3.1. Method Validation
The validated analysis method was acceptable (
Table S1), and the sensitivity of the proposed method for detecting incredibly low concentrations of heroin biomarkers and higher concentrations of morphine in urine and bile had an LOQ of 1 ng/mL for all analytes. As indicated in
Table S1, the autosampler was set to 4 °C during the stability experiments, which showed that the three controls were stable up to one week, with concentrations of analytes of interest expressed as percentages to their target concentration, which were within ±10%. As most heroin users are known to be polydrug users, the ability of the method to distinguish between analytes of interest and other co-ingested drugs is crucial, especially when opioids with similar drug chemistry can be used. Peaks were not observed in the chromatogram following the injection of blank samples alone, internal standards, or standards of the analytes of interest. Similar results were obtained when only internal standards were injected and no response to heroin biomarkers, morphine, or codeine was observed. This confirmed that both the standards and the internal standards were pure.
Linearity was accepted, with coefficients of determination greater than 0.99 for 6-MAM, 6-AC, morphine, and codeine in multiple body fluid samples. The LOD values were estimated from ten different calibration curves and ranged between 0.2 and 0.4 ng/g, while the LOQ was evaluated by spiking with 1 ng/mL of each analyte of interest, and the results were calculated using freshly prepared calibration curves for all analytes of interest in different matrices of interest. The precision, accuracy, dilution, and autosampler stability results were all within 15% of the nominal value, thus confirming that the method is suitable for the quantification of target analytes in the matrices of interest. In addition, carryover contamination from the previous positive control test was not detected.
3.2. Case Samples
3.2.1. Demographic Profile
The number of heroin-related deaths in the city of Jeddah within the study period represents 2% of the total number of postmortem cases received by the JPCC between 2008 and 2018 (
