
Visual Blood, a 3D Animated Computer Model to Optimize the Interpretation of Blood Gas Analysis
 , , , , , ,
, , , , , ,  , , and
, , and
Abstract
:
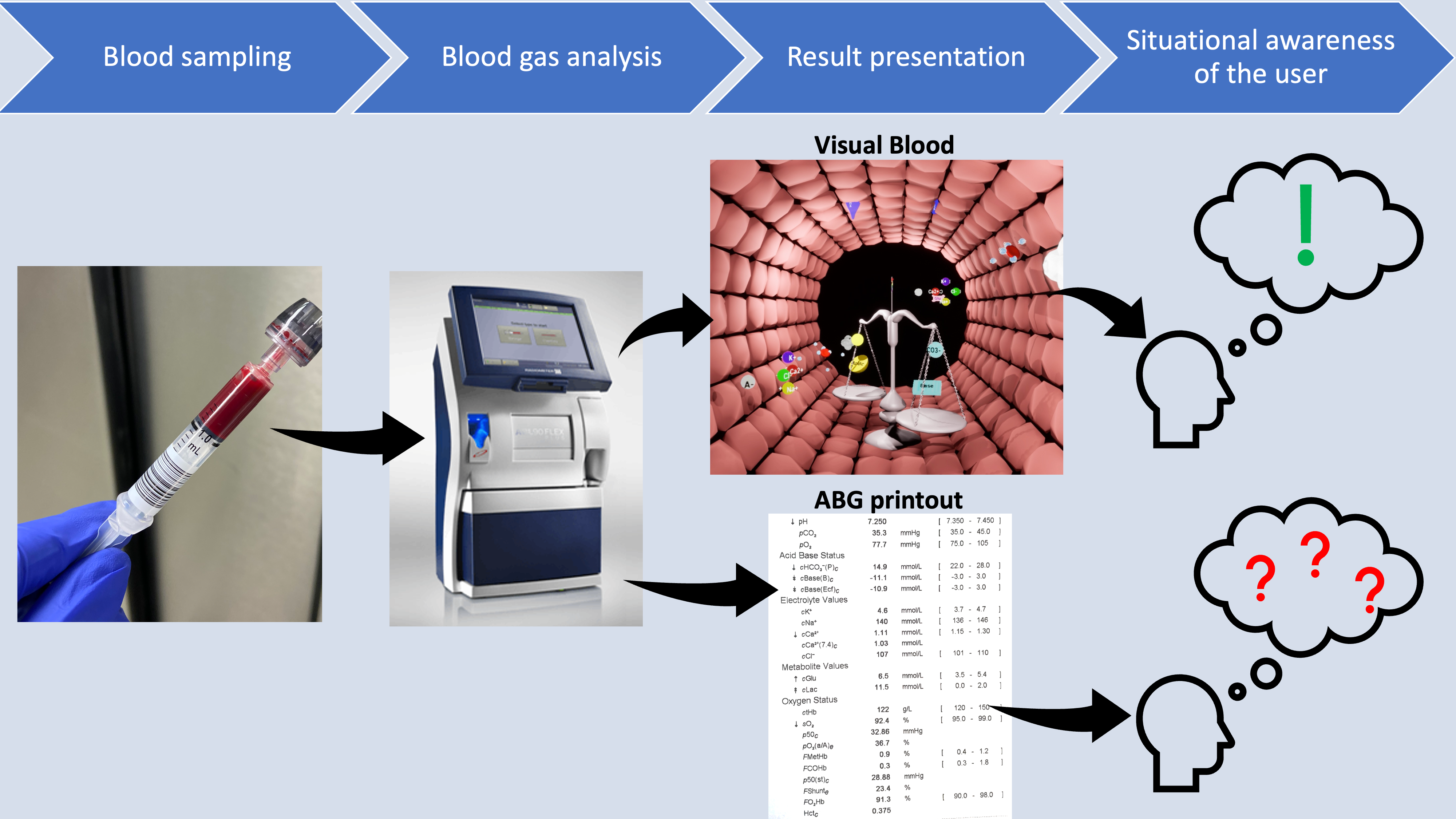
1. Introduction
2. Materials and Methods
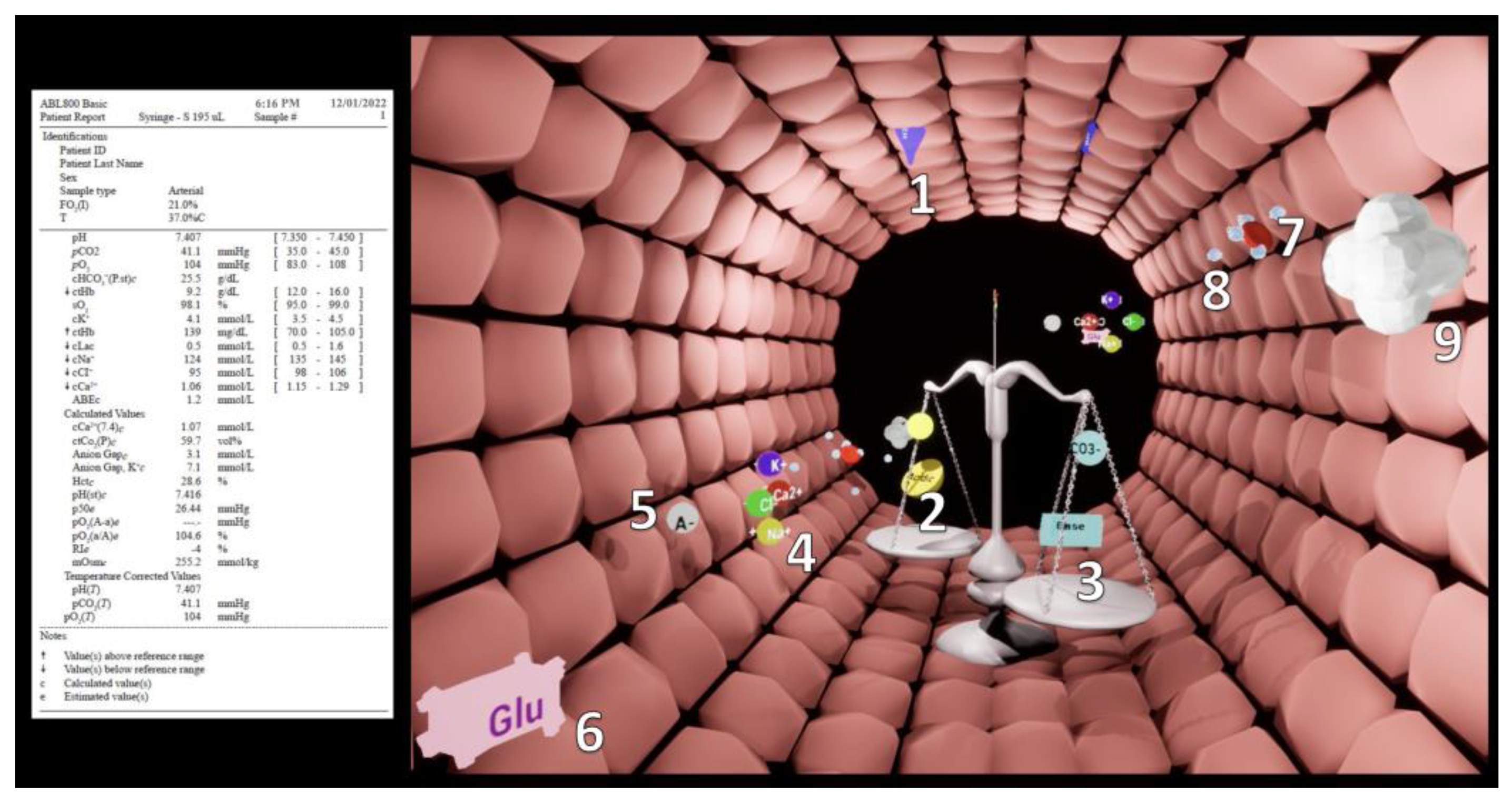
2.1. Visual Blood
2.2. Study Design and Participants
2.3. Study Procedure and Outcome Measures
2.4. Statistical Analysis
2.5. Sample Size Calculation
3. Results
3.1. Study, Part One
3.2. Study, Part Two
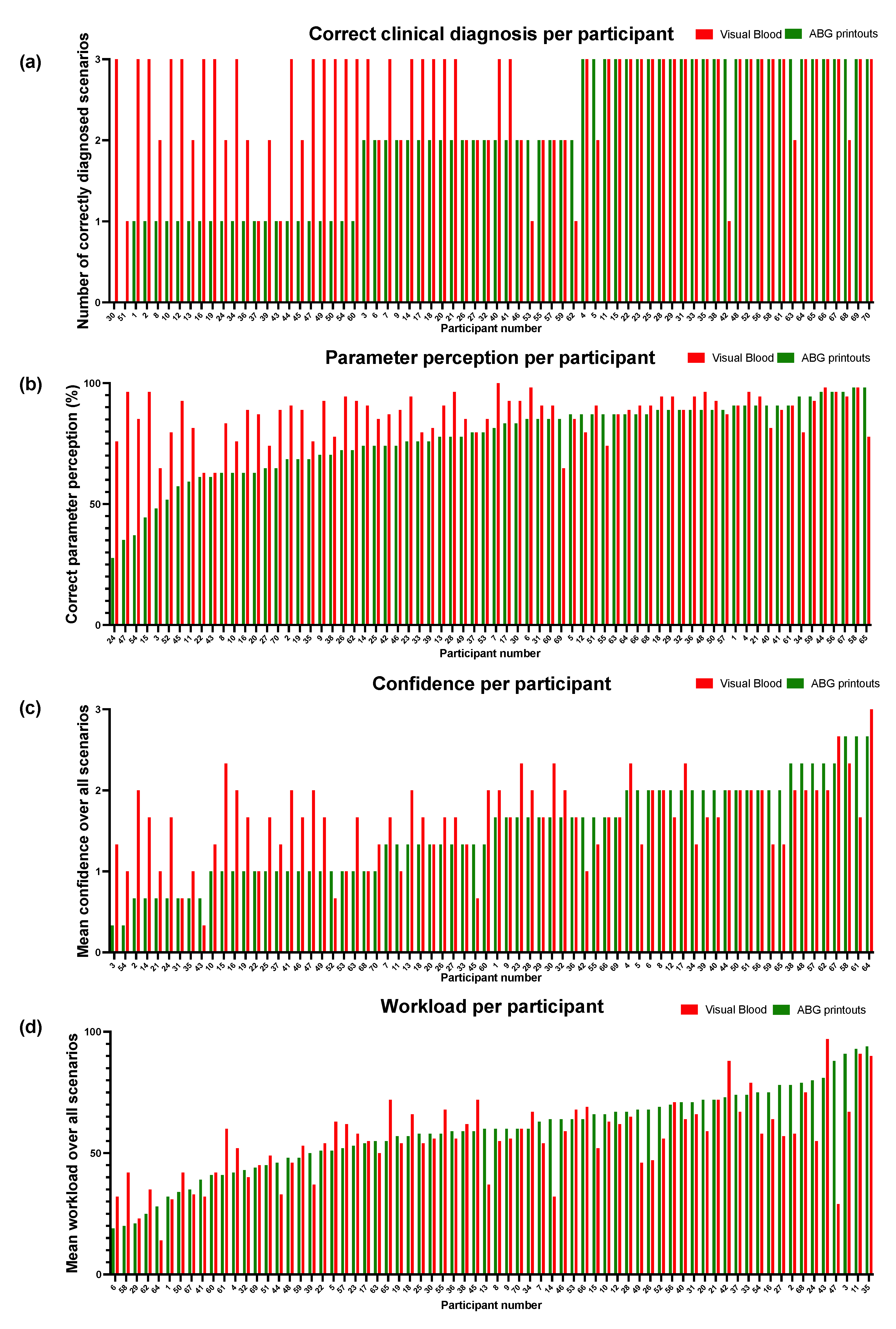
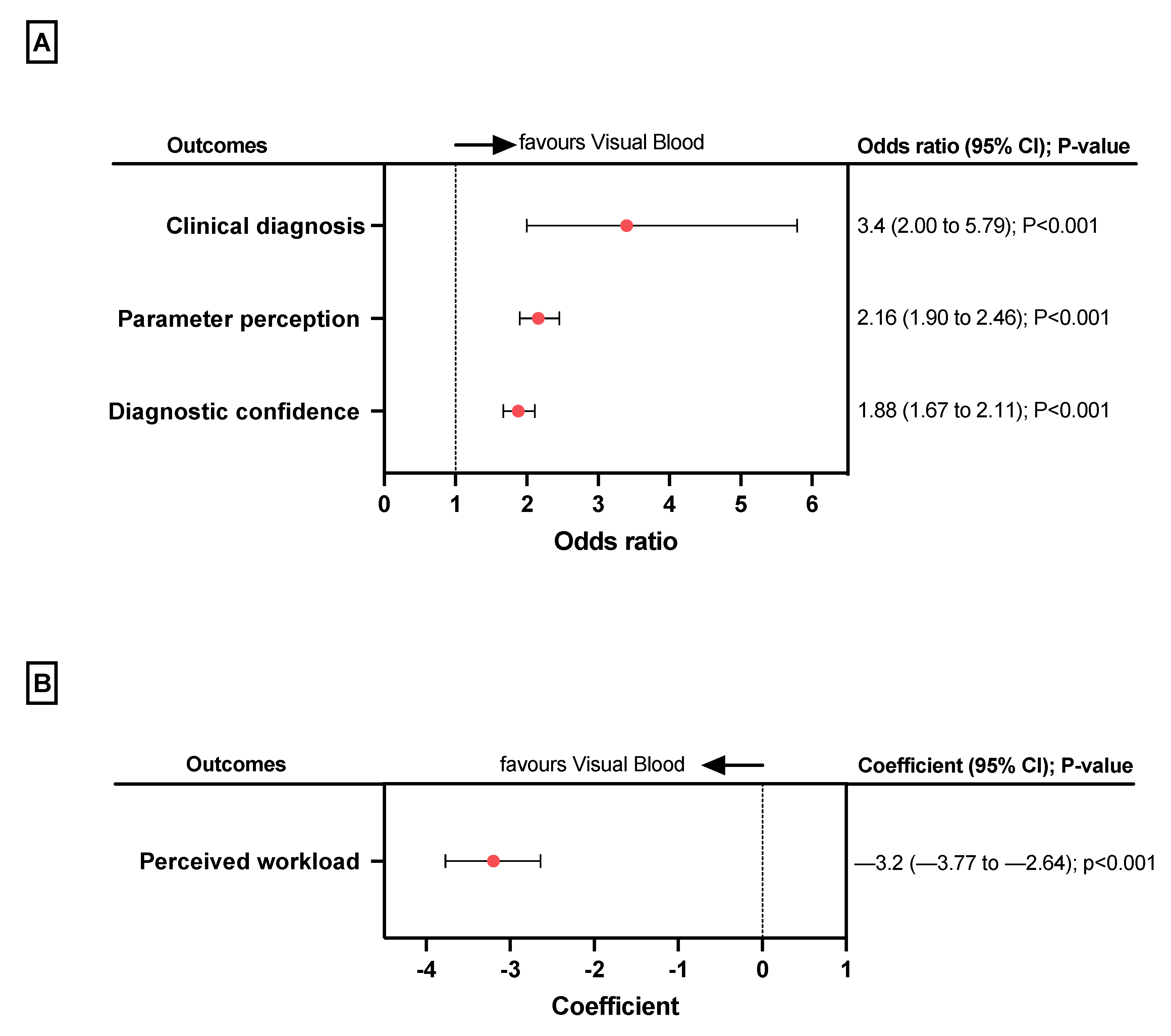
3.2.1. Clinical Diagnoses
3.2.2. Parameter Perception
3.2.3. Diagnostic Confidence
3.2.4. Perceived Workload
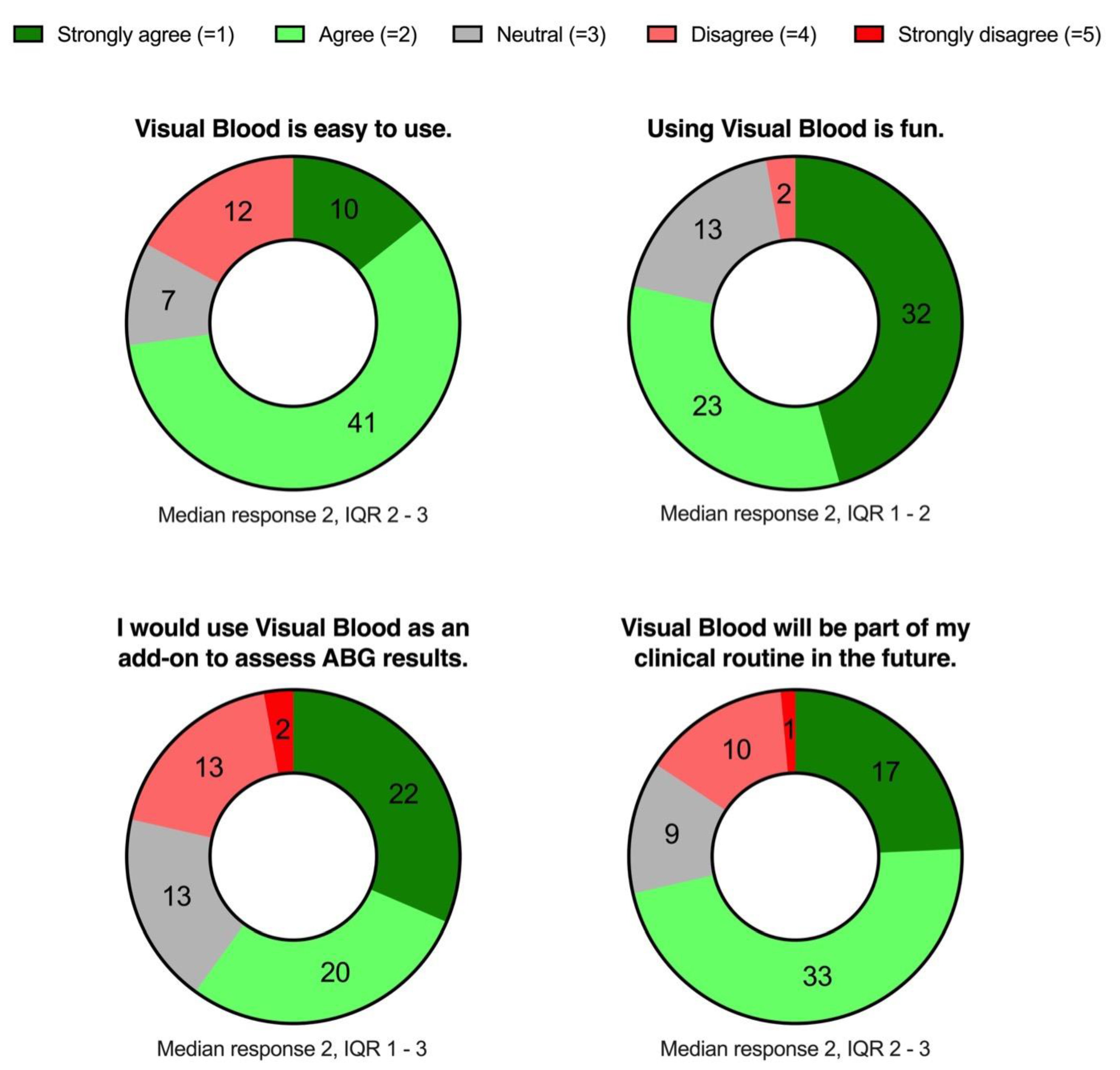
3.2.5. Participant Opinions about VB
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berend, K.; de Vries, A.P.; Gans, R.O. Physiological approach to assessment of acid-base disturbances. N. Engl. J. Med. 2014, 371, 1434–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gattinoni, L.; Pesenti, A.; Matthay, M. Understanding blood gas analysis. Intensive Care Med. 2018, 44, 91–93. [Google Scholar] [CrossRef]
- Berend, K.; Duits, A.J. The role of the clinical laboratory in diagnosing acid-base disorders. Crit. Rev. Clin. Lab. Sci. 2019, 56, 147–169. [Google Scholar] [CrossRef] [PubMed]
