
Development of a Metaphyseal Non-Union Model in the Osteoporotic Rat Femur
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Animals
2.2. Animal Study Design
2.3. Osteoporotic Induction
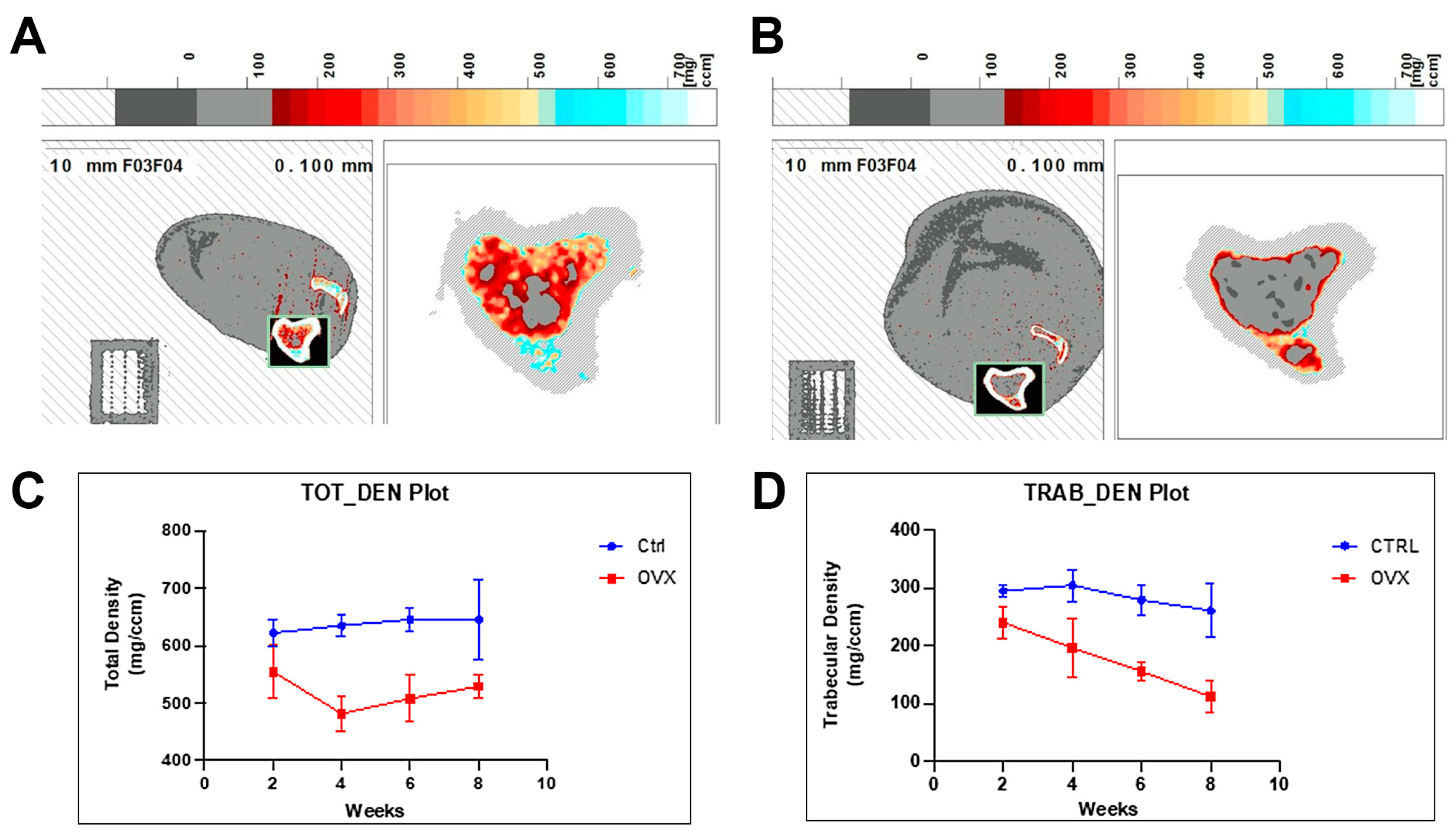
2.4. Quantitative Assessment of the Osteoporotic Bone Phenotype
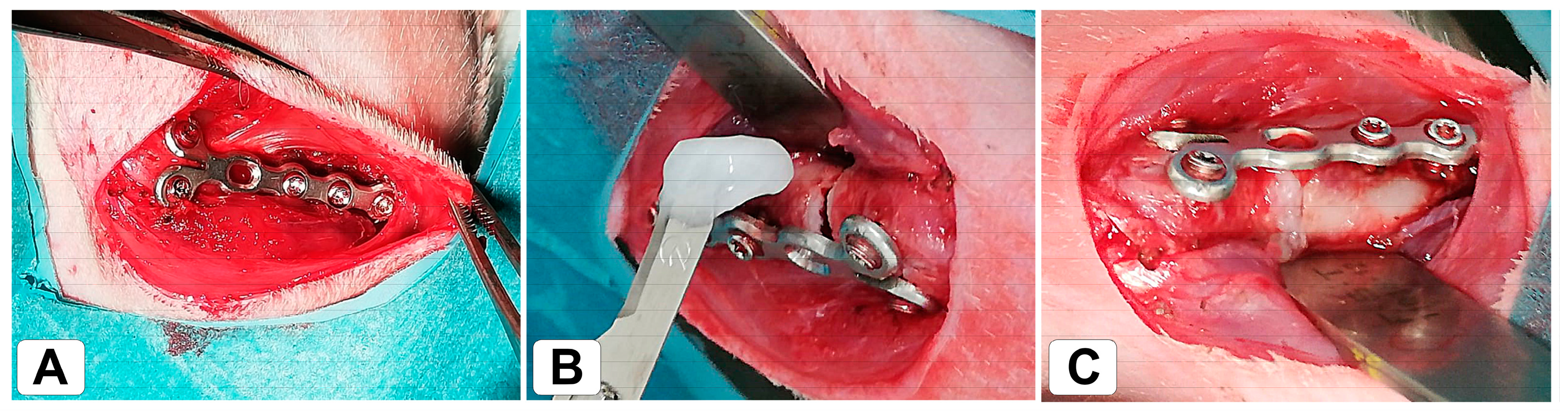
2.5. Surgical Procedure: Metaphyseal Non-Union Model
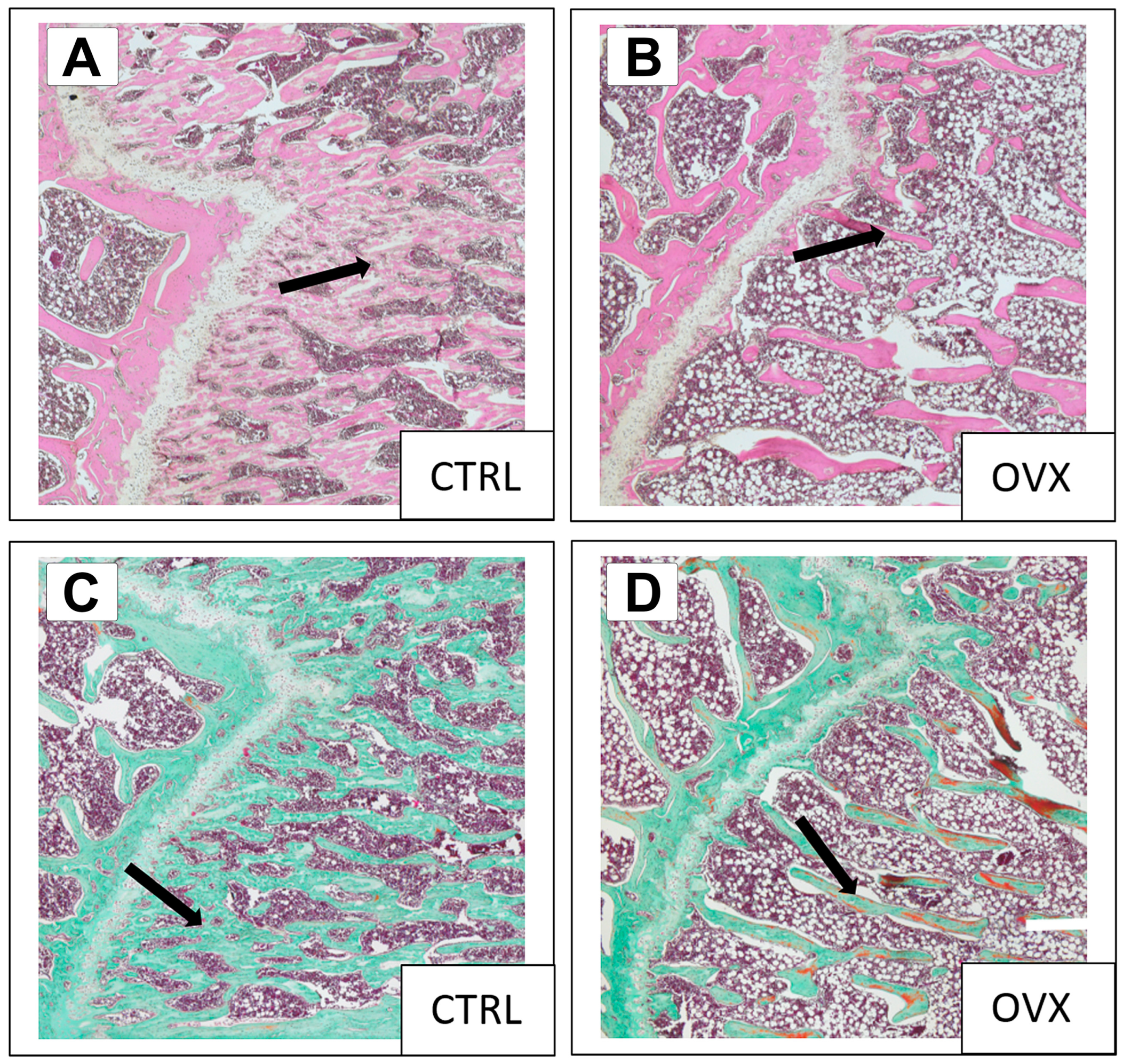
2.6. Histological Examination and Staining
2.7. Radiological and Histological Scoring
2.8. Statistical Analysis
3. Results
3.1. Experimental Results
3.2. Osteoporotic Induction
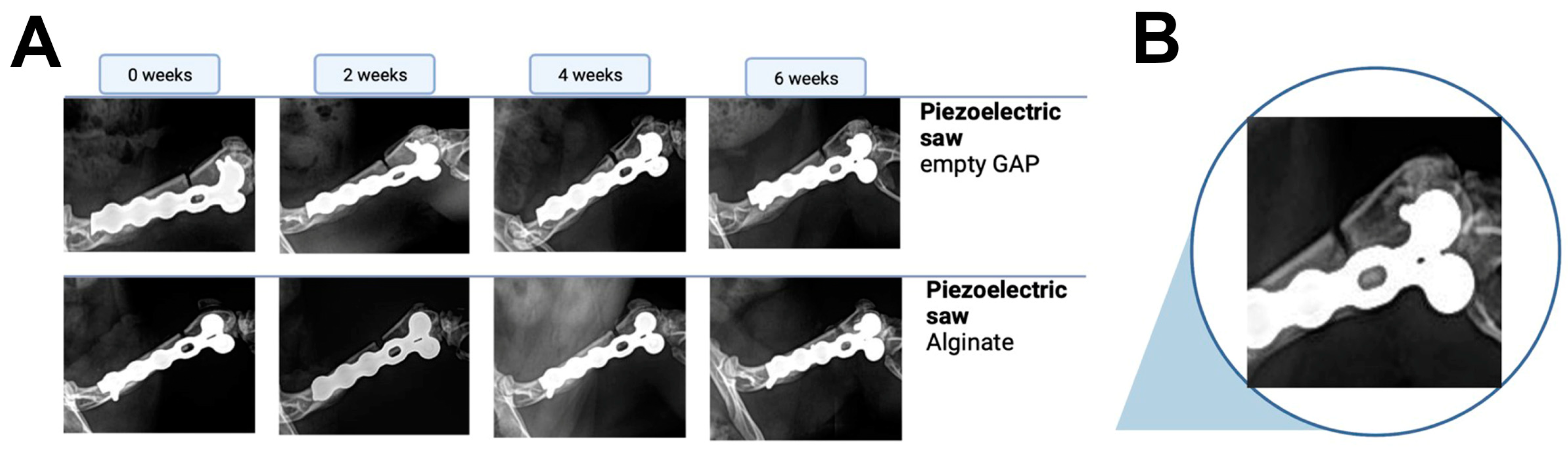
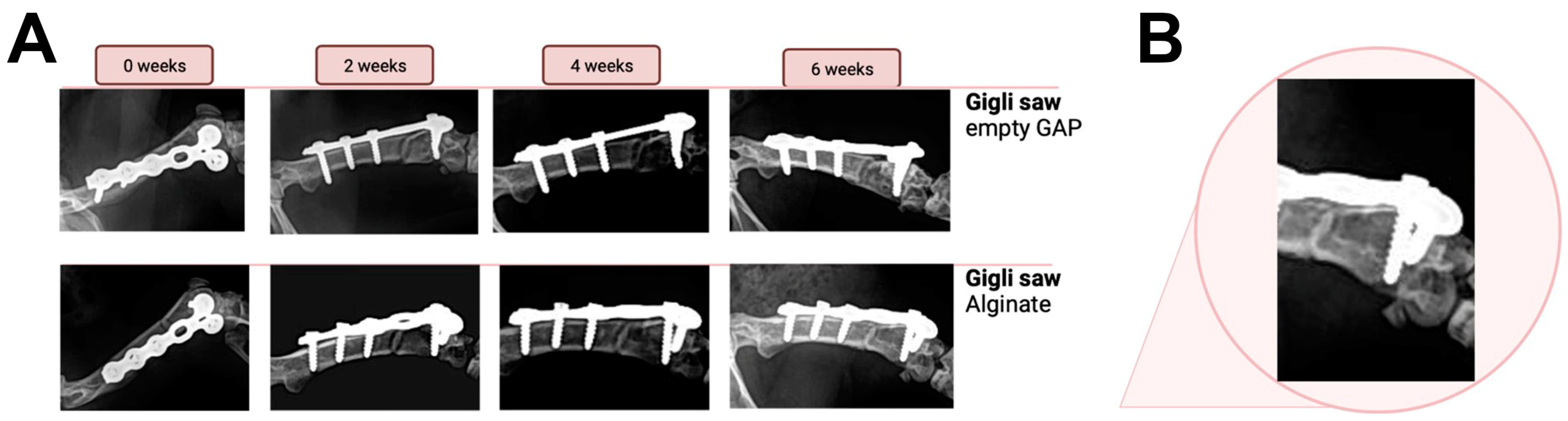
3.3. Radiographic Evaluation
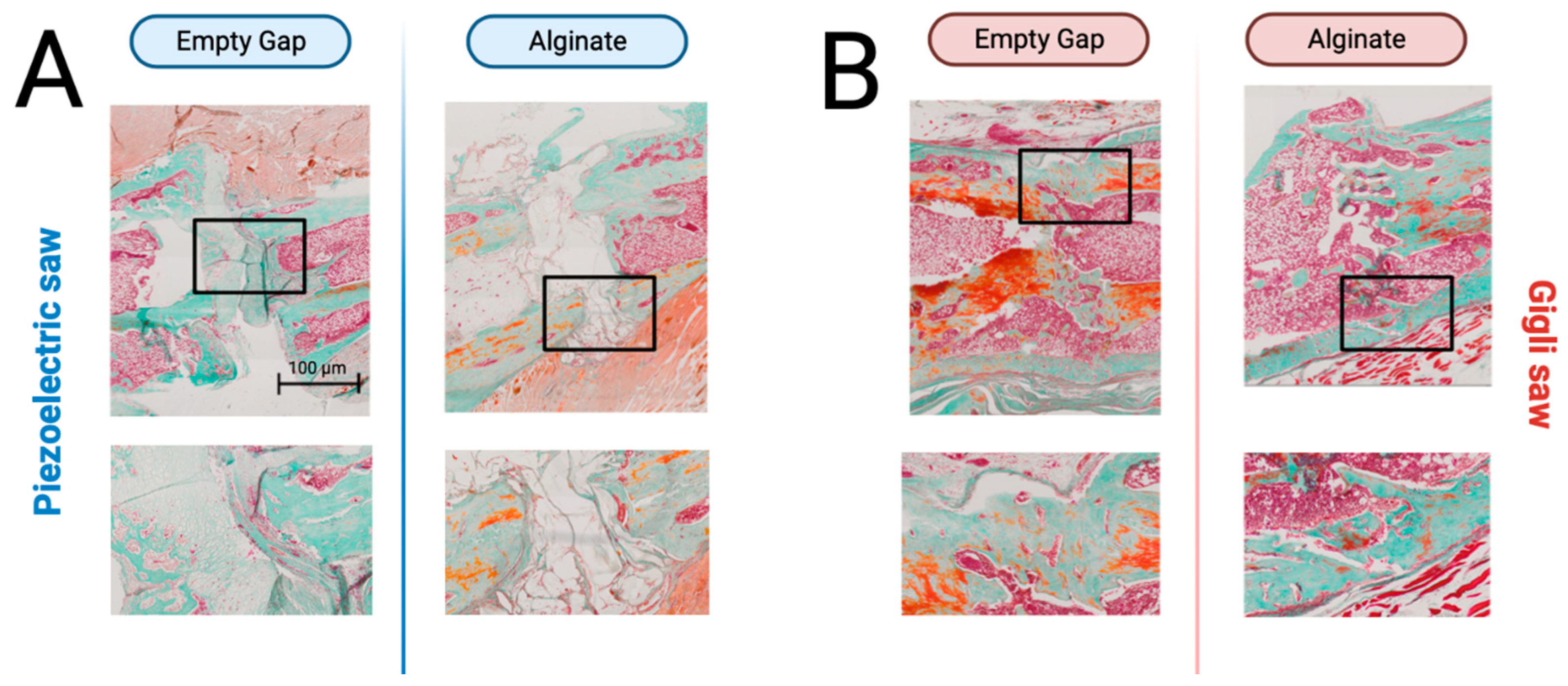
3.4. Histology
3.5. Radiological and Histological Scoring
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.Y. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2019, 30, 3–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, S. Treatment of osteoporotic fractures. Scand J. Surg. 2002, 91, 140–146. [Google Scholar] [CrossRef]
- Osterhoff, G.; Morgan, E.F.; Shefelbine, S.J.; Karim, L.; McNamara, L.M.; Augat, P. Bone mechanical properties and changes with osteoporosis. Injury 2016, 47 (Suppl S2), S11–S20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollensteiner, M.; Sandriesser, S.; Bliven, E.; von Rüden, C.; Augat, P. Biomechanics of Osteoporotic Fracture Fixation. Curr. Osteoporos. Rep. 2019, 17, 363–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Rüden, C.; Augat, P. Failure of fracture fixation in osteoporotic bone. Injury 2016, 47 (Suppl S2), S3–S10. [Google Scholar] [CrossRef] [PubMed]