Figure 1). Although the Jeddah population has increased in recent years, the number of heroin-related fatalities has remained unchanged, with a median of 9 cases per year (ranging 4–15 cases/year). Almost 70% of the heroin-related deaths occurred among Saudi citizens, while 30% occurred among other nationalities. In addition, 64% of the deceased were unemployed and supported by their families. As indicated in
Figure 2 and
Table S2, the median BNaF morphine concentration was 282 ng/mL (
n = 85; range, 23–4400 ng/mL); the highest median BNaF morphine concentration occurred in 2012 (470 ng/mL), while the lowest median concentration occurred in 2008 (141 ng/mL).
3.2.2. Age Groups and Analyte Concentrations
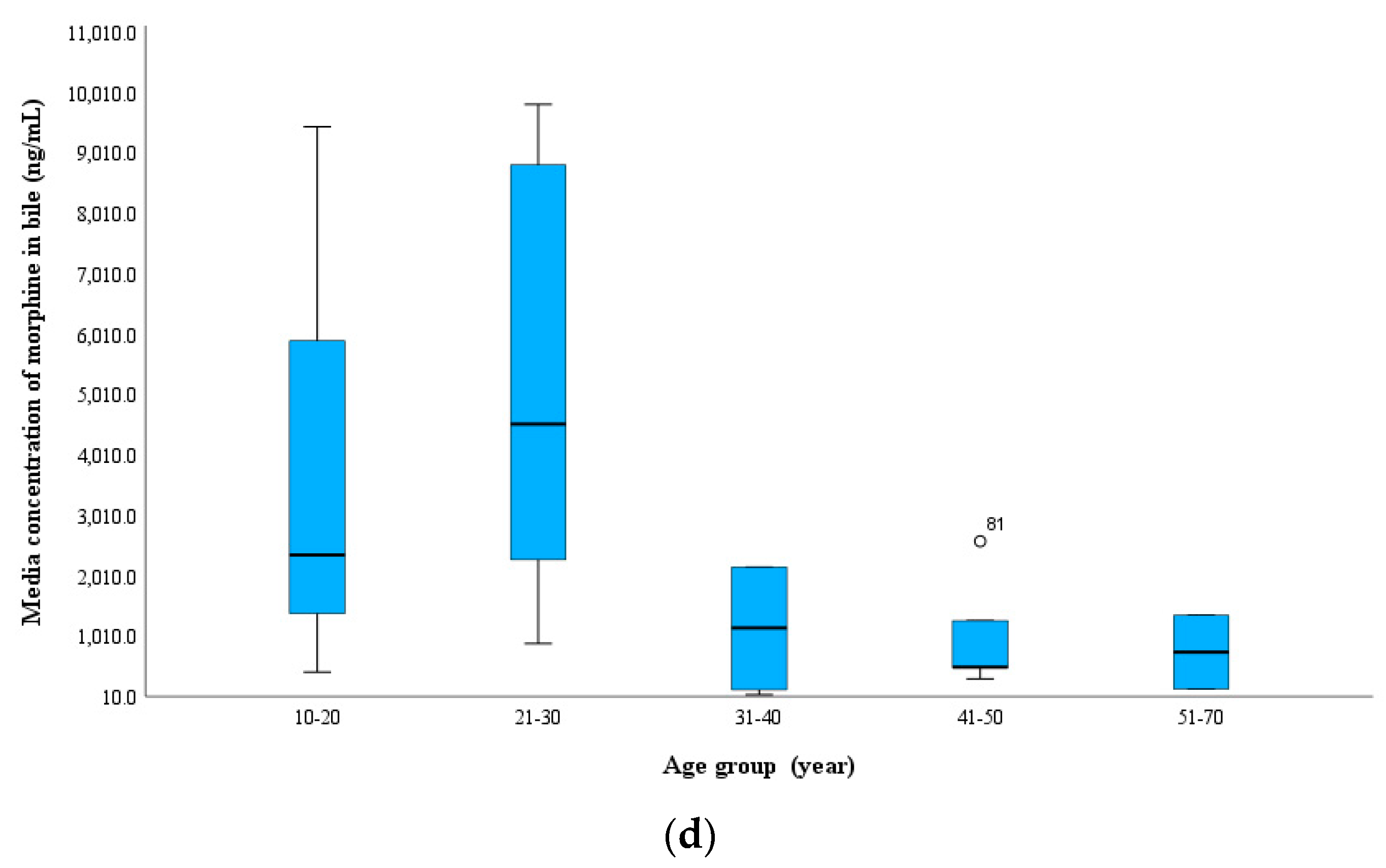
The mean age of the patients was 38 ± 12 years (range, 16–70 years; males, 98%). The 21–30 age group had the highest number of deaths, with almost 33% of the total cases (n = 32 cases), followed by the 31–40 age group (n = 26 cases, 27%), while the 10–20 age group had the lowest number of heroin-related death cases (n = 4 cases, 4%;
Figure 3 and
Table S3). Notably, a gradual increase in the median blood morphine concentration occurred from the youngest to the oldest age groups, with a median of 190 ng/mL in the 10–20 group and 302 ng/mL in the 51–70 group. This was also observed for morphine in the vitreous humor; in relation to age, the 6-MAM median concentration showed the same trend as morphine. 6-MAM was not detected in 75% of the cases in the 10–20 year age group, whereas it was present in 40% in the 61–70 year age group and at concentrations (BNaF median, 21 ng/mL; vitreous humor median, 52 ng/mL). This can be understood by the increase in tolerance that occurred as the duration of heroin addiction increased. Therefore, 6-MAM was more likely to be detected in the older age groups than the younger age groups. In contrast, 6-MAM was higher in the biliary specimens of the youngest age groups, as indicated in
Figure 3.
