
The Relationship of Arsenic Exposure with Hypertension and Wide Pulse Pressure: Preliminary Evidence from Coal-Burning Arsenicosis Population in Southwest China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Areas and Subject Selection
2.2. Interviews and Sample Collection
2.3. Measurement of Blood Pressure
2.4. Detection of Urinary Arsenic Species Levels
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Subjects
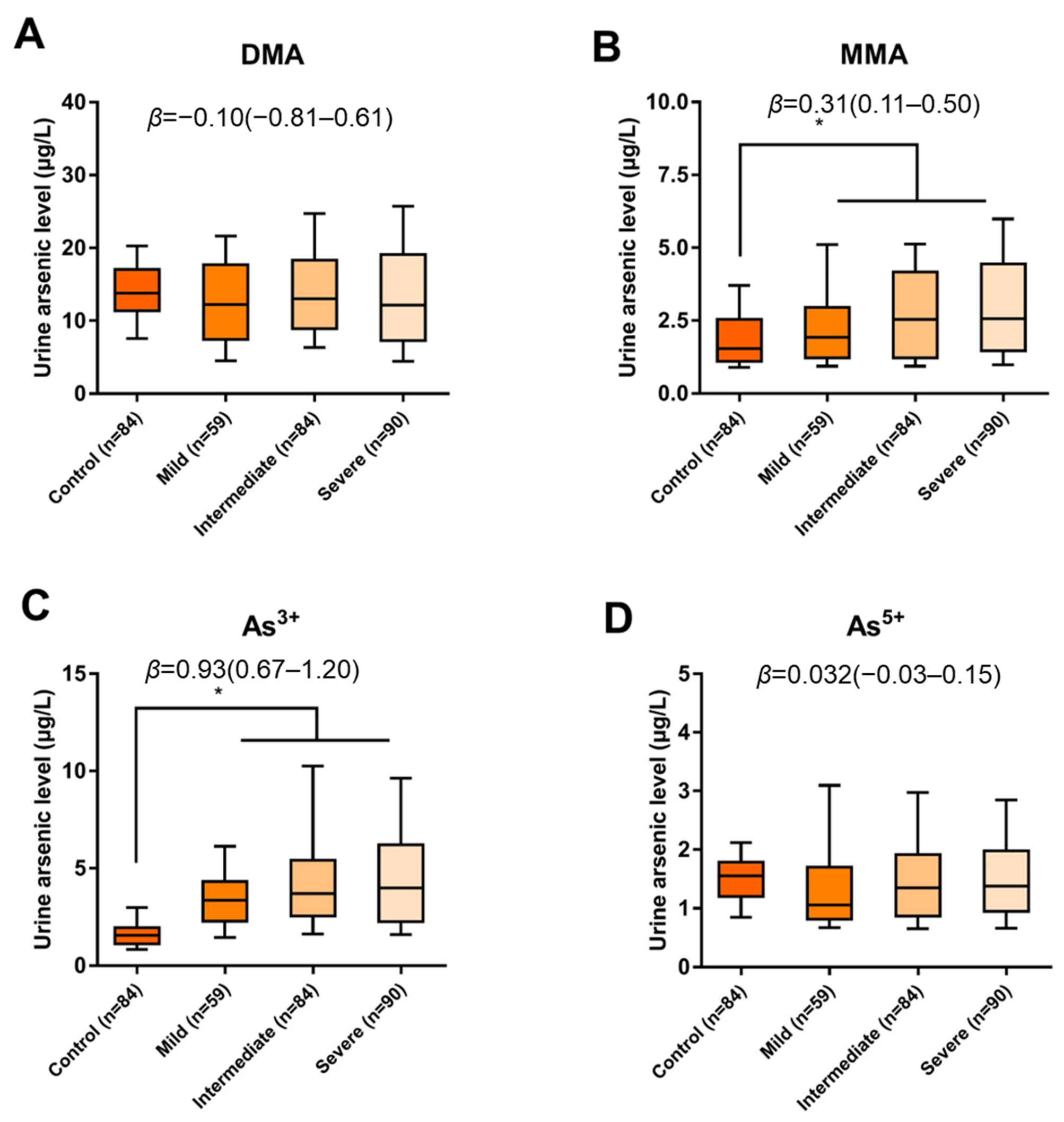
3.2. Levels of Certain Arsenic Species in Urine Were Higher in the Arsenicosis Population
3.3. SBP and PP Levels Increased in Subjects with Varying Degrees of Arsenicosis
3.4. The Incidence of Hypertension and WPP Was Higher in Arsenicosis Subjects
3.5. Urinary MMA and As3+ Levels Positively Correlate with Blood Pressure and Pulse Pressure in the Arsenicosis Population
3.6. Levels of Urinary MMA and As3+ Were Associated with Hypertension and WPP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Podgorski, J.; Berg, M. Global threat of arsenic in groundwater. Science 2020, 368, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Wei, D.; Tan, Z.; Lin, A.; Du, Y. The potential risk assessment for different arsenic species in the aquatic environment. J. Environ. Sci. 2015, 27, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Raju, N.J. Arsenic in the geo-environment: A review of sources, geochemical processes, toxicity and removal technologies. Environ. Res. 2022, 203, 111782. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Zou, Z.; Wang, Q.; Sun, B.; Liu, Y.; Liang, B.; Liu, Q.; Zhang, A. Association and risk of five miRNAs with arsenic-induced multiorgan damage. Sci. Total Environ. 2019, 680, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Seltenrich, N. Arsenic and Blood Pressure: A Long-Term Relationship. Environ. Health Perspect. 2015, 123, A218. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Li, A.; Mei, Y.; Zhou, Q.; Li, Y.; Li, K.; Xu, Q. The association of arsenic exposure with hypertension and blood pressure: A systematic review and dose-response meta-analysis. Environ. Pollut. 2021, 289, 117914. [Google Scholar] [CrossRef] [PubMed]
- Meier, T.; Gräfe, K.; Senn, F.; Sur, P.; Stangl, G.I.; Dawczynski, C.; März, W.; Kleber, M.E.; Lorkowski, S. Cardiovascular mortality attributable to dietary risk factors in 51 countries in the WHO European Region from 1990 to 2016: A systematic analysis of the Global Burden of Disease Study. Eur. J. Epidemiol. 2019, 34, 37–55. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Hsueh, Y.; Lai, M.; Shyu, M.; Chen, S.; Wu, M.; Kuo, T.; Tai, T. Increased prevalence of hypertension and long-term arsenic exposure. Hypertension 1995, 25, 53–60. [Google Scholar] [CrossRef]
