
Potential Application of Lung Ultrasound in Children with Severe Uncontrolled Asthma: Preliminary Hypothesis Based on a Case Series

 ,
,
Abstract
:1. Introduction
- 2 children with acute asthma attack and history of allergic asthma, but not adequately controlled with therapy;
- 1 child with acute asthma attack and history of childhood asthma not adequately controlled with therapy;
- 2 children with acute asthma attack and with history, respectively, of childhood asthma and allergic asthma adequately controlled with therapy; and finally,
- 1 child with severe asthma in the absence of exacerbation.
2. Case Descriptionts
2.1. Case 1
2.2. Case 2
2.3. Case 3
2.4. Case 4
2.5. Case 5
2.6. Case 6
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- GINA Guidelines. Adolescents and Adult with Difficult to Treat and Severe Asthma. Available online: www.ginaasthma.org (accessed on 6 May 2019).
- British Thoracic Society; Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. Thorax 2016, 69, 1–192. [Google Scholar]
- Bateman, E.D.; Hurd, S.S.; Barnes, P.J.; Bousquet, J.; Drazen, J.M.; FitzGerald, M.; Gibson, P.; Ohta, K.; O’Byrne, P.; Pedersen, S.E.; et al. Global strategy for asthma management and prevention: GINA executive summary. Eur. Respir. J. 2008, 31, 143–178. [Google Scholar] [CrossRef] [PubMed]
- Varshney, T.; Mok, E.; Shapiro, A.J.; Li, P.; Dubrovsky, A.S. Point-of-care lung ultrasound in young children with respiratory tract infections and wheeze. Emerg. Med. J. 2016, 33, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Dankoff, S.; Li, P.; Shapiro, A.J.; Varshney, T.; Dubrovsky, A.S. Point of care lung ultrasound of children with acute asthma exacerbations in the pediatric ED. Am. J. Emerg. Med. 2017, 35, 615–622. [Google Scholar] [CrossRef] [PubMed]
- King, G.G.; Farrow, C.E.; Chapman, D.G. Dismantling the pathophysiology of asthma using imaging. Eur. Respir. Rev. 2019, 28, 180111. [Google Scholar] [CrossRef] [PubMed]
