T1), 1 week (T2), and after 1 (T3), 3 (T4) and 6 (T5) months | TTCP/DCPA showed a significant reduction in DH immediately and after 6 months. |
| Porciani et al., 2014, Italy [46] | 100 (NR) | 18–65 years 41.35 (NR) | RCT, DB | G1 (n = 50): calcium HA/DCPD; G1 (n = 50): Placebo. Two pieces of gum to chew together, three times per day, for 2 weeks | Schiff index value for TS, CAS and cold water at baseline (T0), and after 1 (T1) and 2 (T2) weeks | Chewing gum containing HA/DCPD had a statistically significant reduction in DH after one and two weeks. |
| Vano et al., 2014, Italy [47] | 105 (NR) | 20–70 years (NR) | RCT, DB | G1 (n = 35): 15% n-HA paste; G2 (n = 35): fluoride paste; G3 (n = 35): placebo. Toothbrush during 2 min twice a day for 4 weeks | VAS scores for TS, and CAS were evaluated at baseline (T0) and after 2 (T1) and 4 (T2) weeks | n-HA toothpaste significantly reduced DH between baseline and 4 weeks. |
| Ghassemi et al., 2009, USA, Canada [48] | 208 (NR) | 20–64 years 42.22 (NR) | RCT, DB | G1 (n = 106): Single phase ACP + 0.24% NaF paste; G2 (n = 102): Placebo (0.24% NaF). Toothbrush for 1 min twice a day for 8 weeks | VAS score of CAS was evaluated at baseline (T0), 4 weeks (T1) and 8 weeks (T2) | The toothpaste containing ACP showed a significant reduction in CAS VAS score compared to T0. |
| Geiger et al., 2003, Israel [49] | 30 (NR) | NR | RCT, DB | G1 (n = 15): ACP; G2 (n = 15): Placebo 60 s application | VAS scores of TS and CAS were evaluated at baseline (T0), after one week (T1), after four weeks (T2) and after six months (T3) | ACP showed immediate relief of sensibility after application, with CAS and TS stimulation. |
| Study Reference | Dentin Desensitizing Agents | Manufacturer | No.of Participants (Teeth) | Baseline Mean ± SD | 4 Weeks Follow-up Mean ± SD | Mean Difference Random, 95% CI | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Air blast test | Poliakova et al., 2022, Russia [30] | Toothpaste (20% n−HAP) | NR | 10 | 2.5 ± 0.53 | 1.3 ± 0.48 | −1.20 ± 0.22 (−1.67 to −0.72) | <0.05 |
| Eyuboglu et al., 2020, Turkey [33] | Teethmate™ Desensitizer (TTCP/DCPA) | Kuraray Noritake Osaka, Japan | 10 (21) | 5.52 ± 1.66 | 2.14 ± 0.22 | −3.38 ± 0.36 (−4.11 to −2.64) | <0.05 | |
| Usai et al., 2019, Italy [34] | Teethmate™ Desensitizer (TTCP/DCPA) | Kuraray Noritake Dental Inc., Tokyo, Japan | 35 | 4 ± 2.96 | 0.66 ± 1.51 | −3.34 ± 0.56 (−4.46 to −2.21) | <0.05 | |
| Usai et al., 2019, Italy [34] | Dentin Desensitizer (gel phase of n−HAP) | Ghimas, Casalecchio di Reno, Bologna, Italy | 35 | 5.33 ± 2.22 | 1.66 ± 2.22 | −3.67 ± 0.53 (−4.72 to −2.61) | <0.05 | |
