

fNIRS-EEG BCIs for Motor Rehabilitation: A Review
 ,
,
Abstract
:
1. Introduction
2. Identified Publications
3. BCI Systems
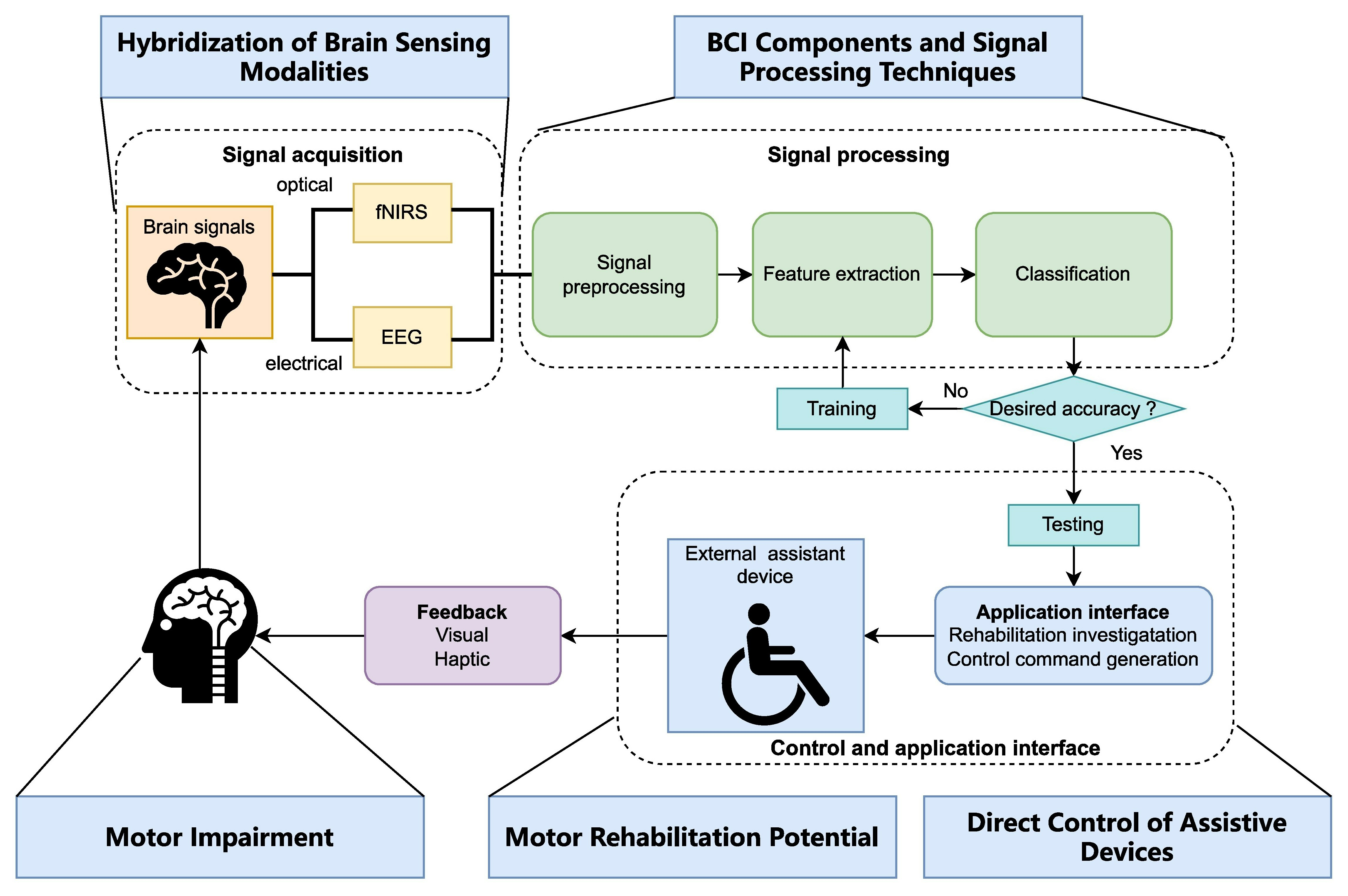
3.1. Typical BCI Structures
3.2. BCI Hardware
3.2.1. fNIRS Devices (Fiber/Fiberless)

3.2.2. fNIRS-EEG Devices
4. Signal Processing in fNIRS and fNIRS-EEG-Based BCIs
4.1. fNIRS-Based BCIs
4.1.1. Data Pre-Processing
4.1.2. Channel Selection and Features Extraction
Channel Selection
Features Extraction
4.1.3. Classification
Deep Learning
4.2. fNIRS-EEG-Based BCIs
4.2.1. Pre-Processing and Improved Reliability of Hybrid Signals
Features and Selection Methods
Sequential Data Processing
4.2.2. Classification for Hybrid fNIRS-EEG
Conventional Machine Learning Classification Algorithms
Deep Learning Classification Algorithms
5. Neuroscience and Clinical Applications
5.1. Upper Limb Applications
5.2. Lower Limb Applications
6. Discussion
6.1. Challenges and Opportunities of Hybrid fNIRS-EEG BCIs in Motor Rehabilitation
6.2. Future Prospects—BCI + ‘X’ for Motor Rehabilitation
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANN | artificial neural network |
| ANOVA | analysis of variance |
| BCI | brain–computer interface |
| Bi-LSTM | bidirectional long short-term memory |
| BMI | brain–machine interface |
| CAR | common average reference |
| CNN | convolutional neural networks |
| CNR | contrast-to-noise ratio |
| COD | cerebral oxygen exchange |
| CSP | common spatial patterns |
| CWT | continuous wavelet transforms |
| DL | deep learning |
| DNN | deep neural networks |
| DOT | diffuse optical tomography |
| DWT | discrete wavelet transforms |
| EEG | electroencephalograph |
| ELM | extreme learning machines |
| ELU | exponential linear unit |
| EMA | exponential moving averages |
| EMG | electromyography |
| ERD | event-related desynchronization |
| ERPs | event-related potentials |
| FES | functional electrical stimulation |
| FIR | finite impulse response |
| fNIRS | functional near-infrared spectroscopy |
| FWHM | full-width-half-maximum |
| GLM | general linear model |
| HbO | oxyhemoglobin |
| HbR | deoxyhemoglobin |
| HMM | hidden Markov model |
| hrf | hemodynamic response filter |
| IA | instantaneous amplitude |
| ICA | independent component analysis |
| IF | instantaneous frequency |
| IP | instantaneous phase |
| JMI | joint mutual information |
| k-NN | k-nearest neighbor |
| LDA | linear discriminant analysis |
| LSTM | long short-term memory |
| MACD | moving average convergence/divergence |
| MCF | multi-channel fusion |
| MCFHNet | multi-channel fusion hybrid network |
| MDL | minimum description length |
| ME | motor execution |
| MI | motor imagery |
| ML | machine learning |
| MLP | multilayer perceptron |
| MLPNN | multilayer perceptron neural network |
| NMES | neuromuscular electrical stimulation |
| PBL-McRBFN | projection-based learning in a meta-cognitive radial basis function network |
