
Development of a Machine Learning Model for Predicting Weaning Outcomes Based Solely on Continuous Ventilator Parameters during Spontaneous Breathing Trials
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
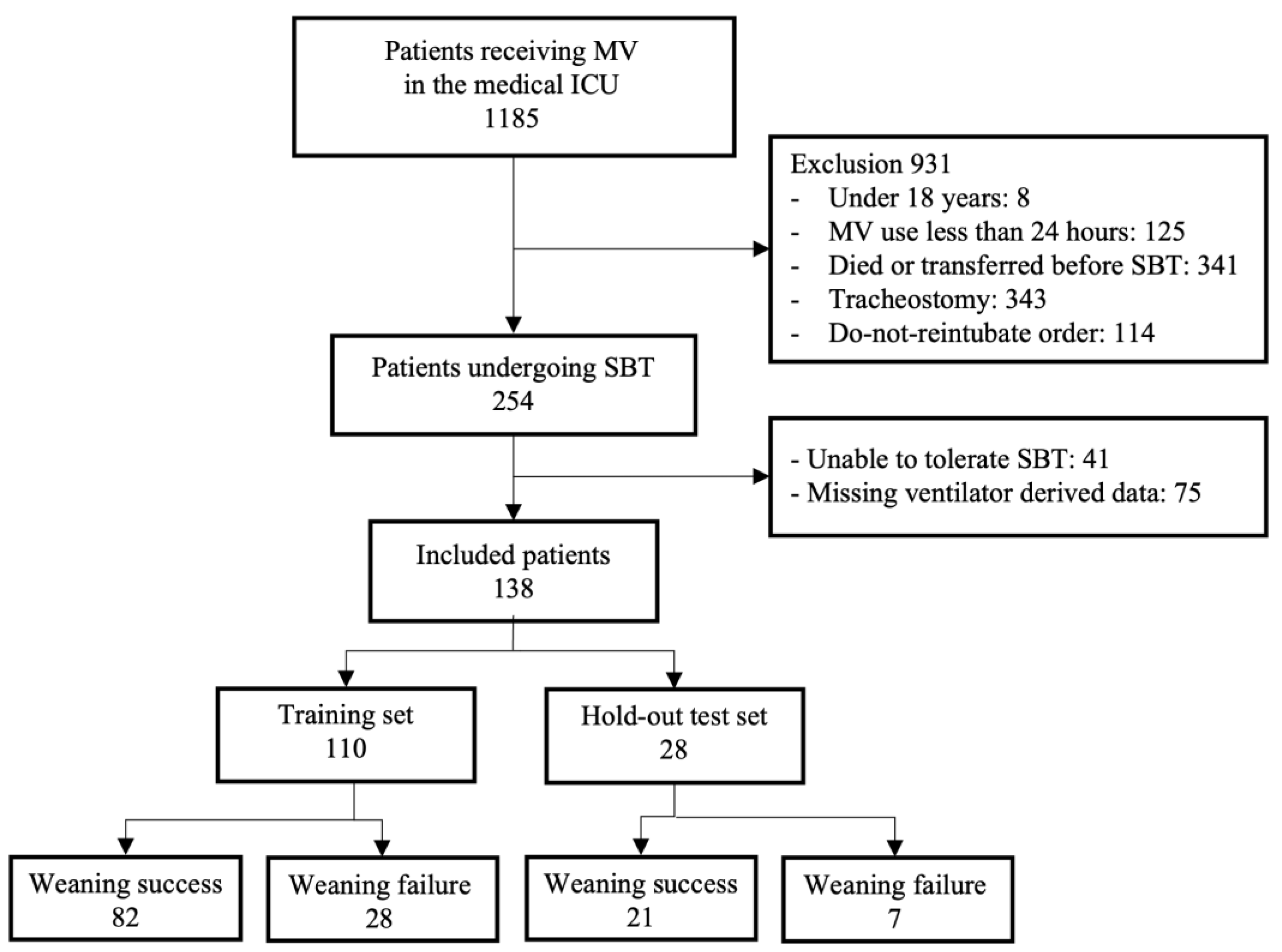
2.1. Data Sources and Participants
2.2. Study Design
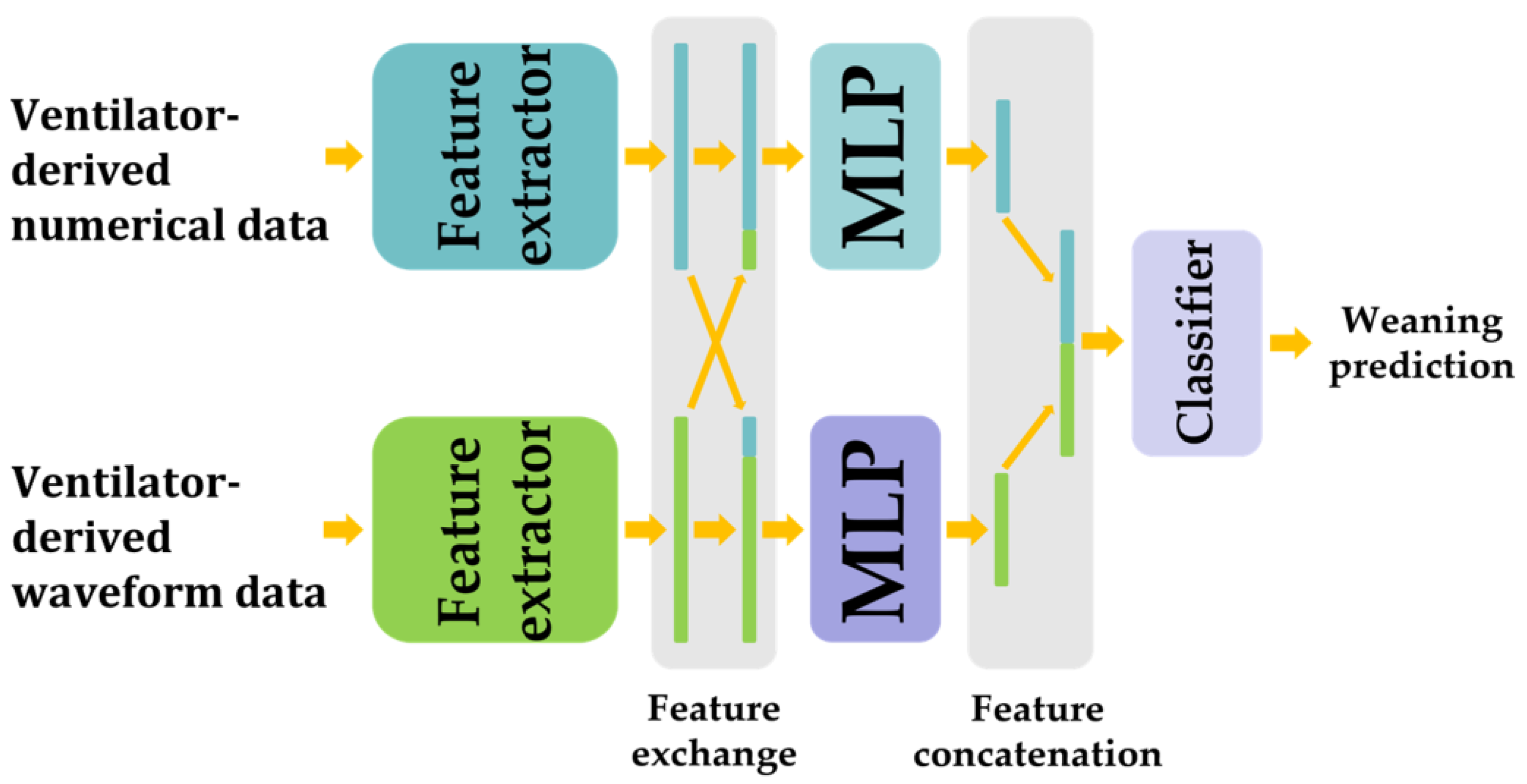
2.3. Proposed Weaning Prediction Model
2.3.1. Data Flow
2.3.2. Feature Extractor and Classifier
2.3.3. MLP and Subblock
2.4. Training and Validation
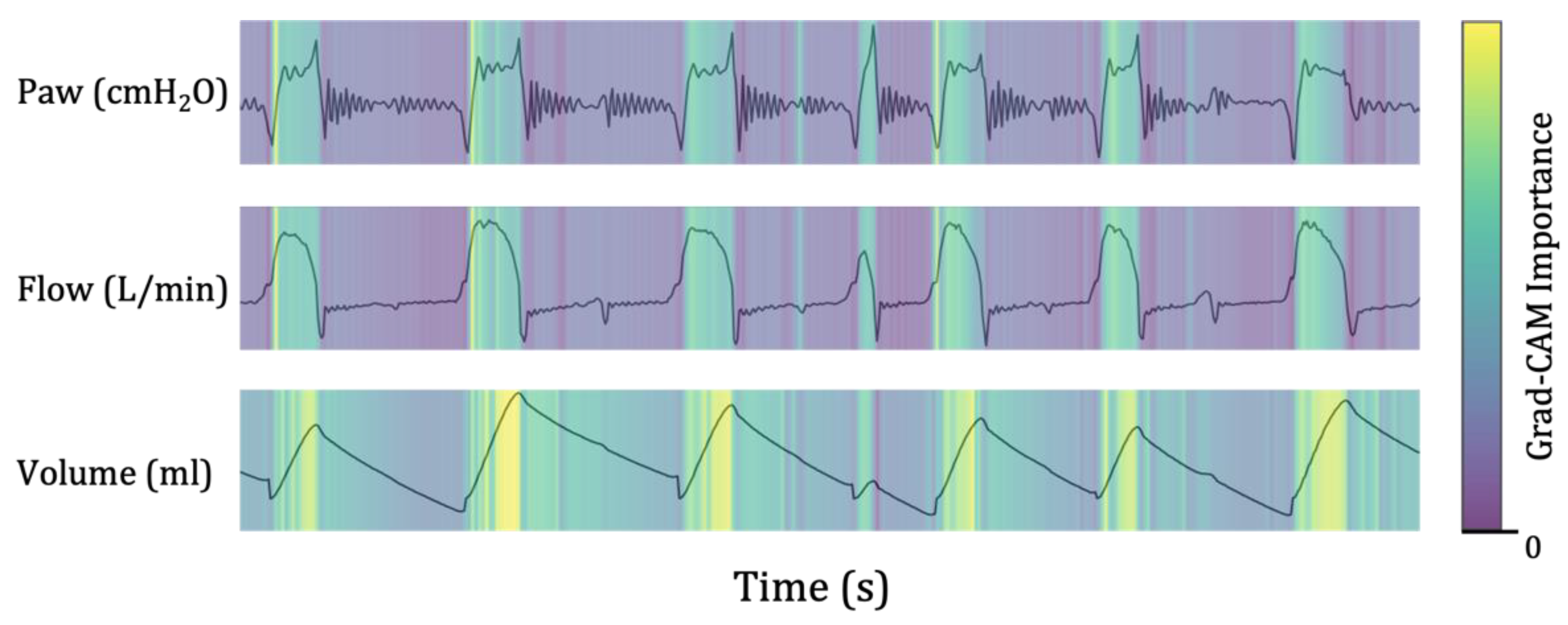
2.5. Gradient-Weighted Class Activation Mapping
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Weaning Prediction Performance
3.3. Gradient-Weighted Class Activation Mapping
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Esteban, A.; Alía, I.; Gordo, F.; Fernández, R.; Solsona, J.F.; Vallverdú, I.; Macías, S.; Allegue, J.M.; Blanco, J.; Carriedo, D.; et al. Extubation outcome after spontaneous breathing trials with T-tube or pressure support ventilation. The Spanish Lung Failure Collaborative Group. Am. J. Respir. Crit. Care Med. 1997, 156, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Chastre, J.; Fagon, J.Y. Ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.K.; Ciubotaru, R.L.; Wong, J.B. Effect of failed extubation on the outcome of mechanical ventilation. Chest 1997, 112, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Gershengorn, H.B. International Variation in Intubation and Extubation Practices and Adverse Events Among Critically Ill Patients Receiving Mechanical Ventilation. Jama 2021, 325, 1157–1159. [Google Scholar] [CrossRef]