- Shi, P.; Jing, H.; Xi, S. Urinary metal/metalloid levels in relation to hypertension among occupationally exposed workers. Chemosphere 2019, 234, 640–647. [Google Scholar] [CrossRef]
- Scannell, M.; Sofer, T.; Mossavar-Rahmani, Y.; Thyagarajan, B.; Zeng, D.; Daviglus, M.; Argos, M. Mendelian randomisation of inorganic arsenic metabolism as a risk factor for hypertension- and diabetes-related traits among adults in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) cohort. Int. J. Epidemiol. 2019, 48, 876–886. [Google Scholar] [CrossRef]
- Hall, E.M.; Acevedo, J.; López, F.G.; Cortés, S.; Ferreccio, C.; Smith, A.H.; Steinmaus, C.M. Hypertension among adults exposed to drinking water arsenic in Northern Chile. Environ. Res. 2017, 153, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.A.; González-Horta, C.; Sánchez-Ramírez, B.; Ballinas-Casarrubias, L.; Cerón, R.H.; Morales, D.V.; Terrazas, F.A.; Ishida, M.C.; Gutiérrez-Torres, D.S.; Saunders, R.J.; et al. Chronic Exposure to Arsenic and Markers of Cardiometabolic Risk: A Cross-Sectional Study in Chihuahua, Mexico. Environ. Health Perspect. 2016, 124, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Islam, A.K.; Majumder, A.A. Hypertension in Bangladesh: A review. Indian Heart J. 2012, 64, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Pichler, G.; Martinez, F.; Vicente, A.; Solaz, E.; Calaforra, O.; Redon, J. Pulse pressure amplification and its determinants. Blood Press. 2016, 25, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Luo, P.; Zou, Z.; Wang, Q.; Yao, M.; Yu, C.; Wei, S.; Sun, B.; Zhu, K.; Zeng, Q.; et al. Alterations of arsenic levels in arsenicosis residents and awareness of its risk factors: A population-based 20-year follow-up study in a unique coal-borne arsenicosis County in Guizhou, China. Environ. Int. 2019, 129, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wang, Q.; Zou, Z.; Zheng, F.; Zhang, A. Human arsenic exposure and lung function impairment in coal-burning areas in Guizhou, China. Ecotoxicol. Environ. Saf. 2020, 190, 110174. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, H.; Kay, P.; Slack, R.; Gong, Y.; Carter, A. Human exposure assessment of different arsenic species in household water sources in a high risk arsenic area. Sci. Total Environ. 2017, 584–585, 631–641. [Google Scholar] [CrossRef]
- Juárez-Reyes, A.; Jiménez-Capdeville, M.E.; Delgado, J.M.; Ortiz-Pérez, D. Time course of arsenic species in the brain and liver of mice after oral administration of arsenate. Arch. Toxicol. 2009, 83, 557–563. [Google Scholar] [CrossRef]
- Bozack, A.K.; Saxena, R.; Gamble, M.V. Nutritional Influences on One-Carbon Metabolism: Effects on Arsenic Methylation and Toxicity. Annu. Rev. Nutr. 2018, 38, 401–429. [Google Scholar] [CrossRef]