| PCA | principal component analysis |
| PD-CTC | proportional derivative computed torque controller |
| PMC | premotor cortex |
| PPC | posterior parietal cortex |
| PR | polynomial regression |
| QDA | quadratic discriminant analysis |
| RAGT | robot-assisted gait training |
| RCNN | recurrent convolutional neural network |
| SDS | source-detector separation |
| SMR | sensory motor rhythm |
| SVM | support vector machines |
| tES | transcranial electrical stimulation |
| TSC | time-series classification |
| WCs | wavelet coefficients |
| WT | wavelet transform |
References
- Cervera, M.A.; Soekadar, S.R.; Ushiba, J.; Millán, J.d.R.; Liu, M.; Birbaumer, N.; Garipelli, G. Brain-Computer Interfaces for Post-Stroke Motor Rehabilitation: A Meta-Analysis. Ann. Clin. Transl. Neurol. 2018, 5, 651–663. [Google Scholar] [CrossRef]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global Estimates of the Need for Rehabilitation Based on the Global Burden of Disease Study 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Hatem, S.M.; Saussez, G.; della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016, 10, 422. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Das, R.; Iversen, H.K.; Puthusserypady, S. Review on Motor Imagery Based BCI Systems for Upper Limb Post-Stroke Neurorehabilitation: From Designing to Application. Comput. Biol. Med. 2020, 123, 103843. [Google Scholar] [CrossRef]
- Ang, K.K.; Guan, C. Brain-Computer Interface in Stroke Rehabilitation. J. Comput. Sci. Eng. 2013, 7, 139–146. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Winstein, C.J. A Systematic Review of Voluntary Arm Recovery in Hemiparetic Stroke. J. Neurol. Phys. Ther. 2009, 33, 2–13. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Neurorehabil. Neural Repair 2017, 31, 793–799. [Google Scholar] [CrossRef]
- Belda-Lois, J.-M.; Mena-del Horno, S.; Bermejo-Bosch, I.; Moreno, J.C.; Pons, J.L.; Farina, D.; Iosa, M.; Molinari, M.; Tamburella, F.; Ramos, A.; et al. Rehabilitation of Gait after Stroke: A Review towards a Top-down Approach. J. Neuroeng. Rehabil. 2011, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Pomeroy, V.M.; Baron, J.C. Motor Imagery: A Backdoor to the Motor System after Stroke? Stroke 2006, 37, 1941–1952. [Google Scholar] [CrossRef]
- Ang, K.K.; Guan, C.; Chua, K.S.G.; Ang, B.T.; Kuah, C.W.K.; Wang, C.; Phua, K.S.; Chin, Z.Y.; Zhang, H. A Large Clinical Study on the Ability of Stroke Patients to Use an EEG-Based Motor Imagery Brain-Computer Interface. Clin. EEG Neurosci. 2011, 42, 253–258. [Google Scholar] [CrossRef]
- Jang, Y.Y.; Kim, T.H.; Lee, B.H. Effects of Brain-Computer Interface-Controlled Functional Electrical Stimulation Training on Shoulder Subluxation for Patients with Stroke: A Randomized Controlled Trial. Occup. Ther. Int. 2016, 23, 175–185. [Google Scholar] [CrossRef]
