

Association of Malnutrition and High Bleeding Risk with Long-Term Prognosis in Patients with Acute Coronary Syndrome following Percutaneous Coronary Intervention
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
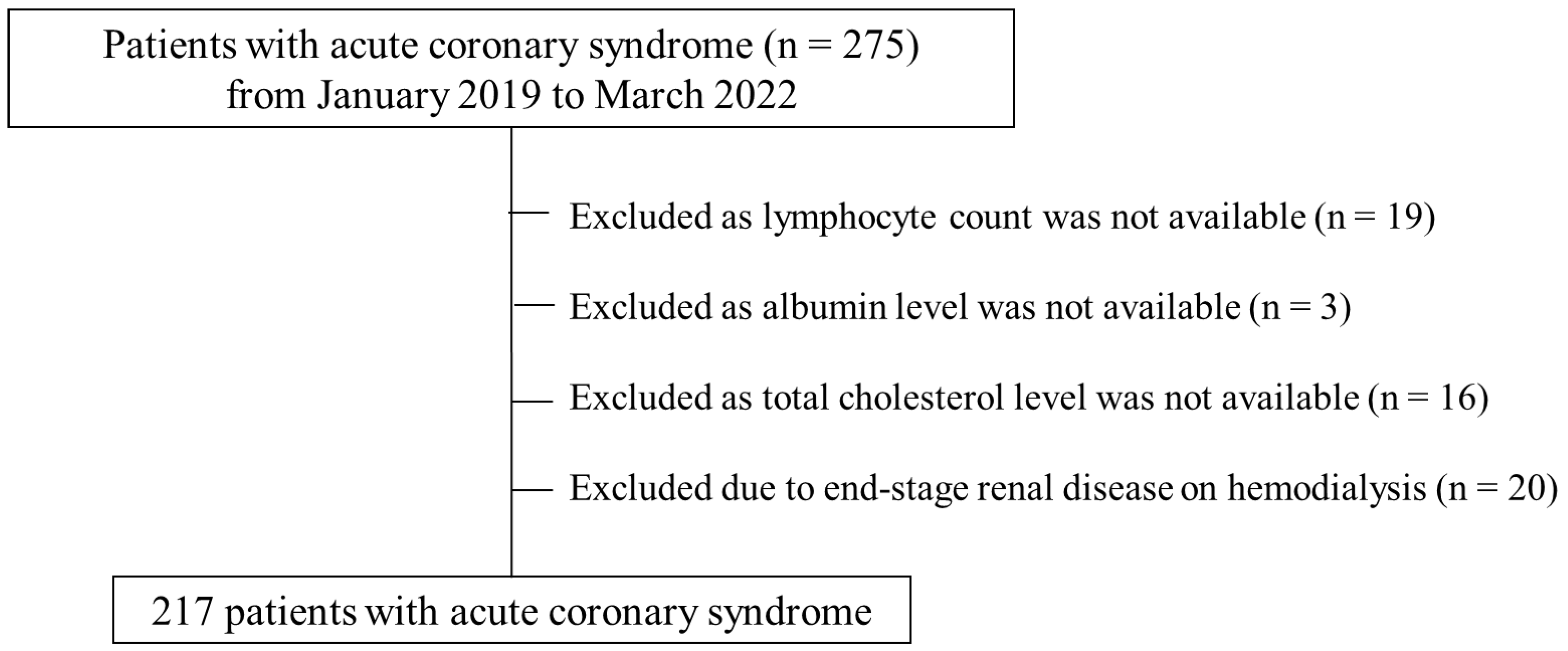
2.1. Patient Population
2.2. Percutaneous Coronary Intervention
2.3. Clinical Assessments
2.4. Nutritional Indices
2.5. Japanese Version of the ARC-HBR Criteria
2.6. Primary and Secondary Outcomes and Exploratory Analysis
2.7. Statistical Analysis
3. Results
3.1. Baseline and Procedural Characteristics
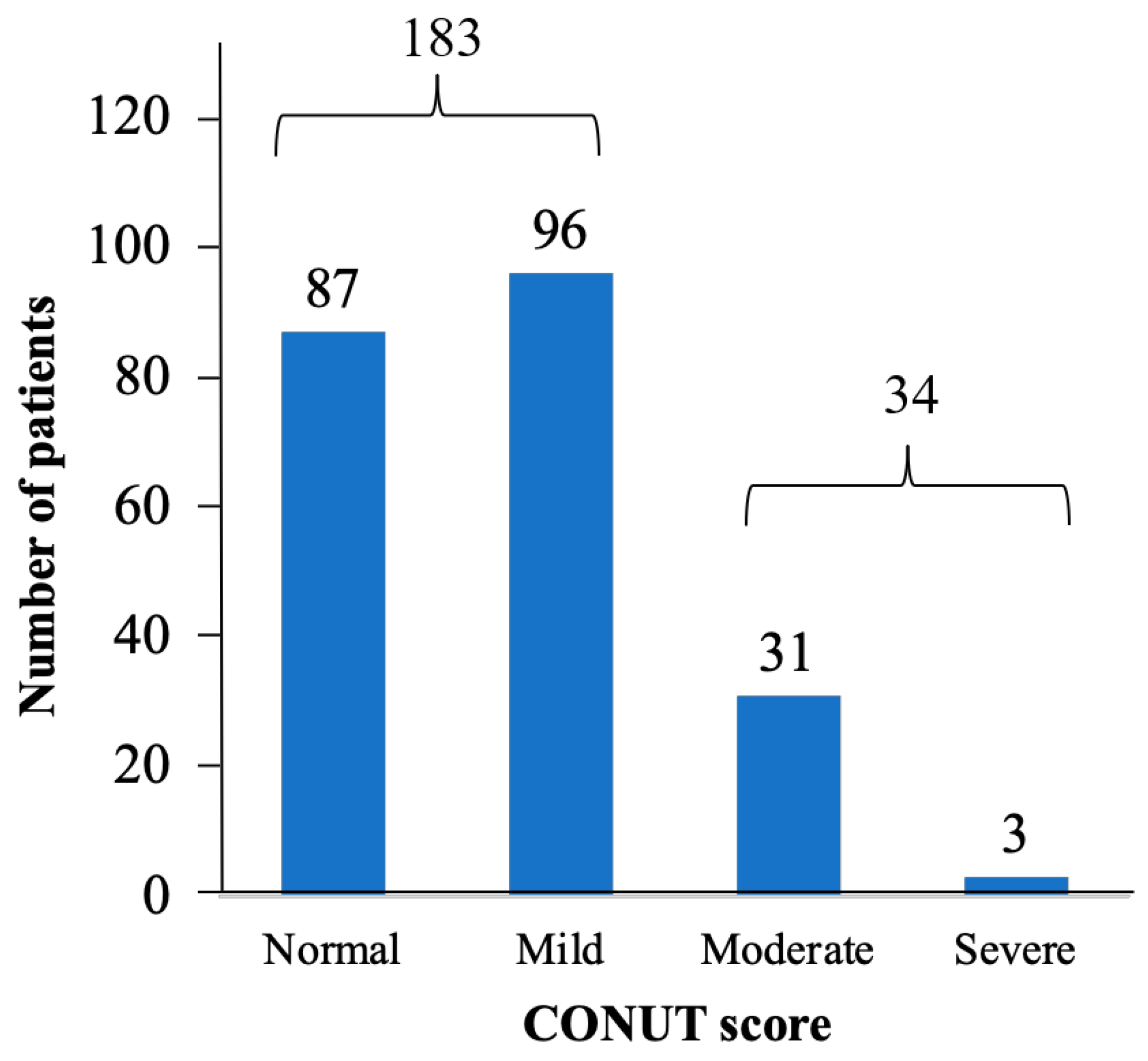
3.2. Nutritional Status of Patients with ACS
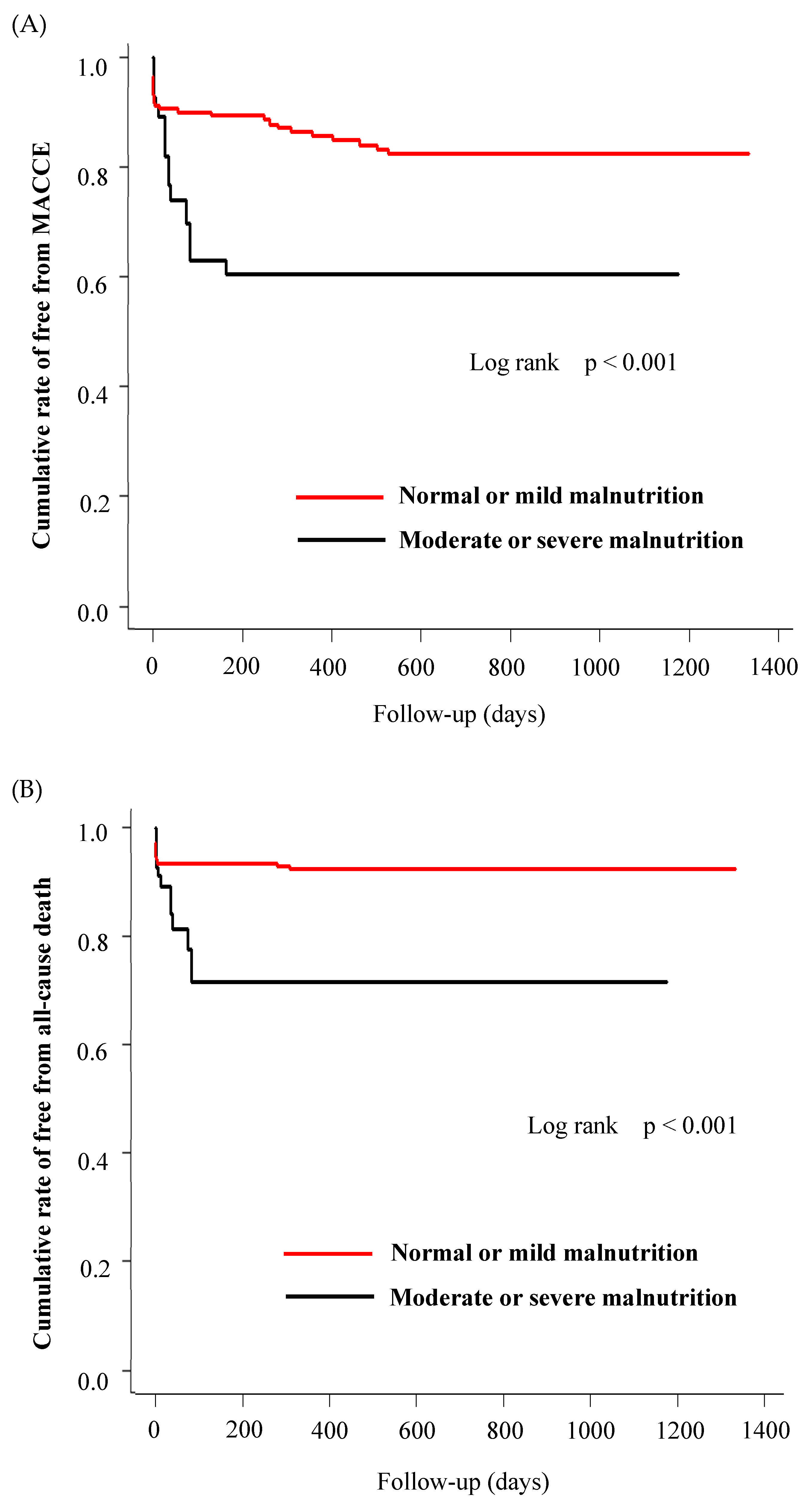
3.3. Long-Term Clinical Outcomes
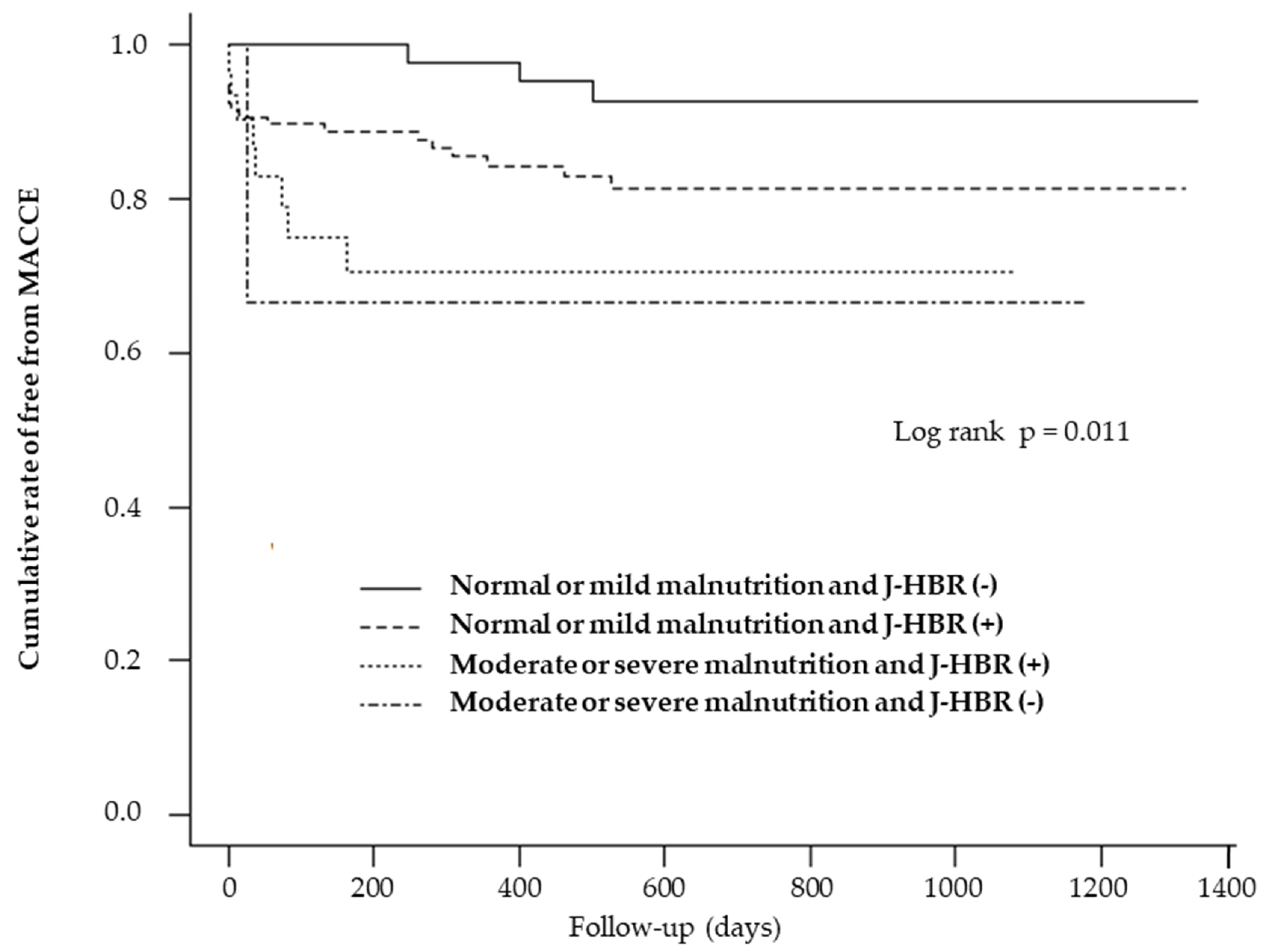
3.4. Association between Nutrition Status and J-HBR Score
4. Discussion
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomson, K.H.; Rice, S.; Arisa, O.; Johnson, E.; Tanner, L.; Marshall, C.; Sotire, T.; Richmond, C.; O’Keefe, H.; Mohammed, W.; et al. Effectiveness and cost-effectiveness of oral nutritional supplements in frail older people who are malnourished or at risk of malnutrition: A systematic review and meta-analysis. Lancet Health Longev. 2022, 3, e654–e666. [Google Scholar] [CrossRef] [PubMed]
- Narumi, T.; Arimoto, T.; Funayama, A.; Kadowaki, S.; Otaki, Y.; Nishiyama, S.; Takahashi, H.; Shishido, T.; Miyashita, T.; Miyamoto, T.; et al. Prognostic importance of objective nutritional indexes in patients with chronic heart failure. J. Cardiol. 2013, 62, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Hamana, T.; Fujimoto, W.; Konishi, A.; Takemoto, M.; Kuroda, K.; Yamashita, S.; Imanishi, J.; Iwasaki, M.; Todoroki, T.; Okuda, M.; et al. Differences in prognostic factors among patients hospitalized for heart failure according to the age category: From the KUNIUMI Registry Acute Cohort. Intern. Med. 2022, 61, 3171–3180. [Google Scholar] [CrossRef]