- Liu, J.; Zheng, B.; Aposhian, H.V.; Zhou, Y.; Chen, M.L.; Zhang, A.; Waalkes, M.P. Chronic arsenic poisoning from burning high-arsenic-containing coal in Guizhou, China. Environ. Health Perspect. 2002, 110, 119–122. [Google Scholar] [CrossRef]
- Li, D.; An, D.; Zhou, Y.; Liu, J.; Waalkes, M.P. Current status and prevention strategy for coal-arsenic poisoning in Guizhou, China. J. Health Popul. Nutr. 2006, 5624, 273–276. [Google Scholar]
- Gibbons, R.J.; Gardner, T.J.; Anderson, J.L.; Goldstein, L.B.; Meltzer, N.; Weintraub, W.S.; Yancy, C.W. The American Heart Association’s principles for comparative effectiveness research: A policy statement from the American Heart Association. Circulation 2009, 119, 2955–2962. [Google Scholar] [CrossRef] [PubMed]
- Bakris, G.L.; Laffin, L.J. Assessing Wide Pulse Pressure Hypertension: Data Beyond the Guidelines. J. Am. Coll. Cardiol. 2019, 73, 2856–2858. [Google Scholar] [CrossRef] [PubMed]
- Montoro-Leal, P.; García-Mesa, J.C.; Morales-Benítez, I.; García de Torres, A.; Vereda Alonso, E. Semiautomatic method for the ultra-trace arsenic speciation in environmental and biological samples via magnetic solid phase extraction prior to HPLC-ICP-MS determination. Talanta 2021, 235, 122769. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhihao, S.; Shen, M.; Xiao, Y.; Huang, X.; Lu, Y.; Yi, B.; Yang, G.; Luo, D.; Xiao, S.; et al. Association between chronic arsenic exposure and hypertension among HEAVY cohort participants. J. Hypertens. 2018, 36, e275. [Google Scholar] [CrossRef]
- Zhong, Q.; Zhang, C.; Zhang, Q.; Jiang, C.X.; Qin, Q.R.; Chen, J.; Liang, L.; Huang, F. Arsenic Exposure and Incident Hypertension of Adult Residents Living in Rural Areas Along the Yangtze River, Anhui, China. J. Occup. Environ. Med. 2019, 61, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Roy, N.K.; Murphy, A.; Costa, M. Arsenic Methyltransferase and Methylation of Inorganic Arsenic. Biomolecules 2020, 10, 1351. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Sun, B.; Wang, Q.; Zou, Z.; Ma, L.; Wang, W.; Zhang, A. Correlation between arsenic methylation metabolism and skin and liver damage in patients with coal-burning arsenism. Chin. J. Public Health 2021, 37, 5. [Google Scholar]
- Palma-Lara, I.; Martínez-Castillo, M.; Quintana-Pérez, J.C.; Arellano-Mendoza, M.G.; Tamay-Cach, F.; Valenzuela-Limón, O.L.; García-Montalvo, E.A.; Hernández-Zavala, A. Arsenic exposure: A public health problem leading to several cancers. Regul. Toxicol. Pharmacol. 2020, 110, 104539. [Google Scholar] [CrossRef]