- Berend, K. Acid-base pathophysiology after 130 years: Confusing, irrational and controversial. J. Nephrol. 2013, 26, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Astrup, P.; Jorgensen, K.; Andersen, O.S.; Engel, K. The acid-base metabolism: A new approach. Lancet 1960, 1, 1035–1039. [Google Scholar] [CrossRef]
- Schulz, C.M.; Endsley, M.R.; Kochs, E.F.; Gelb, A.W.; Wagner, K.J. Situation awareness in anesthesia: Concept and research. Anesthesiology 2013, 118, 729–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Endsley, M. Designing for Situation Awareness: An Approach to User-Centered Design, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Schulz, C.M.; Burden, A.; Posner, K.L.; Mincer, S.L.; Steadman, R.; Wagner, K.J.; Domino, K.B. Frequency and type of situational awareness errors contributing to death and brain damage: A closed claims analysis. Anesthesiology 2017, 127, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.M.; Krautheim, V.; Hackemann, A.; Kreuzer, M.; Kochs, E.F.; Wagner, K.J. Situation awareness errors in anesthesia and critical care in 200 cases of a critical incident reporting system. BMC Anesthesiol. 2016, 16, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drews, F.A.; Westenskow, D.R. The right picture is worth a thousand numbers: Data displays in anesthesia. Hum. Factors 2006, 48, 59–71. [Google Scholar] [CrossRef]
