
Prenatal Cadmium Exposure and Maternal Sex Steroid Hormone Concentrations across Pregnancy
 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Overview and Population
2.2. Exposure: Urinary Cadmium
2.3. Outcome: Maternal Sex Steroid Hormones
2.4. Covariates
2.5. Statistical Analysis
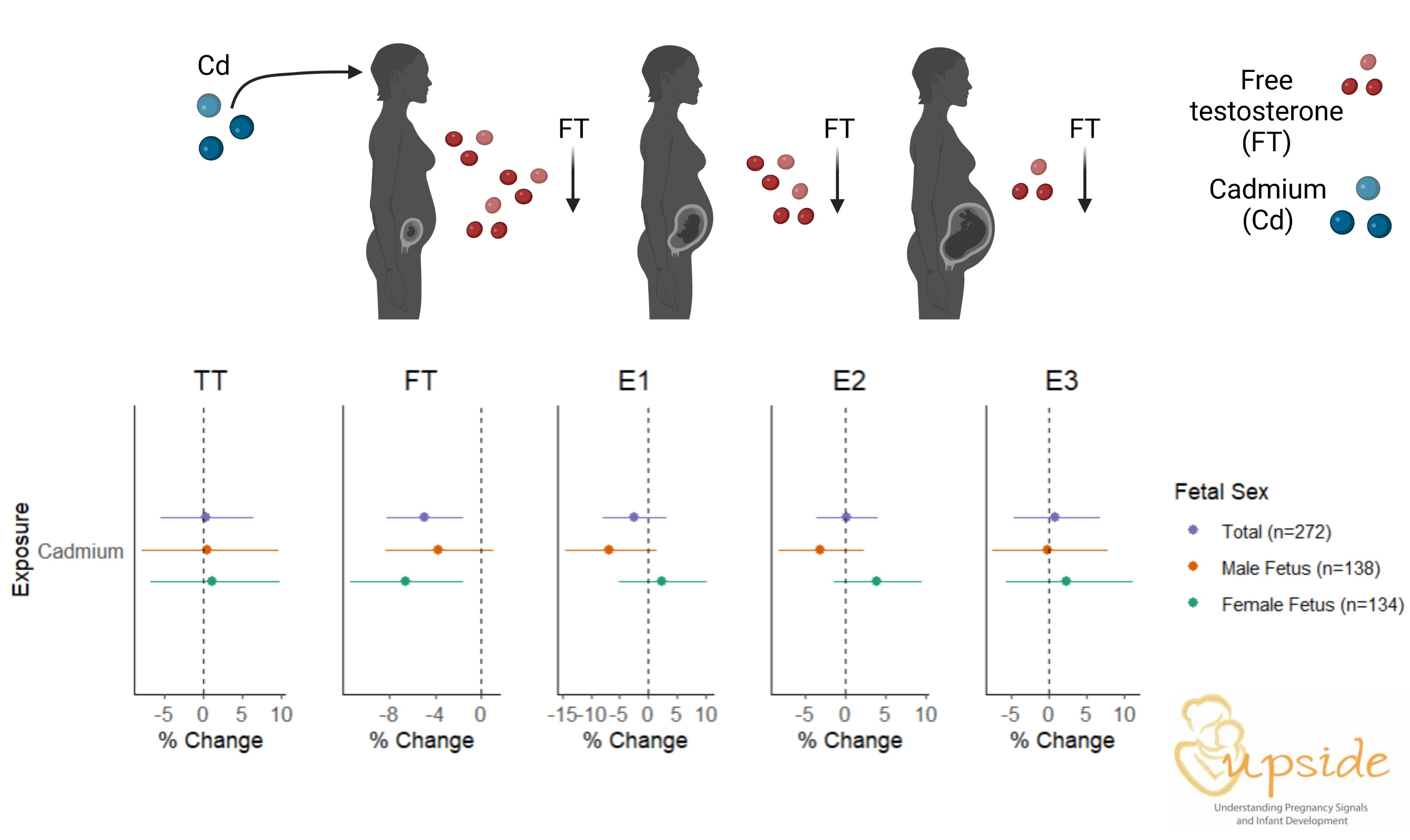
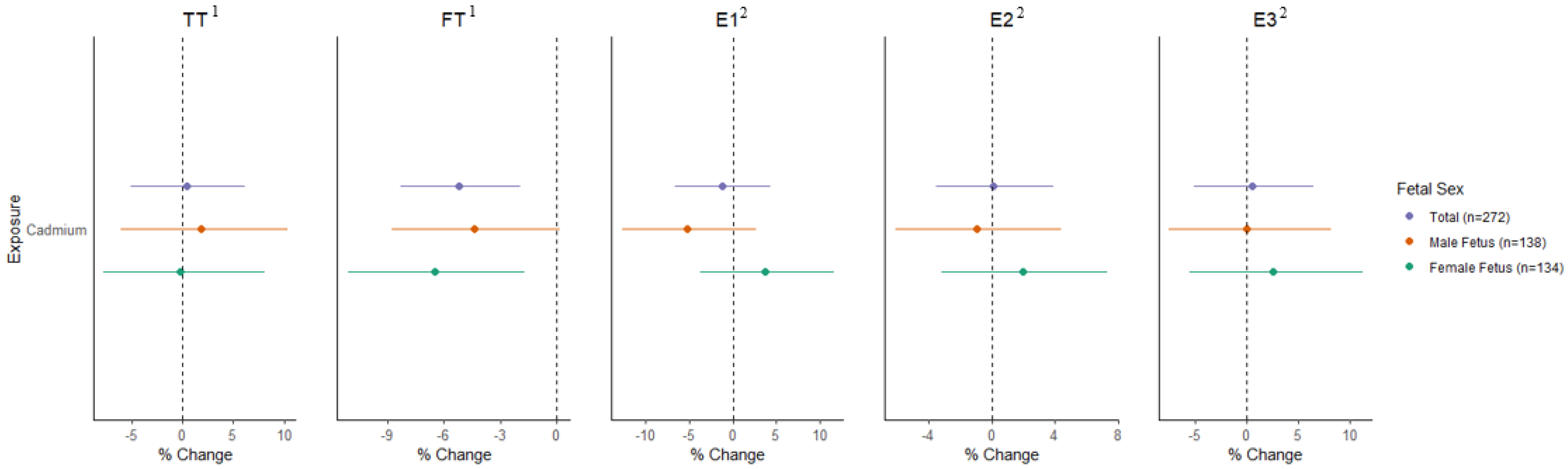
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faroon, O.; Ashizawa, A.; Wright, S.; Tucker, P.; Jenkins, K.; Ingerman, L.; Rudisill, C. Agency for Toxic Substances and Disease Registry (ATSDR). In Toxicological Profile for Cadmium; Department of Health and Human Services, Public Health Service: Gosford, Australia, 2012. [Google Scholar]
- Yang, G.; Sun, T.; Han, Y.-Y.; Rosser, F.; Forno, E.; Chen, W.; Celedon, J. Serum Cadmium and Lead, Current Wheeze, and Lung Function in a Nationwide Study of Adults in the United States. J. Allergy Clin. Immunol. Pract. 2019, 7, 2653–2660.e3. [Google Scholar] [CrossRef] [PubMed]
- Tellez-Plaza, M.; Jones, M.R.; Dominguez-Lucas, A.; Guallar, E.; Navas-Acien, A. Cadmium Exposure and Clinical Cardiovascular Disease: A Systematic Review. Curr. Atheroscler. Rep. 2013, 15, 256. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.-F.; Hsu, P.-C.; Kung, C.-T.; Lee, C.-T.; You, H.-L.; Huang, W.-T.; Li, S.-H.; Cheng, F.-J.; Wang, C.-C.; Lee, W.-C. The Risk Factors of Blood Cadmium Elevation in Chronic Kidney Disease. Int. J. Environ. Res. Public Health 2021, 18, 12337. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.V.; Lewin, M.; Ragin-Wilson, A.; Jones, R.; Jarrett, J.M.; Wallon, K.; Ward, C.; Hilliard, N.; Irvin-Barnwell, E. Characterization of trace elements exposure in pregnant women in the United States, NHANES 1999–2016. Environ. Res. 2020, 183, 109208. [Google Scholar] [CrossRef]
- Amegah, A.K.; Sewor, C.; Jaakkola, J.J.K. Cadmium exposure and risk of adverse pregnancy and birth outcomes: A systematic review and dose–response meta-analysis of cohort and cohort-based case–control studies. J. Expo. Sci. Environ. Epidemiol. 2021, 31, 299–317. [Google Scholar] [CrossRef]
- E Edwards, S.; Maxson, P.; Miranda, M.L.; Fry, R.C. Cadmium levels in a North Carolina cohort: Identifying risk factors for elevated levels during pregnancy. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 427–432. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Xia, W.; Xu, S.; Zhang, B.; Lu, B.; Huang, Z.; Zhang, H.; Jiang, Y.; Liu, W.; Peng, Y.; et al. Cadmium body burden and pregnancy-induced hypertension. Int. J. Hyg. Environ. Health 2018, 221, 246–251. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, B.; Huang, Z.; Pan, X.; Chen, X.; Hu, C.; Liu, H.; Jiang, Y.; Sun, X.; Peng, Y.; et al. Cadmium Body Burden and Gestational Diabetes Mellitus: A Prospective Study. Environ. Health Perspect. 2018, 126, 027006. [Google Scholar] [CrossRef] [Green Version]
- Masumoto, T.; Amano, H.; Otani, S.; Kamijima, M.; Yamazaki, S.; Kobayashi, Y.; Kurozawa, Y. Association between prenatal cadmium exposure and child development: The Japan Environment and Children’s study. Int. J. Hyg. Environ. Health 2022, 243, 113989. [Google Scholar] [CrossRef]
