

A Real-Time Control Method for Upper Limb Exoskeleton Based on Active Torque Prediction Model

Abstract
:1. Introduction
2. Materials and Methods
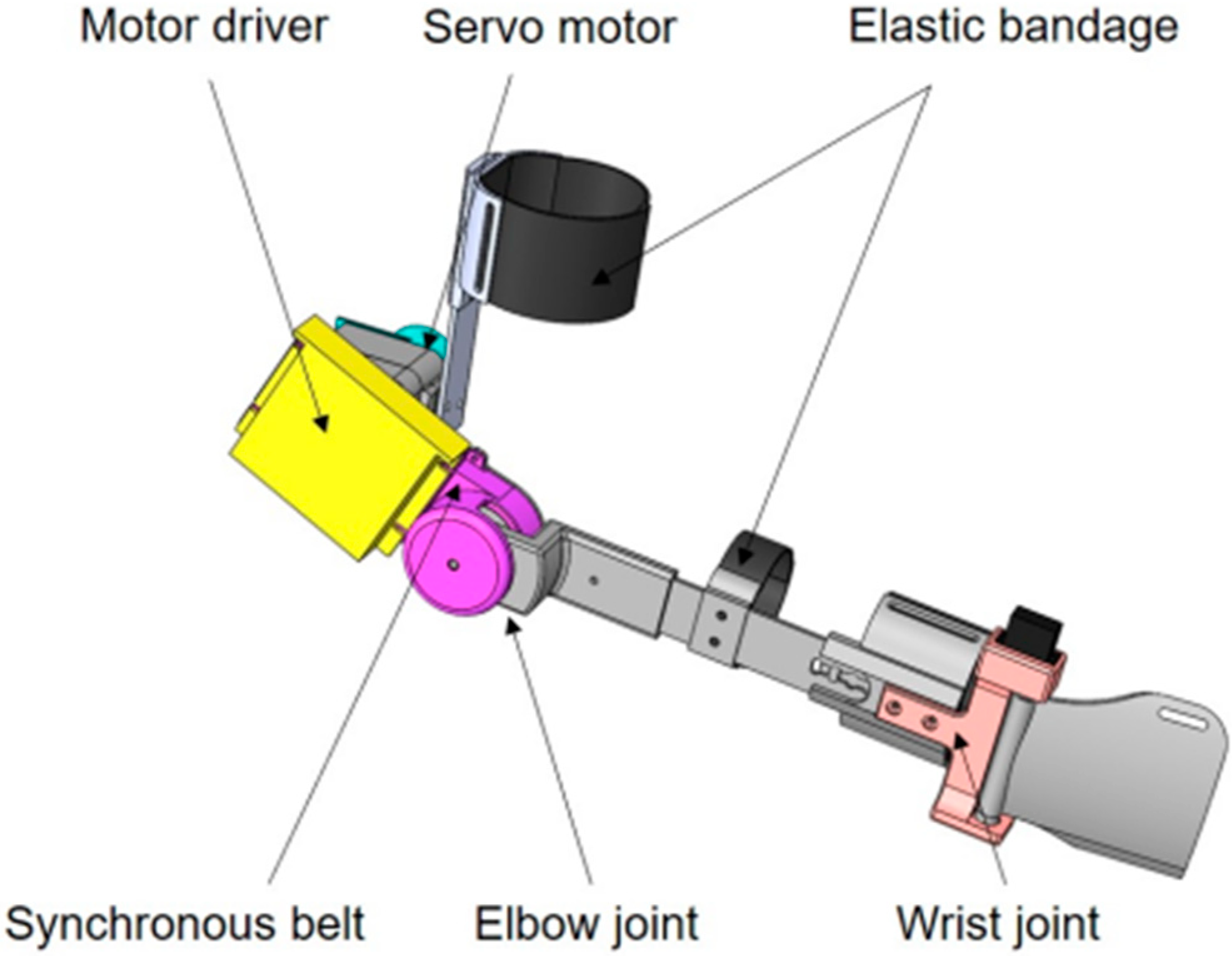
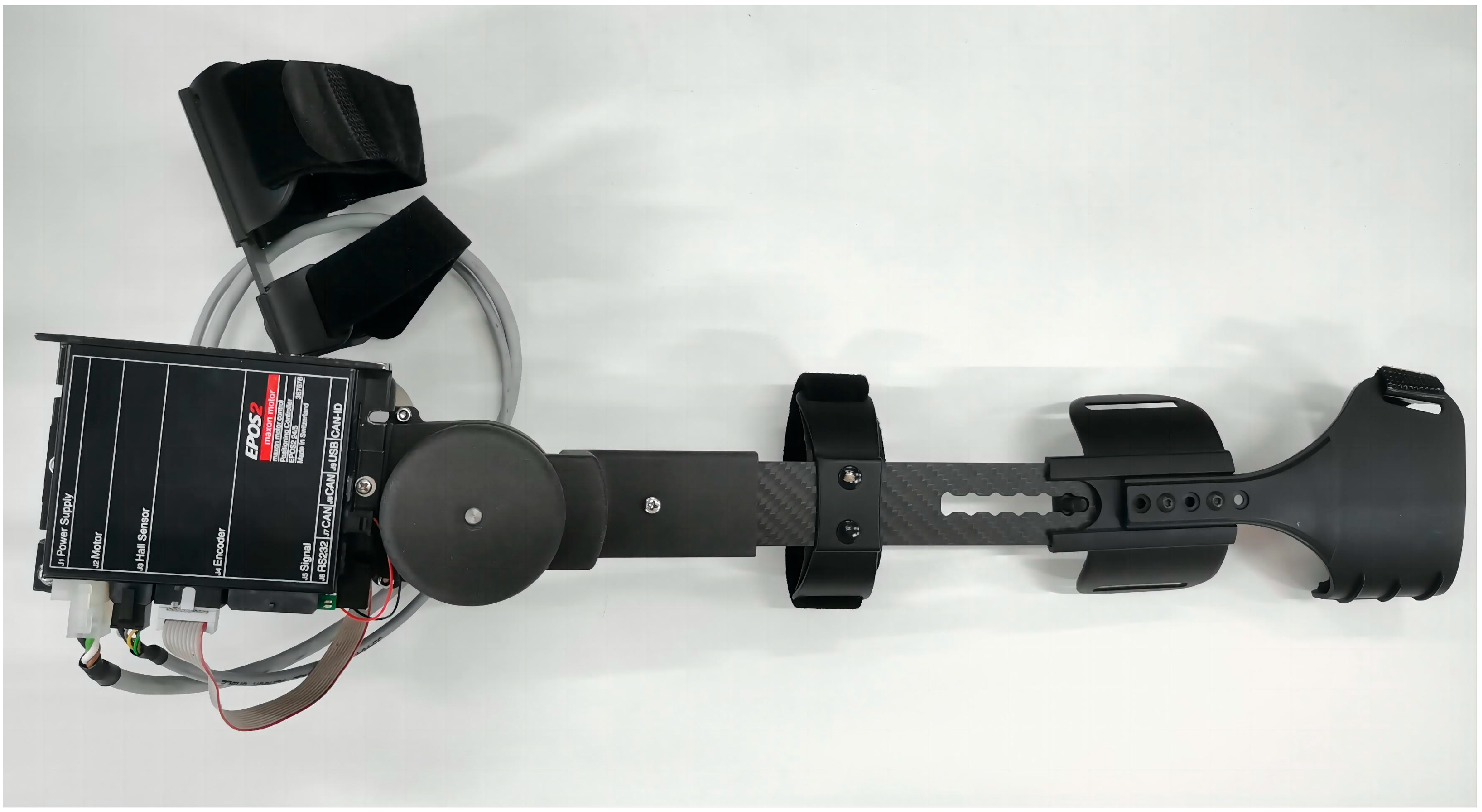
2.1. Upper Limb Rehabilitation Exoskeleton
2.2. Subject Information
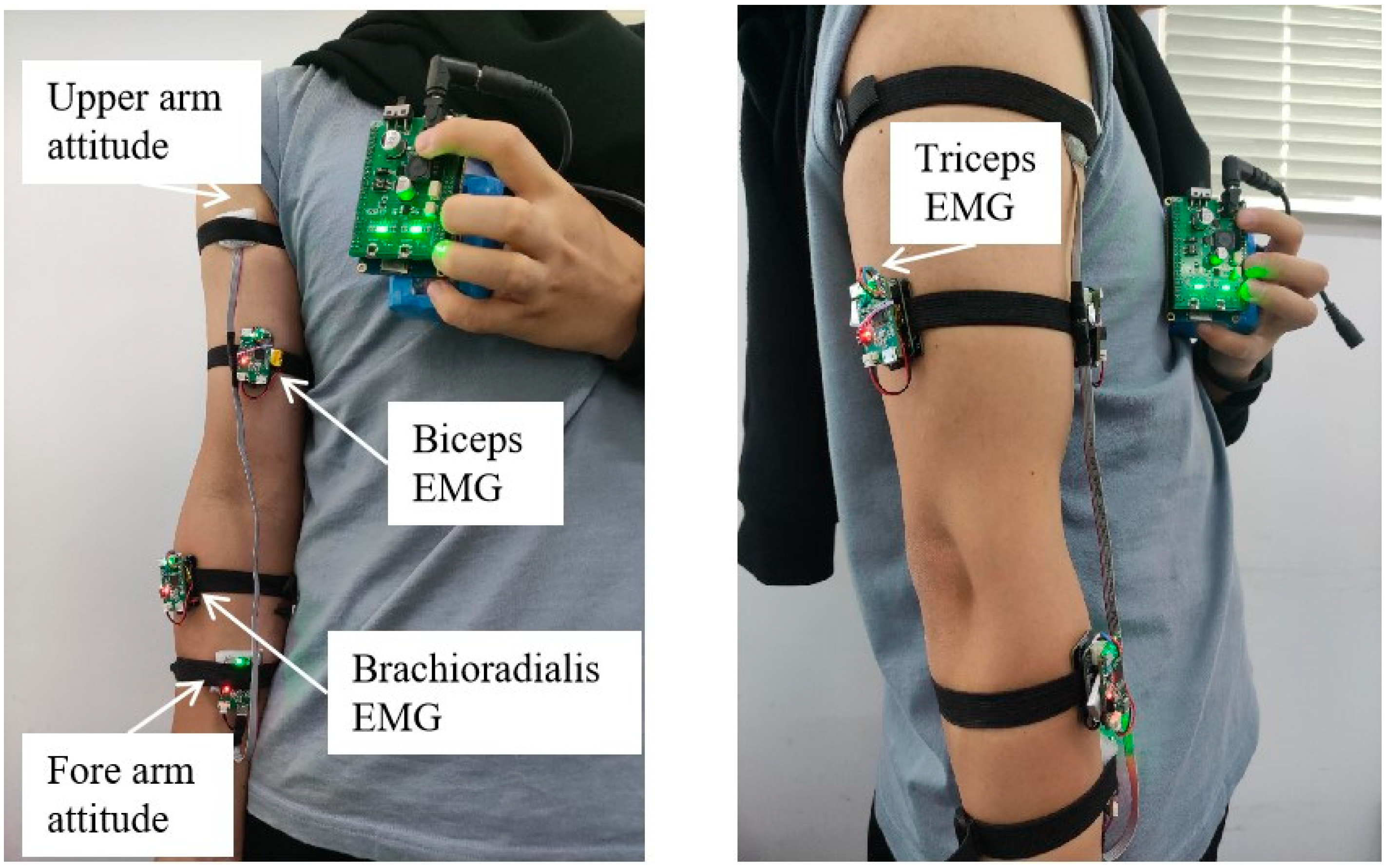
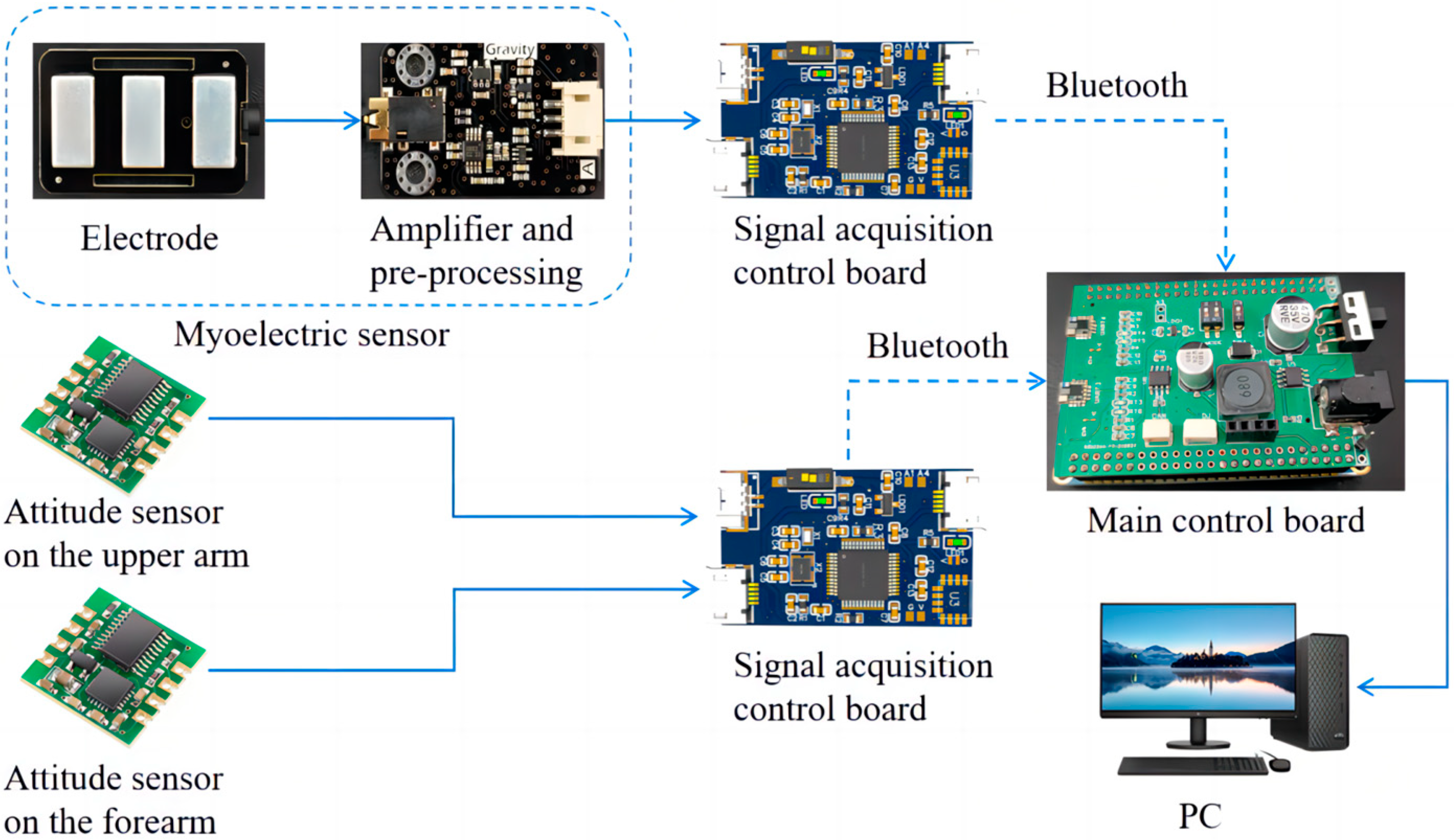
2.3. Data Acquisition
2.4. Data Processing and Feature Extraction
2.5. Multi-Modality Information Fusion
2.6. Active Torque Prediction Model
2.7. Real-Time Active Torque Control Protocol
2.8. Model Evaluation Index
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lu, T.; Wang, Y. Prediction Model Construction for Ischemic Stroke Recurrence with BP Network and Multivariate Logistic Regression and Effect of Individualized Health Education. Comput. Math. Methods Med. 2022, 2022, 4284566. [Google Scholar] [CrossRef]
- Gao, B.; Wei, C.; Ma, H.; Yang, S.; Ma, X.; Zhang, S. Real-Time Evaluation of the Signal Processing of sEMG Used in Limb Exoskeleton Rehabilitation System. Appl. Bionics Biomech. 2018, 2018, 1391032. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, Q.; Wang, Y.; Ru, F. Active Tracking Movements of Flexion and Extension on the Elbow Joint for an Initial Prototype of EMG-Driven Assistant Exoskeleton. In Proceedings of the 2017 IEEE International Conference on Robotics and Biomimetics (ROBIO), Macau, China, 5–8 December 2017; pp. 2687–2692. [Google Scholar]