- Hong, K.S.; Khan, M.J.; Hong, M.J. Feature Extraction and Classification Methods for Hybrid FNIRS-EEG Brain-Computer Interfaces. Front. Hum. Neurosci. 2018, 12, 246. [Google Scholar] [CrossRef] [PubMed]
- Jöbsis, F.F. Noninvasive, Infrared Monitoring of Cerebral and Myocardial Oxygen Sufficiency and Circulatory Parameters. Science 1977, 198, 1264–1267. [Google Scholar] [CrossRef] [PubMed]
- Uchitel, J.; Vidal-Rosas, E.E.; Cooper, R.J.; Zhao, H. Wearable, Integrated Eeg–Fnirs Technologies: A Review. Sensors 2021, 21, 6106. [Google Scholar] [CrossRef] [PubMed]
- Leeb, R.; Tonin, L.; Rohm, M.; Desideri, L.; Carlson, T.; Millan, J.d.R. Towards Independence: A BCI Telepresence Robot for People With Severe Motor Disabilities. Proc. IEEE 2015, 103, 969–982. [Google Scholar] [CrossRef]
- Tonin, L.; Carlson, T.; Leeb, R.; Millan, J.d.R. Brain-Controlled Telepresence Robot by Motor-Disabled People. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 4227–4230. [Google Scholar]
- Pinti, P.; Aichelburg, C.; Lind, F.; Power, S.; Swingler, E.; Merla, A.; Hamilton, A.; Gilber, S.; Burgess, P.; Tachtsidis, I. Using Fiberless, Wearable Fnirs to Monitor Brain Activity in Real-World Cognitive Tasks. J. Vis. Exp. 2015, 2015, e53336. [Google Scholar] [CrossRef]
- Cooper, R.J.; Yucel, M.; Gagnon, L.; Suzuki, N.; Tanaka, N.; Reinsberger, C.; Boas, D.A.; Stufflebeam, S. Combining and Optimizing NIRS and EEG to Study Interictal Epileptic Discharges. In Biomedical Optics and 3-D Imaging; OSA: Washington, DC, USA, 2012; p. BSu2A.5. [Google Scholar]
- Goncharova, I.I.; McFarland, D.J.; Vaughan, T.M.; Wolpaw, J.R. EMG Contamination of EEG: Spectral and Topographical Characteristics. Clin. Neurophysiol. 2003, 114, 1580–1593. [Google Scholar] [CrossRef] [PubMed]
- Huo, C.; Xu, G.; Li, W.; Xie, H.; Zhang, T.; Liu, Y.; Li, Z. A Review on Functional Near-Infrared Spectroscopy and Application in Stroke Rehabilitation. Med. Nov. Technol. Devices 2021, 11, 100064. [Google Scholar] [CrossRef]
- Hong, K.S.; Khan, M.J. Hybrid Brain-Computer Interface Techniques for Improved Classification Accuracy and Increased Number of Commands: A Review. Front. Neurorobot. 2017, 11, 35. [Google Scholar] [CrossRef]
- Hramov, A.E.; Maksimenko, V.A.; Pisarchik, A.N. Physical Principles of Brain–Computer Interfaces and Their Applications for Rehabilitation, Robotics and Control of Human Brain States. Phys. Rep. 2021, 918, 1–133. [Google Scholar] [CrossRef]
- Leamy, D.J.; Collins, R.; Ward, T.E. Combining FNIRS and EEG to Improve Motor Cortex Activity Classification during an Imagined Movement-Based Task; Springer: Berlin/Heidelberg, Germany, 2011; pp. 177–185. [Google Scholar]