- Rajakaruna, C.; Rogers, C.A.; Angelini, G.D.; Ascione, R. Risk factors for and economic implications of prolonged ventilation after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2005, 130, 1270–1277. [Google Scholar] [CrossRef]
- Rello, J.; Ollendorf, D.A.; Oster, G.; Vera-Llonch, M.; Bellm, L.; Redman, R.; Kollef, M.H. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 2002, 122, 2115–2121. [Google Scholar] [CrossRef]
- De Jonghe, B.; Bastuji-Garin, S.; Durand, M.C.; Malissin, I.; Rodrigues, P.; Cerf, C.; Outin, H.; Sharshar, T. Respiratory weakness is associated with limb weakness and delayed weaning in critical illness. Crit. Care Med. 2007, 35, 2007–2015. [Google Scholar] [CrossRef]
- Russotto, V.; Myatra, S.N.; Laffey, J.G.; Tassistro, E.; Antolini, L.; Bauer, P.; Lascarrou, J.B.; Szuldrzynski, K.; Camporota, L.; Pelosi, P.; et al. Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients From 29 Countries. Jama 2021, 325, 1164–1172. [Google Scholar] [CrossRef]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Vieillard-Baron, A.; et al. Weaning from mechanical ventilation. Eur. Respir. J. 2007, 29, 1033–1056. [Google Scholar] [CrossRef]
- Epstein, S.K. Weaning from ventilatory support. Curr. Opin. Crit. Care 2009, 15, 36–43. [Google Scholar] [CrossRef]
- Frutos-Vivar, F.; Ferguson, N.D.; Esteban, A.; Epstein, S.K.; Arabi, Y.; Apezteguía, C.; González, M.; Hill, N.S.; Nava, S.; D’Empaire, G.; et al. Risk factors for extubation failure in patients following a successful spontaneous breathing trial. Chest 2006, 130, 1664–1671. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.L.; Tobin, M.J. A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N. Engl. J. Med. 1991, 324, 1445–1450. [Google Scholar] [CrossRef]