- Song, R.; Tong, K.Y.; Hu, X.L.; Li, L. Assistive control system using continuous myoelectric signal in robot-aided arm training for patients after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Ghrouz, A.; Marco, E.; Muñoz-Redondo, E.; Boza, R.; Ramirez-Fuentes, C.; Duarte, E. The effect of motor relearning on balance, mobility and performance of activities of daily living among post-stroke patients: Study protocol for a randomised controlled trial. Eur. Stroke J. 2022, 7, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Bustamante Valles, K.; Montes, S.; Madrigal, M.D.J.; Burciaga, A.; Martínez, M.E.; Johnson, M.J. Technology-assisted stroke rehabilitation in Mexico: A pilot randomized trial comparing traditional therapy to circuit training in a Robot/technology-assisted therapy gym. J. Neuroeng. Rehabil. 2016, 13, 83. [Google Scholar] [CrossRef]
- Nicholson-Smith, C.; Mehrabi, V.; Atashzar, S.F.; Patel, R.V. A Multi-Functional Lower- and Upper-Limb Stroke Rehabilitation Robot. IEEE Trans. Med. Robot. Bionics 2020, 2, 549–552. [Google Scholar] [CrossRef]
- Uivarosan, D.; Bungau, S.G.; Nistor-Cseppento, C.D.; Negru, P.A.; Bungau, A.F.; Sabau, A.M.; Tit, D.M.; Uivaraseanu, B.; Radu, A.F. Application of Robotic Recovery Techniques to Stroke Survivors-Bibliometric Analysis. J. Pers. Med. 2022, 12, 2066. [Google Scholar] [CrossRef]
- Guo, S.X.; Ding, Y.B.; Guo, J. Control of A Lower Limb Exoskeleton Robot by Upper Limb sEMG Signal. In Proceedings of the 2021 IEEE International Conference on Mechatronics and Automation (ICMA), Takamatsu, Japan, 8–11 August 2021; pp. 1113–1118. [Google Scholar]
- Qassim, H.M.; Wan Hasan, W.Z. A Review on Upper Limb Rehabilitation Robots. Appl. Sci. 2020, 10, 6976. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, S.; Cao, K.; Wei, C.; Zhao, W.; Yao, J. Development of a Wearable Upper Limb Rehabilitation Robot Based on Reinforced Soft Pneumatic Actuators. Chin. J. Mech. Eng. 2022, 35, 83. [Google Scholar] [CrossRef]
