
Two Different Heated Tobacco Products vs. Cigarettes: Comparison of Nicotine Delivery and Subjective Effects in Experienced Users
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aims and Ethics
2.2. Study Products and Groups
2.3. Participants
2.4. Study Design and Questionnaires
2.5. Blood Sampling and Determination of Nicotine, Cotinine, and Hydroxycotinine Plasma Levels
2.6. Pharmacokinetic (PK) Parameters and Statistical Analysis
3. Results
3.1. Participants
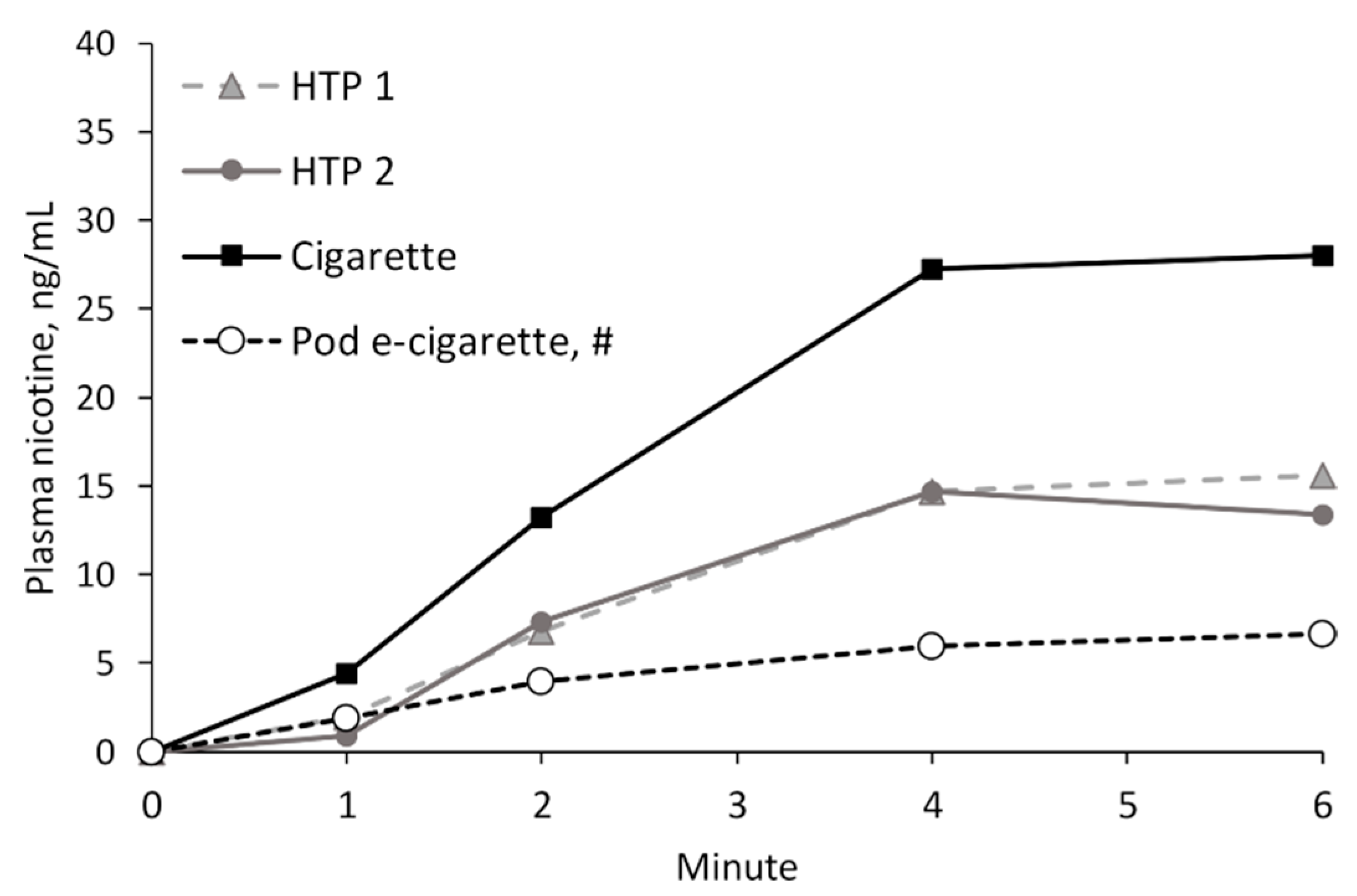
3.2. Nicotine Delivery
3.3. Nicotine Delivery in the Acute Phase
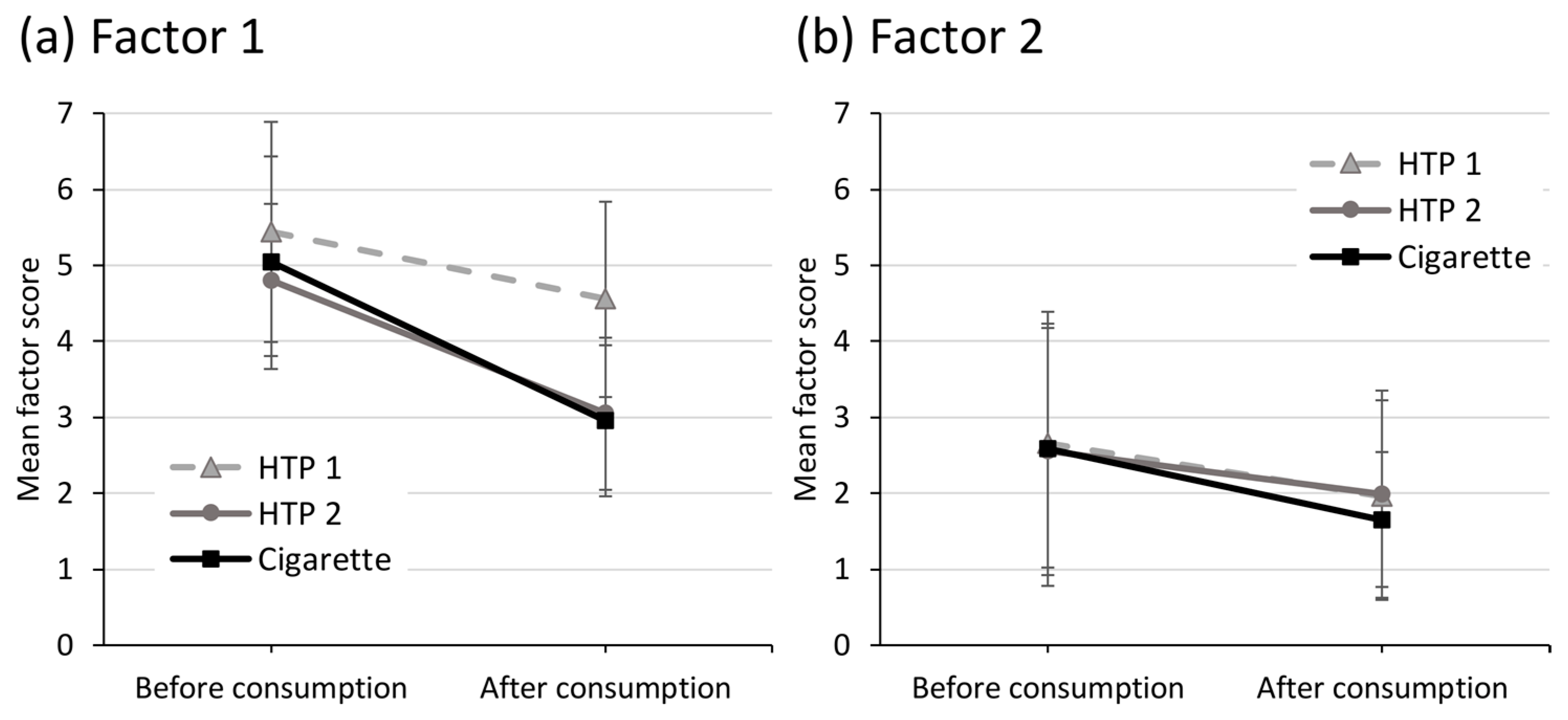
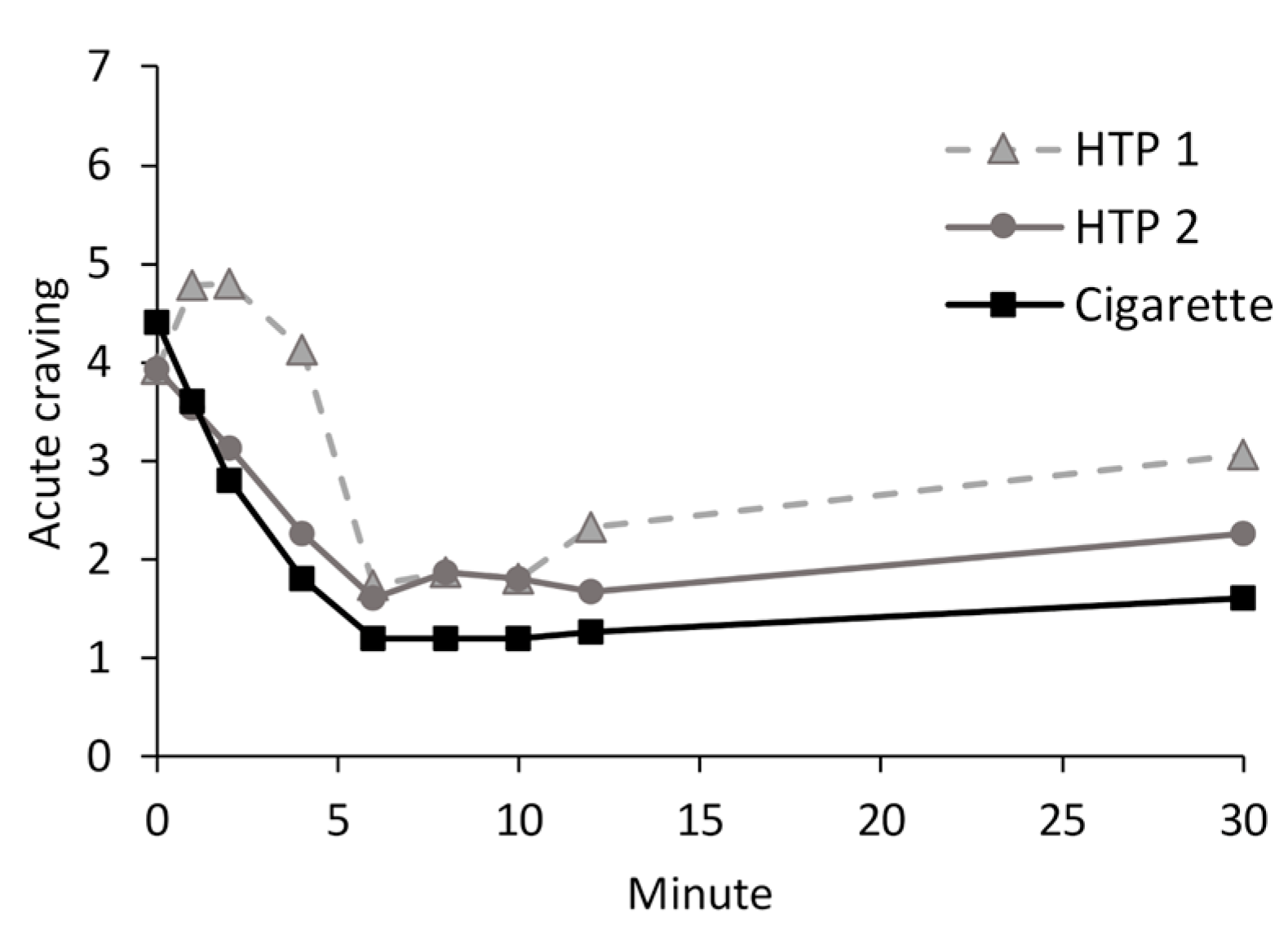
3.4. Relief of Cravings and Urges to Use the Product
3.5. Side Effects
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jankowski, M.; Brozek, G.M.; Lawson, J.; Skoczynski, S.; Majek, P.; Zejda, J.E. New ideas, old problems? Heated tobacco products—A systematic review. Int. J. Occup. Med. Environ. Health 2019, 32, 595–634. [Google Scholar] [CrossRef] [PubMed]
- Mallock, N.; Pieper, E.; Hutzler, C.; Henkler-Stephani, F.; Luch, A. Heated Tobacco Products: A Review of Current Knowledge and Initial Assessments. Front. Public Health 2019, 7, 287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.R.; Clark, B.; Ludicke, F.; Schaller, J.P.; Vanscheeuwijck, P.; Hoeng, J.; Peitsch, M.C. Evaluation of the Tobacco Heating System 2.2. Part 1: Description of the system and the scientific assessment program. Regul. Toxicol. Pharmacol. 2016, 81 (Suppl. 2), S17–S26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, D.; Jakaj, B.; Forster, M.; Nicol, J.; Mavropoulou, E.; Scott, K.; Liu, C.; McAdam, K.; Murphy, J.; Proctor, C.J. Assessment of tobacco heating product THP1.0. Part 2: Product design, operation and thermophysical characterisation. Regul. Toxicol. Pharmacol. 