- Matava, C.; Pankiv, E.; Ahumada, L.; Weingarten, B.; Simpao, A. Artificial intelligence, machine learning and the pediatric airway. Paediatr. Anaesth. 2020, 30, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Feng, T.; Thapa-Chhetry, B.; Cho, B.G.; Shum, T.; Inwald, D.P.; Newth, C.J.L.; Vaidya, V.U. Machine learning model for early prediction of acute kidney injury (AKI) in pediatric critical care. Crit. Care 2021, 25, 288. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, S.; Lai, K.; Chen, Z.; Wan, J.; Xu, Y. Machine learning for the prediction of acute kidney injury in critical care patients with acute cerebrovascular disease. Ren. Fail. 2022, 44, 43–53. [Google Scholar] [CrossRef]
- Alderden, J.; Pepper, G.A.; Wilson, A.; Whitney, J.D.; Richardson, S.; Butcher, R.; Jo, Y.; Cummins, M.R. Predicting Pressure Injury in Critical Care Patients: A Machine-Learning Model. Am. J. Crit. Care 2018, 27, 461–468. [Google Scholar] [CrossRef]
- Moll, M.; Qiao, D.; Regan, E.A.; Hunninghake, G.M.; Make, B.J.; Tal-Singer, R.; McGeachie, M.J.; Castaldi, P.J.; San Jose Estepar, R.; Washko, G.R.; et al. Machine Learning and Prediction of All-Cause Mortality in COPD. Chest 2020, 158, 952–964. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.L.; Huang, M.H.; Lee, C.Y.; Lai, W.W. Data Science for Extubation Prediction and Value of Information in Surgical Intensive Care Unit. J. Clin. Med. 2019, 8, 1709. [Google Scholar] [CrossRef]