- Nam, C.; Rong, W.; Li, W.; Cheung, C.; Ngai, W.; Cheung, T.; Pang, M.; Li, L.; Hu, J.; Wai, H. An Exoneuromusculoskeleton for Self-Help Upper Limb Rehabilitation After Stroke. Soft Robot. 2022, 9, 14–35. [Google Scholar] [CrossRef]
- Liu, Y.; Silva, R.M.; Friedrich, J.B.; Kao, D.S.; Mourad, P.D.; Bunnell, A.E. Surface Electromyography-Driven Therapeutic Gaming for Rehabilitation of Upper Extremity Weakness: A Pilot Study. Plast. Reconstr. Surg. 2022, 150, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Yang, C.; Xie, Q. The development of an Exoskeleton Robot for Co-Manipulation of Human Upper Limb Movement. In Proceedings of the 10th World Congress on Intelligent Control and Automation (WCICA 2012), Beijing, China, 6–8 July 2012; pp. 3909–3914. [Google Scholar]
- Singh, R.M.; Chatterji, S.; Kumar, A. A Review on Surface EMG based Control Schemes of Exoskeleton Robot in Stroke Rehabilitation. In Proceedings of the 2013 International Conference on Machine Intelligence and Research Advancement (ICMIRA 2013), Katra, India, 21–23 December 2013; pp. 310–315. [Google Scholar]
- Yahya, Y.Z.; Al-Sawaff, Z.H. Design and modeling of an upper limb exoskeleton to assist elbow joint movement using surface emg signals. Biomed. Eng. Appl. Basis Commun. 2020, 32, 9. [Google Scholar] [CrossRef]
- Parasuraman, S.; Oyong, A.W. Robot-assisted stroke rehabilitation: Joint torque/force conversion from emg using ga process. J. Mech. Med. Biol. 2011, 11, 827–843. [Google Scholar] [CrossRef]