| Usai et al., 2019, Italy [34] | Bite&White ExSense (gel phase of n−HAP in a water) | Cavex Holland, Haarlem, Netherlands | 35 | 4.33 ± 2.96 | 1.0 ± 0.01 | −3.33 ± 0.50 (−4.32 to −2.33) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 15% nHAP | NR | (10) | 3.01 ± 0.01 | 0 ± 0 | −3.01 ± 0.00 (−3.00 to −2.99) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 15% nHAP + 1%NaF | NR | (10) | 2.6 ± 0.52 | 0 ± 0 | −2.59 ± 0.16 (−2.93 to −2.24) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 25% nHAP | NR | (10) | 3.01 ± 0.01 | 0 ± 0 | −3.01 ± 0.00 (−3.00 to −2.99) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 25%nHAP +1%NaF | NR | (10) | 2.6 ± 0.52 | 0 ± 0 | −2.59 ± 0.16 (−2.93 to −2.24) | <0.05 | |
| Vano et al., 2017, Italy [38] | Bite&White ExSense (Gel, 15% n−HA) | Cavex Holland, Haarlem, Netherlands | 35 | 2.97 ± 0.42 | 1.64 ± 0.43 | −1.33 ± 0.10 (−1.53 to −1.12) | <0.05 | |
| De Oliveira et al., 2016, Brazil [39] | Nano P® (hydroxyapatite) | FGM Ltd.a, Brazil | (39) | 6.23 ± 2.72 | 3.54 ± 3.72 | −2.69 ± 0.73 (−4.15 to −1.22 | <0.05 | |
| Wang et al., 2016, Brazil [40] | Desensibilize Nano−P (20% hydroxyapatite) | FGM−Dentscare, Joinville, Brazil | (31) | 7.04 ± 1.62 | 4.10 ± 3.50 | −2.94 ± 0.69 (−4.32 to −1.55) | <0.05 | |
| Wang et al., 2016, Brazil [40] | Desensibilize Nano−P (20% hydroxyapatite) + 10% HA | FGM−Dentscare, Joinville, Brazil | (22) | 7.04 ± 1.62 | 4.48 ± 2.57 | −2.56 ± 0.64 (−3.86 to −1.25) | <0.05 | |
| Gopinath et al., 2015, India [41] | AclaimTM (Nano−HAP) | Group Pharmaceuticals, Bangalore, India | 18 | 7.06 ± 1.55 | 5.39 ± 1.33 | −1.67 ± 0.48 (−2.64 to −0.69) | <0.05 | |
| Mehta et al., 2014, India [45] | Teethmate™ Desensitizer (TTCP/DCPA) | Kuraray Noritake Osaka, Japan | (50) | 6.4 ± 0.5 | 2.2 ± 0.2 | −4.20 ± 0.07 (−4.35 to −4.04) | <0.05 | |
| Vano et al., 2014, Italy [47] | PrevDent® toothpaste (15% n−HA) | NR | 35 | 2.82 ± 0.35 | 1.2 ± 0.49 | −1.62 ± 0.10 (−1.82 to −1.41) | <.05 | |
| Ghassemi et al. 2009, USA, Canada [48] | Enamel Care (n−HAP) | NR | 106 | 6.34 ± 1.11 | 3.47 ± 2.25 | −2.87 ± 0.24 (−3.35 to −2.38) | <0.05 | |
| Total N | 319 (203) | |||||||
| Total mean score (SD) | 4.63 ± 1.01 | 1.92 ± 1.28 | −2.71 ± 0.07 (−2.85 to −2.57) | <0.05 | ||||
| Tactile sensitivity test | Eyuboglu et al., 2020, Turkey [33] | Teethmate Desensitizer (TTCP/DCPA) | Kuraray Noritake Osaka, Japan | 10 (21) | 2.85 ± 1.19 | 1.04 ± 1.20 | −1.81 ± 0.36 (−2.55 to −1.06) | <0.05 |
| Usai et al., 2019, Italy [34] | Teethmate™ Desensitizer (TTCP/DCPA) | Kuraray Noritake Dental Inc., Tokyo, Japan | 35 | 4.01 ± 2.96 | 0.66 ± 1.48 | −3.35 ± 0.56 (−4.46 to −2.23) | <0.05 | |
| Usai et al., 2019, Italy [34] | Dentin Desensitizer (gel phase of n−HAP) | Ghimas, Casalecchio di Reno, Bologna, Italy | 35 | 5.33 ± 2.22 | 1.33 ± 2.22 | −4.00 ± 0.53 (−5.05 to −2.94) | <0.05 | |
| Usai et al., 2019, Italy [34] | Bite&White ExSense (gel phase of n−HAP in a water) | Cavex Holland, Haarlem, Netherlands | 35 | 4.33 ± 2.96 | 0.01 ± 0.02 | −4.32 ± 0.38 (−5.08 to −3.55) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 15% nHAP | NR | (10) | 2.4 ± 1.03 | 0 ± 0 | −2.39 ± 0.32 (−3.07 to −1.70) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 15% nHAP + 1%NaF | NR | (10) | 2.2 ± 0.52 | 0 ± 0 | −2.19 ± 0.16 (−2.53 to −1.84) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 25% nHAP | NR | (10) | 2.8 ± 1.03 | 0 ± 0 | −2.79 ± 0.32 (−3.47 to −2.10) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 25%nHAP +1%NaF | NR | (10) | 2.3 ± 0.52 | 0 ± 0 | −2.29 ± 0.16 (−2.63 to −1.94) | <0.05 | |