2018, 93, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Bialous, S.A.; Glantz, S.A. Heated tobacco products: Another tobacco industry global strategy to slow progress in tobacco control. Tob. Control 2018, 27, s111–s117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bekki, K.; Inaba, Y.; Uchiyama, S.; Kunugita, N. Comparison of Chemicals in Mainstream Smoke in Heat-not-burn Tobacco and Combustion Cigarettes. J. UOEH 2017, 39, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leigh, N.J.; Palumbo, M.N.; Marino, A.M.; O’Connor, R.J.; Goniewicz, M.L. Tobacco-specific nitrosamines (TSNA) in heated tobacco product IQOS. Tob. Control 2018, 27, s37–s38. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Luo, Y.; Jiang, X.; Zhang, H.; Zhu, F.; Hu, S.; Hou, H.; Hu, Q.; Pang, Y. Chemical Analysis and Simulated Pyrolysis of Tobacco Heating System 2.2 Compared to Conventional Cigarettes. Nicotine Tob. Res. 2019, 21, 111–118. [Google Scholar] [CrossRef]
- Mallock, N.; Boss, L.; Burk, R.; Danziger, M.; Welsch, T.; Hahn, H.; Trieu, H.L.; Hahn, J.; Pieper, E.; Henkler-Stephani, F.; et al. Levels of selected analytes in the emissions of “heat not burn” tobacco products that are relevant to assess human health risks. Arch. Toxicol. 2018, 92, 2145–2149. [Google Scholar] [CrossRef] [Green Version]
- Salman, R.; Talih, S.; El-Hage, R.; Haddad, C.; Karaoghlanian, N.; El-Hellani, A.; Saliba, N.A.; Shihadeh, A. Free-Base and Total Nicotine, Reactive Oxygen Species, and Carbonyl Emissions From IQOS, a Heated Tobacco Product. Nicotine Tob. Res. 2019, 21, 1285–1288. [Google Scholar] [CrossRef]
- Uchiyama, S.; Noguchi, M.; Takagi, N.; Hayashida, H.; Inaba, Y.; Ogura, H.; Kunugita, N. Simple Determination of Gaseous and Particulate Compounds Generated from Heated Tobacco Products. Chem. Res. Toxicol. 2018, 31, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Tattan-Birch, H.; Hartmann-Boyce, J.; Kock, L.; Simonavicius, E.; Brose, L.; Jackson, S.; Shahab, L.; Brown, J. Heated tobacco products for smoking cessation and reducing smoking prevalence. Cochrane Database Syst. Rev. 2022, 1, CD013790. [Google Scholar] [CrossRef]
