
Improved Outcomes in Eosinophilic Esophagitis with Higher Medication Possession Ratio
 , ,
, ,
Abstract
:1. Introduction
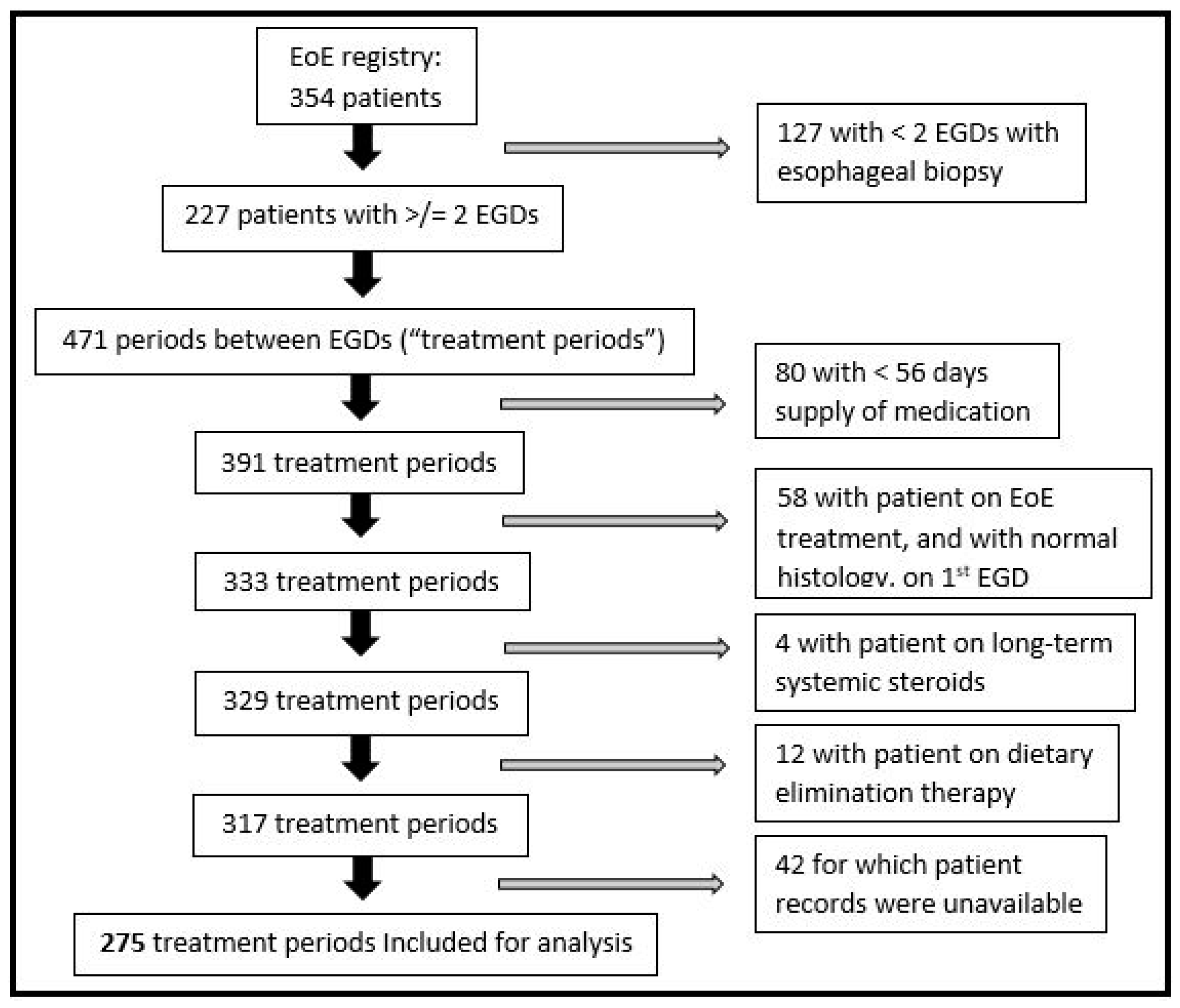
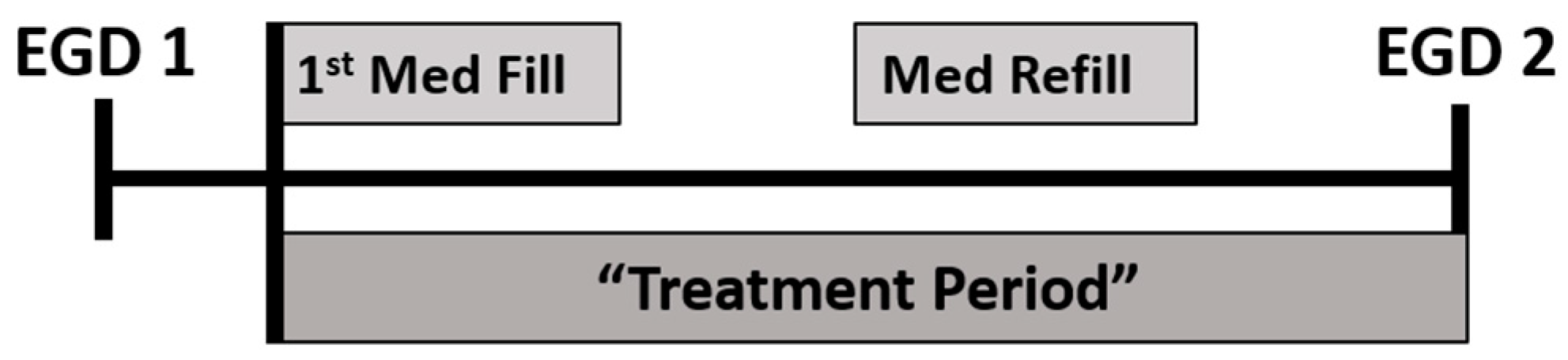
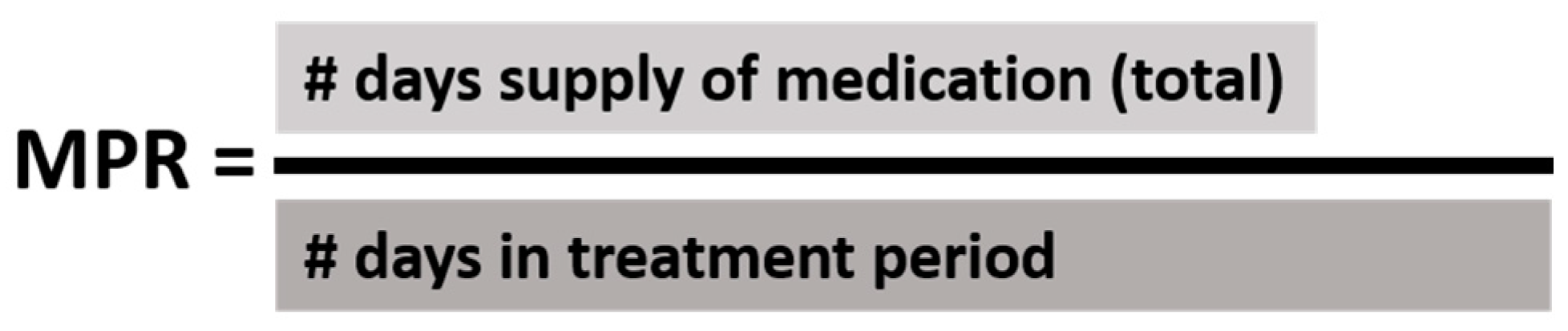
2. Materials and Methods
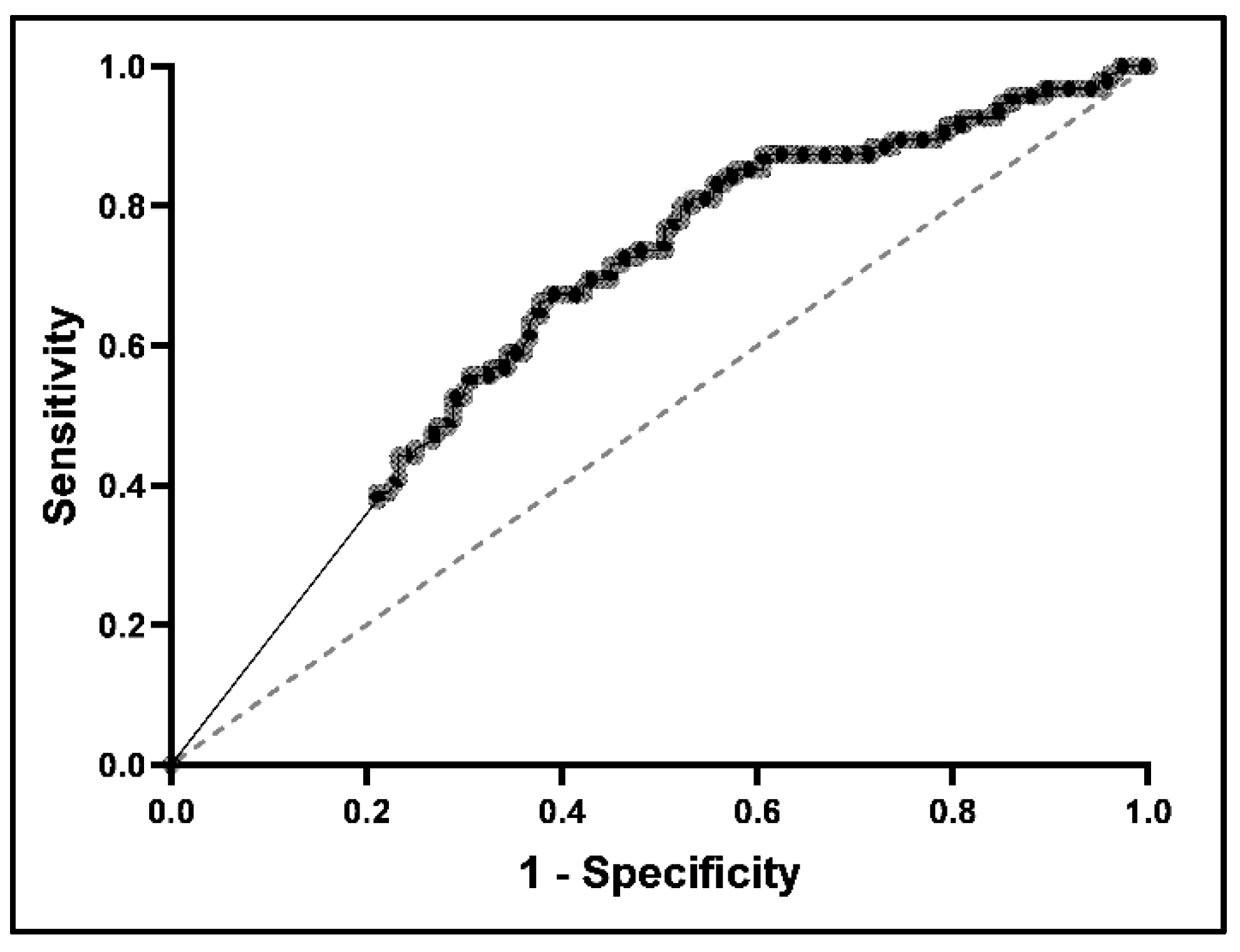
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Furuta, G.T.; Liacouras, C.A.; Collins, M.H.; Gupta, S.K.; Justinich, C.; Putnam, P.E.; Bonis, P.; Hassall, E.; Straumann, A.; Rothenberg, M.E.; et al. Eosinophilic esophagitis in children and adults: A systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology 2007, 133, 1342–1363. [Google Scholar] [CrossRef]
- Dellon, E.S.; Hirano, I. Epidemiology and Natural History of Eosinophilic Esophagitis. Gastroenterology 2018, 154, 319–332.e3. [Google Scholar] [CrossRef]
- Massironi, S.; Mulinacci, G.; Gallo, C.; Elvevi, A.; Danese, S.; Invernizzi, P.; Vespa, E. Mechanistic Insights into Eosinophilic Esophagitis: Therapies Targeting Pathophysiological Mechanisms. Cells 2023, 12, 2473. [Google Scholar] [CrossRef]
- Massironi, S.; Elvevi, A.; Panceri, R.; Mulinacci, G.; Colella, G.; Biondi, A.; Invernizzi, P.; Danese, S.; Vespa, E. Eosinophilic esophagitis: Does age matter? Expert. Rev. Clin. Immunol. 2024, 20, 211–223. [Google Scholar] [CrossRef]
- Liacouras, C.A.; Furuta, G.T.; Hirano, I.; Atkins, D.; Attwood, S.E.; Bonis, P.A.; Burks, A.W.; Chehade, M.; Collins, M.H.; Dellon, E.S.; et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J. Allergy Clin. Immunol. 2011, 128, 3–20.e6. [Google Scholar] [CrossRef]
- Muftah, M.; Bernstein, D.; Patel, A. Eosinophilic Esophagitis: Lessons Learned from Its Evolution. Dig. Dis. Sci. 2024, 69, 318–319. [Google Scholar] [CrossRef]