- Yıldırım, A.; Kucukosmanoglu, M.; Koyunsever, N.Y.; Cekici, Y.; Belibagli, M.C.; Kılıc, S. Combined effects of nutritional status on long-term mortality in patients with non-ST segment elevation myocardial infarction undergoing percutaneous coronary intervention. Rev. Da Assoc. Médica Bras. 2021, 67, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Park, K.W.; Palmerini, T.; Stone, G.W.; Lee, M.S.; Colombo, A.; Chieffo, A.; Feres, F.; Abizaid, A.; Bhatt, D.L.; et al. Racial differences in ischaemia/bleeding risk trade-off during anti-platelet therapy: Individual patient level landmark meta-analysis from seven RCTs. Thromb. Haemost. 2018, 119, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.-H.; Bhatt, D.L.; Shao, M.; Hankey, G.J.; Easton, J.D.; Fox, K.A.; Topol, E.J. Ethnic variation in adverse cardiovascular outcomes and bleeding complications in the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance (CHARISMA) study. Am. Heart J. 2009, 157, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, S.; Miyata, H.; Ueda, I.; Masoudi, F.A.; Peterson, E.D.; Maekawa, Y.; Kawamura, A.; Fukuda, K.; Roe, M.T.; Rumsfeld, J.S.; et al. An international comparison of patients undergoing percutaneous coronary intervention: A collaborative study of the National Cardiovascular Data Registry (NCDR) and Japan Cardiovascular Database-Keio interhospital Cardiovascular Studies (JCD-KiCS). Am. Heart J. 2015, 170, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Park, D.-W.; Kwon, O.; Jang, J.-S.; Yun, S.-C.; Park, H.; Kang, D.-Y.; Ahn, J.-M.; Lee, P.H.; Lee, S.-W.; Park, S.-W.; et al. Clinically significant bleeding with ticagrelor versus clopidogrel in Korean patients with acute coronary syndromes intended for invasive management: A randomized clinical trial. Circulation 2019, 140, 1865–1877. [Google Scholar] [CrossRef]