- Zeng, Q.; Zhang, W.-X.; Zheng, T.-Z.; Zhou, B.; Li, J.-X.; Zhang, B.; Xia, W.; Li, Y.-Y.; Xu, S.-Q. Prenatal and postnatal cadmium exposure and cellular immune responses among pre-school children. Environ. Int. 2020, 134, 105282. [Google Scholar] [CrossRef]
- Ritz, B.; Heinrich, J.; Wjst, M.; Wichmann, E.; Krause, C. Effect of Cadmium Body Burden on Immune Response of School Children. Arch. Environ. Health Int. J. 1998, 53, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Wier, P.J.; Miller, R.K.; Maulik, D.; di Sant’Agnese, P. Toxicity of cadmium in the perfused human placenta. Toxicol. Appl. Pharmacol. 1990, 105, 156–171. [Google Scholar] [CrossRef] [PubMed]
- Breen, J.G.; Nelson, E.; Miller, R.K. Cellular adaptation to chronic cadmium exposure: Intracellular localization of metallothionein protein in human trophoblast cells (JAr). Teratology 1995, 51, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, T.E.; Liang, C.L.; Morisset, A.-S.; Fisher, M.; Weiler, H.; Cirtiu, C.M.; Legrand, M.; Davis, K.; Ettinger, A.S.; Fraser, W.D. Maternal and fetal exposure to cadmium, lead, manganese and mercury: The MIREC study. Chemosphere 2016, 163, 270–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, A.A.; Miller, R.K. Fetal toxicity of cadmium in the rat: Maternal vs fetal injections. Teratology 1980, 22, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Jagodić, J.; Pavlović, S.; Borković-Mitić, S.; Perović, M.; Miković, Ž.; Đurđić, S.; Stojsavljević, A. Examination of trace metals and their potential transplacental transfer in pregnancy. Int. J. Mol. Sci. 2022, 23, 8078. [Google Scholar] [CrossRef]
- Martin, M.B.; Reiter, R.; Pham, T.; Avellanet, Y.R.; Camara, J.; Lahm, M.; Pentecost, E.; Pratap, K.; Gilmore, B.A.; Divekar, S.; et al. Estrogen-Like Activity of Metals in Mcf-7 Breast Cancer Cells. Endocrinology 2003, 144, 2425–2436. [Google Scholar] [CrossRef] [Green Version]
- Stasenko, S.; Bradford, E.M.; Piasek, M.; Henson, M.C.; Varnai, V.M.; Jurasović, J.; Kušec, V. Metals in human placenta: Focus on the effects of cadmium on steroid hormones and leptin. J. Appl. Toxicol. 2010, 30, 242–253. [Google Scholar] [CrossRef]
- Shimada, H.; Hashiguchi, T.; Yasutake, A.; Waalkes, M.P.; Imamura, Y. Sexual dimorphism of cadmium-induced toxicity in rats: Involvement of sex hormones. Arch. Toxicol. 2012, 86, 1475–1480. [Google Scholar] [CrossRef]
- Kumar, S.; Gordon, G.H.; Abbott, D.H.; Mishra, J.S. Androgens in maternal vascular and placental function: Implications for preeclampsia pathogenesis. Reproduction 2018, 156, R155–R167. [Google Scholar] [CrossRef] [Green Version]
- Noyola-Martínez, N.; Halhali, A.; Barrera, D. Steroid hormones and pregnancy. Gynecol. Endocrinol. 2019, 35, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Sferruzzi-Perri, A.N.; Vaughan, O.R.; Forhead, A.; Fowden, A.L. Hormonal and nutritional drivers of intrauterine growth. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 298–309. [Google Scholar] [CrossRef]
- Rivera-Núñez, Z.; Ashrap, P.; Barrett, E.S.; Watkins, D.J.; Cathey, A.L.; Vélez-Vega, C.M.; Rosario, Z.; Cordero, J.F.; Alshawabkeh, A.; Meeker, J.D. Association of biomarkers of exposure to metals and metalloids with maternal hormones in pregnant women from Puerto Rico. Environ. Int. 2021, 147, 106310. [Google Scholar] [CrossRef]