- El Khassawna, T.; Böcker, W.; Brodsky, K.; Weisweiler, D.; Govindarajan, P.; Kampschulte, M.; Thormann, U.; Henss, A.; Rohnke, M.; Bauer, N.; et al. Impaired extracellular matrix structure resulting from malnutrition in ovariectomized mature rats. Histochem. Cell Biol. 2015, 144, 491–507. [Google Scholar] [CrossRef]
- Egermann, M.; Goldhahn, J.; Schneider, E. Animal models for fracture treatment in osteoporosis. Osteoporos. Int. 2005, 16 (Suppl S2), S129–S138. [Google Scholar] [CrossRef]
- Wong, R.M.; Choy, M.H.; Li, M.C.; Leung, K.S.; Chow, S.K.; Cheung, W.H.; Cheng, J.C. A systematic review of current osteoporotic metaphyseal fracture animal models. Bone Joint Res. 2018, 7, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Tao, Z.S.; Zhou, W.S.; Tu, K.K.; Huang, Z.L.; Zhou, Q.; Sun, T.; Lv, Y.X.; Cui, W.; Yang, L. Effect exerted by Teriparatide upon Repair Function of β-tricalcium phosphate to ovariectomised rat’s femoral metaphysis defect caused by osteoporosis. Injury 2015, 46, 2134–2141. [Google Scholar] [CrossRef]
- McDonald, M.M.; Morse, A.; Mikulec, K.; Peacock, L.; Yu, N.; Baldock, P.A.; Birke, O.; Liu, M.; Ke, H.Z.; Little, D.G. Inhibition of sclerostin by systemic treatment with sclerostin antibody enhances healing of proximal tibial defects in ovariectomized rats. J. Orthop. Res. 2012, 30, 1541–1548. [Google Scholar] [CrossRef] [Green Version]
- Komrakova, M.; Hoffmann, D.B.; Nuehnen, V.; Stueber, H.; Wassmann, M.; Wicke, M.; Tezval, M.; Stuermer, K.M.; Sehmisch, S. The Effect of Vibration Treatments Combined with Teriparatide or Strontium Ranelate on Bone Healing and Muscle in Ovariectomized Rats. Calcif. Tissue Int. 2016, 99, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Kolios, L.; Hoerster, A.K.; Sehmisch, S.; Malcherek, M.C.; Rack, T.; Tezval, M.; Seidlova-Wuttke, D.; Wuttke, W.; Stuermer, K.M.; Stuermer, E.K. Do estrogen and alendronate improve metaphyseal fracture healing when applied as osteoporosis prophylaxis? Calcif. Tissue Int. 2010, 86, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thormann, U.; El Khawassna, T.; Ray, S.; Duerselen, L.; Kampschulte, M.; Lips, K.; von Dewitz, H.; Heinemann, S.; Heiss, C.; Szalay, G.; et al. Differences of bone healing in metaphyseal defect fractures between osteoporotic and physiological bone in rats. Injury 2014, 45, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Alt, V.; Thormann, U.; Ray, S.; Zahner, D.; Durselen, L.; Lips, K.; El Khassawna, T.; Heiss, C.; Riedrich, A.; Schlewitz, G.; et al. A new metaphyseal bone defect model in osteoporotic rats to study biomaterials for the enhancement of bone healing in osteoporotic fractures. Acta Biomater. 2013, 9, 7035–7042. [Google Scholar] [CrossRef] [PubMed]
- Komrakova, M.; Weidemann, A.; Dullin, C.; Ebert, J.; Tezval, M.; Stuermer, K.M.; Sehmisch, S. The Impact of Strontium Ranelate on Metaphyseal Bone Healing in Ovariectomized Rats. Calcif. Tissue Int. 2015, 97, 391–401. [Google Scholar] [CrossRef]
- Stuermer, E.K.; Sehmisch, S.; Rack, T.; Wenda, E.; Seidlova-Wuttke, D.; Tezval, M.; Wuttke, W.; Frosch, K.H.; Stuermer, K.M. Estrogen and raloxifene improve metaphyseal fracture healing in the early phase of osteoporosis. A new fracture-healing model at the tibia in rat. Langenbecks Arch Surg. 2010, 395, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Wong, R.M.; Thormann, U.; Choy, M.H.; Chim, Y.N.; Li, M.C.; Wang, J.Y.; Leung, K.S.; Cheng, J.C.; Alt, V.; Chow, S.K.; et al. A metaphyseal fracture rat model for mechanistic studies of osteoporotic bone healing. Eur. Cell Mater. 2019, 37, 420–430. [Google Scholar] [CrossRef]
