1. Introduction
Targeting state of frailty is one of the priorities identified by the World Health Organization. As of 1 January 2021, more than one in five people (20.7%) in France were aged 65 or older. This percentage has been increasing for more than 30 years, and the aging of the population has accelerated since the mid-2010s—particularly with the aging of the first large generation born after WWII, the so-called “Baby Boomers.” The proportion of people aged 65 or over is increasing in every European Union (EU) country. In 2019, this group represented 20.0% of the EU population, compared to 17.4% in 2009 [
1]. While there might not currently be an agreed-upon definition of “frailty syndrome,” there is, however, a reference scale that can be used: the Fried scale [
2], taught in all universities and used daily in geriatric medicine departments. It is also called the “phenotypic fragility scale.” Developed in the 1990s by Professor Linda Fried’s (an American epidemiologist and geriatrician) teams, then adapted by the American Geriatric Society, it revolves around the concept of sarcopenia in phenotypic frailty [
2]. However, this scale is not well suited to ambulatory medicine due to spatial constraints (walking over 4.57 m), the time needed, and material requirements (use of a dynamometer). Since then, using the multidimensional approach developed by the Canadian teams (Rockwood et al.) [
3,
4,
5,
6], many scales have emerged [
7]—some of them remaining in an experimental stage. Their use in ambulatory medicine, in everyday practice, remains problematic. Some point to their time-consuming nature. Others believe these scales are difficult to adapt to general medicine practices, requiring specific equipment, such as a dynamometer or, moreover, medical consultation premises that allow walks of a given duration and distance to realize their full usefulness. As the elderly population grows in number and wants to stay at home as long as possible, it is essential to be able to detect a state of fragility in order to take all possible measures to reverse it. In addition, it should be noted that with the number of general practitioners decreasing, it is important to offer quick and clear scales, without any real training and at hand for the medical profession and also for other health professionals. It should be noted that geriatricians, at the international level by extension, have been unable to agree on a precise definition, which likely contributes to the multiplicity of current frailty scales. One of the grievances also mentioned is the lack of consultation with general practitioners (GPs) in the creation and implementation of frailty scales. A scale created in a hospital without consulting general practitioners can be difficult to accept because it does not necessarily integrate all the constraints primary care medical practices face. Therefore, it is essential to promote this partnership between general medicine and hospitals and generally between different medical specialties and geriatrics. This partnership is even more critical since the general practitioners are the doctors who will see most elderly subjects as outpatients in their clinics or on occasional home visits. It is in this context that we have proposed a new rapid screening scale for frailty (known as “ZULFIQAR”), designed to be used by general practitioners [
8]. We tested and validated it at other general medicine practices to see how easy it is to reproduce. We evaluated its performance and compared it with the reference frailty scale, the Fried scale, the GFST scale, and the SEGA scale, with very satisfactory results [
8]. Our frailty screening scale has been the subject of several published (or soon-to-be-published) studies since the original article appeared in the MEDICINES MDPI journal. The proof-of-concept study results were very satisfactory and reproducible, and similar results have been found in subsequent trials [
8,
9,
10].
The Clinical Frailty Scale is a clinical judgment-based frailty tool developed for the Canadian Study of Health and Aging, which originated from Dalhousie University in Canada [
3,
11]. Based on the biological and physiological criteria of frailty, this scale emphasizes functionality. The description of frailty levels is based on simple clinical observations, including comorbidities, functional status, and activity level. The rating is based on the judgment of the administrator [
7]. The objective of this preliminary task is to determine the performance of the “Zulfiqar Frailty Scale (ZFS)” tool to detect frailty (defined by the CFS) in this ambulatory population.
2. Patients and Methods
2.1. Methods
Prospective study was conducted at four general medicine practices in the Alsace region, specifically in Neuf Brisach, Saint-Louis, Rixheim, and Sarre-Union, for a total period of 9 months (from 17 May 2021 to 10 February 2022).