- Navarro, P.; Laserna-Mendieta, E.J.; Guagnozzi, D.; Casabona, S.; Perelló, A.; Savarino, E.; de la Riva, S.; Olalla, J.M.; Ghisa, M.; Serrano-Moya, N.; et al. Proton pump inhibitor therapy reverses endoscopic features of fibrosis in eosinophilic esophagitis. Dig. Liver Dis. 2021, 53, 1479–1485. [Google Scholar] [CrossRef]
- Dellon, E.S.; Rothenberg, M.E.; Collins, M.H.; Hirano, I.; Chehade, M.; Bredenoord, A.J.; Lucendo, A.J.; Spergel, J.M.; Aceves, S.; Sun, X.; et al. Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis. N. Engl. J. Med. 2022, 387, 2317–2330. [Google Scholar] [CrossRef]
- Bain, S. Press Release: FDA Approves Dupixent® (Dupilumab) as First Treatment for Adults and Children Aged 12 and Older with Eosinophilic Esophagitis. Sanofi, 2022. Available online: www.sanofi.com/en/media-room/press-releases/2022/2022-05-20-19-15-00-2447906 (accessed on 11 January 2024).
- Marasco, G.; Visaggi, P.; Vassallo, M.; Fiocca, M.; Cremon, C.; Barbaro, M.R.; De Bortoli, N.; Bellini, M.; Stanghellini, V.; Savarino, E.V.; et al. Current and Novel Therapies for Eosinophilic Gastrointestinal Diseases. Int. J. Mol. Sci. 2023, 24, 15165. [Google Scholar] [CrossRef]
- Eluri, S.; Iglesia, E.G.A.; Massaro, M.; Peery, A.F.; Shaheen, N.J.; Dellon, E.S. Practice patterns and adherence to clinical guidelines for diagnosis and management of eosinophilic esophagitis among gastroenterologists. Dis. Esophagus. 2020, 33, doaa025. [Google Scholar] [CrossRef]
- Mehta, P.; Pan, Z.; Zhou, W.; Kwan, B.M.; Furuta, G.T. Medication Adherence Rates in Adolescents with Eosinophilic Esophagitis Are Low and Are Associated with Health Habits. J. Pediatr. Gastroenterol. Nutr. 2023, 77, 532–535. [Google Scholar] [CrossRef]
- Philpott, H.; Dellon, E.S. The role of maintenance therapy in eosinophilic esophagitis: Who, why, and how? J. Gastroenterol. 2018, 53, 165–171. [Google Scholar] [CrossRef]