- Nakamura, M.; Kimura, K.; Kimura, T.; Ishihara, M.; Otsuka, F.; Kozuma, K.; Kosuge, M.; Shinke, T.; Nakagawa, Y.; Natsuaki, M.; et al. JCS 2020 guideline focused update on antithrombotic therapy in patients with coronary artery disease. Circ. J. 2020, 84, 831–865. [Google Scholar] [CrossRef]
- Nakamura, M.; Kadota, K.; Nakagawa, Y.; Tanabe, K.; Ito, Y.; Amano, T.; Maekawa, Y.; Takahashi, A.; Shiode, N.; Otsuka, Y.; et al. Ultrathin, biodegradable-polymer sirolimus-eluting stent vs thin, durable-polymer everolimus-eluting stent. JACC Cardiovasc. Interv. 2022, 15, 1324–1334. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.P.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Chen, S.-C.; Yang, Y.-L.; Wu, C.-H.; Huang, S.-S.; Chan, W.L.; Lin, S.-J.; Chou, C.-Y.; Chen, J.-W.; Pan, J.-P.; Charng, M.-J.; et al. Association between preoperative nutritional status and clinical outcomes of patients with coronary artery disease undergoing percutaneous coronary intervention. Nutrients 2020, 12, 1295. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.-T.; Shao, Q.-Y.; Li, Q.-X.; Yang, Z.-Q.; Han, K.-N.; Liang, J.; Shen, H.; Liu, X.-L.; Zhou, Y.-J.; Wang, Z.-J. Nutritional risk index improves the GRACE score prediction of clinical outcomes in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Front. Cardiovasc. Med. 2021, 8, 773200. [Google Scholar] [CrossRef] [PubMed]