- Cheung, W.H.; Miclau, T.; Chow, S.K.; Yang, F.F.; Alt, V. Fracture healing in osteoporotic bone. Injury 2016, 47 (Suppl S2), S21–S26. [Google Scholar] [CrossRef]
- Histing, T.; Klein, M.; Stieger, A.; Stenger, D.; Steck, R.; Matthys, R.; Holstein, J.H.; Garcia, P.; Pohlemann, T.; Menger, M.D. A new model to analyze metaphyseal bone healing in mice. J. Surg. Res. 2012, 178, 715–721. [Google Scholar] [CrossRef]
- Timon, C.; Keady, C. Thermal Osteonecrosis Caused by Bone Drilling in Orthopedic Surgery: A Literature Review. Cureus 2019, 11, e5226. [Google Scholar] [CrossRef] [Green Version]
- Alajmo, G.; Schlegel, U.; Gueorguiev, B.; Matthys, R.; Gautier, E. Plunging when drilling: Effect of using blunt drill bits. J. Orthop. Trauma 2012, 26, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Barquet, A.; Gelink, A.; Giannoudis, P.V. Proximal femoral fractures and vascular injuries in adults: Incidence, aetiology and outcomes. Injury 2015, 46, 2297–2313. [Google Scholar] [CrossRef] [PubMed]
- Heiss, C.; Govindarajan, P.; Schlewitz, G.; Hemdan, N.Y.; Schliefke, N.; Alt, V.; Thormann, U.; Lips, K.S.; Wenisch, S.; Langheinrich, A.C.; et al. Induction of osteoporosis with its influence on osteoporotic determinants and their interrelationships in rats by DEXA. Med. Sci. Monit 2012, 18, BR199–BR207. [Google Scholar] [CrossRef] [Green Version]
- Gasser, J.A.; Willnecker, J. Bone Measurements by Peripheral Quantitative Computed Tomography in Rodents. Methods Mol. Biol. 2019, 1914, 533–558. [Google Scholar] [CrossRef] [PubMed]