- Jevtić, J.; Ristić, N.; Pavlović, V.; Svorcan, J.; Milovanovich, I.; Radusinović, M.; Popovac, N.; Simić, L.; Ćirović, A.; Đuknić, M.; et al. The Usefulness of the Eosinophilic Esophagitis Histology Scoring System in Predicting Response to Proton Pump Inhibitor Monotherapy in Children with Eosinophilic Esophagitis. Diagnostics 2023, 13, 3445. [Google Scholar] [CrossRef]
- Greuter, T.; Safroneeva, E.; Bussmann, C.; Biedermann, L.; Vavricka, S.R.; Katzka, D.A.; Schoepfer, A.M.; Straumann, A. Maintenance Treatment of Eosinophilic Esophagitis with Swallowed Topical Steroids Alters Disease Course over A 5-Year Follow-up Period in Adult Patients. Clin. Gastroenterol. Hepatol. 2019, 17, 419–428.e6. [Google Scholar] [CrossRef]
- Dellon, E.S. No Maintenance, No Gain in Long-term Treatment of Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 2019, 17, 397–399. [Google Scholar] [CrossRef]
- Laserna-Mendieta, E.J.; Casabona, S.; Savarino, E.; Perelló, A.; Pérez-Martínez, I.; Guagnozzi, D.; Barrio, J.; Guardiola, A.; Asensio, T.; de la Riva, S.; et al. Efficacy of Therapy for Eosinophilic Esophagitis in Real-World Practice. Clin. Gastroenterol. Hepatol. 2020, 18, 2903–2911.e4. [Google Scholar] [CrossRef]
- Sperber, C.M.; Samarasinghe, S.R.; Lomax, G.P. An upper and lower bound of the Medication Possession Ratio. Patient Prefer. Adherence 2017, 11, 1469–1478. [Google Scholar] [CrossRef]
- Toh, H.S.; Yang, C.T.; Yang, K.L.; Ku, H.C.; Liao, C.T.; Kuo, S.; Tang, H.J.; Ko, W.C.; Ou, H.T.; Ko, N.Y. Reduced economic burden of AIDS-defining illnesses associated with adherence to antiretroviral therapy. Int. J. Infect. Dis. 2020, 91, 44–49. [Google Scholar] [CrossRef]
- Yu, S.F.; Cheng, J.S.; Chen, Y.C.; Chen, J.F.; Hsu, C.Y.; Lai, H.M.; Ko, C.H.; Chiu, W.C.; Su, Y.J.; Cheng, T.T. Adherence to anti-osteoporosis medication associated with lower mortality following hip fracture in older adults: A nationwide propensity score-matched cohort study. BMC Geriatr. 2019, 19, 290. [Google Scholar] [CrossRef]