- Park, J.E.; Kim, T.Y.; Jung, Y.J.; Han, C.; Park, C.M.; Park, J.H.; Park, K.J.; Yoon, D.; Chung, W.Y. Biosignal-Based Digital Biomarkers for Prediction of Ventilator Weaning Success. Int. J. Environ. Res. Public Health 2021, 18, 9229. [Google Scholar] [CrossRef]
- Zhao, Q.Y.; Wang, H.; Luo, J.C.; Luo, M.H.; Liu, L.P.; Yu, S.J.; Liu, K.; Zhang, Y.J.; Sun, P.; Tu, G.W.; et al. Development and Validation of a Machine-Learning Model for Prediction of Extubation Failure in Intensive Care Units. Front. Med. 2021, 8, 676343. [Google Scholar] [CrossRef]
- Jia, Y.; Kaul, C.; Lawton, T.; Murray-Smith, R.; Habli, I. Prediction of weaning from mechanical ventilation using Convolutional Neural Networks. Artif. Intell. Med. 2021, 117, 102087. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, N.R.; Cook, D.J.; Ely, E.W., Jr.; Epstein, S.K.; Fink, J.B.; Heffner, J.E.; Hess, D.; Hubmayer, R.D.; Scheinhorn, D.J. Evidence-based guidelines for weaning and discontinuing ventilatory support: A collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest 2001, 120, 375s–395s. [Google Scholar] [CrossRef] [PubMed]
- Esteban, A.; Frutos, F.; Tobin, M.J.; Alía, I.; Solsona, J.F.; Valverdú, I.; Fernández, R.; de la Cal, M.A.; Benito, S.; Tomás, R.; et al. A comparison of four methods of weaning patients from mechanical ventilation. Spanish Lung Failure Collaborative Group. N. Engl. J. Med. 1995, 332, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Roh, J.H.; Synn, A.; Lim, C.M.; Suh, H.J.; Hong, S.B.; Huh, J.W.; Koh, Y. A weaning protocol administered by critical care nurses for the weaning of patients from mechanical ventilation. J. Crit. Care 2012, 27, 549–555. [Google Scholar] [CrossRef]