In the current investigation, 6-AC was more likely to be detected in the middle-aged groups and was detected in most urine samples in all age groups in this study. This finding indicates that urine is the best choice matrix for 6-AC analysis in both antemortem and postmortem samples [
17,
30,
31]. In relation to age, the codeine concentration in the blood was slightly higher in the older age groups.
3.2.3. PMI and Analyte Concentrations
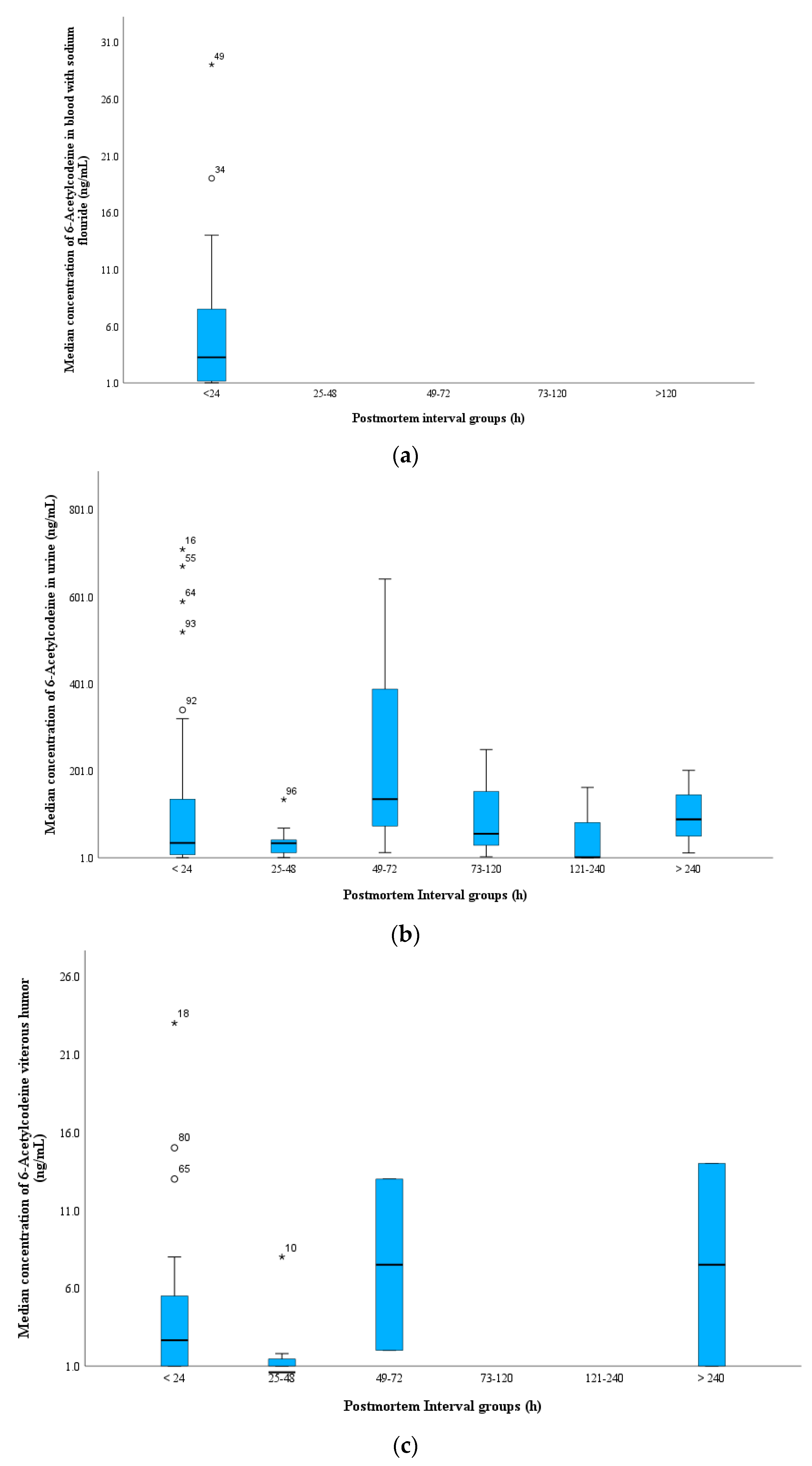
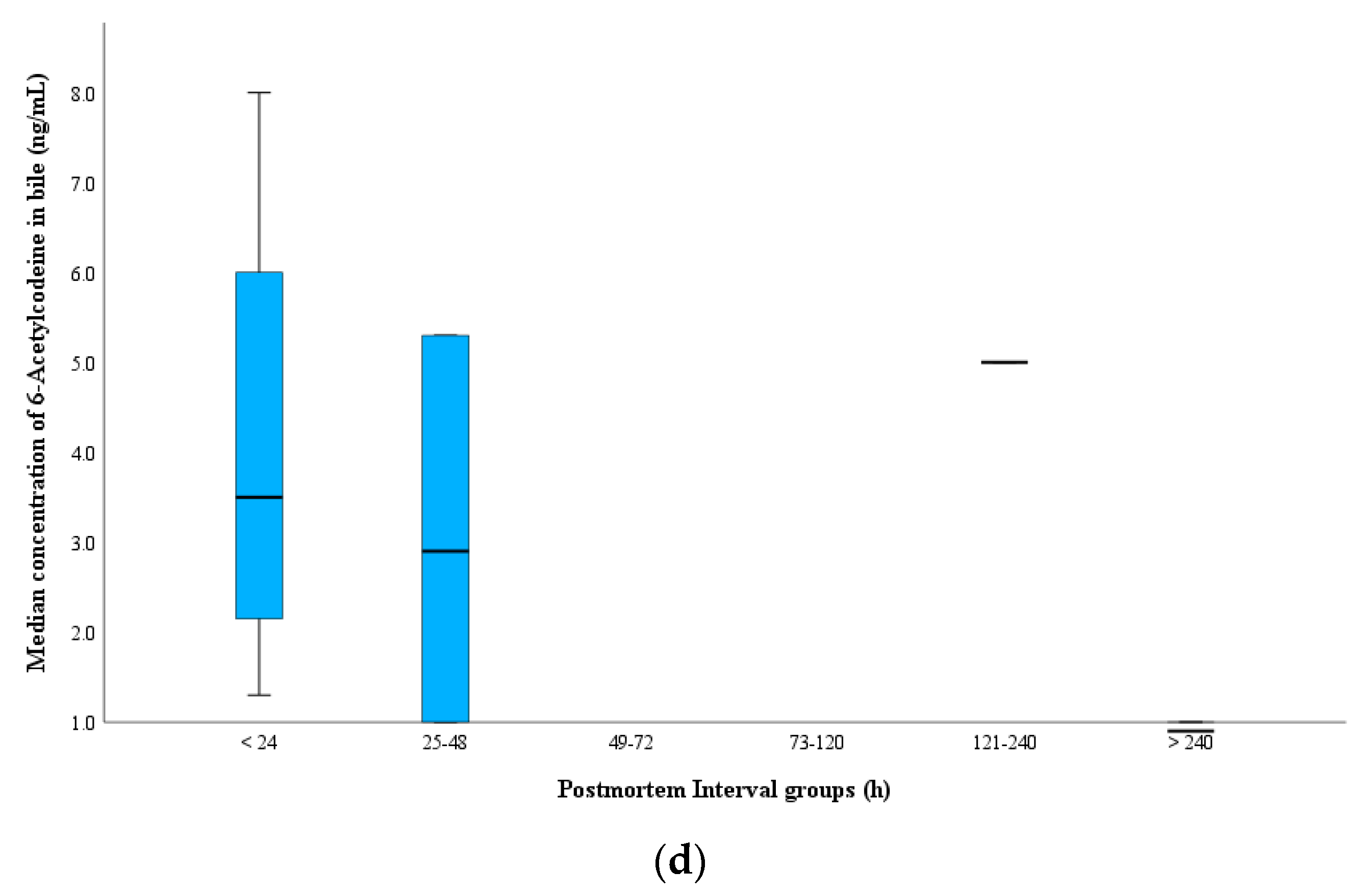
The majority of cases had a PMI within 24 h (51% of total cases), which led to the identification of both heroin biomarkers when the blood was fresh and putrefaction was not observed. The median concentrations of 6-MAM and 6-AC in cases with a PMI within 24 h were 16 and 2 ng/mL, 22 and 3 ng/mL, 324 and 35 ng/mL, and 12 and 4 ng/mL in the BNaF, vitreous humor, urine, and bile samples, respectively (
Table S4). 6-AC was present in the blood at extremely low concentrations in cases where the PMI was less than 48 h, and no 6-AC was detected in any BNaF cases when the PMI was greater than 48 h, although most cases were stored properly following death. In contrast, 6-AC was still detected in the urine samples from all PMI groups (
Figure 4). As expected, the median morphine concentration in BNaF increased with longer PMIs. The lowest median morphine concentration (263 ng/mL) was observed at a PMI of 24 h, and the highest concentration (380 ng/mL) was observed at a PMI ranging from 121–240 h (
Figure S1).
In the current study, both biomarkers were detected in the vitreous humor in two cases with a PMI longer than 10 days, whereas 6-MAM was negative in the BNaF samples, which indicates that the role of PMIs on heroin biomarkers can be minimized if samples are stored correctly following autopsy and if the vitreous humor is the sample of choice for heroin-related fatality investigations.
Figure S2 shows the distribution of 6-MAM in BNaF and vitreous humor samples among PMI groups in the current study.
3.2.4. Mode of Death