- Bidwal, M.; Lor, K.; Yu, J.; Ip, E. Evaluation of asthma medication adherence rates and strategies to improve adherence in the underserved population at a Federally Qualified Health Center. Res. Social. Adm. Pharm. 2017, 13, 759–766. [Google Scholar] [CrossRef]
- Magny-Normilus, C.; Nolido, N.V.; Borges, J.C.; Brady, M.; Labonville, S.; Williams, D.; Soukup, J.; Lipsitz, S.; Hudson, M.; Schnipper, J.L. Effects of an Intensive Discharge Intervention on Medication Adherence, Glycemic Control, and Readmission Rates in Patients with Type 2 Diabetes. J. Patient Saf. 2021, 17, 73–80. [Google Scholar] [CrossRef]
- Kolasinski, N.T.; Pasman, E.A.; Nylund, C.M.; Reeves, P.T.; Brooks, D.I.; Lescouflair, K.G.; Min, S.B. Higher Medication Possession Ratio Correlates with Improved Outcomes in Eosinophilic Esophagitis. Gastroenterology 2021, 160, S-260. [Google Scholar] [CrossRef]
- Kolasinski, N.T.; Pasman, E.A.; Nylund, C.M.; Reeves, P.T.; Brooks, D.I.; Lescouflair, K.G.; Min, S.B. Higher Medication Possession Ratio Correlates with Improved Outcomes in Eosinophilic Esophagitis. Pediatrics 2022, 149, 969. [Google Scholar]
- Rank, M.A.; Sharaf, R.N.; Furuta, G.T.; Aceves, S.S.; Greenhawt, M.; Spergel, J.M.; Falck-Ytter, Y.T.; Dellon, E.S.; AGA Institute; Joint Task Force on Allergy-Immunology Practice Parameters collaborators; et al. Technical review on the management of eosinophilic esophagitis: A report from the AGA institute and the joint task force on allergy-immunology practice parameters. Ann. Allergy Asthma Immunol. 2020, 124, 424–440.e17. [Google Scholar] [CrossRef]
- SAS Institute. SAS/SHARE 9.4: User’s Guide, 2nd ed.; SAS Institute: Cary, NC, USA, 2019. [Google Scholar]