- Romeis, B. Mikroskopische Technik von Mulisch, M., Welsch, U.; Springer: Heidelberg, Germany, 2010; p. 551. [Google Scholar]
- Johnson, K.D.; Frierson, K.E.; Keller, T.S.; Cook, C.; Scheinberg, R.; Zerwekh, J.; Meyers, L.; Sciadini, M.F. Porous ceramics as bone graft substitutes in long bone defects: A biomechanical, histological, and radiographic analysis. J. Orthop. Res. 1996, 14, 351–369. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Simmons, D.J.; Lozano, R. The healing of grafts combining freeze-dried and demineralized allogeneic bone in rabbits. Clin. Orthop. Relat. Res. 1994, 298, 286–295. [Google Scholar] [CrossRef]
- An, Y.H.; Friedman, R.J. Animal Models of Bone Defect Repair; CRC Press LLC: Boca Raton, FL, USA, 1999; pp. 241–260. [Google Scholar]
- Mills, L.A.; Aitken, S.A.; Simpson, A.H.R.W. The risk of non-union per fracture: Current myths and revised figures from a population of over 4 million adults. Acta Orthop. 2017, 88, 434–439. [Google Scholar] [CrossRef] [Green Version]
- Zura, R.; Xiong, Z.; Einhorn, T.; Watson, J.T.; Ostrum, R.F.; Prayson, M.J.; Della Rocca, G.J.; Mehta, S.; McKinley, T.; Wang, Z.; et al. Epidemiology of Fracture Nonunion in 18 Human Bones. JAMA Surg. 2016, 151, e162775. [Google Scholar] [CrossRef] [Green Version]
- Driessen, J.H.; Hansen, L.; Eriksen, S.A.; van Onzenoort, H.A.; Henry, R.M.; van den Bergh, J.; Abrahamsen, B.; Vestergaard, P.; de Vries, F. The epidemiology of fractures in Denmark in 2011. Osteoporos. Int. 2016, 27, 2017–2025. [Google Scholar] [CrossRef] [Green Version]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Williams, J.N.; Li, Y.; Valiya Kambrath, A.; Sankar, U. The Generation of Closed Femoral Fractures in Mice: A Model to Study Bone Healing. J. Vis. Exp. 2018, 138, e58122. [Google Scholar] [CrossRef]