In the current study, heroin alone contributed to death in 68% of the studied cases, whereas intoxication with other co-ingested substances contributed to 32% (
Table 2). A higher median morphine concentration (310 ng/mL) was observed in the heroin-only cause of death cases than in the polydrug intoxication group (250 ng/mL). The median 6-MAM concentration was similar between these two groups, whereas the median 6-AC concentration in the heroin-alone cases was higher (2.5-fold) than that in the polydrug intoxication group. No difference was observed between the codeine concentrations in the two groups.
These findings indicate that the morphine concentration in heroin-related fatalities showing the presence of other CNS drugs is often lower than that in heroin-alone cases. The significant role of the PMI in cases of heroin metabolites is well known, and the tolerance and health status of the deceased contribute to this finding. Similar trends were observed among the various specimens, with slightly higher median concentrations in the urine and bile. Moreover, a polydrug intoxication case showed a slightly higher morphine concentration in the vitreous humor than that with heroin alone.
The most frequently detected drugs, regardless of the cause of death, were methamphetamine, cannabis, amphetamine, alprazolam, cocaine, and ethanol. Thirty-eight cases only showed heroin metabolites. A higher median morphine concentration was measured in only heroin cases compared to those in which heroin was the sole cause of death despite the presence of another drug, such as amphetamine or cannabis (370 ng/mL vs. 310 ng/mL). Similarly, the median morphine concentration (312 ng/mL) decreased when one extra drug was used, and it was further decreased (191 and 198 ng/mL) when two and four extra drugs were co-ingested, respectively.
Notably, methamphetamine was co-ingested with heroin in twenty-three cases (BNaF median morphine concentration, 284 ng/mL). The median morphine concentration for most co-ingested drugs was often higher than 200 ng/mL. A reduction in the median morphine concentration (BNaF, 154 ng/mL) occurred when heroin was used in combination with cocaine.