- Fazli, S.; Mehnert, J.; Steinbrink, J.; Curio, G.; Villringer, A.; Müller, K.R.; Blankertz, B. Enhanced Performance by a Hybrid NIRS-EEG Brain Computer Interface. Neuroimage 2012, 59, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Naseer, N.; Hong, K.S. FNIRS-Based Brain-Computer Interfaces: A Review. Front. Hum. Neurosci. 2015, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Yang, D.; Fang, F.; Hong, K.-S.; Reiss, A.L.; Zhang, Y. Concurrent FNIRS and EEG for Brain Function Investigation: A Systematic, Methodology-Focused Review. Sensors 2022, 22, 5865. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Shore, J.; Wang, M.; Yuan, F.; Buss, A.; Zhao, X. A Systematic Review on Hybrid EEG/FNIRS in Brain-Computer Interface. Biomed. Signal Process. Control 2021, 68, 102595. [Google Scholar] [CrossRef]
- Berger, A.; Horst, F.; Müller, S.; Steinberg, F.; Doppelmayr, M. Current State and Future Prospects of EEG and FNIRS in Robot-Assisted Gait Rehabilitation: A Brief Review. Front. Hum. Neurosci. 2019, 13, 172. [Google Scholar] [CrossRef] [PubMed]
- Holper, L.; Muehlemann, T.; Scholkmann, F.; Eng, K.; Kiper, D.; Wolf, M. Testing the Potential of a Virtual Reality Neurorehabilitation System during Performance of Observation, Imagery and Imitation of Motor Actions Recorded by Wireless Functional near-Infrared Spectroscopy (FNIRS). J. Neuroeng. Rehabil. 2010, 7, 57. [Google Scholar] [CrossRef]
- Schurholz, M.; Rana, M.; Robinson, N.; Ramos-Murguialday, A.; Cho, W.; Rohm, M.; Rupp, R.; Birbaumer, N.; Sitaram, R. Differences in Hemodynamic Activations between Motor Imagery and Upper Limb FES with NIRS. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, San Diego, CA, USA, 28 August–1 September 2012; pp. 4728–4731. [Google Scholar]
- Zimmermann, R.; Marchal-Crespo, L.; Edelmann, J.; Lambercy, O.; Fluet, M.-C.; Riener, R.; Wolf, M.; Gassert, R. Detection of Motor Execution Using a Hybrid FNIRS-Biosignal BCI: A Feasibility Study. J. Neuroeng. Rehabil. 2013, 10, 4. [Google Scholar] [CrossRef]
- Thanh Hai, N.; Cuong, N.Q.; Dang Khoa, T.Q.; Van Toi, V. Temporal Hemodynamic Classification of Two Hands Tapping Using Functional Near-Infrared Spectroscopy. Front. Hum. Neurosci. 2013, 7, 516. [Google Scholar] [CrossRef]
- Rea, M.; Rana, M.; Lugato, N.; Terekhin, P.; Gizzi, L.; Brötz, D.; Fallgatter, A.; Birbaumer, N.; Sitaram, R.; Caria, A. Lower Limb Movement Preparation in Chronic Stroke: A Pilot Study toward an FNIRS-BCI for Gait Rehabilitation. Neurorehabil. Neural Repair 2014, 28, 564–575. [Google Scholar] [CrossRef]
- Lee, J.; Mukae, N.; Arata, J.; Iwata, H.; Iramina, K.; Iihara, K.; Hashizume, M. A Multichannel-near-Infrared-Spectroscopy-Triggered Robotic Hand Rehabilitation System for Stroke Patients. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, London, UK, 17–20 July 2017; pp. 158–163. [Google Scholar]
- Trakoolwilaiwan, T.; Behboodi, B.; Lee, J.; Kim, K.; Choi, J.-W. Convolutional Neural Network for High-Accuracy Functional near-Infrared Spectroscopy in a Brain–Computer Interface: Three-Class Classification of Rest, Right-, and Left-Hand Motor Execution. Neurophotonics 2017, 5, 011008. [Google Scholar] [CrossRef]
