
Antiseizure Medication-Induced Alopecia: A Literature Review

 , ,
, ,
Abstract
:1. Introduction
2. Methods
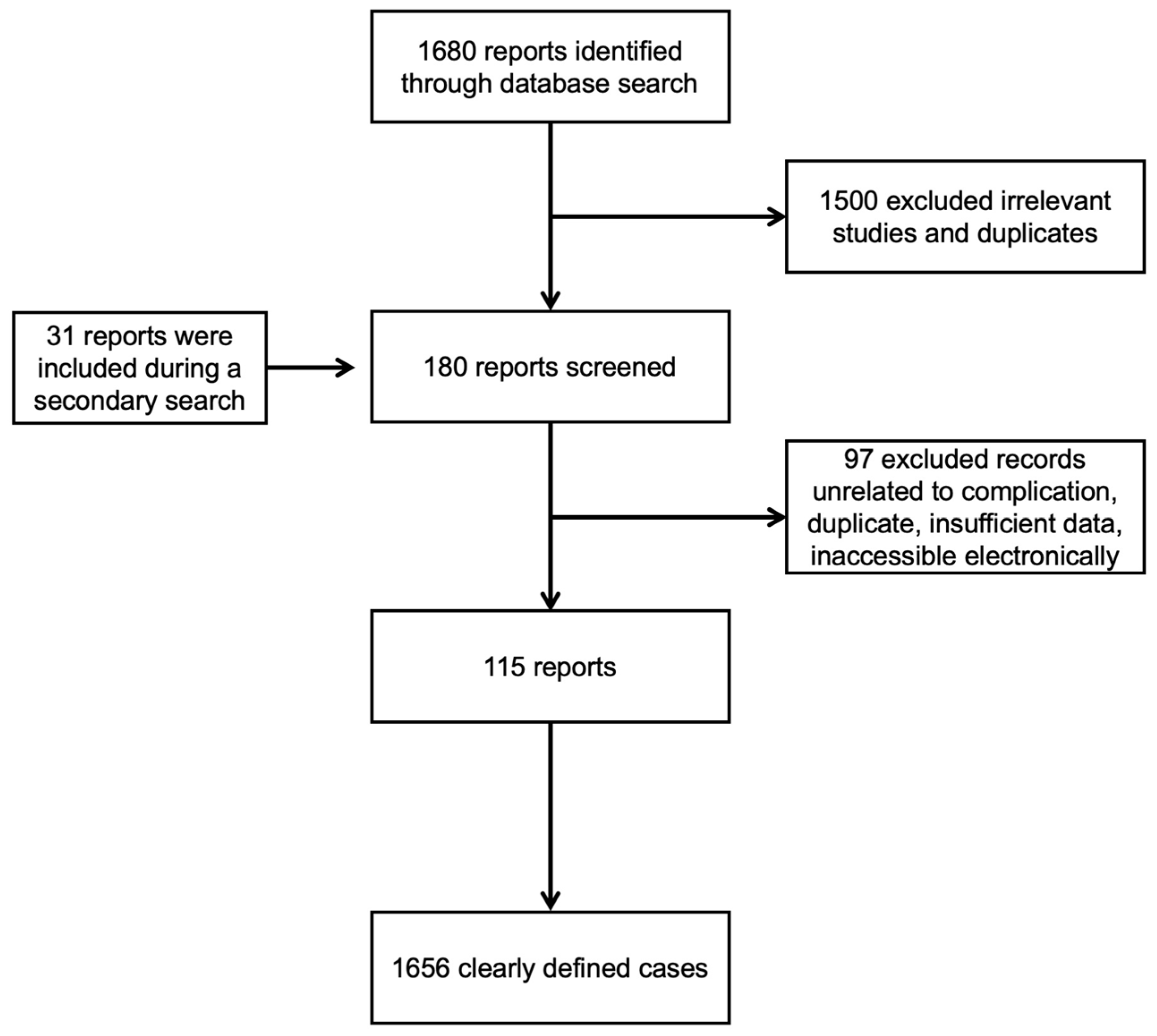
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Antiseizure Medications
3.1. Valproate (VPA)
3.2. Carbamazepine (CBZ)
3.3. Lamotrigine (LTG)
3.4. Levetiracetam (LEV)
3.5. Gabapentin (GBP)
3.6. Topiramate (TPM)
3.7. Phenytoin (PHT)
3.8. Pregabalin (PGB)
3.9. Perampanel (PMP)
3.10. Phenobarbital, Vigabatrin, Tiagabine, and Trimethadione
4. Discussion
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Getnet, A.; Woldeyohannes, S.M.; Bekana, L.; Mekonen, T.; Fekadu, W.; Menberu, M.; Yimer, S.; Assaye, A.; Belete, A.; Belete, H. Antiepileptic Drug Nonadherence and Its Predictors among People with Epilepsy. Behav. Neurol. 2016, 2016, 3189108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buck, D.; Jacoby, A.; Baker, G.A.; Chadwick, D.W. Factors influencing compliance with antiepileptic drug regimes. Seizure 1997, 6, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Kanner, A.M. To comply with AED therapy… what patients are not told! Epilepsy Curr. 2009, 9, 139–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Choi, H.; Hirsch, L.J.; Moeller, J.; Javed, A.; Kato, K.; Legge, A.; Buchsbaum, R.; Detyniecki, K. Cosmetic side effects of antiepileptic drugs in adults with epilepsy. Epilepsy Behav. 2015, 42, 129–137. [Google Scholar] [CrossRef]
- Perucca, P.; Gilliam, F.G. Adverse effects of antiepileptic drugs. Lancet Neurol. 2012, 11, 792–802. [Google Scholar] [CrossRef]
- Kinderen, R.J.; Evers, S.M.; Rinkens, R.; Postulart, D.; Vader, C.I.; Majoie, M.H.; Aldenkamp, A.P. Side-effects of antiepileptic drugs: The economic burden. Seizure 2014, 23, 184–190. [Google Scholar] [CrossRef] [Green Version]
- Stroud, J.D. Diagnosis and management of the hair loss patient. Cutis 1987, 40, 272–276. [Google Scholar]
- Mercke, Y.; Sheng, H.; Khan, T.; Lippmann, S. Hair loss in psychopharmacology. Ann. Clin. Psychiatry 2000, 12, 35–42. [Google Scholar] [CrossRef]
- Botega, A.R.; Amorim, C.V.; Teixeira, F.; Mello, C.D.; Stelini, R.F.; Velho, P.N.; Cintra, M.L. Scarring versus Non-Scarring Alopecia: An Interobserver Histopathological Reproducibility Study. Ski. Appendage Disord. 2023, 9, 34–41. [Google Scholar] [CrossRef]
- Llau, M.E.; Viraben, R.; Montastruc, J.L. Drug-induced alopecia: Review of the literature. Therapie 1995, 50, 145–150. [Google Scholar]
- Lemieux, J.; Maunsell, E.; Provencher, L. Chemotherapy-induced alopecia and effects on quality of life among women with breast cancer: A literature review. Psychooncology 2008, 17, 317–328. [Google Scholar] [CrossRef]
- Can, G.; Demir, M.; Erol, O.; Aydiner, A. A comparison of men and women’s experiences of chemotherapy-induced alopecia. Eur. J. Oncol. Nurs. 2013, 17, 255–260. [Google Scholar] [CrossRef]
- Paus, R.; Cotsarelis, G. The biology of hair follicles. N. Engl. J. Med. 1999, 341, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Lindner, G.; Botchkarev, V.A.; Botchkareva, N.V.; Ling, G.; Veen, C.; Paus, R. Analysis of apoptosis during hair follicle regression (catagen). Am. J. Pathol. 1997, 151, 1601–1617. [Google Scholar]
- Lousada, M.B.; Lachnit, T.; Edelkamp, J.; Rouillé, T.; Ajdic, D.; Uchida, Y.; Nardo, A.; Bosch, T.C.; Paus, R. Exploring the human hair follicle microbiome. Br. J. Dermatol. 2021, 184, 802–815. [Google Scholar] [CrossRef]
- Natarelli, N.; Gahoonia, N.; Sivamani, R.K. Integrative and Mechanistic Approach to the Hair Growth Cycle and Hair Loss. J. Clin. Med. 2023, 12, 893. [Google Scholar] [CrossRef]
- Popa, A.; Carsote, M.; Cretoiu, D.; Dumitrascu, M.C.; Nistor, C.E.; Sandru, F. Study of the Thyroid Profile of Patients with Alopecia. J. Clin. Med. 2023, 12, 1115. [Google Scholar] [CrossRef]
- Courtois, M.; Loussouarn, G.; Hourseau, C.; Grollier, J.F. Ageing and hair cycles. Br. J. Dermatol. 1995, 132, 86–93. [Google Scholar] [CrossRef]
- Bemt, P.M.; Brodie-Meijer, C.C.; Krijnen, R.M.; Nieboer, C. Drug induced alopecia. Ned. Tijdschr. Geneeskd. 1999, 143, 990–994. [Google Scholar]
- Murad, A.; Maguire, J.; Bergfeld, W. Drug-induced alopecia areata? Clin. Exp. Dermatol. 2021, 46, 363–366. [Google Scholar] [CrossRef]
- Starace, M.; Orlando, G.; Bruni, F.; Alessandrini, A.; Piraccini, B.M. Anagen effluvium and the role of trichoscopy. Clin. Exp. Dermatol. 2022, 47, 589–591. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Caro, G.; Fortuna, M.C.; Pigliacelli, F.; D’Arino, A.; Carlesimo, M. Prevention and Treatment of Chemotherapy-Induced Alopecia. Dermatol. Pract. Concept. 2020, 10, e2020074. [Google Scholar] [CrossRef] [PubMed]
- Moattari, C.R.; Jafferany, M. Psychological Aspects of Hair Disorders: Consideration for Dermatologists, Cosmetologists, Aesthetic, and Plastic Surgeons. Ski. Appendage Disord. 2022, 8, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Tosti, A.; Misciali, C.; Piraccini, B.M.; Peluso, A.M.; Bardazzi, F. Drug-induced hair loss and hair growth. Incidence, management and avoidance. Drug Saf. 1994, 10, 310–317. [Google Scholar] [CrossRef]
- Trüeb, R.M. Chemotherapy-induced hair loss. Ski. Ther. Lett. 2010, 15, 5–7. [Google Scholar]
- Malkud, S. Telogen Effluvium: A Review. J. Clin. Diagn. Res. 2015, 9, 1–3. [Google Scholar] [CrossRef]
- Sinclair, R. Diffuse hair loss. Int. J. Dermatol. 1999, 38, 8–18. [Google Scholar] [CrossRef]
- McKinney, P.A.; Finkenbine, R.D.; DeVane, C.L. Alopecia and mood stabilizer therapy. Ann. Clin. Psychiatry 1996, 8, 183–185. [Google Scholar] [CrossRef]
- Johannessen, C.U. Mechanisms of action of valproate: A commentatory. Neurochem. Int. 2000, 37, 103–110. [Google Scholar] [CrossRef]
- Rissardo, J.P.; Caprara, A.L.; Durante, Í. Valproate-associated Movement Disorder: A Literature Review. Prague Med. Rep. 2021, 122, 140–180. [Google Scholar] [CrossRef]
- Schmidt, D. Adverse effects of valproate. Epilepsia 1984, 25, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Völzke, E.; Doose, H. Dipropylacetate (Dépakine, Ergenyl) in the treatment of epilepsy. Epilepsia 1973, 14, 185–193. [Google Scholar] [CrossRef]
- Pillans, P.I.; Woods, D.J. Drug-associated alopecia. Int. J. Dermatol. 1995, 34, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, A.; Sackellares, J.C.; Shu, V. Safety and efficacy of divalproex sodium monotherapy in partial epilepsy: A double-blind, concentration-response design clinical trial. Depakote Monotherapy for Partial Seizures Study Group. Neurology 1997, 48, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, H.; Xu, D.; Zhu, L.; Liu, L. Risk of valproic acid-related alopecia: A systematic review and meta-analysis. Seizure 2019, 69, 61–69. [Google Scholar] [CrossRef]
- Praharaj, S.K.; Munoli, R.N.; Udupa, S.T.; Vaidyanathan, S. Valproate-associated hair abnormalities: Pathophysiology and management strategies. Hum. Psychopharmacol. 2022, 37, e2814. [Google Scholar] [CrossRef]
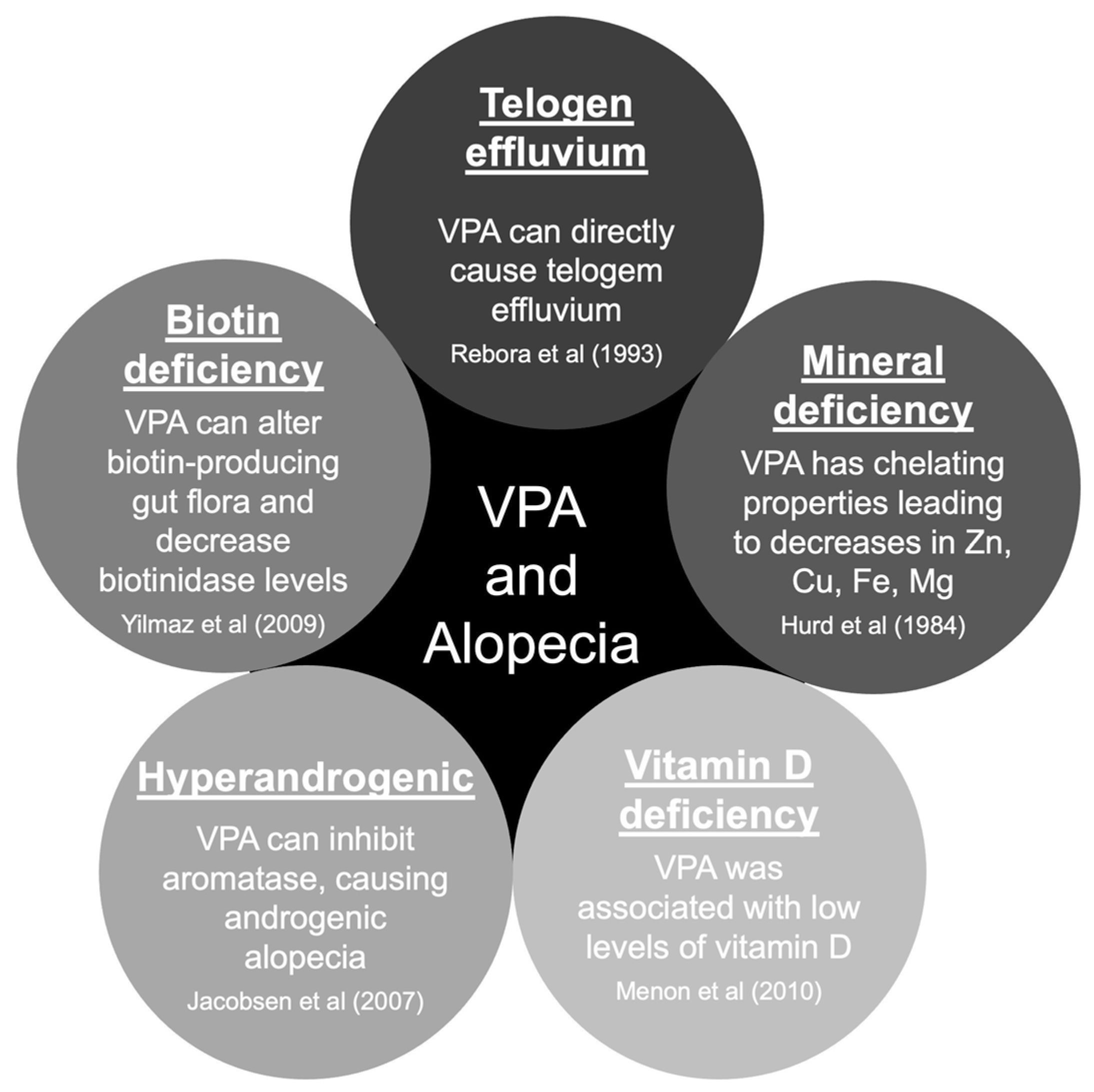
- Rebora, A. Telogen effluvium: An etiopathogenetic theory. Int. J. Dermatol. 1993, 32, 339–340. [Google Scholar] [CrossRef]
- Yilmaz, Y.; Tasdemir, H.A.; Paksu, M.S. The influence of valproic acid treatment on hair and serum zinc levels and serum biotinidase activity. Eur. J. Paediatr. Neurol. 2009, 13, 439–443. [Google Scholar] [CrossRef]
- Hurd, R.W.; Rinsvelt, H.A.; Wilder, B.J.; Karas, B.; Maenhaut, W.; Reu, L. Selenium, zinc, and copper changes with valproic acid: Possible relation to drug side effects. Neurology 1984, 34, 1393–1395. [Google Scholar] [CrossRef]
- Jacobsen, N.W.; Halling-Sorensen, B.; Birkved, F.K. Inhibition of human aromatase complex (CYP19) by antiepileptic drugs. Toxicol. In Vitro 2008, 22, 146–153. [Google Scholar] [CrossRef]
- Menon, B.; Harinarayan, C.V. The effect of anti epileptic drug therapy on serum 25-hydroxyvitamin D and parameters of calcium and bone metabolism--a longitudinal study. Seizure 2010, 19, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Uehlinger, C.; Barrelet, L.; Touabi, M.; Baumann, P. Alopecia and mood stabilizers: Two case reports. Eur. Arch. Psychiatry Clin. Neurosci. 1992, 242, 85–88. [Google Scholar] [CrossRef]
- Henriksen, O.; Johannessen, S.I. Clinical and pharmacokinetic observations on sodium valproate—A 5-year follow-up study in 100 children with epilepsy. Acta Neurol. Scand. 1982, 65, 504–523. [Google Scholar] [CrossRef]
- Fatemi, S.H.; Calabrese, J.R. Treatment of valproate-induced alopecia. Ann. Pharmacother. 1995, 29, 1302. [Google Scholar] [CrossRef]
- Trost, L.B.; Bergfeld, W.F.; Calogeras, E. The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. J. Am. Acad. Dermatol. 2006, 54, 824–844. [Google Scholar] [CrossRef]
- Castro-Gago, M.; Gómez-Lado, C.; Eirís-Puñal, J.; Díaz-Mayo, I.; Castiñeiras-Ramos, D.E. Serum biotinidase activity in children treated with valproic acid and carbamazepine. J. Child. Neurol. 2010, 25, 32–35. [Google Scholar] [CrossRef]
- Sahin, E.K.; Can, S.S.; Caykoylu, A.; Atagun, M.I. Agomelatine may alleviate valproate induced hair loss. J. Psych. Neurol. Sci. 2017, 30, 269–270. [Google Scholar]
- Thomson, S.R.; Mamulpet, V.; Adiga, S. Sodium Valproate Induced Alopecia: A Case Series. J. Clin. Diagn. Res. 2017, 11, 1–2. [Google Scholar] [CrossRef]