3.2.5. Time Span between Heroin Intake and Death
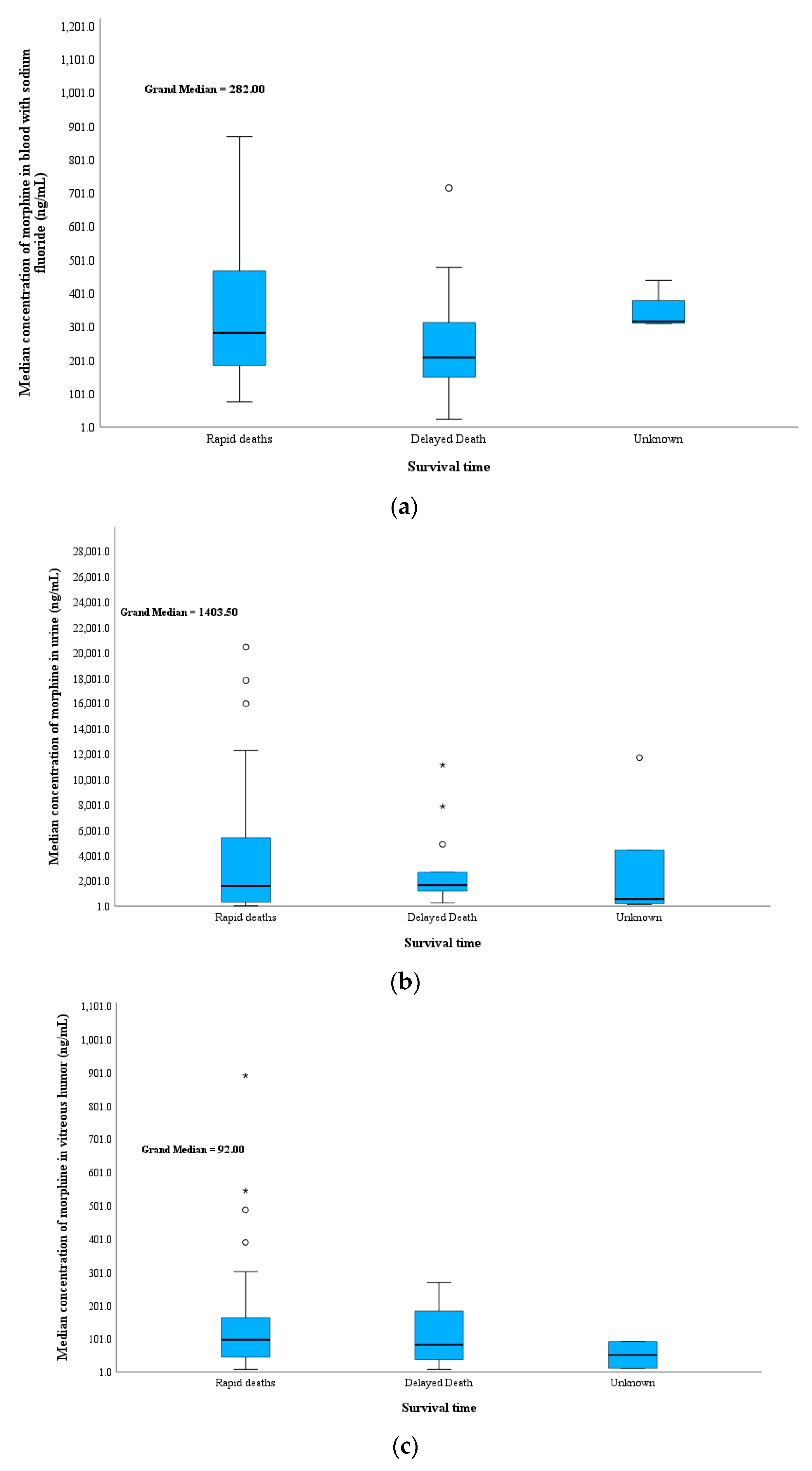
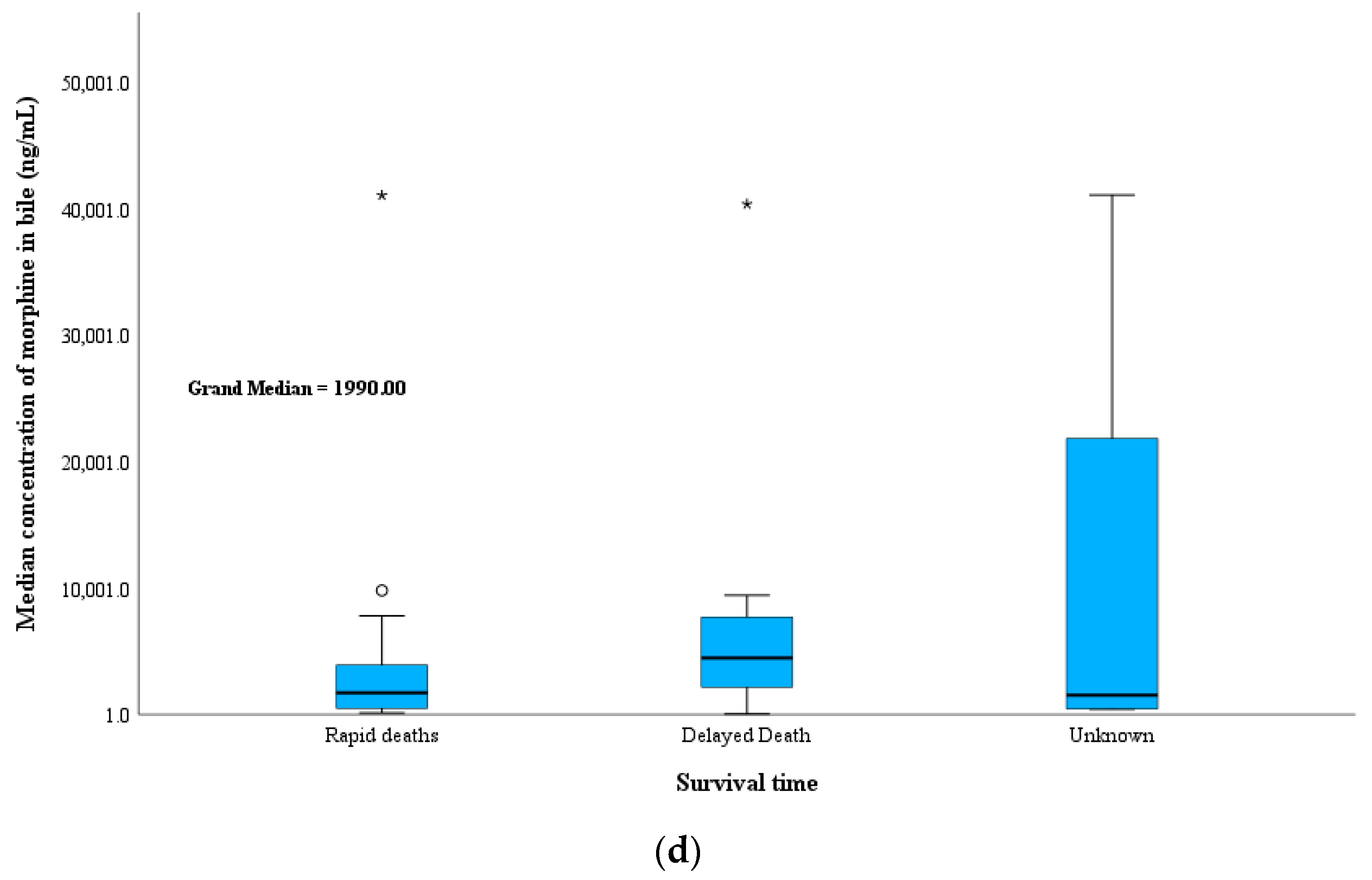
In this study, 61% and 24% of the cases were rapid and delayed deaths, respectively, and 15% had an undetermined time of death. This was either because of a lack of information caused by the deceased dying without a witness or because the bodies were moved after death to a deserted area where the bodies began to decompose and thus did not show signs of heroin use, such as injection marks (
Table 3 and
Figure 5). In these cases, both heroin biomarkers tested negative in the BNaF samples. Although a higher PMI was detected in these cases, heroin biomarkers were detected in alternative body fluids, and all urine samples tested positive for 6-MAM.
This suggests that either the undetermined cases died immediately after heroin was administered and the environmental surroundings allowed for the hydrolysis of 6-MAM to morphine or that a delayed death occurred, which allowed morphine glucuronide to deconjugate to free morphine due to the long PMI before sampling. In contrast, lower median morphine concentrations were observed in the delayed death group (median BNaF = 210 ng/mL) than the rapid death group.
In all groups, the median morphine concentration was much lower in the vitreous humor than the blood. This indicates that some of the heroin biomarkers were converted to their metabolites in the blood but were stable in the vitreous humor after death. Nevertheless, the vitreous humor results should be interpreted with caution because a certain amount of morphine is associated with accumulation from the use of old doses by chronic heroin users. Interestingly, 6-MAM levels were higher for the rapid death cases (36 ng/mL) than the delayed death cases (14 ng/mL) and undetermined death cases (7 ng/mL). This can be explained by many factors, including