- Khan, R.A.; Naseer, N.; Qureshi, N.K.; Noori, F.M.; Nazeer, H.; Khan, M.U. FNIRS-Based Neurorobotic Interface for Gait Rehabilitation. J. Neuroeng. Rehabil. 2018, 15, 7. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Mukae, N.; Arata, J.; Iihara, K.; Hashizume, M. Comparison of Feature Vector Compositions to Enhance the Performance of NIRS-BCI-Triggered Robotic Hand Orthosis for Post-Stroke Motor Recovery. Appl. Sci. 2019, 9, 3845. [Google Scholar] [CrossRef]
- Arivudaiyanambi, J.; M, S.; Chhabra, H.; Shajil, N.; Venkatasubramanian, G. Investigation of Deep Convolutional Neural Network for Classification of Motor Imagery FNIRS Signals for BCI Applications. Biomed. Signal Process. Control 2020, 62, 102133. [Google Scholar] [CrossRef]
- Hamid, H.; Naseer, N.; Nazeer, H.; Khan, M.J.; Khan, R.; Khan, U.S. Analyzing Classification Performance of FNIRS-BCI for Gait Rehabilitation Using Deep Neural Networks. Sensors 2022, 22, 1932. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.J.; Hong, K.-S.; Naseer, N.; Raheel Bhutta, M.; Yoon, S.-H. Hybrid EEG-NIRS BCI for Rehabilitation Using Different Brain Signals; The Annual Conference of the Society of Instrument and Control Engineers (SICE): Sapporo, Japan, 2014. [Google Scholar]
- Jawad Khan, M.; Hong, M.J.; Hong, K.S. Decoding of Four Movement Directions Using Hybrid NIRS-EEG Brain-Computer Interface. Front. Hum. Neurosci. 2014, 8, 244. [Google Scholar] [CrossRef]
- Koo, B.; Lee, H.G.; Nam, Y.; Kang, H.; Koh, C.S.; Shin, H.C.; Choi, S. A Hybrid NIRS-EEG System for Self-Paced Brain Computer Interface with Online Motor Imagery. J. Neurosci. Methods 2015, 244, 26–32. [Google Scholar] [CrossRef]
- Yin, X.; Xu, B.; Jiang, C.; Fu, Y.; Wang, Z.; Li, H.; Shi, G. A Hybrid BCI Based on EEG and FNIRS Signals Improves the Performance of Decoding Motor Imagery of Both Force and Speed of Hand Clenching. J. Neural Eng. 2015, 12, 036004. [Google Scholar] [CrossRef]
- Buccino, A.P.; Keles, H.O.; Omurtag, A. Hybrid EEG-FNIRS Asynchronous Brain-Computer Interface for Multiple Motor Tasks. PLoS ONE 2016, 11, e0146610. [Google Scholar] [CrossRef]
- Li, R.; Potter, T.; Huang, W.; Zhang, Y. Enhancing Performance of a Hybrid EEG-FNIRS System Using Channel Selection and Early Temporal Features. Front. Hum. Neurosci. 2017, 11, 462. [Google Scholar] [CrossRef]
- Chiarelli, A.M.; Croce, P.; Merla, A.; Zappasodi, F. Deep Learning for Hybrid EEG-FNIRS Brain-Computer Interface: Application to Motor Imagery Classification. J. Neural Eng. 2018, 15, 036028. [Google Scholar] [CrossRef]
- Wang, Z.; Zhou, Y.; Chen, L.; Gu, B.; Yi, W.; Liu, S.; Xu, M.; Qi, H.; He, F.; Ming, D. BCI Monitor Enhances Electroencephalographic and Cerebral Hemodynamic Activations during Motor Training. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 780–787. [Google Scholar] [CrossRef]