- Hatsukami, D.K.; Carroll, D.M. Tobacco harm reduction: Past history, current controversies and a proposed approach for the future. Prev. Med. 2020, 140, 106099. [Google Scholar] [CrossRef] [PubMed]
- Abrams, D.B.; Glasser, A.M.; Pearson, J.L.; Villanti, A.C.; Collins, L.K.; Niaura, R.S. Harm Minimization and Tobacco Control: Reframing Societal Views of Nicotine Use to Rapidly Save Lives. Annu. Rev. Public Health 2018, 39, 193–213. [Google Scholar] [CrossRef] [Green Version]
- Goniewicz, M.L.; Smith, D.M.; Edwards, K.C.; Blount, B.C.; Caldwell, K.L.; Feng, J.; Wang, L.; Christensen, C.; Ambrose, B.; Borek, N.; et al. Comparison of Nicotine and Toxicant Exposure in Users of Electronic Cigarettes and Combustible Cigarettes. JAMA Netw. Open 2018, 1, e185937. [Google Scholar] [CrossRef] [Green Version]
- Dawkins, L.; Cox, S.; Goniewicz, M.; McRobbie, H.; Kimber, C.; Doig, M.; Kosmider, L. ‘Real-world’ compensatory behaviour with low nicotine concentration e-liquid: Subjective effects and nicotine, acrolein and formaldehyde exposure. Addiction 2018, 113, 1874–1882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmider, L.; Kimber, C.F.; Kurek, J.; Corcoran, O.; Dawkins, L.E. Compensatory Puffing With Lower Nicotine Concentration E-liquids Increases Carbonyl Exposure in E-cigarette Aerosols. Nicotine Tob. Res. 2018, 20, 998–1003. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Jacob, P., 3rd; Bernert, J.T.; Wilson, M.; Wang, L.; Allen, F.; Dempsey, D. Carcinogen exposure during short-term switching from regular to “light” cigarettes. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1376–1383. [Google Scholar] [CrossRef] [Green Version]
- Harris, J.E. Incomplete compensation does not imply reduced harm: Yields of 40 smoke toxicants per milligram nicotine in regular filter versus low-tar cigarettes in the 1999 Massachusetts Benchmark Study. Nicotine Tob. Res. 2004, 6, 797–807. [Google Scholar] [CrossRef]
