
Is Stress Taking the Pleasure Out of Food?—A Characterization of the Food Pleasure Profiles, Appetite, and Eating Behaviors of People with Chronic Stress

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
1.1. What Is ‘Stress’?
1.2. Stress-Induced Eating and Altered Perception of Reward
1.3. Purpose of this Study
- How consumers suffering from varying degrees of chronic stress perceived pleasure from food and food experiences.
- How the perception of pleasure from food, by this specific consumer group, is demonstrated in their sense of appetite, food preferences, and eating behavior.
2. Materials and Methods
2.1. Data Collection
2.2. Participants and Recruitment
2.3. Data Analysis
3. Results
3.1. Sociodemographic and Lifestyle Characteristics of the Two Groups
3.2. Perception of Pleasure
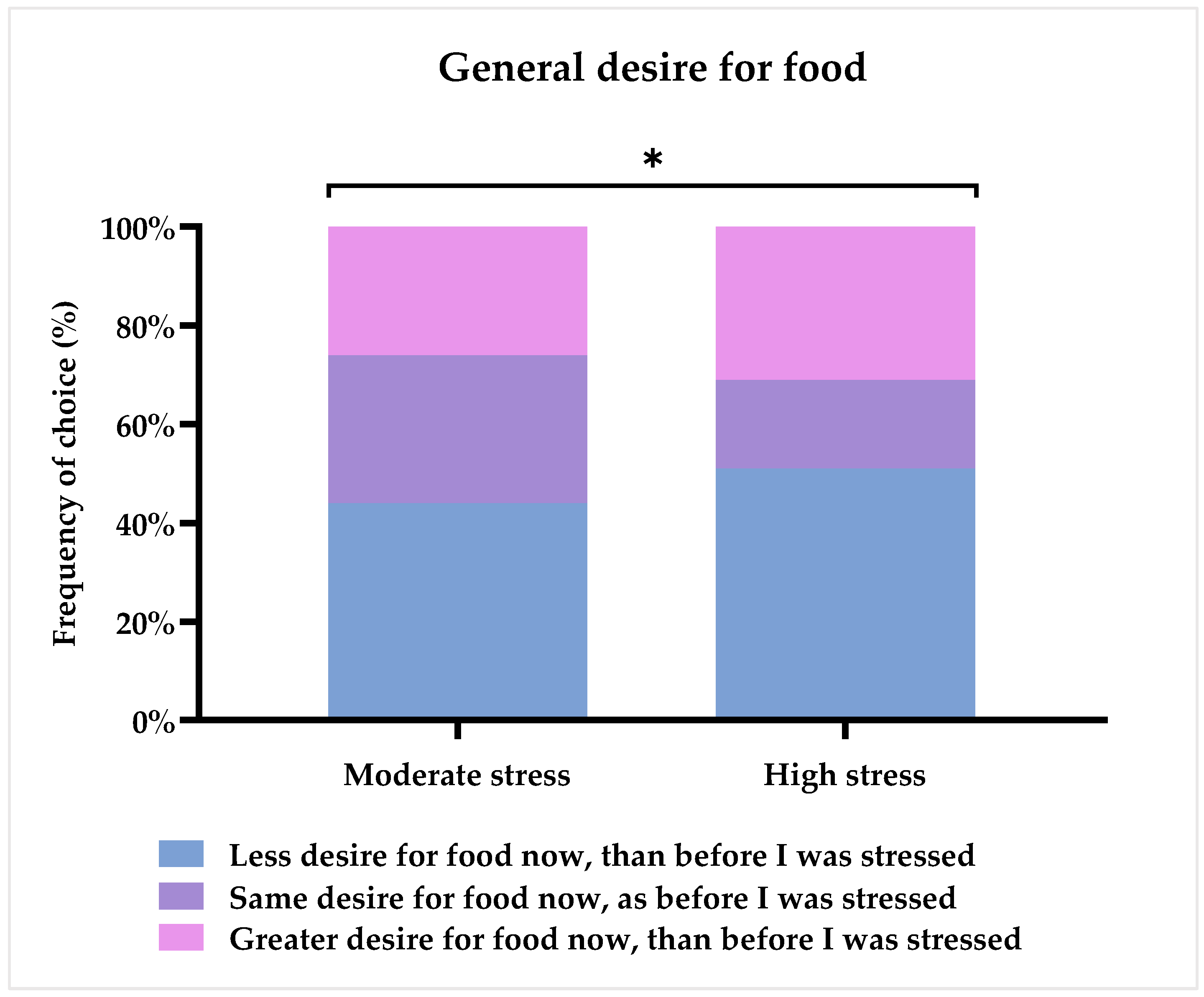
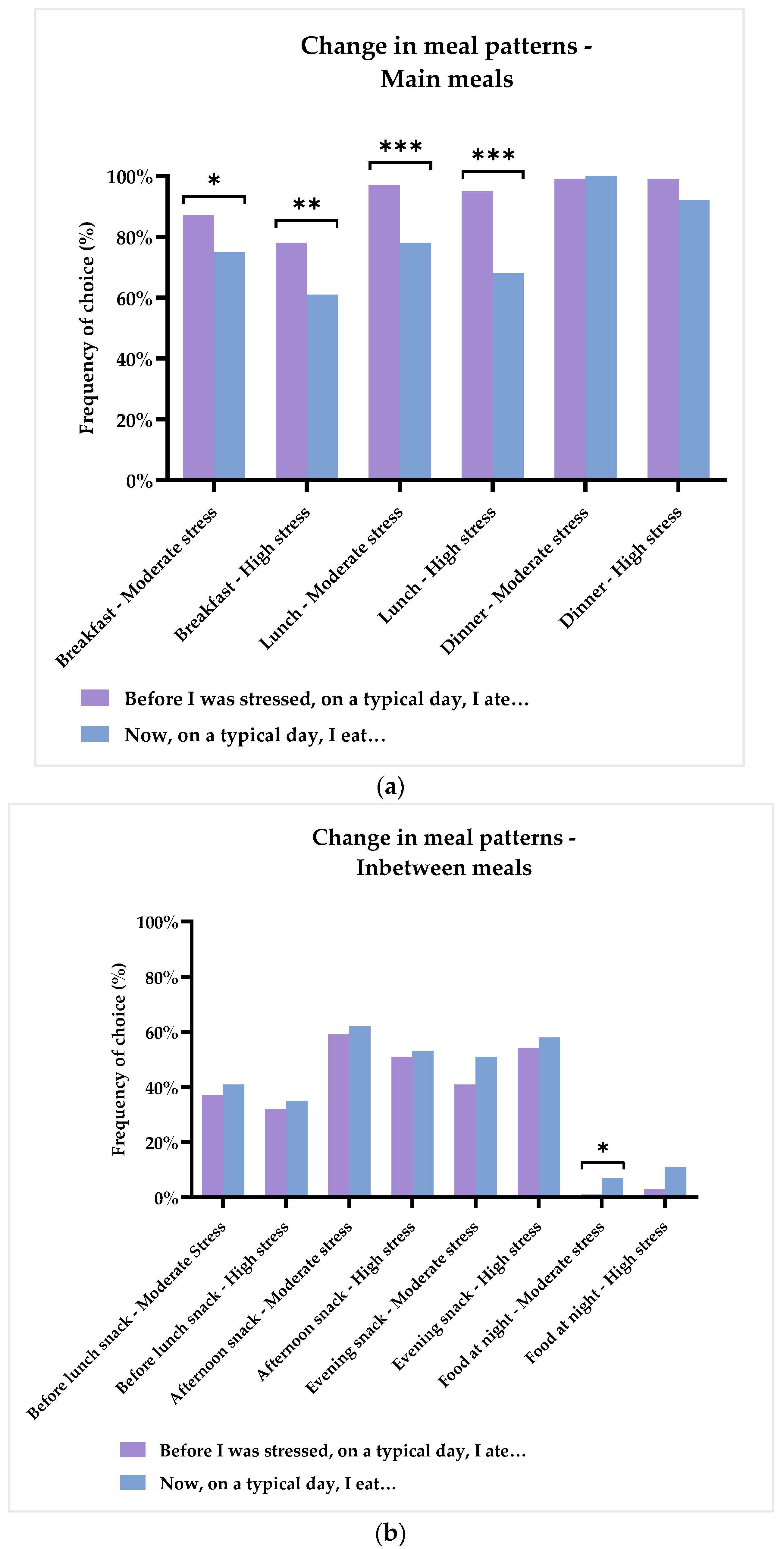
3.3. Appetite and Meal Patterns
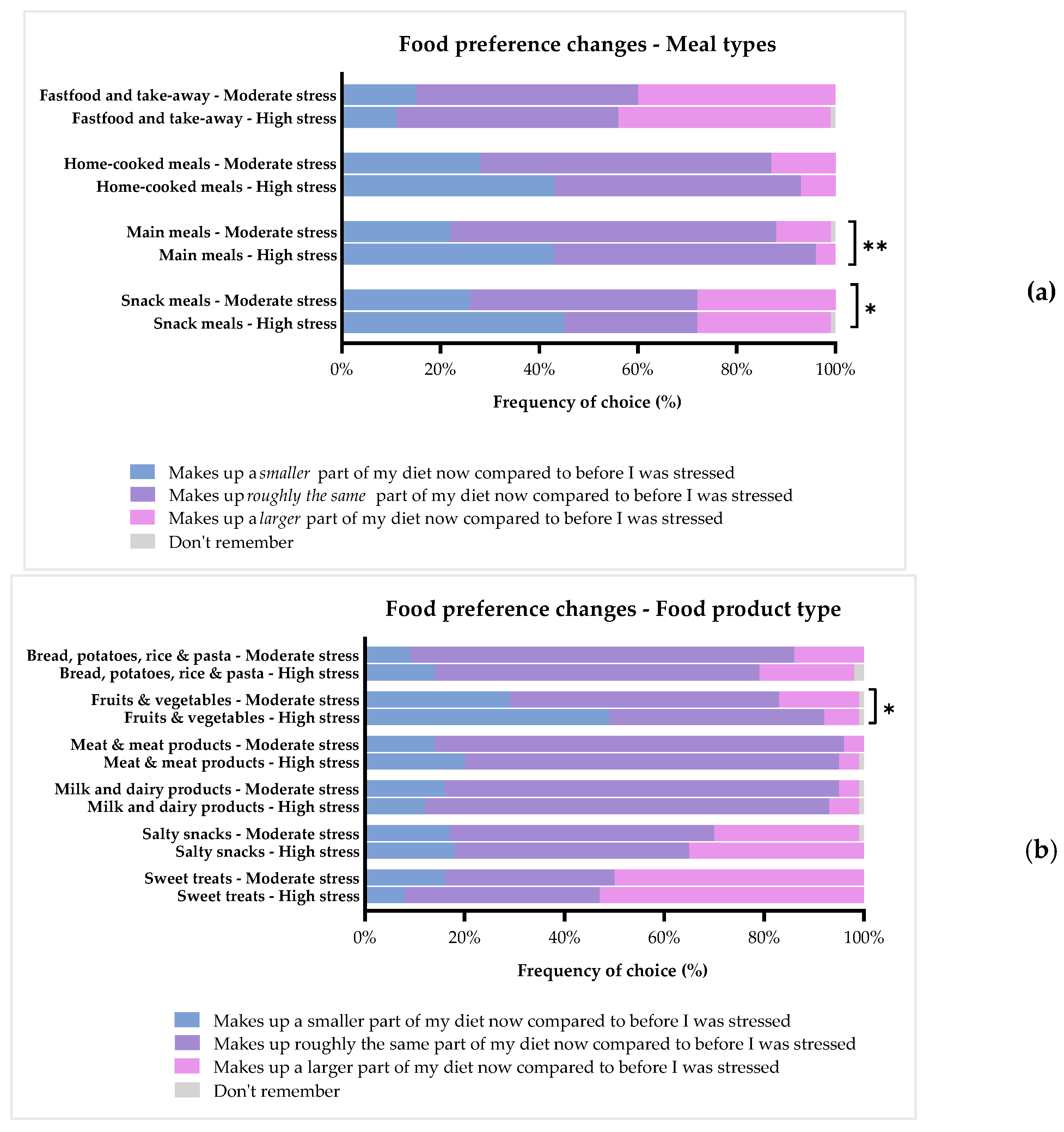