- Kataife, E.D.; Said, S.; Braun, J.; Roche, T.R.; Rössler, J.; Kaserer, A.; Spahn, D.R.; Mileo, F.G.; Tscholl, D.W. The haemostasis traffic light, a user-centred coagulation management tool for acute bleeding situations: A simulation-based randomised dual-centre trial. Anaesthesia 2021, 76, 902–910. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Rossler, J.; Said, S.; Kaserer, A.; Spahn, D.R.; Nothiger, C.B. Situation awareness-oriented patient monitoring with visual patient technology: A qualitative review of the primary research. Sensors 2020, 20, 2112. [Google Scholar] [CrossRef] [Green Version]
- Rössler, J.; Meybohm, P.; Spahn, D.R.; Zacharowski, K.; Braun, J.; Nöthiger, C.B.; Tscholl, D.W. Improving decision making through presentation of viscoelastic tests as a 3D animated blood clot: The visual clot. Anaesthesia 2020, 75, 1059–1069. [Google Scholar] [CrossRef]
- Molina, R.L.; Bobanski, L.; Dhingra-Kumar, N.; Moran, A.C.; Taha, A.; Kumar, S.; Semrau, K.E.A. The WHO safe childbirth checklist after 5 years: Future directions for improving outcomes. Lancet Glob. Health 2022, 10, e324–e325. [Google Scholar] [CrossRef] [PubMed]
- Abbott, T.E.F.; Ahmad, T.; Phull, M.K.; Fowler, A.J.; Hewson, R.; Biccard, B.M.; Chew, M.S.; Gillies, M.; Pearse, R.M.; (ISOS) Group. The surgical safety checklist and patient outcomes after surgery: A prospective observational cohort study, systematic review and meta-analysis. Br. J. Anaesth. 