- Kakunje, A.; Prabhu, A.; Priya, E.S.; Karkal, R.; Kumar, P.; Gupta, N.; Rahyanath, P.K. Valproate: It’s Effects on Hair. Int. J. Trichol. 2018, 10, 150–153. [Google Scholar] [CrossRef]
- Pellock, J.M. Carbamazepine side effects in children and adults. Epilepsia 1987, 28, 64–70. [Google Scholar] [CrossRef]
- Shuper, A.; Stahl, B.; Weitz, R. Carbamazepine-induced hair loss. Drug Intell. Clin. Pharm. 1985, 19, 924–925. [Google Scholar] [CrossRef] [PubMed]
- Mattson, R.H.; Cramer, J.A.; Collins, J.F. A comparison of valproate with carbamazepine for the treatment of complex partial seizures and secondarily generalized tonic-clonic seizures in adults. N. Engl. J. Med. 1992, 327, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, A.; Shibasaki, H.; Shiozaki, A.; Kimura, J. Alopecia with carbamazepine in two patients with focal seizures. J. Neurol. Neurosurg. Psychiatry 1997, 63, 549–550. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Kim, D.S.; Kwon, Y.S.; Lee, J.H.; Lee, K.H. Concurrence of palmoplantar psoriasiform eruptions and hair loss during carbamazepine treatment. Acta Derm. Venereol. 2008, 88, 532–533. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, M.M. Overview of drugs used for epilepsy and seizures: Etiology, diagnosis, and treatment. Pharm. Ther. 2010, 35, 392–415. [Google Scholar]
- Rybakowski, J.K. Mood Stabilizers of First and Second Generation. Brain Sci. 2023, 13, 741. [Google Scholar] [CrossRef]
- Shirazi, Z.; Inaloo, S. Intravenous immunoglobulin in the treatment of lamotrigine- induced toxic epidermal necrolysis. Iran. J. Allergy Asthma Immunol. 2008, 7, 239–241. [Google Scholar]
- Patrizi, A.; Savoia, F.; Negosanti, F.; Posar, A.; Santucci, M.; Neri, I. Telogen effluvium caused by magnesium valproate and lamotrigine. Acta Derm. Venereol. 2005, 85, 77–78. [Google Scholar] [CrossRef] [Green Version]
- Hillemacher, T.; Bleich, S.; Kornhuber, J.; Frieling, H. Hair loss as a side effect of lamotrigine treatment. Am. J. Psychiatry 2006, 163, 1451. [Google Scholar] [CrossRef]
- Solmi, M.; Tamiello, G.I.; Manuli, G. Lamotrigine Induces Hair Loss in a Patient with Treatment-Resistant Major Depressive Disorder. Am. J. Ther. 2017, 24, 611–612. [Google Scholar] [CrossRef]
- Tengstrand, M.; Star, K.; Puijenbroek, E.P.; Hill, R. Alopecia in association with lamotrigine use: An analysis of individual case safety reports in a global database. Drug Saf. 2010, 33, 653–658. [Google Scholar] [CrossRef]
- Stephen, L.J.; Kelly, K.; Parker, P.; Brodie, M.J. Levetiracetam monotherapy--outcomes from an epilepsy clinic. Seizure 2011, 20, 554–557. [Google Scholar] [CrossRef] [Green Version]
- Hovinga, C.A. Levetiracetam: A novel antiepileptic drug. Pharmacotherapy 2001, 21, 1375–1388. [Google Scholar] [CrossRef]
- Neyens, L.G.; Alpherts, W.C.; Aldenkamp, A.P. Cognitive effects of a new pyrrolidine derivative (levetiracetam) in patients with epilepsy. Prog. Neuropsychopharmacol. Biol. Psychiatry 1995, 19, 411–419. [Google Scholar] [CrossRef]
- Zou, X.; Hong, Z.; Zhou, D. Hair loss with levetiracetam in five patients with epilepsy. Seizure 2014, 23, 158–160. [Google Scholar] [CrossRef] [Green Version]
- Aghamollaii, V.; Khan, Z.G.; Maneshi, A.; Ghaeli, P. Role of Zinc Supplementation in the Treatment of Levetiracetam-Induced Hair Loss: A Case Series. J. Pharm. Care. 2017, 4, 44–45. [Google Scholar]
- Goa, K.L.; Sorkin, E.M. Gabapentin. A review of its pharmacological properties and clinical potential in epilepsy. Drugs 1993, 46, 409–427. [Google Scholar] [CrossRef]
- Rose, M.A.; Kam, P.C. Gabapentin: Pharmacology and its use in pain management. Anaesthesia 2002, 57, 451–462. [Google Scholar] [CrossRef]
- Eker, H.E.; Cok, O.Y.; Aribogan, A. Alopecia associated with gabapentin in the treatment of neuropathic pain. J. Pain Symptom Manag. 2009, 37, 5–6. [Google Scholar] [CrossRef]
- Picard, C.; Jonville-Bera, A.P.; Billard, C.; Autret, E. Alopecia associated with gabapentin: First case. Ann. Pharmacother. 1997, 31, 1260. [Google Scholar] [CrossRef]
- Chuang, Y.C.; Chang, W.N.; Chen, I.L.; Yang, J.Y.; Ho, J.C.; Kuo, H.W. Topiramate-induced hair loss: Case report. Dermatol. Psychosom. 2002, 3, 183–184. [Google Scholar] [CrossRef]
- Ghafoor, I.; Hosseini, H. Hair Loss Following The Topiramate Treatment. J. Babol. Univ. Med. Sci. 2017, 19, 71–74. [Google Scholar]
- Lagrand, T.J.; Lehn, A.C. Tremor Drugs in the Crosshairs. Tremor Other Hyperkinetic Mov. 2021, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Herranz, J.L.; Armijo, J.A.; Arteaga, R. Clinical side effects of phenobarbital, primidone, phenytoin, carbamazepine, and valproate during monotherapy in children. Epilepsia 1988, 29, 794–804. [Google Scholar] [CrossRef]
- Wallace, S.J. A comparative review of the adverse effects of anticonvulsants in children with epilepsy. Drug Saf. 1996, 15, 378–393. [Google Scholar] [CrossRef]
- Kuhne, A.C.; Pitta, A.C.; Galassi, S.C.; Gonçalves, A.M.; Cardoso, A.C.; Paz, J.A.; Campos, L.M.; Silva, C.A. Munchausen by proxy syndrome mimicking childhood-onset systemic lupus erythematosus. Lupus 2019, 28, 249–252. [Google Scholar] [CrossRef]
- Mangalvedhekar, S.S.; Gogtay, N.J.; Manjula, S.; Kadam, V.S.; Dalvi, S.S.; Shah, P.U.; Badakere, S.S.; Pradhan, V.D.; Kshirsagar, N.A. Phenytoin associated alopecia: Drug induced lupus. J. Assoc. Physicians India 2001, 49, 929–930. [Google Scholar]
- Neki, N.S.; Shah, D.M. Phenytoin induced alopecia & Lupus: A case report. RGUHS J. Med. Sci. 2015, 5, 188–189. [Google Scholar]
- Onaolapo, A.Y.; Adebayo, A.A.; Onaolapo, O.J. Oral phenytoin protects against experimental cyclophosphamide-chemotherapy induced hair loss. Pathophysiology 2018, 25, 31–39. [Google Scholar] [CrossRef]
- Harmark, L.; Puijenbroek, E.; Straus, S.; Grootheest, K. Intensive monitoring of pregabalin: Results from an observational, Web-based, prospective cohort study in the Netherlands using patients as a source of information. Drug Saf. 2011, 34, 221–231. [Google Scholar] [CrossRef]
- Morse, D.C.; Henck, J.W.; Bailey, S.A. Developmental Toxicity Studies with Pregabalin in Rats: Significance of Alterations in Skull Bone Morphology. Birth Defects Res. B Dev. Reprod. Toxicol. 2016, 107, 94–107. [Google Scholar] [CrossRef] [Green Version]
- Turgut, C.; İzki, A.A. Hair loss due to pregabaline: A case report. Med. Res. Rep. 2020, 3, 41–45. [Google Scholar]
- Suh, J.H.; Oh, W.J.; Park, K.Y.; Seo, S.J.; Hong, C.K. DRESS syndrome induced by pregabalin in postherpetic neuralgia. Korean J. Derm. 2016, 68, 475–476. [Google Scholar]
- Franco, V.; Crema, F.; Iudice, A.; Zaccara, G.; Grillo, E. Novel treatment options for epilepsy: Focus on perampanel. Pharmacol. Res. 2013, 70, 35–40. [Google Scholar] [CrossRef]
- French, J.A.; Krauss, G.L.; Biton, V.; Squillacote, D.; Yang, H.; Laurenza, A.; Kumar, D.; Rogawski, M.A. Adjunctive perampanel for refractory partial-onset seizures: Randomized phase III study 304. Neurology 2012, 79, 589–596. [Google Scholar] [CrossRef]
- French, J.A.; Krauss, G.L.; Wechsler, R.T.; Wang, X.F.; DiVentura, B.; Brandt, C.; Trinka, E.; O’Brien, T.J.; Laurenza, A.; Patten, A.; et al. Perampanel for tonic-clonic seizures in idiopathic generalized epilepsy A randomized trial. Neurology 2015, 85, 950–957. [Google Scholar] [CrossRef] [Green Version]
- Lin, K.L.; Lin, J.J.; Chou, M.L.; Hung, P.C.; Hsieh, M.Y.; Chou, I.J.; Lim, S.N.; Wu, T.; Wang, H.S. Efficacy and tolerability of perampanel in children and adolescents with pharmacoresistant epilepsy: The first real-world evaluation in Asian pediatric neurology clinics. Epilepsy Behav. 2018, 85, 188–194. [Google Scholar] [CrossRef] [Green Version]
- Rohracher, A.; Zimmermann, G.; Villanueva, V.; Garamendi, I.; Sander, J.W.; Wehner, T.; Shankar, R.; Ben-Menachem, E.; Brodie, M.J.; Pensel, M.C.; et al. Perampanel in routine clinical use across Europe: Pooled, multicenter, observational data. Epilepsia 2018, 59, 1727–1739. [Google Scholar] [CrossRef]
- Villanueva, V.; Garcés, M.; López-González, F.J.; Rodriguez-Osorio, X.; Toledo, M.; Salas-Puig, J.; González-Cuevas, M.; Campos, D.; Serratosa, J.M.; González-Giráldez, B.; et al. Safety, efficacy and outcome-related factors of perampanel over 12 months in a real-world setting: The FYDATA study. Epilepsy Res. 2016, 126, 201–210. [Google Scholar] [CrossRef]
- Johansen, T.N.; Greenwood, J.R.; Frydenvang, K.; Madsen, U.; Krogsgaard-Larsen, P. Stereostructure-activity studies on agonists at the AMPA and kainate subtypes of ionotropic glutamate receptors. Chirality 2003, 15, 167–179. [Google Scholar] [CrossRef]
- Jara, C.P.; Berti, B.A.; Mendes, N.F.; Engel, D.F.; Zanesco, A.M.; Souza, G.F.; Bezerra, R.M.; Bagatin, J.T.; Maria-Engler, S.S.; Morari, J.; et al. Glutamic acid promotes hair growth in mice. Sci. Rep. 2021, 11, 15453. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.L.; Hsieh, M.Y.; Hsiao, P.F.; Sheen, J.M.; Yu, H.R.; Kuo, H.C.; Chen, S.T.; Huang, J.L.; Yang, K.D.; Lee, W.I. Alopecia areata universalis after phenobarbital-induced anti-convulsant hypersensitivity syndrome. Immunol. Investig. 2009, 38, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Knutsen, A.P.; Shah, M.; Schwarz, K.B.; Tsai, C.C. Graft versus host-like illness in a child with phenobarbital hypersensitivity. Pediatrics 1986, 78, 581–584. [Google Scholar] [CrossRef] [PubMed]