- Rosner, W.; Auchus, R.J.; Azziz, R.; Sluss, P.M.; Raff, H. Position statement: Utility, Limitations, and Pitfalls in Measuring Testosterone: An Endocrine Society Position Statement. J. Clin. Endocrinol. Metab. 2007, 92, 405–413. [Google Scholar] [CrossRef]
- Rosner, W.; Hankinson, S.E.; Sluss, P.M.; Vesper, H.W.; Wierman, M.E. Challenges to the Measurement of Estradiol: An Endocrine Society Position Statement. J. Clin. Endocrinol. Metab. 2013, 98, 1376–1387. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Liu, J.; Wu, S.; Zheng, W.; Li, H.; Bao, S.; Chen, Y.; Guo, X.; Zhang, L.; Ge, R.-S. In utero single low-dose exposure of cadmium induces rat fetal Leydig cell dysfunction. Chemosphere 2018, 194, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Pollack, A.Z.; Nobles, C.J.; Sjaarda, L.A.; Zolton, J.R.; Radoc, J.G.; Schisterman, E.F.; Mumford, S.L. Associations between blood cadmium and endocrine features related to PCOS-phenotypes in healthy women of reproductive age: A prospective cohort study. Environ. Health 2021, 20, 64. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.W.; Howards, P.P.; Wactawski-Wende, J.; Schisterman, E.F. The association between cadmium, lead and mercury blood levels and reproductive hormones among healthy, premenopausal women. Hum. Reprod. 2011, 26, 2887–2895. [Google Scholar] [CrossRef] [Green Version]
- Pollack, A.Z.; Schisterman, E.F.; Goldman, L.R.; Mumford, S.L.; Albert, P.S.; Jones, R.L.; Wactawski-Wende, J. Cadmium, Lead, and Mercury in Relation to Reproductive Hormones and Anovulation in Premenopausal Women. Environ. Health Perspect. 2011, 119, 1156–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, I.; Engström, A.; Vahter, M.; Skerfving, S.; Lundh, T.; Lidfeldt, J.; Samsioe, G.; Halldin, K.; Åkesson, A. Associations between cadmium exposure and circulating levels of sex hormones in postmenopausal women. Environ. Res. 2014, 134, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Nagao, Y.; Shibuya, C.; Kashiki, Y.; Shimizu, H. Urinary Cadmium and Serum Levels of Estrogens and Androgens in Postmenopausal Japanese Women. Cancer Epidemiol. Biomark. Prev. 2005, 14, 705–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kresovich, J.K.; Argos, M.; Turyk, M.E. Associations of lead and cadmium with sex hormones in adult males. Environ. Res. 2015, 142, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Tao, C.; Li, Z.; Fan, Y.; Li, X.; Qian, H.; Yu, H.; Xu, Q.; Lu, C. Independent and combined associations of urinary heavy metals exposure and serum sex hormones among adults in NHANES 2013–2016. Environ. Pollut. 2021, 281, 117097. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wang, N.; Nie, X.; Han, B.; Li, Q.; Chen, Y.; Zhai, H.; Zhu, C.; Chen, Y.; Xia, F.; et al. Blood Cadmium Level Associates with Lower Testosterone and Sex Hormone-Binding Globulin in Chinese men: From SPECT-China Study, 2014. Biol. Trace Element Res. 2016, 171, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Ciarrocca, M.; Capozzella, A.; Tomei, F.; Tomei, G.; Caciari, T. Exposure to cadmium in male urban and rural workers and effects on FSH, LH and testosterone. Chemosphere 2013, 90, 2077–2084. [Google Scholar] [CrossRef]