- de Wit, H.; Bodker, B.; Ambre, J. Rate of increase of plasma drug level influences subjective response in humans. Psychopharmacology 1992, 107, 352–358. [Google Scholar] [CrossRef]
- Henningfield, J.E.; Keenan, R.M. Nicotine delivery kinetics and abuse liability. J. Consult. Clin. Psychol. 1993, 61, 743–750. [Google Scholar] [CrossRef]
- Ruther, T.; Hagedorn, D.; Schiela, K.; Schettgen, T.; Osiander-Fuchs, H.; Schober, W. Nicotine delivery efficiency of first- and second-generation e-cigarettes and its impact on relief of craving during the acute phase of use. Int. J. Hyg. Environ. Health 2018, 221, 191–198. [Google Scholar] [CrossRef]
- Picavet, P.; Haziza, C.; Lama, N.; Weitkunat, R.; Ludicke, F. Comparison of the Pharmacokinetics of Nicotine Following Single and Ad Libitum Use of a Tobacco Heating System or Combustible Cigarettes. Nicotine Tob. Res. 2016, 18, 557–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brossard, P.; Weitkunat, R.; Poux, V.; Lama, N.; Haziza, C.; Picavet, P.; Baker, G.; Ludicke, F. Nicotine pharmacokinetic profiles of the Tobacco Heating System 2.2, cigarettes and nicotine gum in Japanese smokers. Regul. Toxicol. Pharmacol. 2017, 89, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Hardie, G.; Gale, N.; McEwan, M.; Oscar, S.M.; Ziviani, L.; Proctor, C.J.; Murphy, J. An abuse liability assessment of the glo tobacco heating product in comparison to combustible cigarettes and nicotine replacement therapy. Sci. Rep. 2022, 12, 14701. [Google Scholar] [CrossRef]
- Goldenson, N.I.; Augustson, E.M.; Chen, J.; Shiffman, S. Pharmacokinetic and subjective assessment of prototype JUUL2 electronic nicotine delivery system in two nicotine concentrations, JUUL system, IQOS, and combustible cigarette. Psychopharmacology 2022, 239, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Phillips-Waller, A.; Przulj, D.; Pesola, F.; Smith, K.M.; Hajek, P. Nicotine Delivery and User Ratings of IQOS Heated Tobacco System Compared With Cigarettes, Juul, and Refillable E-Cigarettes. Nicotine Tob. Res. 2021, 23, 1889–1894. [Google Scholar] [CrossRef]