- Bavdekar, S.B.; Muranjan, M.N.; Gogtay, N.J.; Kantharia, V.; Kshirsagar, N.A. Anticonvulsant hypersensitivity syndrome: Lymphocyte toxicity assay for the confirmation of diagnosis and risk assessment. Ann. Pharmacother. 2004, 38, 1648–1650. [Google Scholar] [CrossRef]
- Ghorani-Azam, A.; Balali-Mood, M.; Riahi-Zanjani, B.; Darchini-Maragheh, E.; Sadeghi, M. Acute Phenobarbital Poisoning for the Management of Seizures in Newborns and Children; A Systematic Literature Review. CNS Neurol. Disord. Drug Targets 2021, 20, 174–180. [Google Scholar] [CrossRef]
- Lampl, Y.; Gilad, R.; Sarova-Pinchas, I.; Barak, Y. Hair loss-an adverse reaction to treatment with vigabatrin. Acta Therap. 1996, 22, 51–55. [Google Scholar]
- Graham, D. Neuropathology of vigabatrin. Br. J. Clin. Pharmacol. 1989, 27, 43–45. [Google Scholar] [CrossRef] [Green Version]
- Vossler, D.G.; Morris, G.L.; Harden, C.L.; Montouris, G.; Faught, E.; Kanner, A.M.; Fix, A.; French, J.A. Tiagabine in clinical practice: Effects on seizure control and behavior. Epilepsy Behav. 2013, 8, 211–216. [Google Scholar] [CrossRef]
- Holowach, J.; Sanden, H.V. Alopecia as a side effect of treatment of epilepsy with trimethadione: Report of two cases. N. Engl. J. Med. 1960, 263, 1187. [Google Scholar] [CrossRef]
- Wadhwa, S. Carbamazepine Induced Hypersensitivity Syndrome with Alopecia. J. Assoc. Physic. Ind. 1997, 45, 1. [Google Scholar]
- Kohno, Y.; Ishii, A.; Shoji, S. A case of hair loss induced by carbamazepine. Rinsho Shinkeigaku 2004, 44, 379–381. [Google Scholar]
- Zenkov, L.R. Alopecia associated with treatment of symptomatic focal epilepsy with carbamazepine. Neurol. J. 2008, 13, 31–32. [Google Scholar]
- Kenyon, K.; Mintzer, S.; Nei, M. Carbamazepine treatment of generalized tonic-clonic seizures in idiopathic generalized epilepsy. Seizure 2014, 23, 234–236. [Google Scholar] [CrossRef] [Green Version]
- Rathore, C.; Rawat, K.S.; Prakash, S.; Rana, K. Carbamazepine-Induced Acute Alopecia Areata. Neurology 2021, 97, 501–502. [Google Scholar] [CrossRef]
- Chen, C.M.; Chen, J.Y.; Chen, K.T.; Chu, C.C.; Tzeng, J.I.; Lan, K.M. A Case Report-Alopecia as a Rare but Possible Side Effect of Gabapentin. Chin. J. Pain 2010, 20, 40–44. [Google Scholar]
- Calabro, R.S.; Bramanti, P.; Spina, E.; Italiano, D. Can zinc depletion play a role in LEV-induced hair loss? Considerations from a case study. Epilepsy Behav. 2013, 29, 254–255. [Google Scholar] [CrossRef]
- Hamd, R.S.; Hasbini, D.A. Adolescent’s Hair Loss due to Levetiracetam. J. Pediatr. Epilepsy 2018, 7, 152–153. [Google Scholar] [CrossRef]
- Missori, P.; Currà, A. Reversible subacute hair loss induced by levetiracetam. Neurol. Sci. 2023, 44, 2207–2208. [Google Scholar] [CrossRef]
- Krivda, L.K.; Campagna, L.J.; Mignano, M.S.; Cho, C.S. Prolonged Drug-Induced Hypersensitivity Syndrome/DRESS with Alopecia Areata and Autoimmune Thyroiditis. Fed. Pract. 2022, 39, 350–354. [Google Scholar] [CrossRef]
- Laljee, H.C.; Parsonage, M.J. Unwanted effects of sodium valproate (Epilim) in the treatment of adult patients with epilepsy. R. Soc. Med 1980, 1, 141–158. [Google Scholar]
- Khan, T.A.; Sheng, H.; Mercke, Y.K.; Lippmann, S.B. Divalproex-induced alopecia: A case report. Psychiatr. Serv. 1999, 50, 1500. [Google Scholar] [CrossRef] [PubMed]
- Cinbis, M.; Parlaz, N. A case of alopecia areata associated with low dosage VPA treatment. Eur. J. Paediatr. Neurol. 2007, 11, 121. [Google Scholar] [CrossRef]
- Wilting, I.; Laarhoven, J.H.; Koning-Verest, I.F.; Egberts, A.C. Valproic acid-induced hair-texture changes in a white woman. Epilepsia 2007, 48, 400–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.; Beste, B. Valproate-induced hair loss: What to tell patients. Curr. Psychiatry 2011, 10, 74–75. [Google Scholar]
- Ramakrishnappa, S.K.; Belhekar, M.N. Serum drug level-related sodium valproate-induced hair loss. Indian J. Pharmacol. 2013, 45, 187–188. [Google Scholar] [CrossRef]
- Panwar, J.B.; Ishwar, C.; Bhardwaj, B.L.; Tilakraj, R.; Bansal, R. Sodium valproate induced alopecia in a patient of epilepsy. J. Dent. Med. Sci. 2016, 15, 112–114. [Google Scholar]
- Grootens, K.P.; Hartong, E.G. A Case Report of Biotin Treatment for Valproate-Induced Hair Loss. J. Clin. Psychiatry 2017, 78, e838. [Google Scholar] [CrossRef] [Green Version]
- Uygur, Ö.F.; Uygur, H. Valproate Induced Hair Loss and Curly Hair in Bipolar Disorder. Clin. Psychopharmacol. Neurosci. 2019, 17, 566–567. [Google Scholar] [CrossRef]
- Govindan, K.; Mandadi, G.D. Alopecia in Breastfed Infant Possibly Due to Mother Getting Valproate. Indian J. Pediatr. 2021, 88, 519–520. [Google Scholar] [CrossRef]
- Breathnach, S.M.; McGibbon, D.H.; Ive, F.A.; Black, M.M. Carbamazepine (‘Tegretol’) and toxic epidermal necrolysis: Report of three cases with histopathological observations. Clin. Exp. Dermatol. 1982, 7, 585–591. [Google Scholar] [CrossRef]
- Jeavons, P.M.; Clark, J.E.; Harding, G.F. Valproate and curly hair. Lancet 1977, 1, 359. [Google Scholar] [CrossRef]
- Tomita, T.; Goto, H.; Yoshida, T.; Tanaka, K.; Sumiya, K.; Kohda, Y. Dose-dependent valproate-induced alopecia in patients with mental disorders. Indian J. Pharmacol. 2015, 47, 690–692. [Google Scholar] [CrossRef] [Green Version]
- Cooper-Mahkorn, D.; Bauer, J. Alopecia areata during treatment with zonisamide—Two case reports. Aktuelle Neurol. 2007, 34, 354–355. [Google Scholar] [CrossRef]
- Hirsch, M.; Hintz, M.; Specht, A.; Schulze-Bonhage, A. Tolerability, efficacy and retention rate of Brivaracetam in patients previously treated with Levetiracetam: A monocenter retrospective outcome analysis. Seizure 2018, 61, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Ryvlin, P.; Dimova, S.; Elmoufti, S.; Floricel, F.; Laloyaux, C.; Nondonfaz, X.; Biton, V. Tolerability and efficacy of adjunctive brivaracetam in adults with focal seizures by concomitant antiseizure medication use: Pooled results from three phase 3 trials. Epilepsia 2022, 63, 2024–2036. [Google Scholar] [CrossRef]
- Talati, R.; Scholle, J.M.; Phung, O.J. Effectiveness and Safety of Antiepileptic Medications in Patients with Epilepsy [Internet]; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011; (Comparative Effectiveness Reviews, No. 40.) Results. Available online: https://www.ncbi.nlm.nih.gov/books/NBK83942/ (accessed on 28 May 2023).
- Richens, A.; Davidson, D.L.; Cartlidge, N.E.; Easter, D.J. A multicentre comparative trial of sodium valproate and carbamazepine in adult onset epilepsy. J. Neurol. Neurosurg. Psychiatry 1994, 57, 682–687. [Google Scholar] [CrossRef] [Green Version]
- Verity, C.M.; Hosking, G.; Easter, D.J. A multicentre comparative trial of sodium valproate and carbamazepine in paediatric epilepsy. Dev. Med. Child. Neurol. 1995, 37, 97–108. [Google Scholar] [CrossRef]
- Steinhoff, B.J.; Ueberall, M.A.; Siemes, H.; Kurlemann, G.; Schmitz, B.; Bergmann, L. The LAM-SAFE Study: Lamotrigine versus carbamazepine or valproic acid in newly diagnosed focal and generalised epilepsies in adolescents and adults. Seizure 2005, 14, 597–605. [Google Scholar] [CrossRef] [Green Version]
- Privitera, M.D.; Brodie, M.J.; Mattson, R.H.; Chadwick, D.W.; Neto, W.; Wang, S. Topiramate, carbamazepine and valproate monotherapy: Double-blind comparison in newly diagnosed epilepsy. Acta Neurol. Scand. 2003, 107, 165–175. [Google Scholar] [CrossRef]
- Wheless, J.W.; Neto, W.; Wang, S. Topiramate, carbamazepine, and valproate monotherapy: Double-blind comparison in children with newly diagnosed epilepsy. J. Child Neurol. 2004, 19, 135–141. [Google Scholar] [CrossRef]
- Donati, F.; Gobbi, G.; Campistol, J.; Rapatz, G.; Daehler, M.; Sturm, Y.; Aldenkamp, A.P. The cognitive effects of oxcarbazepine versus carbamazepine or valproate in newly diagnosed children with partial seizures. Seizure 2007, 16, 670–679. [Google Scholar] [CrossRef] [Green Version]
- Koeppen, D.; Baruzzi, A.; Capozza, M.; Chauvel, P.; Courjon, J.; Favel, P.; Harmant, J.; Lorenz, H.; Oller, F.V.; Procaccianti, G.; et al. Clobazam in therapy-resistant patients with partial epilepsy: A double-blind placebo-controlled crossover study. Epilepsia 1987, 28, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Satishchandra, P.; Rathore, C.; Apte, A.; Kumar, A.; Mandal, A.; Chauhan, D.; Agadi, J.; Gurumukhani, J.; Asokan, K.; Venkateshwarlu, K.; et al. Evaluation of one-year effectiveness of clobazam as an add-on therapy to anticonvulsant monotherapy in participants with epilepsy having uncontrolled seizure episodes: An Indian experience. Epilepsy Behav. 2022, 130, 108671. [Google Scholar] [CrossRef] [PubMed]
- Klein, P.; Aboumatar, S.; Brandt, C.; Dong, F.; Krauss, G.L.; Mizne, S.; Sanchez-Alvarez, J.C.; Steinhoff, B.J.; Villanueva, V. Long-Term Efficacy and Safety From an Open-Label Extension of Adjunctive Cenobamate in Patients with Uncontrolled Focal Seizures. Neurology 2022, 99, e989–e998. [Google Scholar] [CrossRef] [PubMed]
- Sperling, M.R.; Klein, P.; Aboumatar, S.; Gelfand, M.; Halford, J.J.; Krauss, G.L.; Rosenfeld, W.E.; Vossler, D.G.; Wechsler, R.; Borchert, L.; et al. Cenobamate (YKP3089) as adjunctive treatment for uncontrolled focal seizures in a large, phase 3, multicenter, open-label safety study. Epilepsia 2020, 61, 1099–1108. [Google Scholar] [CrossRef]