the longer PMI in delayed deaths, putrefaction effects, and body storage effects, especially when the time of death is unknown. These conditions led to a decrease in the 6-MAM concentration in the vitreous humor. This highlights the importance of testing the vitreous humor in cases of longer PMIs and negative 6-MAM in the blood.
Morphine levels in bile were primarily detected in chronic heroin users, which limits the use of these values in distinguishing between rapid and delayed deaths. 6-MAM in bile was detected in 10 of 17 rapid deaths, 3 of 6 delayed deaths, and not detected of 4 undermined cases. Urine is most likely to be positive for heroin biomarkers and their metabolites in these types of deaths. In this study, the free morphine concentration was high for rapid deaths (2100 ng/mL) compared to that for delayed deaths (1300 ng/mL) and undetermined cases (550 ng/mL). An almost 4-fold higher median concentration of 6-AC in urine was observed for rapid death (40 ng/mL) compared with delayed death (10 ng/mL). Moreover, the median codeine concentration was higher in the unknown group (30 ng/mL) than in the rapid (20 ng/mL) and delayed groups (10 ng/mL). Codeine forms quickly after heroin ingestion as a product of 6-AC degradation. Most codeine is metabolized to codeine-6-glucuronide, while some is metabolized to morphine.
3.2.6. Manner of Death
In the current study, 76% of the total cases were ascribed to accidental death, and they had a median age, median BNaF morphine concentration, and PMI of 38 years, 280 ng/mL, and 24 h, respectively. Nevertheless, most heroin abusers in Saudi Arabia used drugs in private or remote areas, such as deserted areas and open land outside the city. In the case of overdoses, deceased bodies left behind without witnesses complicated the identification of the mode of death, especially if the bodies were heavily putrefied.