- Zengin, A.; Karataş, M.B.; Çanga, Y.; Durmuş, G.; Güzelburç, Ö.; Durak, F.; Emre, A.; Turkey, I. Prognostic performance of Controlling Nutritional Status score in patients with ST segment elevation myocardial infarction treated with primary percutaneous coronary intervention. Anatol. J. Cardiol. 2022, 26, 23–28. [Google Scholar] [CrossRef]
- Inohara, T.; Kohsaka, S.; Yamaji, K.; Iida, O.; Shinke, T.; Sakakura, K.; Ishii, H.; Amano, T.; Ikari, Y. Use of thrombus aspiration for patients with acute coronary syndrome: Insights from the nationwide J-PCI Registry. J. Am. Heart Assoc. 2022, 11, e025728. [Google Scholar] [CrossRef]
- Shoji, S.; Kohsaka, S.; Kumamaru, H.; Yamaji, K.; Nishimura, S.; Ishii, H.; Amano, T.; Fushimi, K.; Miyata, H.; Ikari, Y. Cost reduction associated with transradial access in percutaneous coronary intervention: A report from a Japanese nationwide registry. Lancet Reg. Health West. Pac. 2022, 28, 100555. [Google Scholar] [CrossRef] [PubMed]
- Natsuaki, M.; Morimoto, T.; Shiomi, H.; Ehara, N.; Taniguchi, R.; Tamura, T.; Tada, T.; Suwa, S.; Kaneda, K.; Watanabe, H.; et al. Application of the modified high bleeding risk criteria for Japanese patients in an all-comers registry of percutaneous coronary intervention: From the CREDO-Kyoto Registry Cohort-3. Circ. J. 2021, 85, 769–781. [Google Scholar] [CrossRef]
- Lu, C.; Chen, Q.; Fei, L.; Wang, J.; Wang, C.; Yu, L. Prognostic impact of the controlling nutritional status score in patients with hematologic malignancies: A systematic review and meta-analysis. Front. Immunol. 2022, 13, 952802. [Google Scholar] [CrossRef]
- Eckart, A.; Struja, T.; Kutz, A.; Baumgartner, A.; Baumgartner, T.; Zurfluh, S.; Neeser, O.; Huber, A.; Stanga, Z.; Mueller, B.; et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: A prospective study. Am. J. Med. 2020, 133, 713–722.e7. [Google Scholar] [CrossRef]