2.2. Primary Objective
The objective of the study was to validate the Zulfiqar Frailty Scale (ZFS) and to analyze its concordance with Clinical Frailty Scale (CFS) as established by Rockwood et al. and translated into French [
3,
12].
2.3. Inclusion Criteria
The patients needed to be 75 years of age or over, in consultation with a general practitioner, and with an ADL (Activity of Daily Living) greater than or equal to four.
2.4. Exclusion Criteria
Patients less than 65 years old and subjects with an ADL of less than four were excluded from this study. Those living in nursing homes were also excluded, as were patients unable to express themselves or give their consent.
2.5. Data Collected and Analyzed
Data for the study was recorded by the general practitioner during routine consultations. The Clinical Frailty Scale, as well as the Zulfiqar Frailty Scale, was screened for each patient. The information was then anonymized before being transmitted for collection in the study.
2.5.1. Frailty Screening with the “Zulfiqar Frailty Scale” (ZFS) Tool
The score has six items. A point was assigned for each positive indicator (maximum score = 6). See details about the ZFS tool in
Table 1.
2.5.2. Frailty Screening with the “Clinical Frailty Scale” (CFS)
We used the Clinical Frailty Scale (CFS) in our study, evolving from the Canadian Study of Health and Aging. It was developed as a grading tool with seven scales in 2005 [
3] and revised in 2008 to a 9-point scale [
13]: 1-Very Fit; 2-Well; 3-Managing Well; 4-Living With Very Mild Frailty; 5-Living with Mild Frailty; 6-Living With Moderate Frailty; 7-Living With Severe Frailty; 8-Living with Very Severe Frailty; 9-Terminally Ill. For scores of 5 or more, the elderly patient was considered by CFS to be “frail”.
2.6. Statistical Analysis
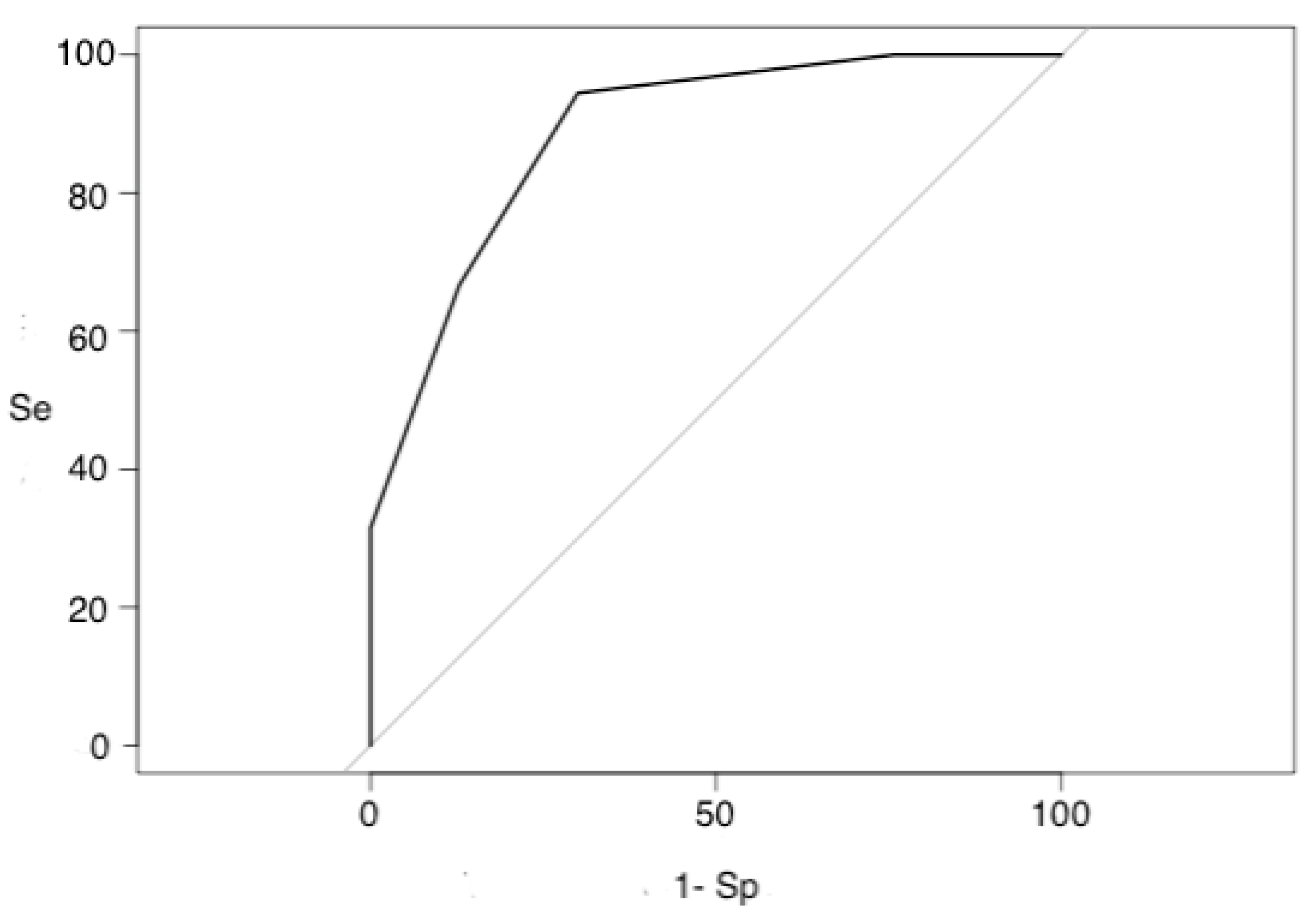
The data was analyzed by XL-Stat software (Addinsoft Inc., New York, NY., USA) and collected anonymously using an MS Excel spreadsheet. First, a descriptive analysis of the results obtained was prepared. Quantitative variables were expressed as mean ± standard deviation and qualitative variables as absolute and relative numbers (percentages). Next, the “ZFS” tool was compared to CFS using the student’s t-test for quantitative variables and Chi² for