- Ghonchi, H.; Fateh, M.; Abolghasemi, V.; Ferdowsi, S.; Rezvani, M. Deep Recurrent-Convolutional Neural Network for Classification of Simultaneous EEG-FNIRS Signals. IET Signal Process. 2020, 14, 142–153. [Google Scholar] [CrossRef]
- Chen, J.; Wang, D.; Hu, B.; Yi, W.; Xu, M.; Chen, D.; Zhao, Q. MCFHNet: Multi-Channel Fusion Hybrid Network for Efficient EEG-FNIRS Multi-Modal Motor Imagery Decoding. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Glasgow, UK, 11–15 July 2022; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2022; pp. 4821–4825. [Google Scholar]
- Khan, H.; Naseer, N.; Yazidi, A.; Eide, P.K.; Hassan, H.W.; Mirtaheri, P. Analysis of Human Gait Using Hybrid EEG-FNIRS-Based BCI System: A Review. Front. Hum. Neurosci. 2021, 14, 613254. [Google Scholar] [CrossRef]
- Yücel, M.A.; Lühmann, A.; Scholkmann, F.; Gervain, J.; Dan, I.; Ayaz, H.; Boas, D.; Cooper, R.J.; Culver, J.; Elwell, C.E.; et al. Best Practices for FNIRS Publications. Neurophotonics 2021, 8, 012101. [Google Scholar] [CrossRef]
- Li, R.; Li, S.; Roh, J.; Wang, C.; Zhang, Y. Multimodal Neuroimaging Using Concurrent EEG/FNIRS for Poststroke Recovery Assessment: An Exploratory Study. Neurorehabil. Neural Repair 2020, 34, 1099–1110. [Google Scholar] [CrossRef]
- Liu, L.; Feng, L.; Wang, W.; Jin, M.; Qu, X.; Zhang, L.; Zhang, Q.; Jin, L. Effects of Brain Computer Interface-Robot System on Upper Limb Function Recovery in Stroke Patients: A Protocol Study for a Randomized Controlled Trial. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Lin, Q.; Zhang, Y.; Zhang, Y.; Zhuang, W.; Zhao, B.; Ke, X.; Peng, T.; You, T.; Jiang, Y.; Yilifate, A.; et al. The Frequency Effect of the Motor Imagery Brain Computer Interface Training on Cortical Response in Healthy Subjects: A Randomized Clinical Trial of Functional Near-Infrared Spectroscopy Study. Front. Neurosci. 2022, 16, 810553. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Cooper, R.J. Review of Recent Progress toward a Fiberless, Whole-Scalp Diffuse Optical Tomography System. Neurophotonics 2017, 5, 011012. [Google Scholar] [CrossRef] [PubMed]
- Gowerlabs Ltd. LUMO—FNIRS Neuroimaging Device. Available online: https://www.gowerlabs.co.uk/lumo (accessed on 13 May 2023).
- NIRx GmbH NIRx FNIRS/EEG Cap with Collocated Electrodes with FNIRS Probe. Available online: https://nirx.net/fnirs-eeg (accessed on 13 May 2023).
- Shimadzu Corporation. LABNIRS System. Available online: https://www.shimadzu.com/an/products/life-science-lab-instruments/imaging/labnirs/index.html (accessed on 12 May 2023).
- NIRx GmbH, Berlin, Germany. NIRScout. Available online: https://nirx.net/nirscout (accessed on 12 May 2023).
- g.Tec Medical Engineering GmbH G.GAMMAcap FNIRS System. Available online: https://www.gtec.at/2021/04/12/combining-fnirs-eeg-recordings/ (accessed on 13 May 2023).
- Wearable Sensing Wearable Sensing’s Wireless DSI-EEG+fNIRS System. Available online: https://wearablesensing.com/dsi-eegfnirs/ (accessed on 13 May 2023).