2018, 120, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.; Kessler, D.; Mackinnon, R.; Chang, T.P.; Nadkarni, V.M.; Hunt, E.A.; Duval-Arnould, J.; Lin, Y.; Cook, D.A.; Pusic, M.; et al. Reporting guidelines for health care simulation research: Extensions to the CONSORT and STROBE statements. Simul. Healthc. 2016, 11, 238–248. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Handschin, L.; Neubauer, P.; Weiss, M.; Seifert, B.; Spahn, D.R.; Noethiger, C.B. Using an animated patient avatar to improve perception of vital sign information by anaesthesia professionals. Br. J. Anaesth. 2018, 121, 662–671. [Google Scholar] [CrossRef] [Green Version]
- Roche, T.R.; Said, S.; Braun, J.; Maas, E.J.C.; Machado, C.; Grande, B.; Kolbe, M.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Avatar-based patient monitoring in critical anaesthesia events: A randomised high-fidelity simulation study. Br. J. Anaesth. 2021, 126, 1046–1054. [Google Scholar] [CrossRef] [PubMed]
- Tscholl, D.W.; Rössler, J.; Handschin, L.; Seifert, B.; Spahn, D.R.; Nöthiger, C.B. The mechanisms responsible for improved information transfer in avatar-based patient monitoring: Multicenter comparative eye-tracking study. J. Med. Internet Res. 2020, 22, e15070. [Google Scholar] [CrossRef] [PubMed]
- Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Noethiger, C.B.; Tscholl, D.W. Avatar-based patient monitoring with peripheral vision: A multicenter comparative eye-tracking study. J. Med. Internet Res. 2019, 21, e13041. [Google Scholar] [CrossRef]
- Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Noethiger, C.B.; Tscholl, D.W. Effects of a standardized distraction on caregivers’ perceptive performance with avatar-based and conventional patient monitoring: A multicenter comparative study. J. Clin. Monit. Comput. 2020, 34, 1369–1378. [Google Scholar] [CrossRef]
- Rössler, J.; Kaserer, A.; Albiez, B.; Braun, J.; Breckwoldt, J.; Spahn, D.R.; Nöthiger, C.; Tscholl, D.W. Comparing classroom instruction to individual instruction as an approach to teach avatar-based patient monitoring with visual patient: Simulation study. JMIR Med. Educ. 2020, 6, e17922. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Weiss, M.; Handschin, L.; Spahn, D.R.; Nöthiger, C.B. User perceptions of avatar-based patient monitoring: A mixed qualitative and quantitative study. BMC Anesthesiol. 2018, 18, 188. [Google Scholar] [CrossRef]
- Said, S.; Roche, T.R.; Braun, J.; Ganter, M.T.; Meybohm, P.; Herrmann, J.; Zacharowski, K.; Raimann, F.J.; Piekarski, F.; Rivas, E.; et al. Effects of an animated blood clot technology (visual clot) on the decision-making of users inexperienced in viscoelastic testing: Multicenter trial. J. Med. Internet Res. 2021, 23, e27124. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, C.; Braun, J.; Said, S.; Roche, T.R.; Nöthiger, C.B.; Spahn, D.R.; Tscholl, D.W.; Akbas, S. Faster time to treatment decision of viscoelastic coagulation test results through improved perception with the animated visual clot: A multicenter comparative eye-tracking study. Diagnostics 2022, 12, 1269. [Google Scholar] [CrossRef]
- Hart, S.G.; Staveland, L.E. Development of NASA-TLX (Task Load Index): Results of empirical and yheoretical research. Adv. Psychol. 1988, 52, 139–183. [Google Scholar]
- Lowndes, B.R.; Forsyth, K.L.; Blocker, R.C.; Dean, P.G.; Truty, M.J.; Heller, S.F.; Blackmon, S.; Hallbeck, M.S.; Nelson, H. NASA-TLX assessment of surgeon workload variation across specialties. Ann. Surg. 2020, 271, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Said, S.; Gozdzik, M.; Roche, T.R.; Braun, J.; Rössler, J.; Kaserer, A.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Validation of the raw national aeronautics and space administration task load index (NASA-TLX) questionnaire to assess perceived workload in patient monitoring tasks: Pooled analysis study using mixed models. J. Med. Internet Res. 2020, 22, e19472. [Google Scholar] [CrossRef]
- Tscholl, D.W.; Weiss, M.; Spahn, D.R.; Noethiger, C.B. How to conduct multimethod field studies in the operating room: The iPad combined with a survey app as a valid and reliable data collection tool. JMIR Res. Protoc. 2016, 5, e4. [Google Scholar] [CrossRef] [Green Version]