- Cattarossi, L.; Copetti, R.; Poskurica, B. Radiation Exposure Early in Life Can Be Reduced by Lung Ultrasound. Chest 2011, 139, 730–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpicelli, G. Lung Sonography. J. Ultrasound Med. 2013, 32, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Musolino, A.M.; Tomà, P.; Supino, M.C.; Scialanga, B.; Mesturino, A.; Scateni, S.; Battaglia, M.; Pirozzi, N.; Bock, C.; Buonsenso, D. Lung ultrasound features of children with complicated and non-complicated community acquired pneumonia: A prospective study. Pediatr. Pulmonol. 2019, 54, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Tomà, P. Lung ultrasound in pediatric radiology-cons. Pediatr. Radiol. 2020, 50, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.C.; Ringel, L.; Dyjack, N.; Herrin, R.; Woodruff, P.G.; Rios, C.; O’Connor, B.; Fahy, J.V.; Seibold, M.A. A transcriptomics method to determine airway immune dysfunction in T2 high and T2 low asthma. Am. J. Respir. Crit. Care Med. 2019, 199, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Chupp, G. Phenotypes and endotypes of adult asthma: Moving toward precision medicine. J. Allergy Clin. Immunol. 2019, 144, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Berce, V.; Tomazin, M.; Gorenjak, M.; Berce, T.; Lovrenčič, B. The Usefulness of Lung Ultrasound for the Aetiological Diagnosis of Community-Acquired Pneumonia in Children. Sci. Rep. 2019, 9, 17957. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Musolino, A.; Ferro, V.; De Rose, C.; Morello, R.; Ventola, C.; Liotti, F.M.; De Sanctis, R.; Chiaretti, A.; Biasucci, D.G.; et al. Role of lung ultrasound for the etiological diagnosis of acute lower respiratory tract infection (ALRTI) in children: A prospective study. J. Ultrasound 2021, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Buckmaster, A.; Boon, R. Reduce the rads: A quality assurance project on reducing unnecessary chest X-rays in children with asthma. J. Paediatr. Child Health 2005, 41, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Soldati, G.; Demi, M.; Inchingolo, R.; Smargiassi, A.; Demi, L. On the Physical Basis of Pulmonary Sonographic Interstitial Syndrome. J. Ultrasound Med. 2016, 35, 2075–2086. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | |
|---|---|---|---|---|---|---|
| Years and Gender | 8-year-old Female | 10-year-old Male | 2-year-old Female | 10-year-old Male | 3-year-and-5-month-old Female | 10-year-old Female |
| Asthmatic phenotype | T2—atopic, non-eosinophilic | T2—atopic, hypereosinophilic | Recurrent wheezing/Childhood Asthma | T2—atopic, hypereosinophilic phenotype | Recurrent wheezing/Childhood Asthma | T2—atopic, eosinophilic phenotype—“T2-high” |
| ACT | 19 | 18 | / | 25 | / | 20 |
| Clinical presentation | Acute Asthmatic Attack -Severe dyspnea and tachypnea -Absence of language -Tachycardia -OSI: 88% | Acute Asthmatic Attack -Severe dyspnea and tachypnea -Absence of language -Tachycardia -OSI: 88–90% | Acute Asthmatic Attack/Asthamatic Bronchitis -Moderate dyspna -Presence of language -Fever and rhinitis -Stable vital signs | Acute Asthmatic Attack -Mild dyspnea -Presence of linguage -Stable vital signs | Acute Asthmatic Attack/Asthamatic Bronchitis -Mild dyspnea -Presence of language -Fever and rhinitis -Stable vital signs | Absence of acute state -Recurrent symptoms (cough, wheezing, fatigue) |
| Severity grading of acute asthmatic attack | Moderate–Severe | Moderate–Severe | Mild–Moderate | Mild | Mild | / |
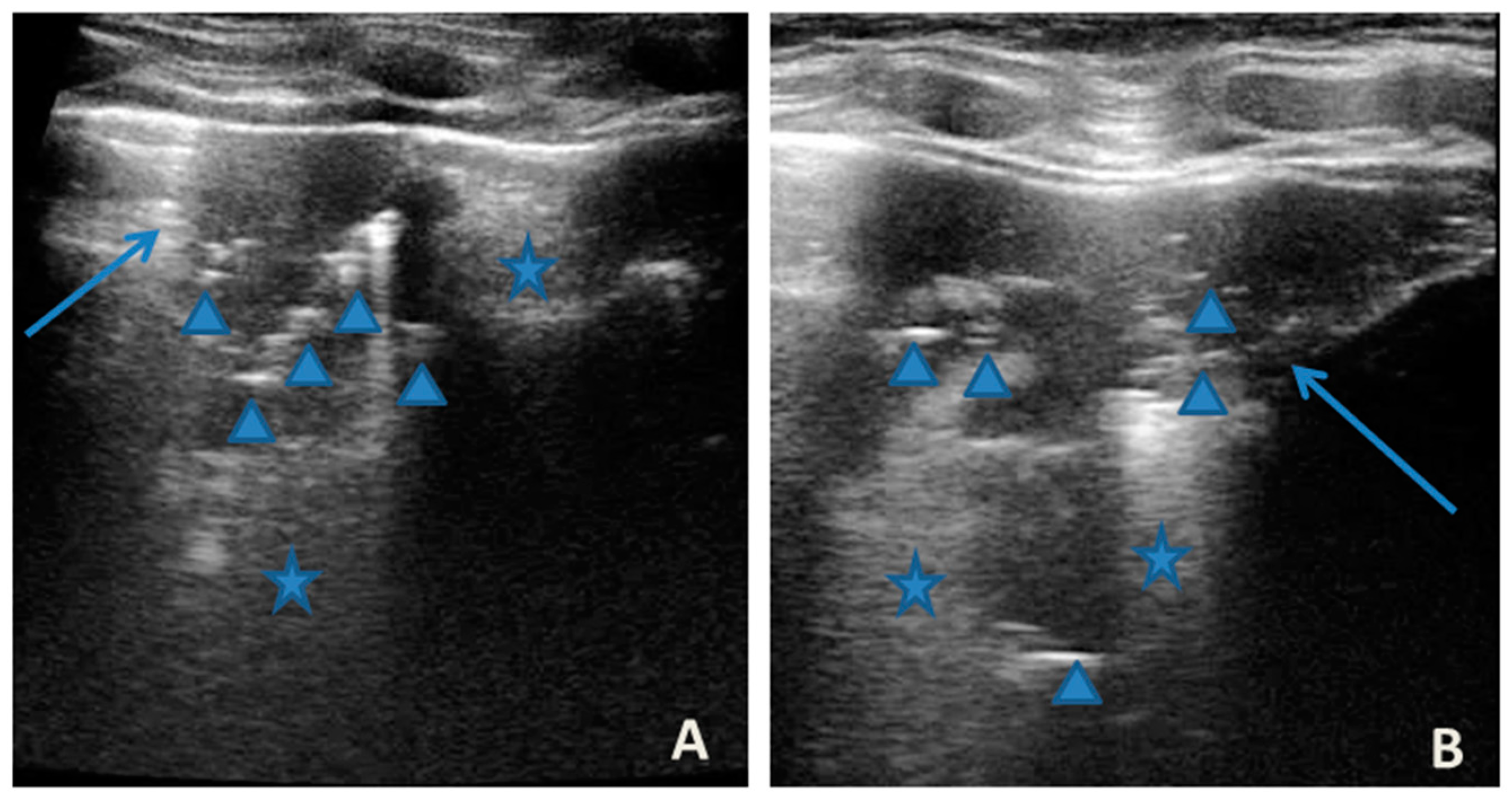
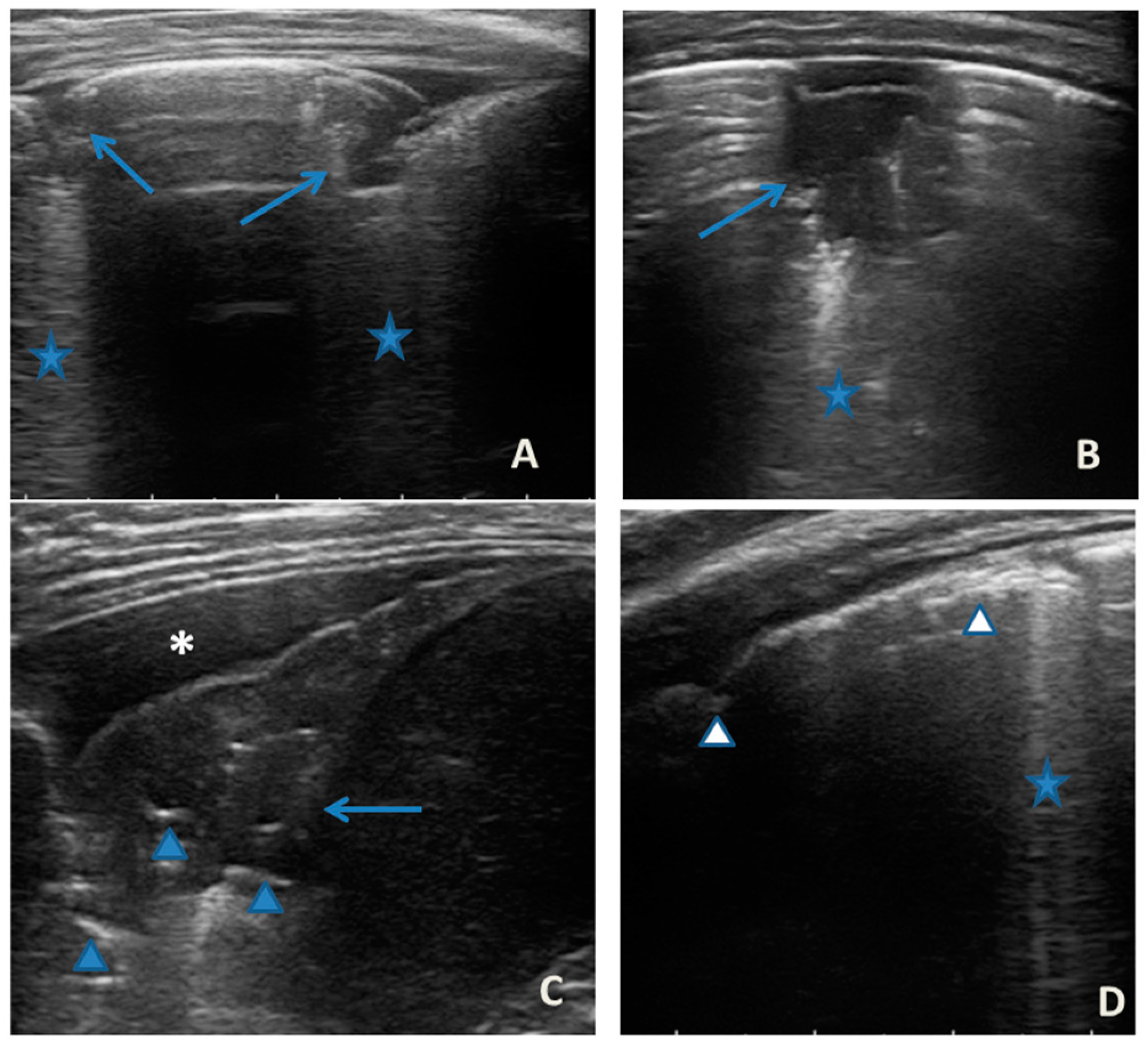
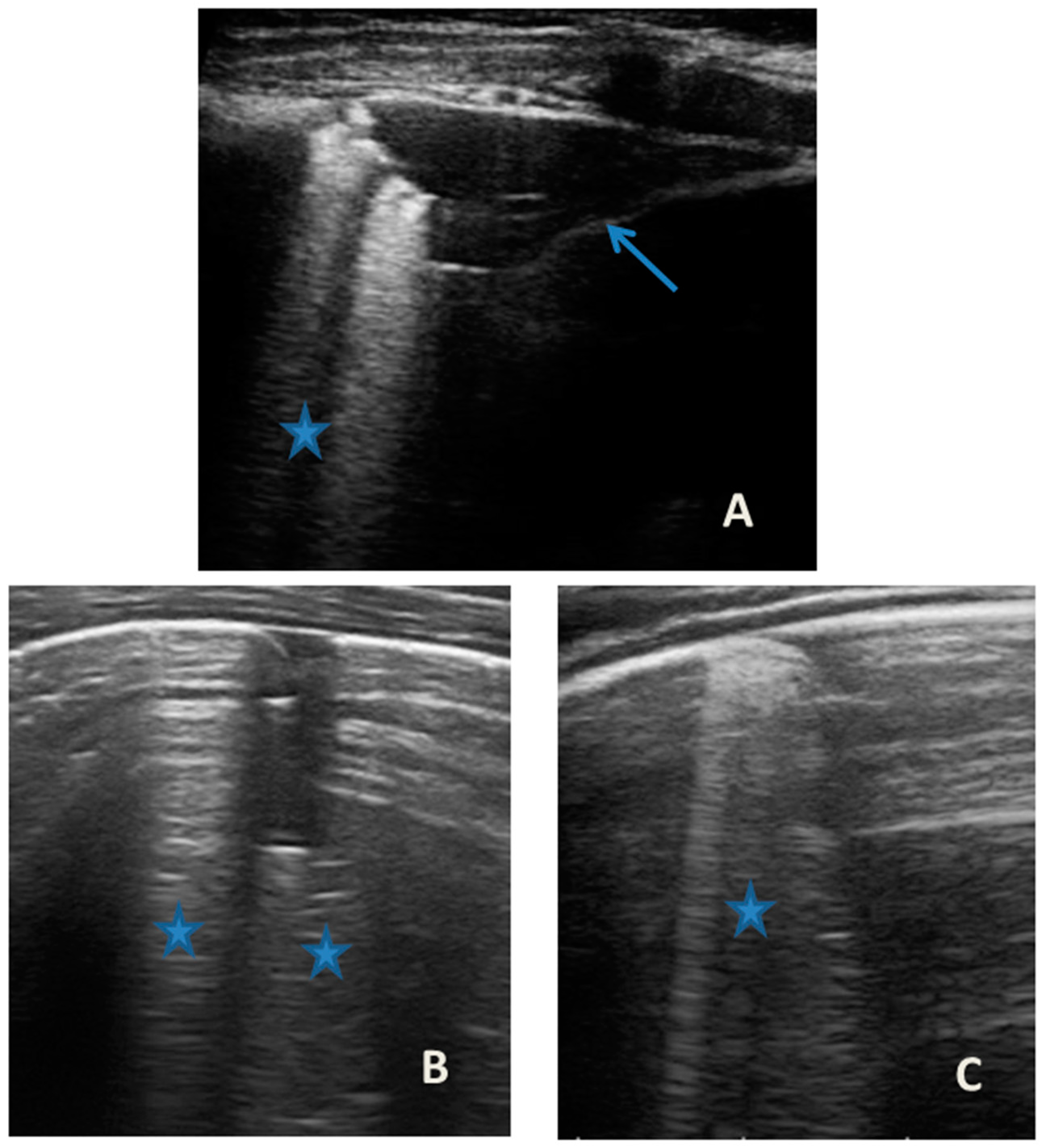
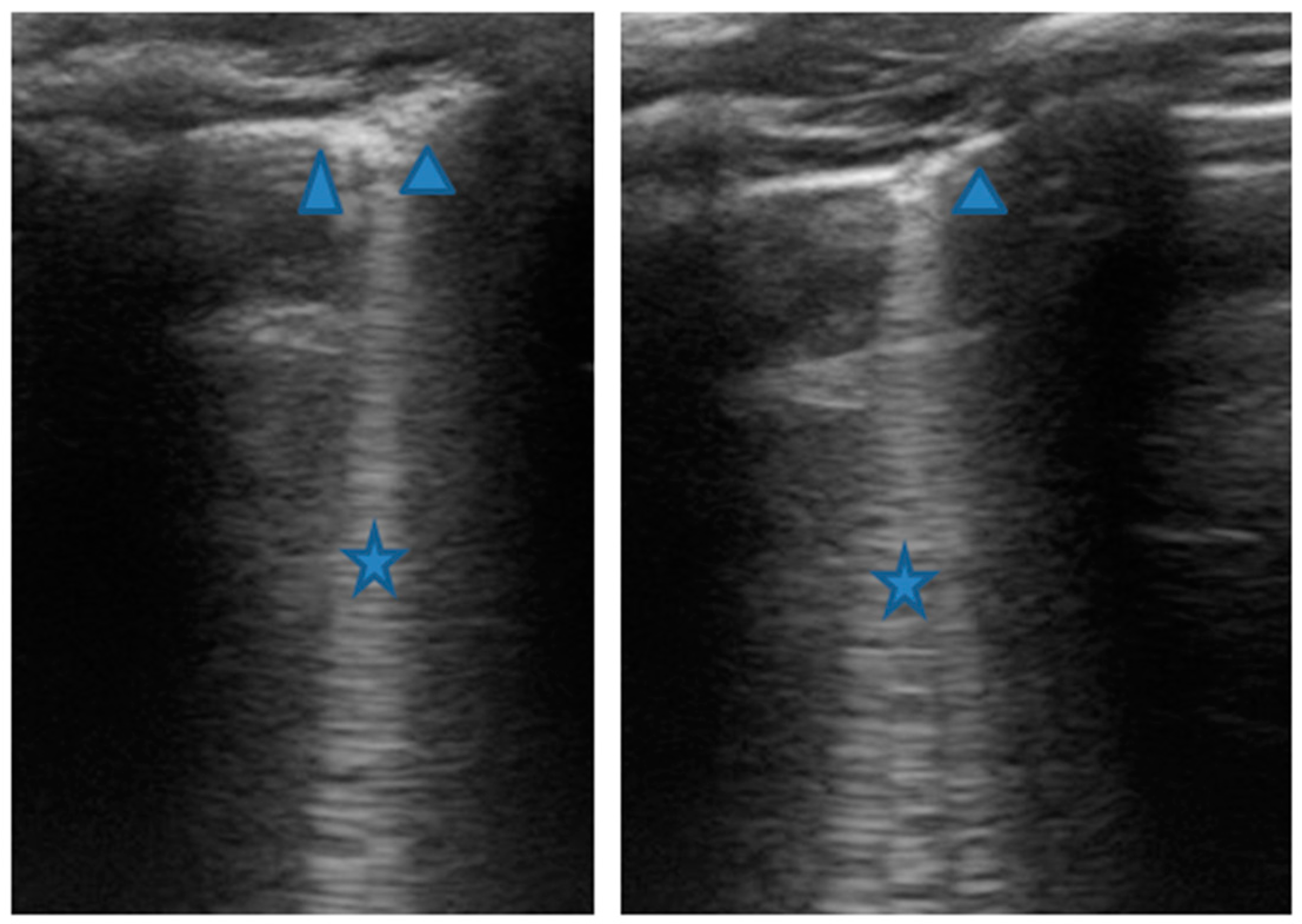
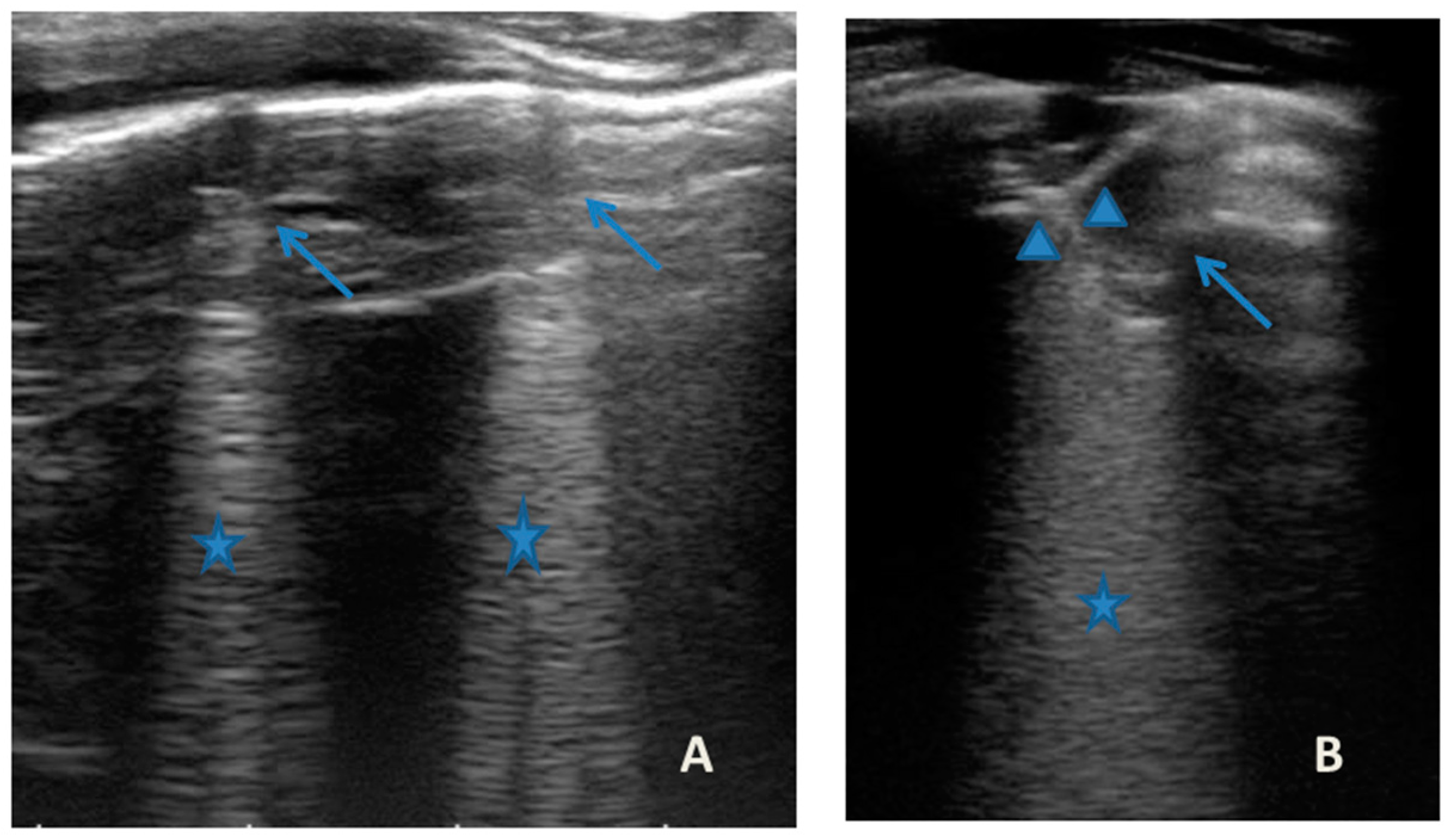
| LUS findings | Two areas of moderate lung atelectasis, associated with SIS (Figure 1) | Diffuse SIS, and three areas of lung atelectasis, one of which associated with mild reactive effusion (Figure 3) | Diffuse SIS and several areas of lung atelectasis, one of which involved the middle lobe (Figure 5) | Diffuse SIS (Figure 6) | Acute inflammation of the small airways: sub-centimeter consolidations with elements of dynamic air bronchogram, associated with confluent artifacts/“white lung” (Figure 7) | SIS picture (Figure 9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Rose, C.; Miceli Sopo, S.; Valentini, P.; Morello, R.; Biasucci, D.; Buonsenso, D. Potential Application of Lung Ultrasound in Children with Severe Uncontrolled Asthma: Preliminary Hypothesis Based on a Case Series. Medicines 2022, 9, 11. https://doi.org/10.3390/medicines9020011
De Rose C, Miceli Sopo S, Valentini P, Morello R, Biasucci D, Buonsenso D. Potential Application of Lung Ultrasound in Children with Severe Uncontrolled Asthma: Preliminary Hypothesis Based on a Case Series. Medicines. 2022; 9(2):11. https://doi.org/10.3390/medicines9020011
Chicago/Turabian StyleDe Rose, Cristina, Stefano Miceli Sopo, Piero Valentini, Rosa Morello, Daniele Biasucci, and Danilo Buonsenso. 2022. "Potential Application of Lung Ultrasound in Children with Severe Uncontrolled Asthma: Preliminary Hypothesis Based on a Case Series" Medicines 9, no. 2: 11. https://doi.org/10.3390/medicines9020011