- Son, J.; Rymer, W.Z. Effects of Changes in Ankle Joint Angle on the Relation Between Plantarflexion Torque and EMG Magnitude in Major Plantar Flexors of Male Chronic Stroke Survivors. Front. Neurol. 2020, 11, 224. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L. An upper limb movement estimation from electromyography by using BP neural network. Biomed. Signal Process. Control 2019, 49, 434–439. [Google Scholar]
- Asokan, A.; Vigneshwar, M.; IEEE. Design and Control of an EMG-based Low-cost Exoskeleton for Stroke Rehabilitation. In Proceedings of the 2019 5th Indian Control Conference (ICC), New Delhi, India, 9–11 January 2019; pp. 478–483. [Google Scholar]
- Wu, Q.; Chen, Y. Development of an Intention-Based Adaptive Neural Cooperative Control Strategy for Upper-Limb Robotic Rehabilitation. IEEE Robot. Autom. Lett. 2021, 6, 335–342. [Google Scholar] [CrossRef]
- Li, L.; Fu, Q.; Tyson, S.; Preston, N.; Weightman, A. A scoping review of design requirements for a home-based upper limb rehabilitation robot for stroke. Top. Stroke Rehabil. 2022, 29, 449–463. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, X.; Zhao, Z.Y.; Yang, J.H.; Lantz, V.; Wang, K.Q. Hand Gesture Recognition Research based on Surface EMG Sensors and 2D-Accelerometers. In Proceedings of the 11th IEEE International Symposium on Wearable Computers, Boston, MA, USA, 11–13 October 2007; p. 11. [Google Scholar]
- GB/T 10000-1988; Human Dimensions of Chinese Adults. Standardization Administration of China: Beijing, China, 1988.
- Liang, J.; Zhang, Q.; Liu, Y.; Wang, T.; Wan, G. A review of the design of load-carrying exoskeletons. Sci. China (Technol. Sci.) 2022, 65, 2051–2067. [Google Scholar] [CrossRef]