- Schmidt, G.A.; Girard, T.D.; Kress, J.P.; Morris, P.E.; Ouellette, D.R.; Alhazzani, W.; Burns, S.M.; Epstein, S.K.; Esteban, A.; Fan, E.; et al. Liberation From Mechanical Ventilation in Critically Ill Adults: Executive Summary of an Official American College of Chest Physicians/American Thoracic Society Clinical Practice Guideline. Chest 2017, 151, 160–165. [Google Scholar] [CrossRef]
- Howard, A.; Sandler, M.; Chen, B.; Wang, W.; Chen, L.C.; Tan, M.; Chu, G.; Vasudevan, V.; Zhu, Y.; Pang, R.; et al. Searching for MobileNetV3. In Proceedings of the 2019 IEEE/CVF International Conference on Computer Vision (ICCV), Seoul, Korea, 27 October–2 November 2019; pp. 1314–1324. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Iandola, F.N.; Han, S.; Moskewicz, M.W.; Ashraf, K.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50x fewer parameters and< 0.5 MB model size. arXiv 2016, arXiv:1602.07360. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. In Proceedings of the International Conference on Machine Learning, Lille, France, 7–9 July 2015; pp. 448–456. [Google Scholar]
- Elfwing, S.; Uchibe, E.; Doya, K. Sigmoid-weighted linear units for neural network function approximation in reinforcement learning. Neural Netw. 2018, 107, 3–11. [Google Scholar] [CrossRef]
- Loshchilov, I.; Hutter, F. Decoupled weight decay regularization. arXiv 2017, arXiv:1711.05101. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE international Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Wightman, R. PyTorch Image Models. 2019. Available online: https://doi.org/10.5281/zenodo.7618837 (accessed on 4 October 2023).