- Maloney, S.; Eversole, A.; Crabtree, M.; Soule, E.; Eissenberg, T.; Breland, A. Acute effects of JUUL and IQOS in cigarette smokers. Tob. Control 2020, 30, 449–452. [Google Scholar] [CrossRef]
- Mallock, N.; Rabenstein, A.; Gernun, S.; Laux, P.; Hutzler, C.; Karch, S.; Koller, G.; Henkler-Stephani, F.; Parr, M.K.; Pogarell, O.; et al. Nicotine delivery and relief of craving after consumption of European JUUL e-cigarettes prior and after pod modification. Sci. Rep. 2021, 11, 12078. [Google Scholar] [CrossRef]
- Rabenstein, A.; Rahofer, A.; Vukas, J.; Rieder, B.; Störzenhofecker, K.; Stoll, Y.; Burgmann, N.; Pieper, E.; Laux, P.; Luch, A.; et al. Usage pattern and nicotine delivery during ad libitum consumption of pod e-cigarettes and heated tobacco products. Toxics 2023, 11, 434. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerstrom Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Müller, V.; Mucha, R.F.; Ackermann, K.; Pauli, P. Die Erfassung des Cravings bei Rauchern mit einer deutschen Version des “Questionnaire on Smoking Urges“ (QSU-G). Z. Für Klin. Psychol. Psychother. 2001, 30, 164–171. [Google Scholar] [CrossRef]
- Mallock, N.; Rabenstein, A.; Laux, P.; Ruther, T.; Hutzler, C.; Parr, M.K.; Luch, A. Rapid, sensitive, and reliable quantitation of nicotine and its main metabolites cotinine and trans-3’-hydroxycotinine by LC-MS/MS: Method development and validation for human plasma. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2021, 1179, 122736. [Google Scholar] [CrossRef] [PubMed]