- Cubadda, F.; Jackson, B.P.; Cottingham, K.L.; Van Horne, Y.O.; Kurzius-Spencer, M. Human exposure to dietary inorganic arsenic and other arsenic species: State of knowledge, gaps and uncertainties. Sci. Total Environ. 2017, 579, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Tamayo, L.I.; Kumarasinghe, Y.; Tong, L.; Balac, O.; Ahsan, H.; Gamble, M. Inherited genetic effects on arsenic metabolism: A comparison of effects on arsenic species measured in urine and in blood. Environ. Epidemiol. 2022, 6, e230. [Google Scholar] [CrossRef] [PubMed]
- Kligerman, A.D.; Doerr, C.L.; Tennant, A.H.; Harrington-Brock, K.; Allen, J.W.; Winkfield, E.; Poorman-Allen, P.; Kundu, B.; Funasaka, K.; Roop, B.C.; et al. Methylated trivalent arsenicals as candidate ultimate genotoxic forms of arsenic: Induction of chromosomal mutations but not gene mutations. Environ. Mol. Mutagen. 2003, 42, 192–205. [Google Scholar] [CrossRef] [PubMed]
- Tang, K.S.; Medeiros, E.D.; Shah, A.D. Wide pulse pressure: A clinical review. J. Clin. Hypertens. 2022, 22, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Geng, Y.J.; Chen, Z.; Krishnam, M.S.; Detrano, R.; Liu, H.; Yang, W.; Ouyang, T.; Dong, Y.; Yang, Y.; et al. Pulse pressure correlates with coronary artery calcification and risk for coronary heart disease: A study of elderly individuals in the rural region of Southwest China. Coron. Artery Dis. 2019, 30, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Lee, J.; Kwon, S.U.; Sung Kwon, H.; Hwan Lee, M.; Kang, D.W. Elevated Pulse Pressure and Recurrent Hemorrhagic Stroke Risk in Stroke with Cerebral Microbleeds or Intracerebral Hemorrhage. J. Am. Heart Assoc. 2022, 11, e022317. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, H.; Yano, Y.; Itoh, H.; Morita, K.; Kiriyama, H.; Kamon, T.; Fujiu, K.; Michihata, N.; Jo, T.; Takeda, N.; et al. Association of Blood Pressure Classification Using the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline with Risk of Heart Failure and Atrial Fibrillation. Circulation 2021, 143, 2244–2253. [Google Scholar] [CrossRef]
- Souza, A.C.F.; de Paiva Coimbra, J.L.; Ervilha, L.O.G.; Bastos, D.S.S.; Cossolin, J.F.S.; Santos, E.C.; de Oliveira, L.L.; Machado-Neves, M. Arsenic induces dose-dependent structural and ultrastructural pathological remodeling in the heart of Wistar rats. Life Sci. 2020, 257, 118132. [Google Scholar] [CrossRef]
- Bae, O.N.; Lim, E.K.; Lim, K.M.; Noh, J.Y.; Chung, S.M.; Lee, M.Y.; Yun, Y.P.; Kwon, S.C.; Lee, J.H.; Nah, S.Y.; et al. Vascular smooth muscle dysfunction induced by monomethylarsonous acid (MMA III): A contributing factor to arsenic-associated cardiovascular diseases. Environ. Res. 2009, 108, 300–308. [Google Scholar] [CrossRef]
- Van Oort, S.; Beulens, J.W.J.; Van Ballegooijen, A.J.; Grobbee, D.E.; Larsson, S.C. Association of Cardiovascular Risk Factors and Lifestyle Behaviors With Hypertension: A Mendelian Randomization Study. Hypertension 2020, 76, 1971–1979. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Control (n = 84) | Arsenicosis (n = 233) | Statistic-Value | p-Value |