- GraphPad Software. Prism 9 User Guide; GraphPad Software: La Jolla, CA, USA, 2020. [Google Scholar]
- Jensen, E.T.; Kappelman, M.D.; Martin, C.F.; Dellon, E.S. Health-care utilization, costs, and the burden of disease related to eosinophilic esophagitis in the United States. Am. J. Gastroenterol. 2015, 110, 626–632. [Google Scholar] [CrossRef]
- Esophagogastroduodenoscopy, Flexible, Transoral; with Biopsy, Single or Multiple Code: 43239. Procedure Price Lookup for Outpatient Services, U.S. Centers for Medicare & Medicaid Services. Available online: www.medicare.gov/procedure-price-lookup/cost/43239/ (accessed on 14 May 2021).
- Ing, C.; DiMaggio, C.; Whitehouse, A.; Hegarty, M.K.; Brady, J.; von Ungern-Sternberg, B.S.; Davidson, A.; Wood, A.J.; Li, G.; Sun, L.S. Long-term differences in language and cognitive function after childhood exposure to anesthesia. Pediatrics 2012, 130, e476–e485. [Google Scholar] [CrossRef]
- Thakkar, K.; El-Serag, H.B.; Mattek, N.; Gilger, M.A. Complications of pediatric EGD: A 4-year experience in PEDS-CORI. Gastrointest Endosc. 2007, 65, 213–221. [Google Scholar] [CrossRef]
- FDA Drug Safety Communication: FDA Review Results in New Warnings about Using General Anesthetics and Sedation Drugs in Young Children and Pregnant Women. Center for Drug Evaluation and Research, U.S. Food and Drug Administration. Available online: www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-review-results-new-warnings-about-using-general-anesthetics-and (accessed on 11 January 2024).
- Rogal, S.S.; Powell, B.J.; Chinman, M.; Gastroenterology and Hepatology Implementation Research Group. Moving Toward Impact: An Introduction to Implementation Science for Gastroenterologists and Hepatologists. Gastroenterology 2020, 159, 2007–2012. [Google Scholar] [CrossRef]