- Lafuente, A. The hypothalamic–pituitary–gonadal axis is target of cadmium toxicity. An update of recent studies and potential therapeutic approaches. Food Chem. Toxicol. 2013, 59, 395–404. [Google Scholar] [CrossRef]
- Sangalang, G.B.; O’Halloran, M.J. Cadmium-induced Testicular Injury and Alterations of Androgen Synthesis in Brook Trout. Nature 1972, 240, 470–471. [Google Scholar] [CrossRef]
- Martin, M.B.; Voeller, H.J.; Gelmann, E.P.; Lu, J.; Stoica, E.-G.; Hebert, E.J.; Reiter, R.; Singh, B.; Danielsen, M.; Pentecost, E.; et al. Role of Cadmium in the Regulation of AR Gene Expression and Activity. Endocrinology 2002, 143, 263–275. [Google Scholar] [CrossRef]
- Iavicoli, I.; Fontana, L.; Bergamaschi, A. The Effects of Metals as Endocrine Disruptors. J. Toxicol. Environ. Health Part B 2009, 12, 206–223. [Google Scholar] [CrossRef]
- Huang, Y.; Zhu, J.; Li, H.; Wang, W.; Li, Y.; Yang, X.; Zheng, N.; Liu, Q.; Zhang, Q.; Zhang, W.; et al. Cadmium exposure during prenatal development causes testosterone disruption in multigeneration via SF-1 signaling in rats. Food Chem. Toxicol. 2020, 135, 110897. [Google Scholar] [CrossRef]
- Xiong, Y.-W.; Zhu, H.-L.; Nan, Y.; Cao, X.-L.; Shi, X.-T.; Yi, S.-J.; Feng, Y.-J.; Zhang, C.; Gao, L.; Chen, Y.-H.; et al. Maternal cadmium exposure during late pregnancy causes fetal growth restriction via inhibiting placental progesterone synthesis. Ecotoxicol. Environ. Saf. 2020, 187, 109879. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.; Best, M.; Brunner, J.; Ciesla, A.A.; Cunning, A.; Kapula, N.; Kautz, A.; Khoury, L.; Macomber, A.; Meng, Y.; et al. Cohort profile: Understanding Pregnancy Signals and Infant Development (UPSIDE): A pregnancy cohort study on prenatal exposure mechanisms for child health. BMJ Open 2021, 11, e044798. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Kozlosky, D.; Zhang, R.; Doherty, C.; Buckley, B.; Barrett, E.; Aleksunes, L.M. BCRP/ABCG2 Transporter Regulates Accumulation of Cadmium in Kidney Cells: Role of the Q141K Variant in Modulating Nephrotoxicity. Drug Metab. Dispos. 2021, 49, 629–637. [Google Scholar] [CrossRef]
- Boeniger, M.F.; Lowry, L.K.; Rosenberg, J. Interpretation of urine results used to assess chemical exposure with emphasis on creatinine adjustments: A review. Am. Ind. Hyg. Assoc. J. 1993, 54, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Hornung, R.W.; Reed, L.D. Estimation of Average Concentration in the Presence of Nondetectable Values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Day, D.B.; Collett, B.R.; Barrett, E.S.; Bush, N.R.; Swan, S.H.; Wang, C.; Sathyanarayana, S. Prenatal sex hormones and behavioral outcomes in children. Psychoneuroendocrinology 2020, 113, 104547. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Núñez, Z.; Kinkade, C.W.; Khoury, L.; Brunner, J.; Murphy, H.; Wang, C.; Kannan, K.; Miller, R.K.; O’Connor, T.G.; Barrett, E.S. Prenatal perfluoroalkyl substances exposure and maternal sex steroid hormones across pregnancy. Environ. Res. 2023, 220, 115233. [Google Scholar] [CrossRef]
- Sathyanarayana, S.; Butts, S.; Wang, C.; Barrett, E.; Nguyen, R.; Schwartz, S.M.; Haaland, W.; Swan, S.H. Tides the TIDES Team Early Prenatal Phthalate Exposure, Sex Steroid Hormones, and Birth Outcomes. J. Clin. Endocrinol. Metab. 2017, 102, 1870–1878. [Google Scholar] [CrossRef] [Green Version]