- Ma, Y.; Xie, S.Q.; Zhang, Y. A Patient-Specific EMG-Driven Musculoskeletal Model for Improving the Effectiveness of Robotic Neurorehabilitation. In Proceedings of the 7th International Conference on Intelligent Robotics and Applications (ICIRA), Guangzhou, China, 17–20 December 2014; Volume 8917, pp. 390–401. [Google Scholar]
- Li, Z.; Wang, B.; Sun, F.; Yang, C.; Xie, Q.; Zhang, W. sEMG-Based Joint Force Control for an Upper-Limb Power-Assist Exoskeleton Robot. IEEE J. Biomed. Health Inform. 2014, 18, 1043–1050. [Google Scholar]
- Kiguchi, K.; Hayashi, Y. An EMG-Based Control for an Upper-Limb Power-Assist Exoskeleton Robot. IEEE Trans. Syst. Man Cybern. Part B (Cybern.) 2012, 42, 1064–1071. [Google Scholar] [CrossRef]
- Fehr, J.; Fuhrer, J.; Kleinbach, C.; Hanss, M.; Eberhard, P. Fuzzy-Based Analysis of a Hill-Type Muscle Model. Proc. Appl. Math. Mech. 2016, 16, 31–34. [Google Scholar] [CrossRef]
- Bayo, E.; Garcia de Jalon, J.; Serna, M.A. A modified Lagrangian formulation for the dynamic analysis of constrained mechanical systems. Comput. Methods Appl. Mech. Eng. 1988, 71, 183–195. [Google Scholar] [CrossRef]
- Abiodun, O.I.; Jantan, A.; Omolara, A.E.; Dada, K.V.; Mohamed, N.A.; Arshad, H. State-of-the-art in artificial neural network applications: A survey. Heliyon 2018, 4, e00938. [Google Scholar] [CrossRef] [PubMed]