- Akboga, M.K.; Inanc, I.H.; Sabanoglu, C.; Akdi, A.; Yakut, I.; Yuksekkaya, B.; Nurkoc, S.; Yalcin, R. Systemic immune-inflammation index and c-reactive protein/albumin ratio could predict acute stent thrombosis and high SYNTAX score in acute coronary syndrome. Angiology 2022, 74, 693–701. [Google Scholar] [CrossRef]
- Nakanishi, N.; Kaikita, K.; Ishii, M.; Kuyama, N.; Tabata, N.; Ito, M.; Yamanaga, K.; Fujisue, K.; Hoshiyama, T.; Kanazawa, H.; et al. Malnutrition-associated high bleeding risk with low thrombogenicity in patients undergoing percutaneous coronary intervention. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Agnoletti, D.; Arcaro, G.; Scaturro, G.; Turcato, E.; Grison, E.; Ferrari, E.; Bonapace, S.; Targher, G.; Valbusa, F. Controlling nutritional status score predicts 2-year outcomes in elderly patients admitted for acute heart failure. Intern. Emerg. Med. 2023, 18, 1031–1039. [Google Scholar] [CrossRef]
- Zhao, J.; Xie, W.; Ye, S.; Zhang, S.; Shi, W.; Cui, M.; Wang, L. The clinical value of the Controlling Nutritional Status score for predicting prognosis in systolic heart failure cases in the vulnerable phase. Front. Nutr. 2023, 10, 1084107. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wang, S.; Sun, X.; Han, Y.; Zhang, L.; Liu, M. Application of food exchange portion method in home-based nutritional intervention for elderly patients with chronic heart failure. BMC Cardiovasc. Disord. 2023, 23, 80. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, M.; Bozkurt, B.; Panjrath, G.; Aggarwal, B.; Ostfeld, R.J.; Barnard, N.D.; Gaggin, H.; Freeman, A.M.; Allen, K.; Madan, S.; et al. Lifestyle Modifications for Preventing and Treating Heart Failure. J. Am. Coll. Cardiol. 2018, 72, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Ikoma, T.; Saito, H.; Oka, T.; Maekawa, Y. The Importance of Objective Nutritional Indexes in Heart Failure Patients. J. Am. Coll. Cardiol. 2021, 78, 855–856. [Google Scholar] [CrossRef] [PubMed]