- Shiraishi, S.; Lee, P.W.N.; Leung, A.; Goh, V.H.H.; Swerdloff, R.S.; Wang, C. Simultaneous Measurement of Serum Testosterone and Dihydrotestosterone by Liquid Chromatography–Tandem Mass Spectrometry. Clin. Chem. 2008, 54, 1855–1863. [Google Scholar] [CrossRef] [Green Version]
- Qoubaitary, A.; Meriggiola, C.; Ng, C.M.; Lumbreras, L.; Cerpolini, S.; Pelusi, G.; Christensen, P.D.; Hull, L.; Swerdloff, R.S.; Wang, C. Pharmacokinetics of Testosterone Undecanoate Injected Alone or in Combination With Norethisterone Enanthate in Healthy Men. J. Androl. 2006, 27, 853–867. [Google Scholar] [CrossRef]
- Bulka, C.M.; Bommarito, P.A.; Fry, R.C. Predictors of toxic metal exposures among US women of reproductive age. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 597–612. [Google Scholar] [CrossRef]
- Ashrap, P.; Watkins, D.J.; Mukherjee, B.; Boss, J.; Richards, M.J.; Rosario, Z.; Vélez-Vega, C.M.; Alshawabkeh, A.; Cordero, J.F.; Meeker, J.D. Predictors of urinary and blood Metal(loid) concentrations among pregnant women in Northern Puerto Rico. Environ. Res. 2020, 183, 109178. [Google Scholar] [CrossRef]
- Gunier, R.B.; Horn-Ross, P.L.; Canchola, A.J.; Duffy, C.N.; Reynolds, P.; Hertz, A.; Garcia, E.; Rull, R.P. Determinants and Within-Person Variability of Urinary Cadmium Concentrations among Women in Northern California. Environ. Health Perspect. 2013, 121, 643–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mijal, R.S.; Holzman, C.B. Blood cadmium levels in women of childbearing age vary by race/ethnicity. Environ. Res. 2010, 110, 505–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of M, National Research Council Committee to Reexamine IOMPWG. The National Academies Collection: Reports funded by National Institutes of Health. In Weight Gain during Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academy of Sciences: Washington, DC, USA, 2009. [Google Scholar]
- ACOG. Methods for estimating the due date. Obstet. Gynecol. 2017, 129, 959–960. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, C.M.; Golding, J.; Emond, A.M. Moderate Prenatal Cadmium Exposure and Adverse Birth Outcomes: A Role for Sex-Specific Differences? Paediatr. Perinat. Epidemiol. 2016, 30, 603–611. [Google Scholar] [CrossRef] [Green Version]
- Kippler, M.; Engström, K.; Mlakar, S.J.; Bottai, M.; Ahmed, S.; Hossain, M.B.; Raqib, R.; Vahter, M.; Broberg, K. Sex-specific effects of early life cadmium exposure on DNA methylation and implications for birth weight. Epigenetics 2013, 8, 494–503. [Google Scholar] [CrossRef] [Green Version]
- Buckley, J.P.; Doherty, B.T.; Keil, A.P.; Engel, S.M. Statistical Approaches for Estimating Sex-Specific Effects in Endocrine Disruptors Research. Environ. Health Perspect. 2017, 125, 067013. [Google Scholar] [CrossRef] [Green Version]
- Romano, M.E.; Enquobahrie, D.A.; Simpson, C.; Checkoway, H.; Williams, M.A. Maternal body burden of cadmium and offspring size at birth. Environ. Res. 2016, 147, 461–468. [Google Scholar] [CrossRef] [Green Version]