Information about intentional overdoses was available for seven heroin-related fatalities. Four of these individuals died at home, and two died outdoors while accompanied by a friend. These cases had a median BNaF morphine concentration of 480 ng/mL, a PMI of 24 h, and an age of 48. The highest levels of vitreous humor and morphine were detected in suicide cases (150 ng/m).
In five cases, the mode of death was identified as homicide, and they presented a median BNaF morphine concentration of 180 ng/mL, a PMI of 24 h, and an age of 22. Notably, most cases were discovered outdoors.
The data in
Table 4 clearly show that heroin biomarkers were higher in suicides, which had median concentrations of 210 ng/mL for 6-MAM. The role of multiple specimens was crucial for the undetected modes of death because few blood specimens were available for testing. The detection of heroin biomarkers facilitates the source of opioid identification and survival time. In some cases, although syringes and heroin bags were found at the scene, the blood samples were negative for heroin biomarkers. No difference in codeine concentrations was observed according to the mode of death. The manner of deaths was not determined in the last 11 cases.
3.2.7. Route of Administration
Table 5 demonstrates that heroin injection was the main route of administration in the current investigation, followed by sniffing. The route of administration was unknown in 16 of cases, with most involving decomposed bodies. Syringes were found at the scene in 36% of the studied cases. Needle marks were identified in 65% of the total cases, whereas heroin powder was found in 18% of the total cases. Heroin was sniffed in only 9% of cases, which indicates that injection is the main route of heroin administration in Saudi Arabia.
Table 6 indicates that the median morphine BNaF concentration when the drug was administered via injection was 300 ng/mL, followed by sniffing at 150 ng/mL and an unknown route of administration at 220 ng/mL (
Table 5). The highest BNaF morphine concentrations (340 ng/mL and 310 ng/mL) were observed when heroin powder and syringes were found near the deceased, respectively. In cases where both syringes and heroin powder were discovered, the median BNaF morphine concentration was 400 ng/mL. No differences were observed in the median vitreous humor concentration among the three routes of administration, with a median of 90–120 ng/mL in all groups. The heroin powder group showed a slightly higher morphine vitreous humor concentration, followed by cases with syringes and heroin bags at 160 ng/mL and 140 ng/mL, respectively (
Table S5). In contrast, the median urine morphine concentration was higher in cases of injected heroin (2400 ng/mL) than in the sniffing heroin group (1400 ng/mL). The median bile morphine concentration was almost double in the sniffing group (4200 ng/mL) than in the injection group (1600 ng/mL).
3.2.8. Location of Deaths and Putrefaction
Most heroin deaths occurred in outdoor environments (63%), with a median PMI of 48 h, whereas 37% of the patients died in a private home (
Table 6), with a median PMI of 24 h. A higher median BNaF morphine level was observed in those who died indoors (320 ng/mL) than outdoors (240 ng/mL), while the level in vitreous humor was similar (100 ng/mL vs. 80 ng/mL, respectively). In contrast, the median urine and bile morphine concentrations were two- and three-fold higher among those who died outdoors than indoors, respectively.
It has been mentioned that the weather in Saudi Arabia is extremely hot most of the year, and the weather in Jeddah is known to be highly humid. Accordingly, it is well-known that putrefaction and postmortem changes would begin a few hours following death if bodies were not stored appropriately [
32,
33]. In cases in which heroin was injected and the person dies alone in a closed indoor area, putrefaction will occur faster owing to the combination of hot weather and high humidity in Jeddah city. Considering that most of the deceased die indoors and are discovered in a closed toilet, garage, or hidden area at home, such as the roof, this could facilitate postmortem changes, especially when deaths occur at night with no witnesses. In contrast, a deceased body on the street (outdoor) would be easily discovered unless it was moved to an empty or deserted area.
In 63 out of 97 cases (65%), police and forensic pathologist reports indicated that no witnesses observed the final moments before death (
Table S5). Nine patients (11%) were transferred to the hospital; however, most patients died either at the scene before transfer to the hospital or during transfer to the hospital. Identifying the mode of death was difficult due to a lack of information and heavy decomposition of the bodies, especially for those who died outdoors, in the desert, under construction bridges, or in old buildings. In 8 of the 97 cases, the manner of death was unknown due to putrefaction, and these cases presented a median BNaF morphine concentration of 380 ng/mL, a PMI of 230 h, and an age of 40. High morphine concentrations can be explained by the administration of a high dose or due to postmortem changes after death that cause the conversion of 6-MAM and morphine conjugates to free morphine.