- Georgopoulos, D.; Prinianakis, G.; Kondili, E. Bedside waveforms interpretation as a tool to identify patient-ventilator asynchronies. Intensive Care Med. 2006, 32, 34–47. [Google Scholar] [CrossRef]
- de Haro, C.; Ochagavia, A.; López-Aguilar, J.; Fernandez-Gonzalo, S.; Navarra-Ventura, G.; Magrans, R.; Montanyà, J.; Blanch, L.; de Haro, C.; López-Aguilar, J.; et al. Patient-ventilator asynchronies during mechanical ventilation: Current knowledge and research priorities. Intensive Care Med. Exp. 2019, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Fabregat, A.; Magret, M.; Ferré, J.A.; Vernet, A.; Guasch, N.; Rodríguez, A.; Gómez, J.; Bodí, M. A Machine Learning decision-making tool for extubation in Intensive Care Unit patients. Comput. Methods Programs Biomed. 2021, 200, 105869. [Google Scholar] [CrossRef]
- Bien, M.Y.; Shui Lin, Y.; Shih, C.H.; Yang, Y.L.; Lin, H.W.; Bai, K.J.; Wang, J.H.; Ru Kou, Y. Comparisons of predictive performance of breathing pattern variability measured during T-piece, automatic tube compensation, and pressure support ventilation for weaning intensive care unit patients from mechanical ventilation. Crit. Care Med. 2011, 39, 2253–2262. [Google Scholar] [CrossRef] [PubMed]
- Bien, M.Y.; Hseu, S.S.; Yien, H.W.; Kuo, B.I.; Lin, Y.T.; Wang, J.H.; Kou, Y.R. Breathing pattern variability: A weaning predictor in postoperative patients recovering from systemic inflammatory response syndrome. Intensive Care Med. 2004, 30, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Wysocki, M.; Cracco, C.; Teixeira, A.; Mercat, A.; Diehl, J.L.; Lefort, Y.; Derenne, J.P.; Similowski, T. Reduced breathing variability as a predictor of unsuccessful patient separation from mechanical ventilation. Crit. Care Med. 2006, 34, 2076–2083. [Google Scholar] [CrossRef]
- Perren, A.; Brochard, L. Managing the apparent and hidden difficulties of weaning from mechanical ventilation. Intensive Care Med. 2013, 39, 1885–1895. [Google Scholar] [CrossRef]
- Jubran, A.; Tobin, M.J. Pathophysiologic basis of acute respiratory distress in patients who fail a trial of weaning from mechanical ventilation. Am. J. Respir. Crit. Care Med. 1997, 155, 906–915. [Google Scholar] [CrossRef]
- McConville, J.F.; Kress, J.P. Weaning Patients from the Ventilator. N. Engl. J. Med. 2012, 367, 2233–2239. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MobileNetV3 Operator | Expand Size | Out Channel | Activation Function | |
|---|---|---|---|---|
| Feature extractor | Conv2d | - | 16 | H-Swish |
| bneck, 3 × 3 | 16 | 16 | ReLU | |
| bneck, 3 × 3 | 64 | 24 | ReLU | |
| bneck, 3 × 3 | 72 | 24 | ReLU | |