|---|---|---|---|---|
| Age (year, mean ±SD) | 54.94 ± 9.21 | 53.55 ± 7.60 | 1.356 a | 0.176 |
| Gender, n (%) | ||||
| Male | 38 (45.2%) | 138 (59.2%) | 4.893 b | 0.027 |
| Female | 46 (54.8%) | 95 (40.8%) | ||
| BMI (kg/m2 mean ±SD) | 23.30 ± 3.79 | 24.27 ± 3.34 | −2.184 a | 0.030 |
| Smoking status, n (%) | ||||
| No | 47 (56.0%) | 105 (45.1%) | 2.933 b | 0.087 |
| Yes | 37 (44.0%) | 128 (54.9%) | ||
| Alcohol usage, n (%) | ||||
| No | 54 (64.3%) | 138 (59.2%) | 0.661 b | 0.416 |
| Yes | 30 (35.7%) | 95 (40.8%) | ||
| Blood pressure (mmHg, mean ± SD) | ||||
| SBP | 126.40 ± 15.03 | 139.37 ± 15.37 | −6.673 a | <0.001 |
| DBP | 79.65 ± 8.33 | 78.79 ± 10.02 | 0.705 a | 0.482 |
| PP | 46.74 ± 11.41 | 60.58 ± 15.14 | −7.626 a | <0.001 |
| Urine arsenic (ug/L, M, P25–P75) | ||||
| t-As | 18.30 (15.89–23.23) | 19.69 (14.08–29.15) | 0.975 c | 0.329 |
| DMA | 13.77 (11.42–17.04) | 12.57 (8.03–18.30) | −1.284 c | 0.199 |
| MMA | 1.54 (1.10–2.55) | 2.27 (1.23–4.02) | 3.406 c | 0.001 |
| As3+ | 1.56 (1.12–1.94) | 3.63 (2.38–5.45) | 9.719 c | <0.001 |
| As5+ | 1.55 (1.20–1.79) | 1.30 (0.88–1.93) | 1.714 c | 0.087 |
| Blood Pressure (mmHg) | Control (n = 84) | Degrees of Arsenicosis | F, p | β (95%CI), p-Trend | ||
|---|---|---|---|---|---|---|
| Mild (n = 59) | Intermediate (n = 84) | Severe (n = 90) | ||||
| SBP | 126.40 ± 15.03 | 136.51 ± 13.31 | 140.20 ± 17.66 | 140.48 ± 14.20 | 15.811, <0.001 | 4.768 (3.267–6.270) <0.001 |
| DBP | 79.66 ± 8.33 | 77.76 ± 9.44 | 78.79 ± 9.56 | 79.47 ± 10.82 | 0.538 0.656 | 0.056 (−0.886–0.997) 0.907 |
| PP | 46.74 ± 11.41 | 58.75 ± 13.21 | 61.41 ± 18.25 | 61.01 ± 13.06 | 19.791, <0.01 | 4.713 (3.265–6.160) <0.001 |
| Control (n = 84) | Degrees of Arsenicosis | OR for Trend | p-Trend | |||
|---|---|---|---|---|---|---|
| Mild (n = 59) | Intermediate (n = 84) | Severe (n = 90) | ||||
| Hypertension SBP ≥ 140 or DBP ≥ 90 mmHg | ||||||
| Yes | 22 (26.2%) | 24 (40.7%) | 44 (52.4%) | 48 (53.3%) | 1.47 (1.19–1.82) a | <0.001 a |
| No | 62 (73.8%) | 35 (59.3%) | 40 (47.6%) | 42 (46.7%) | ||
| OR (95%CI) | -- | 1.82 (0.88–3.79) b | 3.04 (1.55–5.94) b | 3.08 (1.57–6.06) b | ||
| p | -- | 0.108 b | 0.001 b | 0.001 b | ||
| High-normal BP SBP = 103–139 or DBP = 85–90 | ||||||
| Yes | 11 (13.1%) | 16 (27.1%) | 22 (26.2%) | 18 (20%) | 1.25 (0.97–1.62) a | 0.088 a |
| No | 73 (86.9%) | 43 (72.9%) | 62 (73.8%) | 72 (80%) | ||
| OR (95%CI) | -- | 2.53 (1.05–6.11) b | 2.45 (1.07–5.59) b | 2.18 (0.92–5.18) b | ||
| p | -- | 0.039 b | 0.033 b | 0.077 b | ||
| WPP PP ≥ 60 | ||||||
| Yes | 15 (17.9%) | 26 (44.1%) | 41 (48.8%) | 46 (51.1%) | 1.65 (1.32–2.06) a | <0.001 a |
| No | 69 (82.1%) | 33 (55.9%) | 43 (51.2%) | 44 (48.9%) | ||
| OR (95%CI) | -- | 3.60 (1.66–7.79) b | 4.51 (2.19–9.28) b | 5.25 (2.53–10.89) b | ||