- Allenby, C.E.; Boylan, K.A.; Lerman, C.; Falcone, M. Precision Medicine for Tobacco Dependence: Development and Validation of the Nicotine Metabolite Ratio. J. Neuroimmune Pharmacol. 2016, 11, 471–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempsey, D.; Tutka, P.; Jacob, P., 3rd; Allen, F.; Schoedel, K.; Tyndale, R.F.; Benowitz, N.L. Nicotine metabolite ratio as an index of cytochrome P450 2A6 metabolic activity. Clin. Pharmacol. Ther. 2004, 76, 64–72. [Google Scholar] [CrossRef]
- Lerman, C.; Schnoll, R.A.; Hawk, L.W.; Cinciripini, P.; George, T.P.; Wileyto, E.P.; Swan, G.E.; Benowitz, N.l.; Heitjan, D.F.; Tyndale, R.F. Use of the nicotine metabolite ratio as a genetically informed biomarker of response to nicotine patch or varenicline for smoking cessation: A randomised, double-blind placebo-controlled trial. Lancet Respir. Med. 2015, 3, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Forster, M.; Fiebelkorn, S.; Yurteri, C.; Mariner, D.; Liu, C.; Wright, C.; McAdam, K.; Murphy, J.; Proctor, C. Assessment of novel tobacco heating product THP1.0. Part 3: Comprehensive chemical characterisation of harmful and potentially harmful aerosol emissions. Regul. Toxicol. Pharmacol. 2018, 93, 14–33. [Google Scholar] [CrossRef]
- Swan, G.E. Multiple risk factors for the initiation of smoking: The public health imperative for multidisciplinary genetic epidemiological investigations of nicotine addiction. Nicotine Tob. Res. 1999, 1 (Suppl. 2), S71–S73. [Google Scholar] [CrossRef]
- Bechara, A. Decision making, impulse control and loss of willpower to resist drugs: A neurocognitive perspective. Nat. Neurosci. 2005, 8, 1458–1463. [Google Scholar] [CrossRef]
- Wiers, R.W.; Bartholow, B.D.; van den Wildenberg, E.; Thush, C.; Engels, R.C.; Sher, K.J.; Grenard, J.; Ames, S.L.; Stacy, A.W. Automatic and controlled processes and the development of addictive behaviors in adolescents: A review and a model. Pharmacol. Biochem. Behav. 2007, 86, 263–283. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | |
|---|---|
| Age, median (IQR) | 32 (20) |
| Sex, female, n (%) | 8 (53) |
| Sex, male, n (%) | 7 (47) |