| bneck, 5 × 5 | 72 | 32 | ReLU | |
| bneck, 5 × 5 | 96 | 32 | ReLU | |
| bneck, 5 × 5 | 96 | 32 | ReLU | |
| bneck, 3 × 3 | 192 | 64 | H-Swish | |
| bneck, 3 × 3 | 160 | 64 | H-Swish | |
| bneck, 3 × 3 | 144 | 64 | H-Swish | |
| bneck, 3 × 3 | 144 | 64 | H-Swish | |
| bneck, 3 × 3 | 384 | 88 | H-Swish | |
| bneck, 3 × 3 | 528 | 88 | H-Swish | |
| bneck, 5 × 5 | 528 | 120 | H-Swish | |
| bneck, 5 × 5 | 720 | 120 | H-Swish | |
| bneck, 5 × 5 | 720 | 120 | H-Swish | |
| Conv2d, 1 × 1 | - | 720 | H-Swish | |
| Pool, 7 × 7 | - | - | - | |
| Classifier | Conv2d, 1 × 1, NBN | - | 1280 | H-Swish |
| Conv2d, 1 × 1, NBN | - | 1 | - |
| Total (N = 138) | Success Group (N = 103) | Failure Group (N = 35) | p Value | |
|---|---|---|---|---|
| Age, mean ± SD, y | 68.4 ± 15.1 | 68.9 ± 14.6 | 67.0 ± 16.6 | 0.507 |
| Sex, male/female, n | 87/51 | 67/36 | 20/15 | 0.403 |
| Body weight, mean ± SD, kg | 59.7 ± 14.3 | 60.8 ± 15.0 | 56.6 ± 11.5 | 0.136 |
| Height, mean ± SD, cm | 164.2 ± 9.6 | 164.1 ± 9.9 | 164.4 ± 8.6 | 0.899 |
| BMI, mean ± SD, kg/m2 | 22.1 ± 4.6 | 22.5 ± 4.8 | 20.9 ± 3.7 | 0.072 |
| Main cause of ICU admission, n, % | 0.869 | |||
| Pneumonia | 99 (71.7) | 76 (73.8) | 23 (65.7) | |
| COPD/Asthma AE | 10 (7.2) | 7 (6.8) | 3 (8.6) | |
| Pulmonary hemorrhage | 3 (2.2) | 2 (1.9) | 1 (2.9) | |
| Sepsis | 4 (2.9) | 3 (2.9) | 1 (2.9) | |
| Gastrointestinal bleeding | 2 (1.4) | 2 (1.9) | 0 (0) | |
| Neurologic disease | 2 (1.4) | 1 (1.0) | 1 (2.9) | |
| Pulmonary edema | 9 (6.5) | 6 (5.8) | 3 (8.6) | |
| Others | 9 (6.5) | 6 (5.8) | 3 (8.6) | |
| APACHE II score, mean ± SD | 22.6 ± 8.3 | 23.0 ± 8.4 | 21.5 ± 7.9 | 0.332 |
| Comorbidity, n, % | ||||
| HTN | 62 (44.9) | 47 (45.6) | 20 (42.9) | 0.776 |
| Diabetes mellitus | 41 (29.7) | 35 (34.0) | 6 (17.1) | 0.060 |
| COPD | 13 (9.4) | 8 (7.8) | 5 (14.3) | 0.315 |
| Chronic lung disease | 40 (29.0) | 26 (25.2) | 14 (40.0) | 0.096 |
| Neurological disease | 46 (33.3) | 34 (33.0) | 12 (34.3) | 0.890 |
| Cancer | 27 (19.6) | 22 (21.4) | 5 (14.3) | 0.362 |
| Renal disease | 15 (10.9) | 13 (12.6) | 2 (5.7) | 0.355 |
| Liver disease | 12 (8.7) | 10 (9.7) | 2 (5.7) | 0.730 |
| Residence type before admission | 0.411 | |||
| Home | 99 (71.7) | 72 (69.9) | 27 (77.1) | |
| Hospital or nursing home | 39 (28.3) | 31 (30.1) | 8 (22.9) | |
| ABGA before SBT | ||||
| PaO2 | 106.6 ± 32.1 | 107.8 ± 29.7 | 103.3 ± 38.5 | 0.478 |
| PaCO2 | 37.6 ± 10.2 | 36.6 ± 9.9 | 40.3 ± 10.8 | 0.063 |
| PF ratio | 319.5 ± 100.1 | 325.4 ± 92.8 | 302.1 ± 118.6 | 0.235 |
| Length of mechanical ventilation before SBT, mean ± SD | 7.7 ± 6.2 | 7.53 ± 6.5 | 8.2 ± 4.8 | 0.598 |