- Prokopidis, K.; Isanejad, M.; Akpan, A.; Stefil, M.; Tajik, B.; Giannos, P.; Venturelli, M.; Sankaranarayanan, R. Exercise and nutritional interventions on sarcopenia and frailty in heart failure: A narrative review of systematic reviews and meta-analyses. ESC Heart Fail. 2022, 9, 2787–2799. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, M. Nutritional Management of Sarcopenia and Frailty—Shift from Metabolic Syndrome to Frailty. J. Nutr. Sci. Vitaminol. 2022, 68, S67–S69. [Google Scholar] [CrossRef]
- Kanda, D.; Ikeda, Y.; Takumi, T.; Tokushige, A.; Sonoda, T.; Arikawa, R.; Anzaki, K.; Kosedo, I.; Ohishi, M. Impact of nutritional status on prognosis in acute myocardial infarction patients undergoing percutaneous coronary intervention. BMC Cardiovasc. Disord. 2022, 22, 3. [Google Scholar] [CrossRef]
- Roubín, S.R.; Abu Assi, E.; Fernandez, M.C.; Pardal, C.B.; Castro, A.L.; Parada, J.A.; Pérez, D.D.; Prieto, S.B.; Rossello, X.; Ibanez, B.; et al. Prevalence and Prognostic Significance of Malnutrition in Patients with Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2020, 76, 828–840. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Normal or Mild Malnutrition (n = 183) | Moderate or Severe Malnutrition (n = 34) | SMD | p-Value |
|---|---|---|---|---|
| Age, years | 71.6 (11.1) | 72.3 (9.9) | 0.065 | 0.757 |
| Male | 79.2 | 75.3 | 0.093 | 0.650 |
| BMI, kg/m2 | 24.3 (4.3) | 22.6 (4.4) | 0.374 | 0.113 |
| Hypertension | 66.9 | 55.9 | 0.228 | 0.307 |
| DM | 43.4 | 43.0 | 0.029 | 0.892 |
| Dyslipidemia | 66.7 | 51.2 | 0.320 | 0.148 |
| CKD | 34.2 | 33.3 | 0.018 | 0.926 |