- Villanueva, V.; Santos-Carrasco, D.; Cabezudo-García, P.; Gómez-Ibáñez, A.; Garcés, M.; Serrano-Castro, P.; Castro-Vilanova, M.D.; Sayas, D.; Lopez-Gonzalez, F.J.; Rodríguez-Osorio, X.; et al. Real-world safety and effectiveness of cenobamate in patients with focal onset seizures: Outcomes from an Expanded Access Program. Epilepsia Open 2023. epub ahead of print. [Google Scholar] [CrossRef]
- Chaves, J.; Breia, P.; Pimentel, J.; Pelejão, R.; Carvalho, M.; Mateus, P.; Grebe, H.; Mestre, A.; Fernandes, H.; Sousa, R.; et al. Eslicarbazepine acetate as adjunctive therapy in clinical practice: ESLADOBA study. Acta Neurol. Scand. 2017, 136, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Galiana, G.L.; Gauthier, A.C.; Mattson, R.H. Eslicarbazepine Acetate: A New Improvement on a Classic Drug Family for the Treatment of Partial-Onset Seizures. Drugs R D 2017, 17, 329–339. [Google Scholar] [CrossRef] [Green Version]
- Hixson, J.; Gidal, B.; Pikalov, A.; Zhang, Y.; Mehta, D.; Blum, D.; Cantu, D.; Grinnell, T. Efficacy and safety of eslicarbazepine acetate as a first or later adjunctive therapy in patients with focal seizures. Epilepsy Res. 2021, 171, 106561. [Google Scholar] [CrossRef]
- Knoll, J.; Stegman, K.; Suppes, T. Clinical experience using gabapentin adjunctively in patients with a history of mania or hypomania. J. Affect. Disord. 1998, 49, 229–233. [Google Scholar] [CrossRef]
- Collins, A.; Mannion, R.; Broderick, A.; Hussey, S.; Devins, M.; Bourke, B. Gabapentin for the treatment of pain manifestations in children with severe neurological impairment: A single-centre retrospective review. BMJ Paediatr. Open 2019, 3, e000467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runge, U.; Arnold, S.; Brandt, C.; Reinhardt, F.; Kühn, F.; Isensee, K.; Ramirez, F.; Dedeken, P.; Lauterbach, T.; Noack-Rink, M.; et al. A noninterventional study evaluating the effectiveness and safety of lacosamide added to monotherapy in patients with epilepsy with partial-onset seizures in daily clinical practice: The VITOBA study. Epilepsia 2015, 56, 1921–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biton, V.; Levisohn, P.; Hoyler, S.; Vuong, A.; Hammer, A.E. Lamotrigine versus valproate monotherapy-associated weight change in adolescents with epilepsy: Results from a post hoc analysis of a randomized, double-blind clinical trial. J. Child Neurol. 2003, 18, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Morrell, M.J.; Hayes, F.J.; Sluss, P.M.; Adams, J.M.; Bhatt, M.; Ozkara, C.; Warnock, C.R.; Isojärvi, J. Hyperandrogenism, ovulatory dysfunction, and polycystic ovary syndrome with valproate versus lamotrigine. Ann. Neurol. 2008, 64, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Vining, E.P.; Mellitis, E.D.; Dorsen, M.M.; Cataldo, M.F.; Quaskey, S.A.; Spielberg, S.P.; Freeman, J.M. Psychologic and behavioral effects of antiepileptic drugs in children: A double-blind comparison between phenobarbital and valproic acid. Pediatrics 1987, 80, 165–174. [Google Scholar] [CrossRef]
- Kluger, G.; Kurlemann, G.; Haberlandt, E.; Ernst, J.P.; Runge, U.; Schneider, F.; Makowski, C.; Boor, R.; Bast, T. Effectiveness and tolerability of rufinamide in children and adults with refractory epilepsy: First European experience. Epilepsy Behav. 2009, 14, 491–495. [Google Scholar] [CrossRef]
- Tan, H.J.; Awadh, M.; O’Regan, M.; Martland, T.R.; Kneen, R. Effectiveness and Tolerability of Rufinamide in Children and Young People: A Survey of Experience from the United Kingdom. J. Pediatr. Epilepsy 2017, 6, 103–110. [Google Scholar]
- Krymchantowski, A.; Tavares, C. Weight variations in patients receiving topiramate migraine prophylaxis in a tertiary care setting. MedGenMed 2004, 6, 48. [Google Scholar]
- Turanli, G.; Celebi, A.; Yalnizoğlu, D.; Topçu, M.; Topaloğlu, H.; Banu, A.; Aysun, S. Vigabatrin in pediatric patients with refractory epilepsy. Turk. J. Pediatr. 2006, 48, 25–30. [Google Scholar]
- Christe, W.; Krämer, G.; Vigonius, U.; Pohlmann, H.; Steinhoff, B.J.; Brodie, M.J.; Moore, A. A double-blind controlled clinical trial: Oxcarbazepine versus sodium valproate in adults with newly diagnosed epilepsy. Epilepsy Res. 1997, 26, 451–460. [Google Scholar] [CrossRef]
- Jeavons, P.M.; Clark, J.E. Sodium valproate in treatment of epilepsy. Br. Med. J. 1974, 2, 584–586. [Google Scholar] [CrossRef] [Green Version]
- Gram, L.; Wulff, K.; Rasmussen, K.E.; Flachs, H.; Würtz-Jorgensen, A.; Sommerbeck, K.W.; Lohren, V. Valproate sodium: A controlled clinical trial including monitoring of drug levels. Epilepsia 1977, 18, 141–148. [Google Scholar] [CrossRef]
- Hassan, M.N.; Laljee, H.C.; Parsonage, M.J. Sodium valproate in the treatment of resistant epilepsy. Acta Neurol. Scand. 1976, 54, 209–218. [Google Scholar] [CrossRef]
- Coulter, D.L.; Wu, H.; Allen, R.J. Valproic acid therapy in childhood epilepsy. JAMA 1980, 244, 785–788. [Google Scholar] [CrossRef]
- Egger, J.; Brett, E.M. Effects of sodium valproate in 100 children with special reference to weight. Br. Med. J. 1981, 283, 577–581. [Google Scholar] [CrossRef] [Green Version]
- Turnbull, D.M.; Rawlins, M.D.; Weightman, D.; Chadwick, D.W. Plasma concentrations of sodium valproate: Their clinical value. Ann. Neurol. 1983, 14, 38–42. [Google Scholar] [CrossRef]
- Spitz, M.C.; Deasy, D.N. Conversion to valproate monotheraphy in nonretarded adults with primary Generalized tonic-clonic seizures. J. Epilepsy 1991, 4, 33–38. [Google Scholar] [CrossRef]
- Macritchie, K.A.; Geddes, J.R.; Scott, J.; Haslam, D.R.; Goodwin, G.M. Valproic acid, valproate and divalproex in the maintenance treatment of bipolar disorder. Cochrane Database Syst. Rev. 2001, 2001, CD003196. [Google Scholar]
- Schulpis, K.H.; Karikas, G.A.; Tjamouranis, J.; Regoutas, S.; Tsakiris, S. Low serum biotinidase activity in children with valproic acid monotherapy. Epilepsia 2001, 42, 1359–1362. [Google Scholar] [CrossRef]
- Ebrahimi, H.; Shamsadini, S.; Eshkavari, S.E. Frequency of Sodium Valproate-Induced Hair Loss and Curly Hair. Iran. J. Pharmacol. Ther. 2005, 4, 143–145. [Google Scholar]
- Kocer, A.; Sasmaz, S.; Ince, N.; Kutlar, M.; Cagirici, S. Skin findings related to chronic usage of anti-epileptic drugs. Neurosci. (Riyadh) 2005, 10, 268–271. [Google Scholar]
- Joffe, H.; Cohen, L.S.; Suppes, T.; McLaughlin, W.L.; Lavori, P.; Adams, J.M.; Hwang, C.H.; Hall, J.E.; Sachs, G.S. Valproate is associated with new-onset oligoamenorrhea with hyperandrogenism in women with bipolar disorder. Biol. Psychiatry 2006, 59, 1078–1086. [Google Scholar] [CrossRef]
- McCabe, P.H.; Michel, N.C.; McNew, C.D.; Lehman, E.B. Conversion from delayed-release sodium valproate to extended-release sodium valproate: Initial results and long-term follow-up. Epilepsy Behav. 2006, 8, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Jedrzejczak, J.; Kuncíková, M.; Magureanu, S. An observational study of first-line valproate monotherapy in focal epilepsy. Eur. J. Neurol. 2008, 15, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Castro-Gago, M.; Pérez-Gay, L.; Gómez-Lado, C.; Castiñeiras-Ramos, D.E.; Otero-Martínez, S.; Rodríguez-Segade, S. The influence of valproic acid and carbamazepine treatment on serum biotin and zinc levels and on biotinidase activity. J. Child Neurol. 2011, 26, 1522–1524. [Google Scholar] [CrossRef]
- Han, X.N.; Ma, L.; Zhang, H.L.; You, H.S. Analysis of 59 cases of adverse drug reactions induced by valproate sodium. Chin. Hosp. Pharm. J. 2015, 39, 57–60. [Google Scholar]
- Kompally, D.V.; Ananthula, K.; Adla, N.; Rajesh, V. Prospective Observational Study of Sodium Valproate in Seizure Control and Associated Adverse Drug Reactions in Pediatric Population. J. Dent. Med. Sci. 2015, 14, 28–34. [Google Scholar]
- Yamak, W.R.; Hmaimess, G.; Makke, Y.; Sabbagh, S.; Arabi, M.; Beydoun, A.; Nasreddine, W. Valproate-induced enuresis: A prospective study. Dev. Med. Child Neurol. 2015, 57, 737–741. [Google Scholar] [CrossRef] [Green Version]
- Druschky, K.; Bleich, S.; Grohmann, R.; Burda, K.; Frieling, H.; Hillemacher, T.; Neyazi, A.; Stübner, S.; Toto, S. Severe hair loss associated with psychotropic drugs in psychiatric inpatients-Data from an observational pharmacovigilance program in German-speaking countries. Eur. Psychiatry 2018, 54, 117–123. [Google Scholar] [CrossRef]
- Pruccoli, J.; Parmeggiani, A. The Role of Mood Stabilizers in Children and Adolescents with Anorexia Nervosa: A 1-year Follow-Up, Propensity Score-Matched Study. Pharmacopsychiatry 2023, 56, 118–125. [Google Scholar] [CrossRef]
- Liparoti, G.; Burchiani, B.; Mencaroni, E.; Tripodi, D.; Cara, G.; Verrotti, A. Individualizing doses of antiepileptic drugs. Expert Opin. Drug Metab. Toxicol. 2022, 18, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Asghar, F.; Shamim, N.; Farooque, U.; Sheikh, H.; Aqeel, R. Telogen Effluvium: A Review of the Literature. Cureus 2020, 12, e8320. [Google Scholar] [CrossRef] [PubMed]
- Yin, G.O.; Siong-See, J.L.; Wang, E.C. Telogen Effluvium—A review of the science and current obstacles. J. Dermatol. Sci. 2021, 101, 156–163. [Google Scholar]
- Park, S.H.; Seol, J.E.; Kim, D.H.; Kim, H. Analysis of Microscopic Examination of Pulled Out Hair in Telogen Effluvium Patients. Ann. Dermatol. 2020, 32, 141–145. [Google Scholar] [CrossRef]