qualitative variables. It was used to measure the performance of a diagnostic test and to determine optimal threshold values. The relative risk of each item in the “ZFS” tool was estimated by calculating the Odds ratio, with a 95% confidence interval defined by the Miettinen method, resulting in a 5% alpha probability. The “ZFS” score was assessed in terms of sensitivity, specificity, Youden’s index, positive and negative predictive values, and the area under the ROC curve, using the CFS score as the gold standard. A Kappa coefficient and Spearman coefficient were calculated to measure the concordance between the two tests. A Pearson correlation matrix was used to evaluate discrepancies between the total scores and the items of each score.
2.7. Administrative Elements
The work conforms to the provisions of the Declaration of Helsinki (as revised in Tokyo 2004). The material contained in the manuscript has not been previously published and is not being concurrently submitted elsewhere. Informed consent was obtained from all patients included in this study. From a regulatory standpoint, the paper has received ethical approval and is registered with the Comité de Protection des Personnes, registration number: 2022-A01817-36.
4. Discussion
We developed a frailty screening tool that standardizes professional procedures and makes it possible for general practitioners to detect frailty in their elderly patients. The results of this study are very satisfactory and similar to previous studies [
8,
9,
10]: in fact, the correlations between the Zulfiqar scale (and the simplified scale) and other frailty scales are very satisfactory [
14,
15,
16,
17,
18]. In addition, the areas under the curve ranged from 0.70 to 0.94. These results show that the ZFS and sZFS are outstanding tools for detecting frailty. Our goal was to create a rapid frailty screening scale that would be useful for general practitioners. Our scale aims to facilitate the early detection of frail elderly people, which will help to delay the loss of their autonomy. Our tool does not require any equipment whatsoever, making it advantageous and perfectly suitable for primary care. The screening is quick and easy, allowing physicians to do away with other time-consuming methods that inconvenience elderly patients.