| Prior failed weaning attempt | 20 (14.5) | 13 (12.6) | 7 (20.0) | 0.284 |
| Use of NMBAs | 25 (18.1) | 18 (17.5) | 7 (20.0) | 0.738 |
| AUROC | AUPRC | Sensitivity | Specificity | NPV | PPV | Accuracy | F1 Score | |
|---|---|---|---|---|---|---|---|---|
| ML model | 0.912 (0.795–1.000) | 0.767 (0.434–0.983) | 0.857 (0.555–1.000) | 0.808 (0.619–0.952) | 0.943 (0.800–1.000) | 0.608 (0.286–0.889) | 0.821 (0.679–0.929) | 0.698 (0.400–0.909) |
| RBSI | 0.558 (0.265–0.871) | 0.522 (0.148–0.841) | 0.423 (0.000–0.833) | 0.907 (0.762–1.000) | 0.820 (0.667–0.958) | 0.607 (0.001–0.999) | 0.783 (0.607–0.929) | 0.476 (0.001–0.824) |
| Authors | Data Source | Variables | ML Model | Performance | Study Design |
|---|---|---|---|---|---|
| Tsai et al. [18] | Surgical ICU (n = 704) | 17 features
| Machine learning ensemble | Sensitivity: 0.830, Specificity: 0.890 | Retrospective |
| Fabregat et al. [37] | ICU (n = 697) | 20 features
| Support vector machine | AUC: 0.98 | Retrospective |
| Zhao et al. [20] | MIMIC-IV (n = 16,189) | 19 features
| Categorical boosting (CatBoost) | AUC: (internal) 0.835, (external) 0.803 | Retrospective (development), Prospective (validation) |
| Jia et al. [21] | MIMIC-III (n = 2299) | 25 features
| 1d-CNN | AUC: 0.94 | Retrospective |
| Park et al. [19] | Medical ICU (n = 89) | 10 features
| Random forest | AUC: 0.81 | Retrospective |
| Park et al. | Medical ICU (n = 138) | 28 features
| CNN | AUC: 0.912 | Retrospective |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.E.; Kim, D.Y.; Park, J.W.; Jung, Y.J.; Lee, K.S.; Park, J.H.; Sheen, S.S.; Park, K.J.; Sunwoo, M.H.; Chung, W.Y. Development of a Machine Learning Model for Predicting Weaning Outcomes Based Solely on Continuous Ventilator Parameters during Spontaneous Breathing Trials. Bioengineering 2023, 10, 1163. https://doi.org/10.3390/bioengineering10101163
Park JE, Kim DY, Park JW, Jung YJ, Lee KS, Park JH, Sheen SS, Park KJ, Sunwoo MH, Chung WY. Development of a Machine Learning Model for Predicting Weaning Outcomes Based Solely on Continuous Ventilator Parameters during Spontaneous Breathing Trials. Bioengineering. 2023; 10(10):1163. https://doi.org/10.3390/bioengineering10101163
Chicago/Turabian StylePark, Ji Eun, Do Young Kim, Ji Won Park, Yun Jung Jung, Keu Sung Lee, Joo Hun Park, Seung Soo Sheen, Kwang Joo Park, Myung Hoon Sunwoo, and Wou Young Chung. 2023. "Development of a Machine Learning Model for Predicting Weaning Outcomes Based Solely on Continuous Ventilator Parameters during Spontaneous Breathing Trials" Bioengineering 10, no. 10: 1163. https://doi.org/10.3390/bioengineering10101163