- Garot, O.; Rössler, J.; Pfarr, J.; Ganter, M.T.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W. Avatar-based versus conventional vital sign display in a central monitor for monitoring multiple patients: A multicenter computer-based laboratory study. BMC Med. Inform. Decis. Mak. 2020, 20, 26. [Google Scholar] [CrossRef] [Green Version]
- Wetli, D.J.; Bergauer, L.; Nöthiger, C.B.; Roche, T.R.; Spahn, D.R.; Tscholl, D.W.; Said, S. Improving visual-patient-avatar design prior to its clinical release: A mixed qualitative and quantitative study. Diagnostics 2022, 12, 555. [Google Scholar] [CrossRef]
- Ljubenovic, A.; Said, S.; Braun, J.; Grande, B.; Kolbe, M.; Spahn, D.R.; Nöthiger, C.B.; Tscholl, D.W.; Roche, T.R. Visual attention of anesthesia providers in simulated anesthesia emergencies using conventional number-based and avatar-based patient monitoring: Prospective eye-tracking study. JMIR Serious Games 2022, 10, e35642. [Google Scholar] [CrossRef] [PubMed]
- Akbas, S.; Said, S.; Roche, T.R.; Nöthiger, C.B.; Spahn, D.R.; Tscholl, D.W.; Bergauer, L. User perceptions of different vital signs monitor modalities during high-fidelity simulation: Semiquantitative analysis. JMIR Hum. Factors 2022, 9, e34677. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, Switzerland, 2016.