- Histing, T.; Garcia, P.; Holstein, J.H.; Klein, M.; Matthys, R.; Nuetzi, R.; Steck, R.; Laschke, M.W.; Wehner, T.; Bindl, R.; et al. Small animal bone healing models: Standards, tips, and pitfalls results of a consensus meeting. Bone 2011, 49, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, Z.J.; Campbell, Z.R.; McKinley, T.O.; Natoli, R.M.; Kacena, M.A. A comprehensive review of mouse diaphyseal femur fracture models. Injury 2020, 51, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Matsubara, H.; Fang, X.; Hayashi, K.; Nomura, I.; Ugaji, S.; Hamada, T.; Tsuchiya, H. Adipose-derived stem cell sheets accelerate bone healing in rat femoral defects. PLoS ONE 2019, 14, e0214488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, S.; Takito, J.; Nakamura, M. Site-Specific Fracture Healing: Comparison between Diaphysis and Metaphysis in the Mouse Long Bone. Int. J. Mol. Sci. 2021, 22, 9299. [Google Scholar] [CrossRef]
- Eggers, G.; Klein, J.; Blank, J.; Hassfeld, S. Piezosurgery: An ultrasound device for cutting bone and its use and limitations in maxillofacial surgery. Br. J. Oral. Maxillofac. Surg. 2004, 42, 451–453. [Google Scholar] [CrossRef]
- Vercellotti, T.; Pollack, A.S. A new bone surgery device: Sinus grafting and periodontal surgery. Compend Contin Educ. Dent. 2006, 27, 319–325. [Google Scholar]
- Delgado-Ruiz, R.A.; Sacks, D.; Palermo, A.; Calvo-Guirado, J.L.; Perez-Albacete, C.; Romanos, G.E. Temperature and time variations during osteotomies performed with different piezosurgical devices: An in vitro study. Clin. Oral Implants Res. 2016, 27, 1137–1143. [Google Scholar] [CrossRef]