- Abibullaev, B.; An, J. Classification of Frontal Cortex Haemodynamic Responses during Cognitive Tasks Using Wavelet Transforms and Machine Learning Algorithms. Med. Eng. Phys. 2012, 34, 1394–1410. [Google Scholar] [CrossRef]
- Pinti, P.; Tachtsidis, I.; Hamilton, A.; Hirsch, J.; Aichelburg, C.; Gilbert, S.; Burgess, P.W. The Present and Future Use of Functional Near-Infrared Spectroscopy (Fnirs) for Cognitive Neuroscience. Ann. N. Y. Acad. Sci. 2020, 1464, 5–29. [Google Scholar] [CrossRef]
- Bonnal, J.; Monnet, F.; Le, B.T.; Pila, O.; Grosmaire, A.G.; Ozsancak, C.; Duret, C.; Auzou, P. Relation between Cortical Activation and Effort during Robot-Mediated Walking in Healthy People: A Functional Near-Infrared Spectroscopy Neuroimaging Study (FNIRS). Sensors 2022, 22, 5542. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.J.; Hong, K.S. Hybrid EEG-FNIRS-Based Eight-Command Decoding for BCI: Application to Quadcopter Control. Front. Neurorobot. 2017, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Naseer, N.; Noori, F.M.; Qureshi, N.K.; Hong, K.-S. Determining Optimal Feature-Combination for LDA Classification of Functional Near-Infrared Spectroscopy Signals in Brain-Computer Interface Application. Front. Hum. Neurosci. 2016, 10, 237. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Wang, S.; Xia, Y.; Zhu, X.; Evans, J.; Sun, Y.; He, S. CNN-Based Classification of FNIRS Signals in Motor Imagery BCI System. J. Neural Eng. 2021, 18, 056019. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, R.A.; Vasilakos, A. Brain Computer Interface: Control Signals Review. Neurocomputing 2017, 223, 26–44. [Google Scholar] [CrossRef]
- Zafar, A.; Hong, K.-S.; Khan, M.J. Initial Dip Detection Based on Both HbO and HbR Vector-Based Phase Analysis. In Proceedings of the 2016 55th Annual Conference of the Society of Instrument and Control Engineers of Japan (SICE), Tsukuba, Japan, 20–23 September 2016; pp. 543–548. [Google Scholar]
- Power, S.D.; Kushki, A.; Chau, T. Automatic Single-Trial Discrimination of Mental Arithmetic, Mental Singing and the No-Control State from Prefrontal Activity: Toward a Three-State NIRS-BCI. BMC Res. Notes 2012, 5, 141. [Google Scholar] [CrossRef] [PubMed]
- Noori, F.M.; Naseer, N.; Qureshi, N.K.; Nazeer, H.; Khan, R.A. Optimal Feature Selection from FNIRS Signals Using Genetic Algorithms for BCI. Neurosci. Lett. 2017, 647, 61–66. [Google Scholar] [CrossRef]
- Saeedi, S.; Carlson, T.; Chavarriaga, R.; Millán, J.D.R. Making the Most of Context-Awareness in Brain-Computer Interfaces. In Proceedings of the 2013 IEEE International Conference on Cybernetics, CYBCONF, Lausanne, Switzerland, 13–15 June 2013; pp. 68–73. [Google Scholar]
- Saadati, M.; Nelson, J.; Ayaz, H. Convolutional Neural Network for Hybrid FNIRS-EEG Mental Workload Classification. In Advances in Intelligent Systems and Computing; Springer: Cham, Switzerland, 2020; pp. 221–232. ISBN 978-3-030-20472-3. [Google Scholar]
- Shin, J.; von Luhmann, A.; Blankertz, B.; Kim, D.-W.; Jeong, J.; Hwang, H.-J.; Muller, K.-R. Open Access Dataset for EEG+NIRS Single-Trial Classification. IEEE. Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1735–1745. [Google Scholar] [CrossRef]
- van Dokkum, L.E.H.; Ward, T.; Laffont, I. Brain Computer Interfaces for Neurorehabilitation-Its Current Status as a Rehabilitation Strategy Post-Stroke. Ann. Phys. Rehabil. Med. 2015, 58, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.M.; Safa, S.N.; Ashik, M.H.; Masud, M.; Alzain, M.A. Research and Development of a Brain-Controlled Wheelchair for Paralyzed Patients. Intell. Autom. Soft. Comput. 2021, 30, 49–64. [Google Scholar] [CrossRef]
- Carlson, T.; Del, R.; Millan, J. Brain-Controlled Wheelchairs: A Robotic Architecture. IEEE Robot. Autom. Mag. 2013, 20, 65–73. [Google Scholar] [CrossRef]