- Vollmer, W.M.; Feldstein, A.; Smith, D.H.; Dubanoski, J.P.; Waterbury, A.; Schneider, J.L.; Clark, S.A.; Rand, C. Use of health information technology to improve medication adherence. Am. J. Manag. Care 2011, 17, SP79–SP87. [Google Scholar]
- Horvath, T.; Azman, H.; Kennedy, G.E.; Rutherford, G.W. Mobile phone text messaging for promoting adherence to antiretroviral therapy in patients with HIV infection. Cochrane Database Syst Rev. 2012, 2012, CD009756. [Google Scholar] [CrossRef]
- Pang, Y.; Molton, J.S.; Ooi, W.T.; Paton, N.I.; He, H.G. Preliminary Effects of a Mobile Interactive Supervised Therapy Intervention on People Living with HIV: Pilot Randomized Controlled Trial. JMIR Mhealth Uhealth 2020, 8, e15702. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.K.; Touchette, D.R.; Marris, J.C. Research and scholarly methods: Measuring medication adherence. J. Am. Coll. Clin. Pharm. 2023, 6, 416–426. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Histologic Remission † | Dysphagia | Impaction | Stricture | Dilation | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| YES | NO | p Value | NO | YES | p Value | NO | YES | p Value | NO | YES | p Value | NO | YES | p Value | |
| Any Treatment (n = 275) | 95 (35%) | 180 (65%) | 112 (41%) | 163 (59%) | 239 (87%) | 36 (13%) | 209 (76%) | 66 (24%) | 216 (79%) | 59 (22%) | |||||
| Medication Possession Ratio, median (IQR ‡) | 0.91 (0.63–1) | 0.63 (0.31–0.95) | <0.001 | 0.9 (0.65–1) | 0.59 (0.28–0.93) | <0.001 | 0.8 (0.49–1) | 0.29 (0.15–0.83) | <0.001 | 0.78 (0.46–1) | 0.59 (0.28–0.92) | 0.011 | 0.8 (0.5–1) | 0.46 (0.27–0.93) | <0.001 |
| Proton Pump Inhibitor (n = 188) | 65 (35%) | 123 (65%) | 69 (37%) | 119 (63%) | 162 (86%) | 26 (14%) | 137 (73%) | 51 (27%) | 143 (76%) | 45 (24%) | |||||