The CFS has been validated as an adverse outcome predictor in hospitalized older people [
19,
20,
21].
This frailty scale is used mainly in hospitals, for hospitalized patients [
21], particularly in emergency rooms and intensive care/resuscitation units [
21,
22]—and, especially during the COVID-19 pandemic [
23,
24,
25], it plays a supporting role in triage. It has also been used for hospitalized patients in cardiology [
26,
27], orthopedics [
28], geriatrics [
29,
30], and other units [
31]. Less has been published about its use in general medicine than its use in hospitals [
21]. It requires professional training to ensure the practitioner knows how to use it and understands geriatric syndromes. The practitioner must use their judgment. It is also important to note this scale, rated out of 9, goes beyond frailty syndrome: items 7, 8, and 9 are more characteristic of dependency than frailty syndrome. In addition, there is very little difference between items 5 and 6—which is why detailed training for medical and paramedical professionals is needed. Our scale can quickly test all the main frailty syndromes, covering nutrition, socialization, iatrogenic issues, memory, and falls. The questions are simple, based on information available to any health professional, with no prior training necessary. It can be used by general practitioners on a daily basis but can also be administered by nurses, physiotherapists, occupational therapists, or even social workers.
The ZFS scale has the advantage of being composed of six objective items, covering the geriatric syndrome as a whole through nutrition, socialization, memory, falls, and iatrogenics. The items are simple, with a binary answer (yes or no), based on information accessible to any health professional and requiring no prior training. It can be used by general practitioners, nurses, physiotherapists, occupational therapists, or social workers, and this is without any variability between examiners. The ZFS scale is a rapid screening scale for frailty syndrome dedicated to general medicine and ambulatory medicine/primary care. Many scales, both on the phenotypic and multidimensional levels, have emerged. However, due to a mismatch between some of these scales and ambulatory medicine (linked to the time-consuming nature, unsuitability to practices, and a certain level of knowledge to be acquired), these scales remain very little or not used in general medicine. In addition, most scales have been designed and developed in a hospital setting, which is the case with the Clinical Frailty Scale (CFS). In contrast, the ZFS scale has been designed by general medicine and applied only in outpatient medicine.
Our scale can be used in less than two minutes, concurring with our own data—which increases its usefulness in outpatient care. The general practitioner has all the patient’s information about iatrogenic issues, level of social activity, and nutrition. Each item in the questionnaire is scored a “1” if present, for a maximum total of “6”.
The tool is easy to use in a general medical consultation; therefore, it is appropriate for use in multidisciplinary nursing homes where a frailty diagnosis could be accompanied by specific follow-up measures, thanks to the variety of professionals present. Due to the lack of many “frailty day hospitals” and the shortage of geriatricians, the tool could be a significant add-on. The general practitioner can, of course, be the one to initiate the personalized care plan and play a central role in it. The doctor will coordinate care with paramedical and social stakeholders, reassess patient care, and guide family caregivers. In practice, 30–40% of seniors living at home suffer from frailty.
Given the ubiquity of this syndrome and the existence of medical deserts, screening for frailty relies on local paramedical professionals (nurses, physiotherapists, pharmacists, etc.). Therefore, we have also launched a dedicated website, accessible everywhere—in cities, suburban, and rural areas, for all medical professionals, and also for paramedical professionals, such as at-home nurses, physiotherapists, and occupational therapists:
http://zulfiqarfrailtyscale.com/ (accessed on 15 August 2022).
Our work is only limited by its monocentric character and the small sample size. A prospective study conducted across several sites with multiple practitioners would have made it possible to better understand the scope of administrator judgment needed regarding the CFS scale. The predictive nature of our scale, as it pertains to undesired events, such as hospitalizations or falls, has not been studied; however, this will be the subject of further research and investigation.


 ,
, 


{kind=link}
{kind=link}