- Howe, C.G.; Henn, B.C.; Eckel, S.P.; Farzan, S.F.; Grubbs, B.H.; Chavez, T.A.; Hodes, T.L.; Faham, D.; Al-Marayati, L.; Lerner, D.; et al. Prenatal Metal Mixtures and Birth Weight for Gestational Age in a Predominately Lower-Income Hispanic Pregnancy Cohort in Los Angeles. Environ. Health Perspect. 2020, 128, 117001. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Report on Human Exposure to Environmental Chemicals: Biomonitoring Data Tables for Environmental Chemicals (2011–2018); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. [Google Scholar]
- Matsumoto, A.M.; Bremner, W.J. Serum Testosterone Assays—Accuracy Matters. J. Clin. Endocrinol. Metab. 2004, 89, 520–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aker, A.M.; Ferguson, K.K.; Rosario, Z.Y.; Mukherjee, B.; Alshawabkeh, A.N.; Calafat, A.M.; Cordero, J.F.; Meeker, J.D. A repeated measures study of phenol, paraben and Triclocarban urinary biomarkers and circulating maternal hormones during gestation in the Puerto Rico PROTECT cohort. Environ. Health 2019, 18, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuijt, M.P.; Sweep, C.G.J.; van der Steen, R.; Olthaar, A.J.; Stikkelbroeck, N.M.M.L.; A Ross, H.; E van Herwaarden, A. Validity of free testosterone calculation in pregnant women. Endocr. Connect. 2019, 8, 672–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlsen, S.M.; Jacobsen, G.; Romundstad, P. Maternal testosterone levels during pregnancy are associated with offspring size at birth. Eur. J. Endocrinol. 2006, 155, 365–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisner, J.R.; Dumesic, D.A.; Kemnitz, J.W.; Abbott, D.H. Timing of prenatal androgen excess determines differential impairment in insulin secretion and action in adult female rhesus monkeys. J. Clin. Endocrinol. Metab. 2000, 85, 1206–1210. [Google Scholar] [CrossRef] [PubMed]
- Sir-Petermann, T.; Hitchsfeld, C.; Maliqueo, M.; Codner, E.; Echiburu, B.; Gazitua, R.; Cassorla, F. Birth weight in offspring of mothers with polycystic ovarian syndrome. Hum. Reprod. 2005, 20, 2122–2126. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, A.; Verdonck, L.; Kaufman, J.M. A Critical Evaluation of Simple Methods for the Estimation of Free Testosterone in Serum. J. Clin. Endocrinol. Metab. 1999, 84, 3666–3672. [Google Scholar] [CrossRef]
- Hammond, G.L.; Hogeveen, K.N.; Visser, M.; Bennink, H.J.T.C. Estetrol does not bind sex hormone binding globulin or increase its production by human HepG2 cells. Climacteric 2008, 11 (Suppl. S1), 41–46. [Google Scholar] [CrossRef]
- Mustaniemi, S.; Morin-Papunen, L.; Keikkala, E.; Öhman, H.; Surcel, H.M.; Kaaja, R.; Vääräsmäki, M. Associations of low sex hormone-binding globulin and androgen excess in early pregnancy with fasting and post-prandial hyperglycaemia, gestational diabetes, and its severity. Diabetes/Metab. Res. Rev. 2023, 39, e3599. [Google Scholar] [CrossRef]
- Tawfeek, M.A.; Alfadhli, E.M.; Alayoubi, A.M.; El-Beshbishy, H.A.; Habib, F.A. Sex hormone binding globulin as a valuable biochemical marker in predicting gestational diabetes mellitus. BMC Women’s Health 2017, 17, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, B.-K.; Sun, X.-Y.; Xian, J.; Niu, P.-P. Maternal Testosterone and Offspring Birth Weight: A Mendelian Randomization Study. J. Clin. Endocrinol. Metab. 2022, 107, 2530–2538. [Google Scholar] [CrossRef] [PubMed]