- Crosetti, E.; Battiston, B.; Succo, G. Piezosurgery in head and neck oncological and reconstructive surgery: Personal experience on 127 cases. Acta Otorhinolaryngol. Ital. 2009, 29, 1–9. [Google Scholar]
- Schlee, M.; Steigmann, M.; Bratu, E.; Garg, A.K. Piezosurgery: Basics and possibilities. Implant Dent. 2006, 15, 334–340. [Google Scholar] [CrossRef]
- d’Agostino, M.C.; Craig, K.; Tibalt, E.; Respizzi, S. Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. Int. J. Surg. 2015, 24, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Crovace, A.M.; Luzzi, S.; Lacitignola, L.; Fatone, G.; Giotta Lucifero, A.; Vercellotti, T.; Crovace, A. Minimal Invasive Piezoelectric Osteotomy in Neurosurgery: Technic, Applications, and Clinical Outcomes of a Retrospective Case Series. Vet. Sci. 2020, 7, 68. [Google Scholar] [CrossRef] [PubMed]
- Vercellotti, T.; De Paoli, S.; Nevins, M. The piezoelectric bony window osteotomy and sinus membrane elevation: Introduction of a new technique for simplification of the sinus augmentation procedure. Int. J. Periodont. Restor. Dent. 2001, 21, 561–567. [Google Scholar]
- Vercellotti, T. Technological characteristics and clinical indications of piezoelectric bone surgery. Minerva Stomatol. 2004, 53, 207–214. [Google Scholar] [PubMed]
- Stelzle, F.; Frenkel, C.; Riemann, M.; Knipfer, C.; Stockmann, P.; Nkenke, E. The effect of load on heat production, thermal effects and expenditure of time during implant site preparation—An experimental ex vivo comparison between piezosurgery and conventional drilling. Clin. Oral Implants Res. 2014, 25, e140–e148. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Scores | |||
|---|---|---|---|---|
| 3 | 2 | 1 | 0 | |