- Cleophas, T.J.; Cleophas, T.F. Artificial intelligence for diagnostic purposes: Principles, procedures and limitations. Clin. Chem. Lab. Med. 2010, 48, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.S.; Ezhilarasi, D. Performance Analysis of Super Twisting Sliding Mode Controller by ADAMS-MATLAB Co-simulation in Lower Extremity Exoskeleton. Int. J. Precis. Eng. Manuf. Green Technol. 2020, 7, 743–754. [Google Scholar] [CrossRef]
- Tahamipour-Z, S.M.; Kardan, I.; Kalani, H.; Akbarzadeh, A. A PSO-MLPANN Hybrid Approach for Estimation of Human Joint Torques from sEMG Signals. In Proceedings of the 2020 8th Iranian Joint Congress on Fuzzy and Intelligent Systems (CFIS), Mashhad, Iran, 2–4 September 2020. [Google Scholar]
- Huang, Y.; Chen, K.; Zhang, X.; Wang, K.; Ota, J. Joint torque estimation for the human arm from sEMG using backpropagation neural networks and autoencoders. Biomed. Signal Process. Control. 2020, 62, 102051. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, J.; Zeng, J.; Li, K.; Liu, H. Bio-signal based elbow angle and torque simultaneous prediction during isokinetic contraction. Sci. China Technol. Sci. 2019, 62, 21–30. [Google Scholar] [CrossRef]
- Bueno, D.R.; Montano, L.; IEEE. Multijoint Upper Limb Torque Estimation from sEMG Measurements. In Proceedings of the 2013 35th Annual International Conference of The IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 7233–7236. [Google Scholar]
- Ye, W.; Li, Z.; Yang, C.; Chen, F.; Su, C.Y. Motion Detection Enhanced Control of an Upper Limb Exoskeleton Robot for Rehabilitation Training. Int. J. Humanoid Robot. 2017, 14, 1650031. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Age | Height (cm) | Weight (kg) | Upper Arm Length (cm) | Forearm Length (cm) | Hand Length (cm) |
|---|---|---|---|---|---|---|
| 1 | 27 | 165 | 70.2 | 26.0 | 25.0 | 18.0 |