- McDonald, K.A.; Shelley, A.J.; Colantonio, S.; Beecker, J. Hair pull test: Evidence-based update and revision of guidelines. J. Am. Acad. Dermatol. 2017, 76, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Poonia, K.; Thami, G.P.; Bhalla, M.; Jaiswal, S.; Sandhu, J. NonScarring Diffuse Hair Loss in Women: A Clinico-Etiological Study from tertiary care center in North-West India. J. Cosmet. Dermatol. 2019, 18, 401–407. [Google Scholar] [CrossRef]
- Grover, C.; Khurana, A. Telogen effluvium. Indian J. Dermatol. Venereol. Leprol. 2013, 79, 591–603. [Google Scholar] [CrossRef]
- Harrison, S.; Sinclair, R. Telogen effluvium. Clin. Exp. Dermatol. 2002, 27, 389–395. [Google Scholar] [CrossRef]
- Kanwar, A.J.; Narang, T. Anagen effluvium. Indian J. Dermatol. Venereol. Leprol. 2013, 79, 604–612. [Google Scholar] [CrossRef]
- Liyanage, D.; Sinclair, R. Telogen Effluvium. Cosmetics 2016, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Dhurat, R.; Saraogi, P. Hair evaluation methods: Merits and demerits. Int. J. Trichol. 2009, 1, 108–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Springer, K.; Brown, M.; Stulberg, D.L. Common hair loss disorders. Am. Fam. Physician 2003, 68, 93–102. [Google Scholar] [PubMed]
- Hoffmann, A.; Waśkiel-Burnat, A.; Żółkiewicz, J.; Blicharz, L.; Rakowska, A.; Goldust, M.; Olszewska, M.; Rudnicka, L. Pili Torti: A Feature of Numerous Congenital and Acquired Conditions. J. Clin. Med. 2021, 10, 3901. [Google Scholar] [CrossRef] [PubMed]
- Almohanna, H.M.; Ahmed, A.A.; Tsatalis, J.P.; Tosti, A. The Role of Vitamins and Minerals in Hair Loss: A Review. Dermatol. Ther. 2019, 9, 51–70. [Google Scholar] [CrossRef] [Green Version]
- Slonim, A.E.; Sadick, N.; Pugliese, M.; Meyers-Seifer, C.H. Clinical response of alopecia, trichorrhexis nodosa, and dry, scaly skin to zinc supplementation. J. Pediatr. 1992, 121, 890–895. [Google Scholar] [CrossRef]
- Suzuki, T.; Koizumi, J.; Moroji, T.; Shiraishi, H.; Hori, T.; Baba, A.; Kawai, N.; Tada, K. Effects of long-term anticonvulsant therapy on copper, zinc, and magnesium in hair and serum of epileptics. Biol. Psychiatry 1992, 31, 571–581. [Google Scholar] [CrossRef]
- Kuzuya, T.; Hasegawa, T.; Shimizu, K.; Nabeshima, T. Effect of anti-epileptic drugs on serum zinc and copper concentrations in epileptic patients. Int. J. Clin. Pharmacol. Ther. Toxicol. 1993, 31, 61–65. [Google Scholar]
- Asadi-Pooya, A.A.; Rostaminejad, M.; Zeraatpisheh, Z.; Damabi, N.M. Cosmetic adverse effects of antiseizure medications; A systematic review. Seizure 2021, 91, 9–21. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Query | MeSH Terms | Results |
|---|---|---|
| (alopecia) AND (valproate) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“valproat”[All Fields] OR “valproate s”[All Fields] OR “valproates”[All Fields] OR “valproic acid”[MeSH Terms] OR (“valproic”[All Fields] AND “acid”[All Fields]) OR “valproic acid”[All Fields] OR “valproate”[All Fields]) | 70 |
| (alopecia) AND (carbamazepine) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“carbamazepine”[MeSH Terms] OR “carbamazepine”[All Fields] OR “carbamazepin”[All Fields] OR “carbamazepines”[All Fields] OR “carbamazepine s”[All Fields]) | 31 |
| (alopecia) AND (phenytoin) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“phenytoin”[MeSH Terms] OR “phenytoin”[All Fields] OR “phenytoine”[All Fields] OR “phenytoin s”[All Fields] OR “phenytoins”[All Fields]) | 20 |
| (alopecia) AND (phenobarbital) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“phenobarbital”[MeSH Terms] OR “phenobarbital”[All Fields] OR “phenobarbitals”[All Fields]) | 16 |
| (alopecia) AND (lamotrigine) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“lamotrigin”[All Fields] OR “lamotrigine”[MeSH Terms] OR “lamotrigine”[All Fields] OR “lamotrigine s”[All Fields]) | 10 |
| (alopecia) AND (levetiracetam) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“levetiracetam”[MeSH Terms] OR “levetiracetam”[All Fields]) | 8 |
| (alopecia) AND (gabapentin) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“gabapentin”[MeSH Terms] OR “gabapentin”[All Fields] OR “gabapentine”[All Fields] OR “gabapentin s”[All Fields]) | 6 |
| (alopecia) AND (topiramate) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“topiramate”[MeSH Terms] OR “topiramate”[All Fields] OR “topiramate s”[All Fields]) | 5 |
| (alopecia) AND (oxcarbazepine) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“oxcarbazepin”[All Fields] OR “oxcarbazepine”[MeSH Terms] OR “oxcarbazepine”[All Fields]) | 4 |
| (alopecia) AND (clobazam) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“clobazam”[MeSH Terms] OR “clobazam”[All Fields]) | 2 |
| (alopecia) AND (felbamate) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“felbamate”[MeSH Terms] OR “felbamate”[All Fields]) | 2 |
| (alopecia) AND (vigabatrin) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“vigabatrin”[MeSH Terms] OR “vigabatrin”[All Fields] OR “vigabatrine”[All Fields]) | 2 |
| (alopecia) AND (pregabalin) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“pregabalin”[MeSH Terms] OR “pregabalin”[All Fields] OR “pregabalin s”[All Fields] OR “pregabaline”[All Fields]) | 1 |
| (alopecia) AND (primidone) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“primidone”[MeSH Terms] OR “primidone”[All Fields] OR “primidon”[All Fields]) | 1 |
| (alopecia) AND (trimethadione) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“trimethadione”[MeSH Terms] OR “trimethadione”[All Fields]) | 1 |
| (alopecia) AND (zonisamide) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“zonisamid”[All Fields] OR “zonisamide”[MeSH Terms] OR “zonisamide”[All Fields] OR “zonisamide s”[All Fields]) | 1 |
| (alopecia) AND (brivaracetam) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“brivaracetam”[Supplementary Concept] OR “brivaracetam”[All Fields]) | 0 |
| (alopecia) AND (cenobamate) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“cenobamate”[Supplementary Concept] OR “cenobamate”[All Fields] OR “cenobamate”[All Fields]) | 0 |
| (alopecia) AND (eslicarbazepine) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“eslicarbazepine”[Supplementary Concept] OR “eslicarbazepine”[All Fields]) | 0 |
| (alopecia) AND (lacosamide) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“lacosamide”[MeSH Terms] OR “lacosamide”[All Fields]) | 0 |
| (alopecia) AND (perampanel) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“perampanel”[Supplementary Concept] OR “perampanel”[All Fields]) | 0 |
| (alopecia) AND (rufinamide) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“rufinamide”[Supplementary Concept] OR “rufinamide”[All Fields]) | 0 |
| (alopecia) AND (tiagabine) | (“alopecia”[MeSH Terms] OR “alopecia”[All Fields] OR “alopecias”[All Fields]) AND (“tiagabine”[MeSH Terms] OR “tiagabine”[All Fields]) | 0 |
| Management | Comment | Reference |
|---|---|---|
| General measures | Reassurance. Alopecia is a benign side effect and is usually reversible. Additionally, provide hair care techniques. Advise to use soft brushes and mild shampoos and avoid dyes, heated curlers, and hair dryers. | Praharaj et al. (2022) [36] |
| Adjustment of VPA dosage | If feasible, VPA should be discontinued. Dose reduction of VPA was associated with hair regrowth. Additionally, a gradual increase in VPA dose was effective in the management of neurological conditions without affecting hair growth in some cases. | Uehlinger et al. (1992) [42] Henriksen et al. (1982) [43] Wang et al. (2019) [35] |
| Mineral supplementation | Iron, copper, magnesium, selenium, and zinc could be useful in treating hair loss associated with VPA. Zinc and selenium supplementation can help prevent further hair loss and promote regrowth. | Fatemi et al. (1995) [44] Trost et al. (2006) [45] |
| Vitamin supplementation | Oral administration of biotin (10 mg/day) shorted hair regrowth time. Other vitamins can be prescribed, but there is no evidence of their efficacy. | Castro-Gago et al. (2010) [46] Yilmaz et al. (2009) [38] |
| Agomelatine administration | Agomelatine was associated with a reduction of hair loss related to VPA. Agomelatine use should be attempted when the offending drug cannot be discontinued. | Sahin et al. (2017) [47] |
| Minoxidil administration | Minoxidil was associated with a reduction of hair loss related to VPA. Minoxidil use should be attempted when the offending drug cannot be discontinued. | Thomson et al. (2017) [48] |
| Topical VPA therapy | Topical application of VPA was found to promote hair growth. | Kakunje et al. (2018) [49] |
| Others | Advise the patient not to take VPA during meals to reduce its chelating effect on metals. VPA can affect zinc and selenium absorption, two metals associated with hair growth. | Praharaj et al. (2022) [36] |
| Case Reports | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Reference | ASM | Diagnosis | Dose (mg/day) | Duration a | Comment b,c | ||||
| Shuper et al. (1985) [51] | CBZ | Epilepsy | 150–300 | 1 month | Hair loss reversed when CBZ was discontinued. The patient was also taking propranolol, known to cause hair shedding. However, propranolol was discontinued six months before the initiation of CBZ. Objective: primary objective. GRADE: Very low. | ||||
| Wadhwa et al. (1997) [100] | CBZ | Epilepsy | NA | NA | CBZ-hypersensitivity syndrome presenting with alopecia. Objective: primary objective. GRADE: Very low. | ||||