In this study, higher BNaF morphine concentrations were measured in patients whose deaths were pronounced at hospitals (n = 9 cases, 450 ng/mL), followed by those found in the street (n = 9 cases, 335 ng/mL), under bridges (n = 11 cases, 262 ng/mL), in cars (n = 17, 240 ng/mL), in rental flats or hotel rooms (n = 7, 237 ng/mL), and in deserted areas (n = 8 cases, 170 ng/mL). PMI, environmental conditions (location of death and weather), and patient tolerance have major effects on the detection of heroin biomarkers and metabolites. The patients who died at the hospital had a lower PMI, and their deaths were caused by an overdose of heroin alone. In contrast, among individuals who died under bridges, most cases showed putrefaction, and 6 out of 10 cases were polydrug intoxication cases. Notably, a high number of deaths occurred in cars, with 13 out of 17 cases of polydrug intoxication having a relatively low PMI (median 24 h) and 6 cases exhibiting signs of putrefaction, with two heavily putrefied. Vitreous humor and urine were available in 13 and 12 of these cases, respectively, and 6-MAM and 6-AC were detected in 6 and 9 cases, respectively. Only one case was positive for both heroin biomarkers in bile. A higher median of BNaF morphine was observed compared to vitreous humor (60 ng/mL), which suggested a shorter survival time. This was supported by the lower urine morphine concentration (860 ng/mL) and highest bile morphine concentration (9800 ng/mL), suggesting a chronic heroin user.
Twenty-one cases showed signs of putrefaction (
Table 6), 60% showed partial purification, and 8 out of 21 putrefied cases showed heavy decomposition. There was no difference in age between the two groups; however, the PMIs were higher in the heavily putrefied group (heavy putrefaction: 228 h; partial putrefaction: 96 h;
Table 6). 6-MAM was detected in BNaF in two cases in each group. The advantages of testing alternative specimens in determining the source of opioids have been clearly observed in these putrefaction cases because most of the alternative samples, namely urine, vitreous humor, and bile, were positive for 6-MAM. A few cases that showed partial putrefaction tested positive for 6-AC.
3.2.9. Seasonal Distribution
The seasonal distribution of heroin-related fatalities is presented in
Table S6 and
Figure S3. The highest proportion occurred in spring (29%), followed by summer (28%), winter (27%), and autumn (16%). The highest mortality rate occurred in July (12%), followed by April (11%). The lowest proportion of heroin fatalities (4 %) occurred in October.
3.2.10. Multiple Specimens
The median morphine concentrations in the BNaF, urine, vitreous humor, and bile samples were 280, 1400, 90, and 2200 ng/mL, respectively. Among the available BNaF, urine, vitreous humor, and bile specimens, 6-MAM was detected in 60%, 100%, 99%, and 59%, while 6-AC was detected in 24%, 68%, 50%, and 30%, respectively. The presence of sodium fluoride in the blood test tube as a preservative prevented 6-MAM from converting to morphine in most cases. Additionally, the availability of urine, bile, and vitreous humor samples provides valuable information on the opioids that have been administered. The median free morphine concentration ratios among the vitreous humor/BNaF, urine/BNaF, and bile/BNaF were 0.37-fold (n = 63), 5.6-fold (n = 64), and 7.3-fold (n = 23), respectively. In addition, free morphine/free codeine were always higher than 1, with median ratios of 13-fold (n = 84), 13-fold (n = 70), 6-fold (n = 68), and 85-fold (n = 25) for BNaF, urine, vitreous humor, and bile, respectively.
The Spearman correlation coefficient (R) was used to establish the relationship between heroin biomarkers, morphine, and codeine concentrations in various body fluids (
Table S7). 6-MAM in BNaF exhibited a strong positive correlation with the analytes of interest in both the urine and vitreous humor, except for 6-MAM in BNaF vs. 6-AC in the vitreous humor. In contrast, the correlation between 6-MAM in BNaF and analytes of interest in bile was weakly positive for 6-MAM, 6-AC, and codeine but negative for morphine (non-significant
p-values higher than 0.5). The correlation between the 6-AC concentration obtained from multiple biological fluids was always poor and not statistically significant, and it was not calculated for bile due to the lack of positive samples. A negative correlation was observed between 6-AC and morphine in bile and analytes of interest in the BNaF, urine, and vitreous humor samples, as shown in
Table S7. The poor correlation between 6-AC in the different specimens could be explained by the low concentrations, small sample size, and instability of 6-AC in biological specimens. The 6-AC concentrations in BNaF were not significantly correlated with the analytes of interest in the urine and bile, while a significant correlation was obtained with the analytes of interest in the vitreous humor.
Good correlations were obtained between the analytes of interest detected in BNaF vs. vitreous humor, BNAF vs. urine, and vitreous humor vs. urine. The level of 6-AC seemed to be higher in the vitreous humor than the blood, which can directly reflect the anatomical location of the vitreous humor; thus, 6-AC in the vitreous humor is more stable and has a longer half-life before conversion to codeine than that in blood samples.
The bile samples showed the lowest positive results for 6-AC (eight cases) compared to 6-MAM. The 6-MAM was detected in 16 of the 27 bile samples tested in this study. Although the correlation between heroin-related compounds in BNaF and bile was weak, the correlation between these analytes in bile and their corresponding specimens in vitreous humor and urine was strong, except for the 6-AC concentration.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}