| p | -- | 0.001 b | <0.001 b | <0.001 b | ||
| Q1 (Low) | Q2 (Mid-Low) | Q3 (Mid-High) | Q4 (High) | OR for Trend | p for Trend | |
|---|---|---|---|---|---|---|
| Hypertension SBP ≥ 140 or DBP ≥ 90 mmHg | 26/74 (35.1%) | 25/84 (29.8%) | 42/78 (53.8%) | 45/81 (55.6%) | ||
| Model 1 a | -- | 0.78 (0.40–1.53) | 2.15 (1.12–4.14) | 2.31 (1.21–4.11) | 1.43 (1.17–1.76) | 0.001 |
| p-value a | -- | 0.471 | 0.021 | 0.011 | ||
| Model 2 b | -- | 0.69 (0.35–1.37) | 2.01 (1.02–3.97) | 1.99 (1.04–3.80) | 1.37 (1.11–1.70) | 0.004 |
| p-value b | -- | 0.289 | 0.043 | 0.045 | ||
| WPP PP ≥ 60 | 24/74 (32.4%) | 29/84 (34.5%) | 30/78 (38.5%) | 45/81 (55.6%) | ||
| Model 1 a | -- | 1.10 (0.57–2.13) | 1.30 (0.67–2.54) | 2.60 (1.35–5.01) | 1.37 (1.11–1.69) | 0.003 |
| p-value a | -- | 0.781 | 0.438 | 0.004 | ||
| Model 2 b | -- | 1.04 (0.53–2.03) | 1.29 (0.65–2.56) | 2.42 (1.23–4.72) | 1.35 (1.09–1.67) | 0.006 |
| p-value b | -- | 0.920 | 0.462 | 0.010 |
| Q1 (Low) | Q2 (Mid-Low) | Q3 (Mid-High) | Q4 (High) | OR for Trend | p for Trend | |
|---|---|---|---|---|---|---|
| Hypertension SBP ≥ 140 or DBP ≥ 90 mmHg | 24/81 (29.6%) | 32/78 (41.0%) | 33/79 (41.8%) | 49/79 (62.0%) | ||
| Model1 a | -- | 1.65 (0.86–3.19) | 1.70 (0.89–3.28) | 3.88 (2.01–7.50) | 1.51 (1.23–1.85) | <0.001 |
| p-value | -- | 0.134 | 0.110 | <0.001 | ||
| Model2 b | -- | 1.59 (0.81–3.12) | 1.67 (0.85–3.28) | 3.68 (1.86–7.30) | 1.49 (1.20–1.84) | <0.001 |
| p-value | -- | 0.177 | 0.135 | <0.001 | ||
| WPP PP ≥ 60 | 21/81 (25.9%) | 27/78 (34.6%) | 35/79 (44.3%) | 45/79 (57.0%) | ||
| Model1 a | -- | 1.51 (0.77–2.99) | 2.27 (1.17–4.43) | 3.78 (1.94–7.37) | 1.55 (1.26–1.92) | <0.001 |
| p-value | -- | 0.234 | 0.016 | <0.001 | ||
| Model2 b | -- | 1.49 (0.75–2.98) | 2.35 (1.19–4.64) | 3.84 (1.93–7.64) | 1.57 (1.26–1.95) | 0.001 |
| p-value | -- | 0.257 | 0.014 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; Tian, H.; Wang, W.; Liu, S.; Zhang, A. The Relationship of Arsenic Exposure with Hypertension and Wide Pulse Pressure: Preliminary Evidence from Coal-Burning Arsenicosis Population in Southwest China. Toxics 2023, 11, 443. https://doi.org/10.3390/toxics11050443
Wang Q, Tian H, Wang W, Liu S, Zhang A. The Relationship of Arsenic Exposure with Hypertension and Wide Pulse Pressure: Preliminary Evidence from Coal-Burning Arsenicosis Population in Southwest China. Toxics. 2023; 11(5):443. https://doi.org/10.3390/toxics11050443
Chicago/Turabian StyleWang, Qingling, Haidong Tian, Wenjuan Wang, Shuhong Liu, and Aihua Zhang. 2023. "The Relationship of Arsenic Exposure with Hypertension and Wide Pulse Pressure: Preliminary Evidence from Coal-Burning Arsenicosis Population in Southwest China" Toxics 11, no. 5: 443. https://doi.org/10.3390/toxics11050443