| Kohno et al. (2004) [101] | CBZ | NA | NA | 1 week | The serum concentration of CBZ was 8.6 mcg/mL (therapeutic range: 8–12 mcg/mL). CBZ was discontinued, and hair loss stopped. Hair regrowth was observed within several days. Objective: primary objective. GRADE: Very low. | ||||
| Oh et al. (2008) [54] | CBZ | Neuropathic pain | 600 | 3 months | Alopecia was seen at CBZ 600 mg/day. The hair pull test was positive. Alopecia was reversed with a CBZ dose reduction to 200 mg/day. Objective: primary objective. GRADE: Very low. | ||||
| Zenkov et al. (2008) [102] | CBZ | Epilepsy | NA | Weeks (undefined) | CBZ was discontinued. Complete hair regrowth was observed within one year. Objective: primary objective. GRADE: Very low. | ||||
| Kenyon et al. (2014) [103] | CBZ | GTCS | NA | 4.5 years | CBZ was replaced by OXC. Objective: primary objective. GRADE: Very low. | ||||
| Rathore et al. (2021) [104] | CBZ | Focal epilepsy | 200 | 3 days | Hair regrowth was observed within two months of management. Objective: primary objective. GRADE: Very low. | ||||
| Picard et al. (1997) [70] | GBP | Focal epilepsy | 1800 | 4–8 weeks | Hair regrowth commenced three weeks after GBP discontinuation. A complete reversal of alopecia was observed in the first month of follow-up. Objective: primary objective. GRADE: Very low. | ||||
| Eker et al. (2009) [69] | GBP | Neuropathic pain | 1800 | 1 week | Significant hair loss with patchy areas of alopecia among areas of normal hair growth was seen. Hair shedding was more evident in the frontal and parietal regions. Shedding stopped two months after the discontinuation of GBP. Objective: primary objective. GRADE: Very low. | ||||
| Chen et al. (2010) [105] | GBP | Postherpetic neuralgia | 1200 | 3 weeks | Hair regrowth started four weeks after GBP discontinuation. Her hair growth resumed completely within three months. Objective: primary objective. GRADE: Very low. | ||||
| Calabro et al. (2013) [106] | LEV | GTCS | 1500 | 1 month | During LEV therapy, serum zinc levels were low (45 μg/dL [normal range: 70–150 μg/dL]). After one year of LEV discontinuation, serum zinc levels increased to 90 μg/dL. Objective: primary objective. GRADE: Very low. | ||||
| Hamd et al. (2018) [107] | LEV | Focal epilepsy | 750 | 2 months | Hair loss showed moderate improvement after discontinuation of LEV. Additionally, zinc intake was advised. Objective: primary objective. GRADE: Very low. | ||||
| Missori et al. (2023) [108] | LEV | Epilepsy | 1000 | 4 weeks | LEV was discontinued. The progression of alopecia stopped immediately, and the patient’s hair mostly grew back three months later. Objective: primary objective. GRADE: Very low. | ||||
| Patrizi et al. (2005) [58] | LTG | NA | 100 | Months | The exact duration was not specified. It is possibly the first case of alopecia secondary to LTG. Objective: primary objective. GRADE: Very low. | ||||
| Hillemacher et al. (2006) [59] | LTG | BD | 150 | 3 weeks | Rapid regression of hair loss was seen after LTG discontinuation. Objective: primary objective. GRADE: Very low. | ||||
| Solmi et al. (2017) [60] | LTG | Major depressive disorder | NA | NA | Naranjo algorithm scored 8 (probable). Objective: primary objective. GRADE: Very low. | ||||
| Krivda et al. (2022) [109] | LTG | BD type II | 100 | 5 weeks | LTG-associated hypersensitivity syndrome with development of extensive alopecia. Objective: primary objective. GRADE: Very low. | ||||
| Turgut et al. (2020) [82] | PGB | Fibromyalgia | 150 | 21 days | PGB was discontinued. Hair regrowth was complete after two weeks. Objective: primary objective. GRADE: Very low. | ||||
| Suh et al. (2016) [83] | PGB | Postherpetic neuralgia | NA | 36 weeks | She presented focal alopecia and pruritic erythema. After PGB discontinuation, hair regrowth was observed. | ||||
| Knutsen et al. (1986) [93] | PHB | Epilepsy | NA | 3 months | Skin biopsy: prominent miniaturization, no terminal hair, and perifollicular–peribulbar inflammation. Alopecia outcome: hair regrowth within three months. Triamcinolone acetonide was started. Objective: primary objective. GRADE: Very low. | ||||
| Bavdekar et al. (2004) [94] | PHB | Epilepsy | NA | 3 months | Skin biopsy: hyperkeratosis with follicular plugging and a prominent mononuclear perivascular and dermal infiltrate. A prominent panvascular mononuclear cell infiltrates the submucosa and migration to the epidermis, causing spongiosis and the presence of “mummified” cells. Alopecia outcome: hair regrowth was observed within two weeks. Prednisolone was started. Objective: primary objective. GRADE: Very low. | ||||
| Huang et al. (2009) [92] | PHB | Epilepsy | NA | 13th day | Skin biopsy: not performed. Alopecia outcome: total recovery within two months. Objective: primary objective. GRADE: Very low. | ||||
| Mangalvedhekar et al. (2001) [77] | PHT | NA | NA | NA | PHT-induced lupus erythematous. The patient presented with alopecia. Objective: primary objective. GRADE: Very low. | ||||
| Neki et al. (2015) [78] | PHT | GTCS | 300 | 2 years | PHT-induced lupus erythematous. The patient presented with alopecia. Objective: primary objective. GRADE: Very low. | ||||
| Kuhne et al. (2019) [76] | PHT | GTCS | NA | NA | The patient developed alopecia probably due to PHT-induced lupus erythematous. Objective: primary objective. GRADE: Very low. | ||||
| Chuang et al. (2002) [71] | TPM | Focal epilepsy | NA | 2 months | Reversible alopecia upon discontinuation of TPM. Recurred after reintroduction of TPM. Objective: primary objective. GRADE: Very low. | ||||
| Ghafoor et al. (2017) [72] | TPM | Migraine | 50 | 3 months | Alopecia stopped with the dose reduction to TPM 25 mg/day. Alopecia recurred with increasing the dose to 50 mg/day. Objective: primary objective. GRADE: Very low. | ||||
| Lagrand et al. (2021) [73] | TPM | Tremor-dominant Parkinson’s disease | 50 | 2 weeks | Hair regrowth was observed some weeks after. In this patient, alopecia was observed with levodopa, propranolol, and TPM. Objective: primary objective. GRADE: Very low. | ||||
| Laljee et al. (1980) [110] | VPA | Epilepsy | NA | NA | Persistent hair loss was reported in one individual. Objective: primary objective. GRADE: Very low. | ||||
| Uehlinger et al. (1992) [42] | VPA | Schizophrenia | 1300 | 3 months | The VPA was discontinued after alopecia. A rechallenge of VPA did not cause hair loss. Noteworthily, the VPA reintroduction was titrated. Objective: primary objective. GRADE: Very low. | ||||
| Fatemi et al. (1995) [44] | VPA | BD | 3000 | NA | Zinc supplementation led to alopecia remittance. Transient return of alopecia, which was remitted after a temporary VPA dose reduction. Objective: primary objective. GRADE: Very low. | ||||
| McKinney et al. (1996) [28] | VPA | BD | 1500 | 6 weeks | Multivitamin supplementation with selenium was started, but hair loss continued. VPA dose was reduced to 1000 mg/day and maintained. After 16 weeks, hair loss slowed. On the fifth month of VPA therapy, hair regrowth was observed. Objective: primary objective. GRADE: Very low. | ||||
| Khan et al. (1999) [111] | VPA | BD, epilepsy | NA | NA | A patient who developed acute transient alopecia of all scalp hair after a suicidal attempt with VPA overdose. Objective: primary objective. GRADE: Very low. | ||||
| Cinbis et al. (2007) [112] | VPA | NA | NA | 7th day | Alopecia was a secondary effect of a low dose of VPA. The pediatric individual was taking VPA 10 mg/kg/day. Objective: primary objective. GRADE: Very low. | ||||
| Wilting et al. (2007) [113] | VPA | NA | 1000 | NA | Hair texture changes were noted with increasing the dose of VPA from 1000 to 2000 mg/day. When the dosage was lowered again to 1000 mg/day, curliness disappeared but hair thinning was still present. Objective: primary objective. GRADE: Very low. | ||||
| Jain et al. (2011) [114] | VPA | BD | 1250 | 1 month | NA. Objective: primary objective. GRADE: Very low. | ||||
| Ramakrishnappa et al. (2013) [115] | VPA | GTCS | NA | 10 months | Trichogram revealed an increase in resting and dystrophic hair at the expense of growing hair. Co-occurrence between high serum levels of VPA and onset of alopecia. VPA was discontinued, and hair regrowth was observed. Objective: primary objective. GRADE: Very low. | ||||
| Panwar et al. (2016) [116] | VPA | GTCS | 1000 | 25 days | A trichogram and punch biopsy of the scalp revealed a diagnosis of anagen effluvium. Objective: primary objective. GRADE: Very low. | ||||
| Grootens et al. (2017) [117] | VPA | BD type I | NA | 1 month | The VPA-induced alopecia was observed within one month. The VPA was maintained at the same dose until the ninth month. After, biotin was started with VPA therapy. Three months later, her excessive hair loss completely disappeared. Complete hair regrowth was observed. | ||||
| Sahin et al. (2017) [47] | VPA | BD type II | 1250 | NA | Agomelatine (25 mg/day) was added to his therapeutical management. His hair loss stopped, and hair regrowth was observed. VPA dose was unchanged. Objective: primary objective. GRADE: Very low. | ||||
| Uygur et al. (2019) [118] | VPA | BD | 1250 | NA | Alopecia as a secondary effect of VPA was observed. In the ninth month, hair growth was curly. Objective: primary objective. GRADE: Very low. | ||||