- Cathey, A.L.; Watkins, D.J.; Rosario, Z.Y.; Vega, C.M.V.; Mukherjee, B.; O’neill, M.S.; Loch-Caruso, R.; Alshawabkeh, A.N.; Cordero, J.F.; Meeker, J.D. Gestational Hormone Concentrations Are Associated With Timing of Delivery in a Fetal Sex-Dependent Manner. Front. Endocrinol. 2021, 12, 742145. [Google Scholar] [CrossRef] [PubMed]
- Firestein, M.R.; Romeo, R.D.; Winstead, H.; Goldman, D.A.; Grobman, W.A.; Haas, D.M.; Parry, S.; Reddy, U.M.; Silver, R.M.; Wapner, R.J.; et al. Hypertensive disorders during pregnancy and polycystic ovary syndrome are associated with child communication and social skills in a sex-specific and androgen-dependent manner. Front. Endocrinol. 2022, 13, 1000732. [Google Scholar] [CrossRef]
- Firestein, M.R.; Romeo, R.D.; Winstead, H.; Goldman, D.A.; Grobman, W.A.; Haas, D.; Mercer, B.; Parker, C.; Parry, S.; Reddy, U.; et al. Elevated prenatal maternal sex hormones, but not placental aromatase, are associated with child neurodevelopment. Horm. Behav. 2022, 140, 105125. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Tian, L.; Yuan, J.; Xu, X.; Qu, F.; Zhang, R.; Wang, J. Associations Between Sex Hormone Levels and Autistic Traits in Infertile Patients With Polycystic Ovary Syndrome and Their Offspring. Front. Endocrinol. 2021, 12, 789395. [Google Scholar] [CrossRef] [PubMed]
- Rotem, R.S.; Nguyen, V.T.; Chodick, G.; Davidovitch, M.; Shalev, V.; Hauser, R.; A Coull, B.; Bellavia, A.; Weisskopf, M.G. Associations of Maternal Androgen-Related Conditions With Risk of Autism Spectrum Disorder in Progeny and Mediation by Cardiovascular, Metabolic, and Fertility Factors. Am. J. Epidemiol. 2021, 190, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Mitsui, T.; Araki, A.; Miyashita, C.; Ito, S.; Ikeno, T.; Sasaki, S.; Kitta, T.; Moriya, K.; Cho, K.; Morioka, K.; et al. Effects of prenatal sex hormones on behavioral sexual dimorphism. Pediatr. Int. 2019, 61, 140–146. [Google Scholar] [CrossRef]
- Liu, W.-B.; Zhu, H.-L.; Xiong, Y.-W.; Lv, J.; Huang, Y.-C.; Wang, H. Environmental cadmium exposure during gestation impairs fetal brain and cognitive function of adult offspring via reducing placenta-derived E2 level. Chemosphere 2022, 307, 135668. [Google Scholar] [CrossRef]
- Aquino, N.B.; Sevigny, M.B.; Sabangan, J.; Louie, M.C. The role of cadmium and nickel in estrogen receptor signaling and breast cancer: Metalloestrogens or not? J. Environ. Sci. Health Part C 2012, 30, 189–224. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Variable | Mean ± SD | Min, Max |
|---|---|---|
| Maternal age (years) | 29.14 ± 4.60 | 18, 41 |
| Maternal pre-pregnancy BMI (kg/m2) | 27.96 ± 7.17 | 15.31, 49.09 |
| GA at trimester 1 visit (weeks) | 12.24 ± 1.27 | 6.14, 14.43 |
| GA at trimester 2 visit (weeks) | 21.19 ± 1.77 | 18.14, 29.57 |
| GA at trimester 3 visit (weeks) | 31.31 ± 1.88 | 28.14, 39.00 |
| GA at birth (weeks) 1 | 39.50 ± 1.43 | 33.00, 42.71 |
| Frequency | Percentage | |
| Maternal race | ||
| White | 174 | 63.97 |
| Black/African American | 64 | 23.53 |
| Other 2 | 34 | 12.50 |
| Maternal ethnicity | ||
| Non-Hispanic or non-Latino | 246 | 90.44 |
| Hispanic or Latino | 26 | 9.56 |