| 2 | 26 | 175 | 60.5 | 35.8 | 26.2 | 19.1 |
| 3 | 26 | 180 | 79.5 | 33.4 | 27.3 | 19.0 |
| 4 | 28 | 178 | 53.5 | 30.6 | 27.9 | 19.4 |
| 5 | 24 | 166 | 64.4 | 28.6 | 26.0 | 18.1 |
| 6 | 25 | 172 | 70.0 | 29.6 | 27.0 | 18.7 |
| 7 | 24 | 167 | 65.3 | 28.7 | 26.2 | 18.2 |
| Mean ± SD | 26 ± 2 | 173 ± 7 | 66.5 ± 13 | 30.9 ± 4.9 | 26.45 ± 1.45 | 18.7 ± 0.7 |
| Principal Component | Feature | Contribution Rate/% | Cumulative Contribution Rate/% |
|---|---|---|---|
| F1 | 6.4999 | 81.25 | 81.25 |
| F2 | 1.0455 | 13.07 | 94.32 |
| F3 | 0.2404 | 3.01 | 97.32 |
| F4 | 0.1251 | 1.56 | 98.89 |
| F5 | 0.0878 | 1.10 | 99.98 |
| F6 | 0.0006 | 0.01 | 99.99 |
| F7 | 0.0003 | 0.00 | 100.00 |
| F8 | 0.0003 | 0.00 | 100.00 |
| Population Size N | Learning Factor c1 | Maximum Iterations tmax | Linear Decrement in Inertial Weight | |
|---|---|---|---|---|
| Initial Value ωmax | Final Value ωmax | |||
| 100 | 2 | 2000 | 0.9 | 0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Zhang, L.; Meng, Q.; Yu, H. A Real-Time Control Method for Upper Limb Exoskeleton Based on Active Torque Prediction Model. Bioengineering 2023, 10, 1441. https://doi.org/10.3390/bioengineering10121441
Li S, Zhang L, Meng Q, Yu H. A Real-Time Control Method for Upper Limb Exoskeleton Based on Active Torque Prediction Model. Bioengineering. 2023; 10(12):1441. https://doi.org/10.3390/bioengineering10121441
Chicago/Turabian StyleLi, Sujiao, Lei Zhang, Qiaoling Meng, and Hongliu Yu. 2023. "A Real-Time Control Method for Upper Limb Exoskeleton Based on Active Torque Prediction Model" Bioengineering 10, no. 12: 1441. https://doi.org/10.3390/bioengineering10121441