| Govindan et al. (2020) [119] | VPA | BD | NA | 4 months | Alopecia was observed in a breastfed infant, possibly due to the mother taking VPA. Two months after VPA discontinuation by the mother, hair regrowth in the breastfed infant was observed. A complete reversal of alopecia was observed. Objective: primary objective. GRADE: Very low. | ||||
| Case series | |||||||||
| Reference | ASM | N of cases | Diagnosis | Dosage (mg/day) | Duration | Comment | |||
| Breathnach et al. (1982) [120] | CBZ | 2 | Trigeminal neuralgia, mood stabilizer | 300 | 2 weeks | Transient alopecia was observed. Objective: primary objective. GRADE: Low. | |||
| Ikeda et al. (1997) [53] | CBZ | 2 | Focal epilepsy | 300–600 | 2 months | Serum CBZ levels for both patients were 5 mg/L and 6.5 mg/L when hair loss started. Objective: primary objective. GRADE: Low. | |||
| Zou et al. (2014) [65] | LEV | 5 | Focal epilepsy or GTCS | 500–1000 | 3–8 weeks | Hair loss was remitted/improved in all five patients. No relationship of LEV dose with the time of alopecia onset was observed. Objective: primary objective. GRADE: Low. | |||
| Aghamollaii et al. (2017) [66] | LEV | 3 | Myoclonic epilepsy | 1250–1500 | 2 months | In all three patients, zinc supplementation resolved alopecia despite the continuation of LEV. In one individual, the LEV dose was increased to 1750 mg/day without the occurrence of alopecia. Objective: primary objective. GRADE: Low. | |||
| Holowach et al. (1960) [99] | TMD | 2 | Focal epilepsy or GTCS | 900–1200 | 6 weeks | Hair regrowth started after TMD discontinuation. Objective: primary objective. GRADE: Low. | |||
| Lampl et al. (1996) [96] | VGB | 5 | Focal epilepsy | 2000 | 3–7 weeks | Hair regrowth was seen after 1–8 weeks of VGB discontinuation. Objective: primary objective. GRADE: Low. | |||
| Jeavons et al. (1977) [121] | VPA | 5 | NA | NA | NA | Five cases of VPA-induced alopecia. Interestingly, the regrowth of hair was curly. Objective: primary objective. GRADE: Low. | |||
| Tomita et al. (2015) [122] | VPA | 3 | 2 BD and 1 focal epilepsy | 800–1200 | 40 days | A patient showed hair loss improvement within 15 days of the management. The other individual improved after 84 days. Objective: primary objective. GRADE: Low. | |||
| Thomson et al. (2017) [48] | VPA | 3 | GTCS | 500–1500 | 7 months | Zinc supplementation improved hair loss in two patients within 1–2 months. Higher doses of VPA caused alopecia earlier than lower doses of VPA. Objective: primary objective. GRADE: Low. | |||
| Cooper-Mahkorn et al. (2007) [123] | ZNS | 2 | Focal epilepsy | 300–500 | 9 months | In both patients, hair loss was reversible after ZNS discontinuation. Objective: primary objective. GRADE: Low. | |||
| Mixed studies | |||||||||
| Reference | ASM | Study type | N of cases | Comment | |||||
| Hirsch et al. (2018) [124] | BRV | Observational study | 102 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Ryvlin et al. (2022) [125] | BRV | Clinical trial | 1164 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Talati et al. (2011) [126] | CBZ | Systematic review | NA | No differences in the risk of alopecia were noted with newer antiseizure medications and CBZ. Newer antiseizure medications decreased the risk of experiencing alopecia when compared with VPA and when LTG and TPM were individually compared with VPA. Objective: primary objective. GRADE: High. | |||||
| Mattson et al. (1992) [52] | CBZ; VPA | Randomized controlled trial | 480 | Overall, failure in management was more commonly due to seizures in VPA patients and to serious side effects in CBZ individuals. Dose investigate: CBZ: 722 mg/day (mean); VPA: 2099 mg/day (mean). Objective: secondary objective. GRADE: Low. | |||||
| Richens et al. (1994) [127] | CBZ; VPA | Clinical trial | 300 | VPA: five cases; CBZ: one case. Objective: secondary objective. GRADE: Low. | |||||
| Pillans et al. (1995) [33] | CBZ; VPA | Systematic review | 820 | Reports of alopecia in the World Health Organization (WHO) database on 24 August 1994. Objective: primary objective. GRADE: High. | |||||
| Verity et al. (1995) [128] | CBZ; VPA | Clinical trial | 260 | VPA: five cases; CBZ: two cases. The drug therapy duration was 3 months. Objective: secondary objective. GRADE: Low. | |||||
| Steinhoff et al. (2005) [129] | CBZ; LTG; VPA | Clinical trial | 239 | LTG: six (4.95%) cases of alopecia; VPA: three (10%) cases of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Privitera et al. (2003) [130] | CBZ; TPM; VPA | Clinical trial | 613 | TPM 100 mg: four (1.9%) cases of alopecia; TPM 200 mg: two (1%) cases of alopecia; CBZ 600 mg: two (1.58%) cases of alopecia; VPA 1250 mg: 14 (17.94%) cases of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Wheless et al. (2004) [131] | CBZ; TPM; VPA | Clinical trial | 613 | VPA 1250 mg: two (11%) cases of alopecia. CBZ: one (4%) case of alopecia. There were no cases of TPM-induced alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Donati et al. (2007) [132] | CBZ, OXC, VPA | Clinical trial | 112 | CBZ: one case; VPA: three cases. There was no report of OXC-induced alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Koeppen et al. (1987) [133] | CLB | Clinical trial | 129 | The study reported one case of alopecia. The study was a double-blind, placebo-controlled crossover. Objective: secondary objective. GRADE: Low. | |||||
| Satishchandra et al. (2022) [134] | CLB | Observational study | 429 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Klein et al. (2022) [135] | CNB | Clinical trial | 355 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Sperling et al. (2020) [136] | CNB | Clinical trial | 1347 | The study reported fifteen cases of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Villanueva et al. (2023) [137] | CNB | Observational study | 2 | The study reported two cases of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Chaves et al. (2017) [138] | ESL | Cohort study | 52 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Galiana et al. (2017) [139] | ESL | Review | NA | Most common skin reactions were rash, alopecia, and hyperhidrosis, which occurred in 0.5–3.2% of the ESL users. Objective: secondary objective. GRADE: Low. | |||||
| Hixson et al. (2021) [140] | ESL | Clinical trial | 102 | ESL was taken as adjunctive therapy to LEV or LTG. Objective: secondary objective. GRADE: Low. | |||||
| Knoll et al. (1998) [141] | GBP | Observational study | 12 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Collins et al. (2019) [142] | GBP | Observational study | 42 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Runge et al. (2015) [143] | LCM | Observational analysis | 571 | The study reported seven cases of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Biton et al. (2003) [144] | LTG, VPA | Clinical trial | 38 | Three individuals developed alopecia secondary to VPA. There were no reports of LTG-induced alopecia. The drug therapy duration was 8 months. Objective: secondary objective. GRADE: Low. | |||||
| Morrell et al. (2008) [145] | LTG, VPA | Clinical trial | 447 | VPA: 25 (11%) cases of alopecia; LTG: three (1%) cases of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Tengstrand et al. (2010) [61] | LTG | Retrospective analysis | 337 | Hair loss due to LTG occurs more often in women. Specific time of alopecia onset was <1 month: 22/110; 1–6 months: 50/110; ≥6 months: 38/110. Of 337 cases, 112 individualsused LTG. Rash was the most common co-reported reaction alongside alopecia (18/337). The drug therapy duration was 1–6 months. The dose investigated was 200–500 mg/day. Objective: primary objective. GRADE: Moderate. | |||||
| Chen et al. (2015) [4] | CBZ, LEV, LTG, PGB, PHT, TPM, VPA | Retrospective analysis | 1903 | ASM | Number of individuals using ASM | Percentage of individuals who developed alopecia | Percentage of individuals who discontinued ASM due to alopecia | ||
| LEV | 524 | 0.4% | 0.4% | ||||||
| LTG | 521 | 0.8% | 0.6% | ||||||
| PHT | 404 | 0.3% | 0.3% | ||||||
| CBZ | 326 | 0.3% | 0.3% | ||||||
| VPA | 270 | 8.9% | 8.2% | ||||||
| TPM | 230 | 1.7% | 1.7% | ||||||
| PGB | 143 | 0.7% | 0.7% | ||||||
| Objective: primary objective. GRADE: Moderate. | |||||||||
| Herranz et al. (1988) [74] | PHB, PRM, PHT, CBZ, VPA | Observational analysis | 392 | PHB: one case; PRM: one case; VPA: three cases. There were no cases of alopecia associated with PHT or CBZ. Objective: secondary objective. GRADE: Low. | |||||
| Vining et al. (1987) [146] | PHB, VPA | Clinical trial | 21 | VPA: seven cases; PHB: one case. Objective: secondary objective. GRADE: Low. | |||||
| Harmark et al. (2011) [80] | PGB | Observational analysis | 1373 | Web-based intensive monitoring system based at the Netherlands Pharmacovigilance Centre Lareb. Objective: primary objective. GRADE: Low. | |||||
| Villanueva et al. (2016) [89] | PMP | Observational analysis | 464 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Rohracher et al. (2018) [88] | PMP | Observational analysis | 2396 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Kluger et al. (2009) [147] | RFM | Observational analysis | 60 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Tan et al. (2017) [148] | RFM | Observational analysis | 76 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Vossler et al. (2013) [98] | TGB | Randomized controlled trial | 292 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Mercke et al. (2000) [8] | TGB | Review | NA | The incidence tiagabine-induced alopecia was 1%. Objective: primary objective. GRADE: Low. | |||||