- Yang, M.; Yang, Z.; Yuan, T.; Feng, W.; Wang, P. A Systemic Review of Functional Near-Infrared Spectroscopy for Stroke: Current Application and Future Directions. Front. Neurol. 2019, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Blokland, Y.; Spyrou, L.; Thijssen, D.; Eijsvogels, T.; Colier, W.; Floor-Westerdijk, M.; Vlek, R.; Bruhn, J.; Farquhar, J. Combined EEG-FNIRS Decoding of Motor Attempt and Imagery for Brain Switch Control: An Offline Study in Patients With Tetraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 222–229. [Google Scholar] [CrossRef]
- Levac, D.E.; Sveistrup, H. Motor Learning and Virtual Reality; Springer: New York, NY, USA, 2014; pp. 25–46. [Google Scholar]
- Pavlidou, A.; Walther, S. Using Virtual Reality as a Tool in the Rehabilitation of Movement Abnormalities in Schizophrenia. Front. Psychol. 2021, 11, 607312. [Google Scholar] [CrossRef] [PubMed]
- Sebastián-Romagosa, M.; Udina, E.; Ortner, R.; Dinarès-Ferran, J.; Cho, W.; Murovec, N.; Matencio-Peralba, C.; Sieghartsleitner, S.; Allison, B.Z.; Guger, C. EEG Biomarkers Related With the Functional State of Stroke Patients. Front. Neurosci. 2020, 14, 582. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. (★ Clinical) | Feature Extraction (FE)/Channel Selection (CS) | Features | Classifier |
|---|---|---|---|
| ★ [29] | - | Median of HbO, HbR | ANOVA |
| [30] | FE: GLM | HbO, HbR | SVM |
| [31] | FE: Linear-combination-based | HbO, HbR | HMM |
| [32] | FE: PR algorithm | HbO | SVM, ANN |
| ★ [33] | CS: Individual-based T-map | Mean of HbT | LDA |
| ★ [34] | - | HbO, HbD | LDA, SVM |
| [35] | FE: Convolutional filters | HbO, HbR | SVM, ANN, CNN |
| ★ [36] | - | HbO, HbR (mean, peak, variance, slope, kurtosis, skewness) | k-NN, QDA, LDA, Naïve Bayes, SVM |
| ★ [37] | CS: CNR | HbO, HbR (mean, slope) | LDA |
| [38] | - | HbO, HbR, HbT, HbD (mean, peak, variance) | ML: SVM, MLPNN, PBL-McRBFN DL: CNN |
| ★ [39] | - | HbO, HbR (mean, peak, variance, kurtosis, skewness) | ML: k-NN, SVM, LDA DL: CNN, LSTM, Bi-LSTM |
| Ref. (★ Clinical) | Feature Extraction (FE)/Channel Selection (CS) | fNIRS Features | EEG Features | Classifier |
|---|---|---|---|---|
| [23] | - | HbO, HbR | µ, β-band | LDA |
| [24] | - | HbO, HbR | α, β-band | LDA |
| ★ [40] | - | HbO, HbR | α, β-band (peak) | SVM |
| [41] | - | HbO and HbR (mean) | β-band (mean, peak) | LDA |
| [42] | - | HbO | δ, θ, α, β-band | SVM |
| [43] | FE: JMI | HbR, HbO, HbT, HbD | μ, β-band (time-phase-frequency features) | ELM |
| [44] | FE: CSP | HbO, HbR (mean, slope) | μ, β-band | LDA |
| [45] | CS: GLM FE: PCA (fNIRS), DWT(EEG) | HbO, HbR, initial dip | DWT (approximation coefficients) | SVM |
| [46] | - | HbO, HbR | μ, β-band | SVM, LDA, DNN |
| ★ [47] | FE: CSP | HbO, HbR (peak, peak latency, integral area) | α, β-band | ANOVA, SVM |
| [48] | - | HbO, HbR | α, β-band | CNN-LSTM |
| [49] | - | HbO, HbR (mean) | δ, θ, α, β-band (mean) | DNN, CNN, CNN-LSTM, MCFHNet |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Xia, Y.; Zhou, X.; Vidal Rosas, E.; Thomas, A.; Loureiro, R.; Cooper, R.J.; Carlson, T.; Zhao, H. fNIRS-EEG BCIs for Motor Rehabilitation: A Review. Bioengineering 2023, 10, 1393. https://doi.org/10.3390/bioengineering10121393
Chen J, Xia Y, Zhou X, Vidal Rosas E, Thomas A, Loureiro R, Cooper RJ, Carlson T, Zhao H. fNIRS-EEG BCIs for Motor Rehabilitation: A Review. Bioengineering. 2023; 10(12):1393. https://doi.org/10.3390/bioengineering10121393
Chicago/Turabian StyleChen, Jianan, Yunjia Xia, Xinkai Zhou, Ernesto Vidal Rosas, Alexander Thomas, Rui Loureiro, Robert J. Cooper, Tom Carlson, and Hubin Zhao. 2023. "fNIRS-EEG BCIs for Motor Rehabilitation: A Review" Bioengineering 10, no. 12: 1393. https://doi.org/10.3390/bioengineering10121393