- Meara, J.G.; Leather, A.J.; Hagander, L.; Alkire, B.C.; Alonso, N.; Ameh, E.A.; Bickler, S.W.; Conteh, L.; Dare, A.J.; Davies, J.; et al. Global surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Int. J. Obstet. Anesth. 2016, 25, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Weiser, T.G.; Haynes, A.B.; Molina, G.; Lipsitz, S.R.; Esquivel, M.M.; Uribe-Leitz, T.; Fu, R.; Azad, T.; Chao, T.E.; Berry, W.R.; et al. Size and distribution of the global volume of surgery in 2012. Bull. World Health Organ. 2016, 94, 201–209F. [Google Scholar] [CrossRef]
- Budowski, A.D.; Bergauer, L.; Castellucci, C.; Braun, J.; Nöthiger, C.B.; Spahn, D.R.; Tscholl, D.W.; Roche, T.R. Improved task performance, low workload, and user-centered design in medical diagnostic equipment enhance decision confidence of anesthesia providers: A meta-analysis and a multicenter online survey. Diagnostics 2022, 12, 1835. [Google Scholar] [CrossRef]
- Stawschenko, E.; Schaller, T.; Kern, B.; Bode, B.; Dörries, F.; Kusche-Vihrog, K.; Gehring, H.; Wegerich, P. Current status of measurement accuracy for total hemoglobin concentration in the clinical context. Biosensors 2022, 12, 1147. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants, n/N (%) | 70 |
|---|---|
| Participants from USZ, n/N (%) | 35 (50) |
| Participants from UKW, n/N (%) | 18 (26) |
| Participants from UKF, n/N (%) | 17 (24) |
| Gender, female, n (%) | 42 (60) |
| Resident physicians, n (%) | 55 (79) |
| Staff physicians, n (%) | 15 (21) |
| Participant age in years, median (IQR) | 31 (28 to 35) |
| Work experience in years, median (IQR) | 3.5 (2 to 6) |
| Self-rated theoretical ABG skills (0 = novice, 100 = expert), Median (IQR) | 70 (58 to 78) |
| Parameter | Number (Percent) of Correct Visualisation Assignment | Estimated Proportion (95%CI) of Correct Visualisation Assignment |
|---|---|---|
| Lactate | 70 of 70 (100) | 1.00 |
| Methaemoglobin | 70 of 0 (100) | 1.00 |
| Partial pressure of carbon dioxide | 140 of 140 (100) | 1.00 |
| Osmolarity | 127 of 140 (91) | 0.99 (0.96 to 1.00) |
| Glucose | 138 of 140 (99) | 0.99 (0.97 to 1.00) |
| Anion gap | 133 of 140 (95) | 0.98 (0.95 to 0.99) |
| Chloride | 137 of 140 (98) | 0.98 (0.95 to 0.99) |
| Potassium | 137 of 140 (98) | 0.98 (0.95 to 0.99) |
| Calcium | 134 of 140 (96) | 0.97 (0.94 to 0.99) |
| Bicarbonate | 134 of 140 (96) | 0.97 (0.93 to 0.99) |
| Sodium | 133 of 140 (95) | 0.96 (0.92 to 0.98) |
| Carboxyhaemoglobin | 64 of 70 (91) | 0.94 (0.85 to 0.97) |
| pH value | 115 of 140 (82) | 0.94 (0.89 to 0.97) |
| Haemoglobin | 121 of 140 (86) | 0.89 (0.82 to 0.93) |
| Partial pressure of oxygen | 109 of 140 (78) | 0.87 (0.80 to 0.92) |
| P50 | 105 of 140 (75) | 0.86 (0.78 to 0.91) |
| Base excess | 104 of 140 (74) | 0.78 (0.69 to 0.85) |
| Oxygen saturation | 40 of 70 (57) | 0.58 (0.44 to 0.70) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schweiger, G.; Malorgio, A.; Henckert, D.; Braun, J.; Meybohm, P.; Hottenrott, S.; Froehlich, C.; Zacharowski, K.; Raimann, F.J.; Piekarski, F.; et al. Visual Blood, a 3D Animated Computer Model to Optimize the Interpretation of Blood Gas Analysis. Bioengineering 2023, 10, 293. https://doi.org/10.3390/bioengineering10030293
Schweiger G, Malorgio A, Henckert D, Braun J, Meybohm P, Hottenrott S, Froehlich C, Zacharowski K, Raimann FJ, Piekarski F, et al. Visual Blood, a 3D Animated Computer Model to Optimize the Interpretation of Blood Gas Analysis. Bioengineering. 2023; 10(3):293. https://doi.org/10.3390/bioengineering10030293
Chicago/Turabian StyleSchweiger, Giovanna, Amos Malorgio, David Henckert, Julia Braun, Patrick Meybohm, Sebastian Hottenrott, Corinna Froehlich, Kai Zacharowski, Florian J. Raimann, Florian Piekarski, and et al. 2023. "Visual Blood, a 3D Animated Computer Model to Optimize the Interpretation of Blood Gas Analysis" Bioengineering 10, no. 3: 293. https://doi.org/10.3390/bioengineering10030293