| Highest maternal Education | ||
| High school or less | 97 | 35.66 |
| Some college, bachelors | 106 | 38.97 |
| Postgraduate | 69 | 25.37 |
| Parity | ||
| Yes (>1) | 181 | 66.54 |
| No (0) | 91 | 33.46 |
| Fetal Sex | ||
| Male | 138 | 50.74 |
| Female | 134 | 49.26 |
| Smoking during pregnancy | ||
| No | 254 | 93.38 |
| Yes | 18 | 6.62 |
| Pregnancy complications | ||
| Any | 35 | 12.87 |
| None | 237 | 87.13 |
| Term birth (>37 weeks) | ||
| Yes | 257 | 94.49 |
| No | 15 | 5.51 |
| Cadmium | n | Percent > LOD 1,2 | Min | Q1 (25%) | Median | Q3 (75%) | Max | Mean ± SD |
|---|---|---|---|---|---|---|---|---|
| Trimester 1 | 263 | 83.71% | 0.04 | 0.16 | 0.23 | 0.36 | 2.82 | 0.30 ± 0.26 |
| Trimester 2 | 267 | 86.14% | 0.03 | 0.10 | 0.15 | 0.24 | 2.91 | 0.21 ± 0.26 |
| Trimester 3 | 270 | 91.48% | 0.03 | 0.12 | 0.17 | 0.24 | 3.75 | 0.22 ± 0.27 |
| Hormone | Min | Q1 (25%) | Median | Q3 (75%) | Max | Mean ± SD |
|---|---|---|---|---|---|---|
| Trimester 1 (n = 270) | ||||||
| TT (ng/dL) | 8.80 | 37.10 | 59.90 | 88.30 | 303.00 | 70.54 ± 45.40 |
| FT (ng/dL) | 0.23 | 0.48 | 0.56 | 0.66 | 1.17 | 0.58 ± 0.16 |
| E1 (pg/mL) | 124.00 | 564.00 | 945.00 | 1430.00 | 5640.00 | 1156.21 ± 893.42 |
| E2 (pg/mL) | 356.00 | 1170.00 | 1610.00 | 2330.00 | 6390.00 | 1856.06 ± 995.65 |
| E3 1 (pg/mL) | 10.00 | 116.00 | 270.50 | 486.00 | 1470.00 | 326.41 ± 265.56 |
| Trimester 2 (n = 272) | ||||||
| TT (ng/dL) | 6.90 | 42.90 | 63.15 | 101.50 | 413.50 | 78.95 ± 54.68 |
| FT (ng/dL) | 0.19 | 0.43 | 0.48 | 0.56 | 0.93 | 0.50 ± 0.13 |
| E1 (pg/mL) | 423.00 | 2275.00 | 3570.00 | 5185.00 | 20,500.00 | 4215.79 ± 2986.52 |
| E2 (pg/mL) | 1750.00 | 4660.00 | 5955.00 | 7935.00 | 27,700.00 | 6509.85 ± 2968.77 |
| E3 (pg/mL) | 799.00 | 2340.00 | 3115.00 | 3890.00 | 11,900.00 | 3236.09 ± 1324.36 |
| Trimester 3 (n = 270) | ||||||
| TT (ng/dL) | 9.60 | 36.90 | 62.15 | 101.00 | 349.50 | 77.72 ± 57.45 |
| FT (ng/dL) | 0.20 | 0.43 | 0.50 | 0.58 | 1.04 | 0.51 ± 0.15 |
| E1 (pg/mL) | 751.00 | 3640.00 | 5855.00 | 8130.00 | 37,700.00 | 6803.49 ± 5153.37 |
| E2 (pg/mL) | 2380.00 | 8980.00 | 11,050.00 | 14,200.00 | 31,900.00 | 11,966.78 ± 4872.46 |
| E3 (pg/mL) | 1030.00 | 5130.00 | 6615.00 | 8340.00 | 26,300.00 | 7167.04 ± 3368.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Núñez, Z.; Hansel, M.; Capurro, C.; Kozlosky, D.; Wang, C.; Doherty, C.L.; Buckley, B.; Ohman-Strickland, P.; Miller, R.K.; O’Connor, T.G.; et al. Prenatal Cadmium Exposure and Maternal Sex Steroid Hormone Concentrations across Pregnancy. Toxics 2023, 11, 589. https://doi.org/10.3390/toxics11070589
Rivera-Núñez Z, Hansel M, Capurro C, Kozlosky D, Wang C, Doherty CL, Buckley B, Ohman-Strickland P, Miller RK, O’Connor TG, et al. Prenatal Cadmium Exposure and Maternal Sex Steroid Hormone Concentrations across Pregnancy. Toxics. 2023; 11(7):589. https://doi.org/10.3390/toxics11070589
Chicago/Turabian StyleRivera-Núñez, Zorimar, Megan Hansel, Camila Capurro, Danielle Kozlosky, Christina Wang, Cathleen L. Doherty, Brian Buckley, Pamela Ohman-Strickland, Richard K. Miller, Thomas G. O’Connor, and et al. 2023. "Prenatal Cadmium Exposure and Maternal Sex Steroid Hormone Concentrations across Pregnancy" Toxics 11, no. 7: 589. https://doi.org/10.3390/toxics11070589