| Smoking | 65.4 | 49.0 | 0.337 | 0.130 |
| Past history of HF | 12.1 | 10.6 | 0.047 | 0.779 |
| Family history of CAD | 2.9 | 1.5 | 0.097 | 0.532 |
| Previous MI | 17.4 | 27.3 | 0.239 | 0.271 |
| Previous PCI | 28.1 | 30.1 | 0.045 | 0.841 |
| Previous AF/AFL | 12.5 | 23.7 | 0.295 | 0.166 |
| Previous PAD | 10.6 | 13.1 | 0.075 | 0.709 |
| CONUT | 1.74 (1.29) | 5.94 (1.25) | 3.293 | <0.001 |
| J-HBR (+) | 66.6 | 83.0 | 0.384 | 0.168 |
| ACS classification | ||||
| STEMI | 56.1 | 67.2 | 0.231 | 0.283 |
| NSTEMI | 17.9 | 14.8 | 0.085 | 0.652 |
| UA | 26.0 | 18.0 | 0.195 | 0.390 |
| Access site | ||||
| Radial approach | 90.6 | 84.7 | 0.180 | 0.374 |
| Medications | ||||
| Aspirin | 93.2 | 83.4 | 0.311 | 0.121 |
| Clopidogrel | 24.8 | 32.1 | 0.162 | 0.432 |
| Prasugrel | 70.5 | 54.6 | 0.334 | 0.127 |
| ACE-inhibitor/ARBs | 70.2 | 36.0 | 0.730 | 0.001 |
| β blockers | 67.5 | 55.6 | 0.247 | 0.270 |
| Statin | 95.8 | 81.8 | 0.456 | 0.006 |
| Ca channel blockers | 29.4 | 10.2 | 0.495 | 0.012 |
| DOAC | 9.2 | 17.9 | 0.254 | 0.215 |
| Warfarin | 4.5 | 1.3 | 0.193 | 0.211 |
| Echocardiographic data | ||||
| LVEF, % | 49.6 (12.4) | 44.5 (14.3) | 0.379 | 0.160 |
| Laboratory data | ||||
| White blood cell count, /μl | 7809.7 (2837.6) | 8176.1 (3094.4) | 0.123 | 0.566 |
| Total lymphocyte count, /μl | 1707.8 (732.8) | 1146.1 (775.6) | 0.744 | 0.003 |
| Triglyceride, mg/dL | 131.0 (98.8) | 78.1 (57.4) | 0.655 | <0.001 |
| Total cholesterol, mg/dL | 174.3 (44.5) | 136.6 (45.9) | 0.834 | <0.001 |
| HDL-C, mg/dL | 45.0 (12.2) | 38.1 (15.1) | 0.503 | 0.045 |
| LDL-C, mg/dL | 102.6 (37.4) | 78.0 (30.5) | 0.720 | <0.001 |
| Albumin, mg/dL | 4.0 (0.4) | 3.1 (0.4) | 2.136 | <0.001 |
| Total protein, mg/dL | 7.1 (4.5) | 6.0 (0.9) | 0.349 | 0.002 |