| Krymchantowski et al. (2004) [149] | TPM | Randomized controlled trial | 175 | Alopecia was observed in one individual (3.7%). The dose investigated was 100 mg/day. Objective: secondary objective. GRADE: Low. | |||||
| Turanli et al. (2006) [150] | VGB | Observational study | 111 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Christe et al. (1997) [151] | VPA, OXC | Clinical trial | 249 | VPA: four cases. There was no case report of alopecia secondary to OXC. Objective: secondary objective. GRADE: Low. | |||||
| Jeavons et al. (1974) [152] | VPA | Clinical trial | 63 | All the individuals were in use of VPA and PHT. Definite hair loss was only observed in two patients. Objective: secondary objective. GRADE: Low. | |||||
| Gram et al. (1977) [153] | VPA | Clinical trial | 39 | The study reported two cases of alopecia. VPA dose was maintained. Objective: secondary objective. GRADE: Low. | |||||
| Hassan et al. (1979) [154] | VPA | Clinical trial | 115 | The study reported one case of alopecia. He had diffuse alopecia unassociated with any evidence of a primary hair or scalp disorder. The dose investigated was 400–2400 mg/day. Objective: secondary objective. GRADE: Low. | |||||
| Coulter et al. (1980) [155] | VPA | Clinical trial | 100 | The study reported one case of alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Egger et al. (1981) [156] | VPA | Observational study | 100 | VPA-induced alopecia was observed in six individuals. In three of them, the hair became curly, especially in the frontal region. Additionally, a microscopic examination did not show any abnormality. Objective: secondary objective. GRADE: Low. | |||||
| Turnbull et al. (1983) [157] | VPA | Clinical trial | 54 | The study reported four cases of alopecia. One patient developed alopecia with plasma VPA levels of 118 and 109 p,g/mL. Objective: secondary objective. GRADE: Low. | |||||
| Spitz et al. (1991) [158] | VPA | Clinical trial | 71 | The VPA-induced alopecia was transient. Objective: secondary objective. GRADE: Low. | |||||
| Beydoun et al. (1997) [34] | VPA | Clinical trial | 143 | High doses (27 individuals) when compared to lower doses (two individuals) of VPA, were more frequently associated with alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Macritchie et al. (2001) [159] | VPA | Review | NA | The VPA group had significantly more patients suffering from alopecia (RRI 143%; RR 2.43; 95% C.I. 1.05 to 5.65) than the placebo group. Objective: secondary objective. GRADE: Low. | |||||
| Schulpis et al. (2001) [160] | VPA | Clinical trial | 75 | VPA impaired liver mitochondrial function, resulting in low biotinidase activity. Biotin supplementation could restore some of the side effects of the drug. Objective: secondary objective. GRADE: Low. | |||||
| Ebrahimi et al. (2005) [161] | VPA | Observational study | 211 | Three cases were female, and three were male. The estimated frequency of hair loss was 3.5% of the VPA user population, which is lower than previously reported frequencies (6–12%). The drug therapy duration was 3 months. Objective: primary objective. GRADE: Moderate. | |||||
| Kocer et al. (2005) [162] | VPA | Observational study | 62 | The authors assessed the skin findings associated with the long-term use of ASMs. Alopecia was the only skin condition related to ASM usage, and it was seen in four patients (6.5%) using VPA. Objective: primary objective. GRADE: Moderate. | |||||
| Joffe et al. (2006) [163] | VPA | Randomized controlled trial | 86 | Among subjects who developed oligomenorrhea while taking VPA, 22% had male-pattern alopecia. Objective: secondary objective. GRADE: Low. | |||||
| McCabe et al. (2006) [164] | VPA | Clinical trial | 41 | Assessment of efficacy and safety of conversion from delayed-release VPA to extended-release VPA. The drug therapy duration was 3 months. Objective: secondary objective. GRADE: Low. | |||||
| Jedrzejczak et al. (2007) [165] | VPA | Clinical trial | 1984 | The incidence of VPA-induced alopecia was 2.2%. Seven individuals discontinued VPA due to alopecia. Objective: secondary objective. GRADE: Low. | |||||
| Yilmaz et al. (2009) [38] | VPA | Observational study | 32 | Findings suggest hair loss can be attributed to serum zinc levels and serum biotinidase activity depletion within the first 3 months. After 6 months, biotinidase activity returns to normal, but serum zinc levels stay depleted. The drug therapy duration was 3–6 months. Objective: primary objective. GRADE: Moderate. | |||||
| Castro-Gago et al. (2011) [166] | VPA, CBZ | Observational study | 20 | Hair loss was observed in three patients treated with VPA, with normal serum levels of biotin, zinc, and biotinidase activity, and the alopecia disappeared with the oral administration of biotin (10 mg/d) within three months. Objective: secondary objective. GRADE: Low. | |||||
| Han et al. (2015) [167] | VPA | Observational study | 561 | A partial recovery of hair growth was observed in all the individuals. Objective: primary objective. GRADE: low. | |||||
| Kompally et al. (2015) [168] | VPA | Observational study | 70 | VPA-induced alopecia was transient. Objective: primary objective. GRADE: Low. | |||||
| Yamak et al. (2015) [169] | VPA | Observational study | 72 | VPA-induced alopecia was mild in two cases, moderate in six cases, and severe in four cases. The drug therapy duration was 1 month. Objective: secondary objective. GRADE: Low. | |||||
| Druschky et al. (2018) [170] | VPA, LTG | Observational study | 47,613 | VPA: 16 cases; LTG: one case. Objective: primary objective. GRADE: Moderate. | |||||
| Kakunje et al. (2018) [49] | VPA | Review | NA | Hair curling can occur in about 3.5% of individuals. Topical VPA can induce hair growth. Starting with a low dose and with a progressive dose increase, VPA might counteract alopecia. The drug therapy duration was 25–90 days. The dose investigated was >800 mg/day. Objective: primary objective. GRADE: Moderate. | |||||
| Wang et al. (2019) [35] | VPA | Systematic review | 25 | Patients taking a lower dose (≤750 mg/d) had a similar risk of developing alopecia to patients administered a higher dose (>750 mg/d). Patients taking VPA for longer than 6 months did not increase the risk of alopecia compared to taking VPA for less than 6 months. The dose investigated was 400–2099 mg/day. Objective: primary objective. GRADE: High. | |||||
| Pruccoli et al. (2023) [171] | VPA | Observational study | NA | One patient developed alopecia due to VPA use. Objective: secondary objective. GRADE: low. | |||||
| Antiseizure Medication | Pubmed (n: 180) i | Literature (n: 1656) ii | Incidence, Reference |
|---|---|---|---|
| Valproate | 70 | 983 | 2.2%, Jedrzejczak et al. (2007) [165] 3.5%, Ebrahimi et al. (2005) [161] 12%, Mattson et al. (1992) [52] |
| Carbamazepine | 31 | 225 | 0.3%, Chen et al. (2015) [4] 6%, Mattson et al. (1992) [52] |
| Phenytoin | 20 | 4 | 0.3%, Chen et al. (2015) [4] |
| Phenobarbital | 16 | 5 | 1.2%, Herranz et al. (1988) [74] |
| Lamotrigine | 10 | 355 | 0.8%, Chen et al. (2015) [4] |
| Levetiracetam | 8 | 14 | 0.4%, Chen et al. (2015) [4] |
| Gabapentin | 6 | 5 | 2.3%, Collins et al. (2019) [142] |
| Topiramate | 5 | 13 | 1.7%, Chen et al. (2015) [4] 3.7%, Krymchantowski et al. (2004) [149] |
| Oxcarbazepine | 4 | 0 | NA |
| Clobazam | 2 | 2 | 0.23%, Satishchandra et al. (2022) [134] |
| Felbamate | 2 | 0 | NA |
| Vigabatrin | 2 | 6 | 0.9%, Turanli et al. (2006) [150] 9.6%, Lampl et al. (1996) [96] |
| Pregabalin | 1 | 4 | 0.07%, Harmark et al. (2011) [80] 0.7%, Chen et al. (2015) [4] |
| Primidone | 1 | 1 | 1.5%, Herranz et al. (1988) [74] |
| Trimethadione | 1 | 2 | NA |
| Zonisamide | 1 | 2 | NA |
| Brivaracetam | 0 | 2 | 0.08%, Ryvlin et al. (2022) [125] 0.9%, Hirsch et al. (2018) [124] |
| Cenobamate | 0 | 18 | 0.28%, Klein et al. (2022) [135] 1.11%, Sperling et al. (2020) [136] |
| Eslicarbazepine | 0 | 3 | 1.92%, Chaves et al. (2017) [138] 1.93%, Hixson et al. (2021) [140] |
| Lacosamide | 0 | 7 | 1.22%, Runge et al. (2015) [143] |
| Perampanel | 0 | 2 | 0.04%, Rohracher et al. (2018) [88] 0.21%, Villanueva et al. (2016) [89] |
| Rufinamide | 0 | 2 | 1.31%, Tan et al. (2017) [148] 1.66%, Kluger et al. (2009) [147] |
| Tiagabine | 0 | 1 | 1%, Mercke et al. (2000) [8] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitton Rissardo, J.; Fornari Caprara, A.L.; Casares, M.; Skinner, H.J.; Hamid, U. Antiseizure Medication-Induced Alopecia: A Literature Review. Medicines 2023, 10, 35. https://doi.org/10.3390/medicines10060035
Pitton Rissardo J, Fornari Caprara AL, Casares M, Skinner HJ, Hamid U. Antiseizure Medication-Induced Alopecia: A Literature Review. Medicines. 2023; 10(6):35. https://doi.org/10.3390/medicines10060035
Chicago/Turabian StylePitton Rissardo, Jamir, Ana Leticia Fornari Caprara, Maritsa Casares, Holly J. Skinner, and Umair Hamid. 2023. "Antiseizure Medication-Induced Alopecia: A Literature Review" Medicines 10, no. 6: 35. https://doi.org/10.3390/medicines10060035