| Medication Possession Ratio, median (IQR ‡) | 0.88 (0.59–1) | 0.61 (0.31–0.92) | 0.001 | 0.85 (0.57–1) | 0.59 (0.28–0.92) | 0.001 | 0.76 (0.45–1) | 0.34 (0.17–0.74) | 0.001 | 0.72 (0.41–1) | 0.65 (0.31–0.93) | 0.196 | 0.74 (0.45–1) | 0.46 (0.28–0.94) | 0.044 |
| Topical Steroid (n = 40) | 12 (30%) | 28 (70%) | 19 (48.5%) | 21 (52.5%) | 36 (90%) | 4 (10%) | 33 (82.5%) | 7 (17.5%) | 34 (85%) | 6 (15%) | |||||
| Medication Possession Ratio, median (IQR ‡) | 0.98 (0.88–1) | 0.69 (0.44–0.98) | 0.02 | 0.95 (0.83–1) | 0.59 (0.27–0.92) | 0.005 | 0.85 (0.61–1) | 0.14 (0.08–0.59) | 0.071 | 0.91 (0.63–1) | 0.58 (0.24–0.86) | 0.065 | 0.89 (0.63–1) | 0.48 (0.27–0.59) | 0.052 |
| Combination Therapy (n = 47) | 18 (38%) | 29 (62%) | 24 (51%) | 23 (49%) | 41 (87%) | 6 (13%) | 39 (83%) | 8 (17%) | 39 (83%) | 8 (17%) | |||||
| Medication Possession Ratio, median (IQR ‡) | 0.88 (0.63–1) | 0.63 (0.21–1) | 0.08 | 0.88 (0.63–1) | 0.6 (0.26–0.94) | 0.09 | 0.83 (0.58–1) | 0.19 (0.16–1) | 0.156 | 0.87 (0.6–1) | 0.51 (0.13–0.76) | 0.076 | 0.9 (0.6–1) | 0.44 (0.14–0.56) | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolasinski, N.T.; Pasman, E.A.; Nylund, C.M.; Reeves, P.T.; Brooks, D.I.; Lescouflair, K.G.; Min, S.B. Improved Outcomes in Eosinophilic Esophagitis with Higher Medication Possession Ratio. Medicines 2024, 11, 8. https://doi.org/10.3390/medicines11040008
Kolasinski NT, Pasman EA, Nylund CM, Reeves PT, Brooks DI, Lescouflair KG, Min SB. Improved Outcomes in Eosinophilic Esophagitis with Higher Medication Possession Ratio. Medicines. 2024; 11(4):8. https://doi.org/10.3390/medicines11040008
Chicago/Turabian StyleKolasinski, Nathan T., Eric A. Pasman, Cade M. Nylund, Patrick T. Reeves, Daniel I. Brooks, Katerina G. Lescouflair, and Steve B. Min. 2024. "Improved Outcomes in Eosinophilic Esophagitis with Higher Medication Possession Ratio" Medicines 11, no. 4: 8. https://doi.org/10.3390/medicines11040008