| Procedural Characteristics | Normal or Mild Malnutrition (n = 183) | Moderate or Severe Malnutrition (n = 34) | p-Value |
|---|---|---|---|
| TIMI grade 3 | 94.3 | 75.4 | 0.002 |
| Complication | |||
| Coronary perforation, | 0 | 0 | 1 |
| BARC 3a or 5 Bleeding | 9.9 | 19.7 | 0.192 |
| Clinical Outcomes | Normal or Mild Malnutrition (n = 183) | Moderate or Severe Malnutrition (n = 34) | p-Value |
|---|---|---|---|
| MACCE | 12.1 | 37.1 | 0.003 |
| All-cause death | 4.8 | 28.2 | <0.001 |
| Myocardial infarction | 0.5 | 0 | 0.668 |
| Stroke | 1.8 | 6.7 | 0.219 |
| TVF | 4.5 | 2.1 | 0.475 |
| Stent thrombosis | 1.0 | 0 | 0.545 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kataoka, H.; Suzuki, S.; Suzuki, Y.; Sato, R.; Sano, M.; Mogi, S.; Sakamoto, A.; Suwa, K.; Naruse, Y.; Ohtani, H.; et al. Association of Malnutrition and High Bleeding Risk with Long-Term Prognosis in Patients with Acute Coronary Syndrome following Percutaneous Coronary Intervention. Medicines 2023, 10, 62. https://doi.org/10.3390/medicines10120062
Kataoka H, Suzuki S, Suzuki Y, Sato R, Sano M, Mogi S, Sakamoto A, Suwa K, Naruse Y, Ohtani H, et al. Association of Malnutrition and High Bleeding Risk with Long-Term Prognosis in Patients with Acute Coronary Syndrome following Percutaneous Coronary Intervention. Medicines. 2023; 10(12):62. https://doi.org/10.3390/medicines10120062
Chicago/Turabian StyleKataoka, Hiromitsu, Sayumi Suzuki, Yuichi Suzuki, Ryota Sato, Makoto Sano, Satoshi Mogi, Atsushi Sakamoto, Kenichiro Suwa, Yoshihisa Naruse, Hayato Ohtani, and et al. 2023. "Association of Malnutrition and High Bleeding Risk with Long-Term Prognosis in Patients with Acute Coronary Syndrome following Percutaneous Coronary Intervention" Medicines 10, no. 12: 62. https://doi.org/10.3390/medicines10120062