| Periosteal reaction | Complete across defect | Moderate (>50%) | Mild (<50%) | None |
| Bone union | Complete bony union | Moderate (>50%) | Mild (<50%) | None |
| Remodeling | Complete remodeled cortex | Mild (<50%) | None | |
| Categories | Scores | |||
|---|---|---|---|---|
| 3 | 2 | 1 | 0 | |
| Callus formation | Complete across defect | Moderate (>50%) | Mild (<50%) | None |
| Bone union | Complete bony union | Moderate (>50%) | Mild (<50%) | None |
| Cortex remodeling | Complete remodeled cortex | Moderate (>50%) | Mild (<50%) | None |
| Marrow changes | Adult type fatty marrow | Moderate (>50%) | Mild (<50%) | None |
| Animal | Blood Glucose Levels (mg/dL) | ||
|---|---|---|---|
| Week 0 | Week 4 | Week 8 | |
| OVX1 | 129 | 115 | 131 |
| OVX1 | 132 | 162 | 149 |
| OVX1 | 127 | 139 | 107 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deluca, A.; Wagner, A.; Faustini, B.; Weissenbacher, N.; Deininger, C.; Wichlas, F.; Tempfer, H.; Mueller, E.J.; Traweger, A. Development of a Metaphyseal Non-Union Model in the Osteoporotic Rat Femur. Bioengineering 2023, 10, 338. https://doi.org/10.3390/bioengineering10030338
Deluca A, Wagner A, Faustini B, Weissenbacher N, Deininger C, Wichlas F, Tempfer H, Mueller EJ, Traweger A. Development of a Metaphyseal Non-Union Model in the Osteoporotic Rat Femur. Bioengineering. 2023; 10(3):338. https://doi.org/10.3390/bioengineering10030338
Chicago/Turabian StyleDeluca, Amelie, Andrea Wagner, Bettina Faustini, Nadja Weissenbacher, Christian Deininger, Florian Wichlas, Herbert Tempfer, Ernst J. Mueller, and Andreas Traweger. 2023. "Development of a Metaphyseal Non-Union Model in the Osteoporotic Rat Femur" Bioengineering 10, no. 3: 338. https://doi.org/10.3390/bioengineering10030338