| Fagerstrom Test for Nicotine Dependence (FTND) *, median (IQR) | 2 (3) |
| Nicotine metabolite ratio (NMR), median (IQR) | 0.46 (0.28) |
| Number of days on which cigarettes were smoked within the last 30 days, median (IQR) | 4.5 (9) |
| Number of cigarettes smoked per day when cigarettes were smoked, median (IQR) | 3 (2.5) |
| Number of days on which the HTP was used within the last 30 days, median (IQR) | 30 (0) |
| HTP sticks used per day, median (IQR) | 11 (5) |
| HTP 1 | HTP 2 | Cigarette | HTP 1 vs. HTP 2 | HTP 1 vs. Cigarette | HTP 2 vs. Cigarette | |
|---|---|---|---|---|---|---|
| Cmax (ng/mL) | 14.9 (70%) | 11.6 (137%) | 25.1 (87%) | p = 0.540 | p = 0.021 * | p = 0.010 * |
| AUC0–30 min (ng/mL × h) | 4.0 (46%) | 3.0 (84%) | 6.1 (64%) | p = 0.279 | p = 0.006 * | p = 0.001 ** |
| tmax (min) | 6 (4–10) | 6 (4–12) | 6 (4–6) | p = 1.114 | p = 0.288 | p = 0.081 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vukas, J.; Mallock-Ohnesorg, N.; Rüther, T.; Pieper, E.; Romano-Brandt, L.; Stoll, Y.; Hoehne, L.; Burgmann, N.; Laux, P.; Luch, A.; et al. Two Different Heated Tobacco Products vs. Cigarettes: Comparison of Nicotine Delivery and Subjective Effects in Experienced Users. Toxics 2023, 11, 525. https://doi.org/10.3390/toxics11060525
Vukas J, Mallock-Ohnesorg N, Rüther T, Pieper E, Romano-Brandt L, Stoll Y, Hoehne L, Burgmann N, Laux P, Luch A, et al. Two Different Heated Tobacco Products vs. Cigarettes: Comparison of Nicotine Delivery and Subjective Effects in Experienced Users. Toxics. 2023; 11(6):525. https://doi.org/10.3390/toxics11060525
Chicago/Turabian StyleVukas, Jochen, Nadja Mallock-Ohnesorg, Tobias Rüther, Elke Pieper, Luna Romano-Brandt, Yvonne Stoll, Lukas Hoehne, Nestor Burgmann, Peter Laux, Andreas Luch, and et al. 2023. "Two Different Heated Tobacco Products vs. Cigarettes: Comparison of Nicotine Delivery and Subjective Effects in Experienced Users" Toxics 11, no. 6: 525. https://doi.org/10.3390/toxics11060525