| Vano et al., 2017, Italy [38] | Bite&White ExSense (Gel, 15% n−HA) | Cavex Bite&White ExSense, Cavex Holland BV | 35 | 3.17 ± 0.49 | 1.83 ± 0.63 | −1.34 ± 0.14 (−1.60 to −1.07) | <0.05 | |
| Gopinath et al., 2015, India [41] | AclaimTM (Nano−HAP) | Group Pharmaceuticals, Bangalore, India | 18 | 4.67 ± 1.08 | 3.78 ± 0.94 | −0.89 ± 0.33 (−1.57 to −0.20) | >0.05 | |
| Mehta et al., 2014, India [43] | Teethmate Desensitizer (TTCP/DCPA) | Kuraray Noritake Osaka, Japan | (50) | 6.21 ± 1.82 | 2.81 ± 1.06 | −3.4 ± 0.29 (−3.99 to −2.80) | <0.05 | |
| Vano et al., 2014, Italy [47] | PrevDent® toothpaste (15% n−HA) | NR | 35 | 2.54 ± 0.52 | 0.95 ± 0.59 | −1.59 ± 0.13 (−1.85 to −1.32) | <0.05 | |
| Total N | 158 (111) | |||||||
| Total mean score (SD) | 3.56 ± 0.91 | 1.03 ± 0.72 | −2.53 ± 0.07 (−2.66 to −2.39) | <0.05 | ||||
| Cold water test | Ameen et al., 2018, Egypt [36] | 15% nHAP | NR | (10) | 3 ± 0 | 0 ± 0 | −2.99 ± 0.01 (−2.99 to −2.98) | <0.05 |
| Ameen et al., 2018,Egypt [36] | 15% nHAP + 1%NaF | NR | (10) | 2.6 ± 0.52 | 0 ± 0 | −2.59 ± 0.16 (−2.93 to −2.24) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 25% nHAP | NR | (10) | 3 ± 0 | 0 ± 0 | −2.99 ± 0.01 (−2.99 to −2.98) | <0.05 | |
| Ameen et al., 2018, Egypt [36] | 25%nHAP + 1%NaF | NR | (10) | 2.4 ± 0.52 | 0 ± 0 | −2.39 ± 0.16 (−2.73 to −2.04) | <0.05 | |
| De Oliveira et al., 2016, Brazil [39] | Nano P® (hydroxyapatite) | FGM Ltd.a, Brazil | (39) | 9.14 ± 1.37 | 6.51 ± 3.65 | −2.63 ± 0.62 (−3.87 to −1.38) | <0.05 | |
| Gopinath et al., 2015, India [41] | AclaimTM (Nano−HAP) | Group Pharmaceuticals, Bangalore, India | 18 | 6.72 ± 1.01 | 4.94 ± 1.05 | −1.78 ± 0.34 (−2.47 to −1.08) | <0.05 | |
| Total N | 18 (79) | |||||||
| Total mean score (SD) | 4.47 ± 0.72 | 1.91 ± 1.46 | −2.56 ± 0.16 (−2.88 to −2.23) | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maillard, M.; Bandiaky, O.N.; Maunoury, S.; Alliot, C.; Alliot-Licht, B.; Serisier, S.; Renard, E. The Effectiveness of Calcium Phosphates in the Treatment of Dentinal Hypersensitivity: A Systematic Review. Bioengineering 2023, 10, 447. https://doi.org/10.3390/bioengineering10040447
Maillard M, Bandiaky ON, Maunoury S, Alliot C, Alliot-Licht B, Serisier S, Renard E. The Effectiveness of Calcium Phosphates in the Treatment of Dentinal Hypersensitivity: A Systematic Review. Bioengineering. 2023; 10(4):447. https://doi.org/10.3390/bioengineering10040447
Chicago/Turabian StyleMaillard, Mélanie, Octave Nadile Bandiaky, Suzanne Maunoury, Charles Alliot, Brigitte Alliot-Licht, Samuel Serisier, and Emmanuelle Renard. 2023. "The Effectiveness of Calcium Phosphates in the Treatment of Dentinal Hypersensitivity: A Systematic Review" Bioengineering 10, no. 4: 447. https://doi.org/10.3390/bioengineering10040447