3.4. Specific Food Preferences
3.4.1. Meal Types
3.4.2. Food Product Types
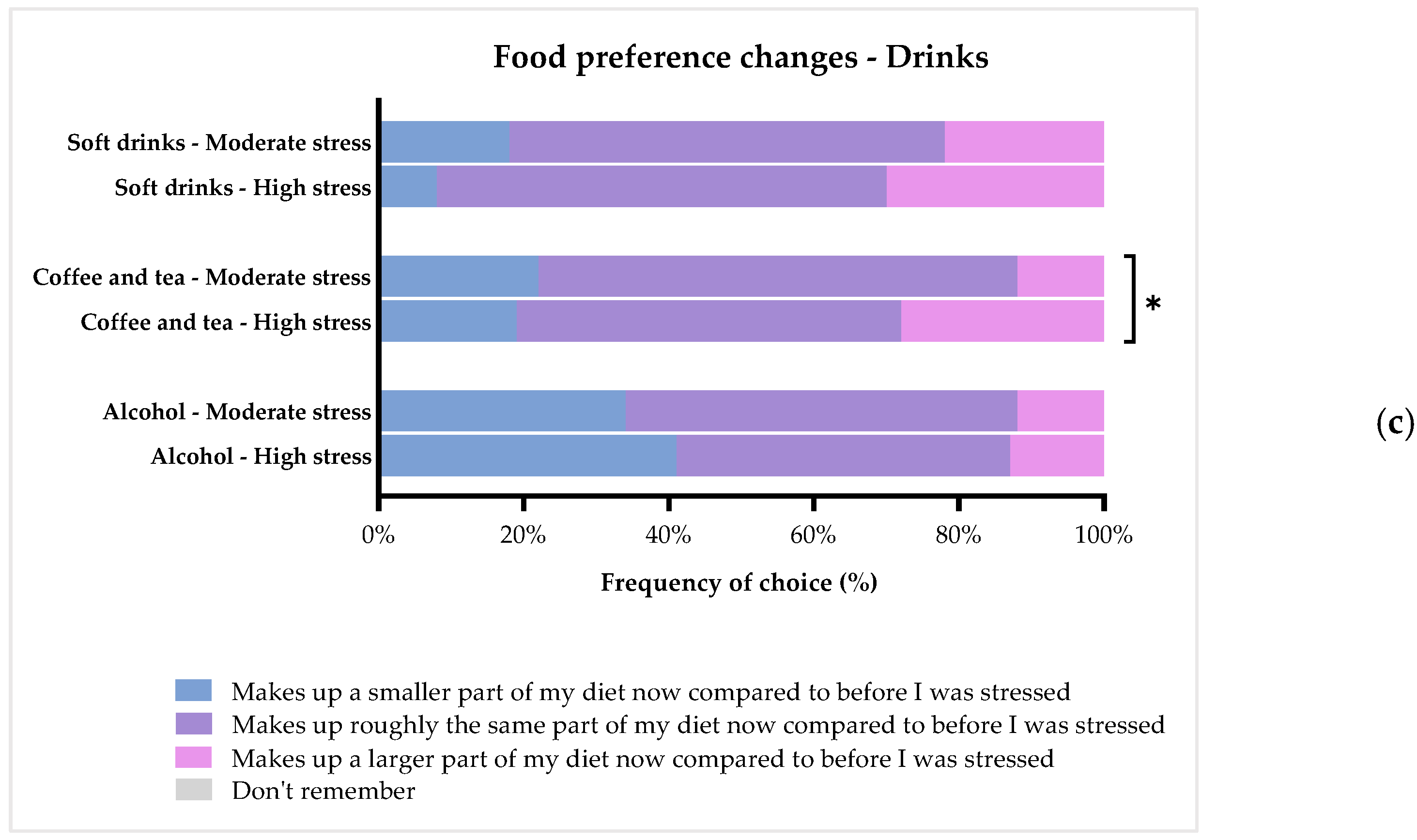
3.4.3. Drinks
4. Discussion
4.1. Altered Hedonic Tone and Food-Related Pleasure as a Consequence of Stress
4.2. The Effect of Chronic Stress on Appetite, Meal Patterns, and Food Preferences
4.3. Implications
4.4. Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brinkmann, S. Stress i Arbejdslivet: Konstitueringen Af En Epidemi. In Nye Perspektiver på Stress; Andersen, M.F., Brinkmann, S., Eds.; Klim: Aarhus, Denmark, 2013; pp. 75–92. ISBN 9788771291674. [Google Scholar]
- Selye, H. History of the Stress Concept. In Handbook of Stress: Theoretical and Clinical Aspects, 2nd ed.; Free Press: New York, NY, USA, 1993; pp. 7–17. ISBN 0-02-912035-7 (Hardcover); 0-02-912036-5 (Paperback). [Google Scholar]
- Rod, N.H. Stress og helbred: Årsager, helbredskonsekvenser og social ulighed, 1st ed.; Munksgaard: Copenhagen, Denmark, 2017; ISBN 978-87-628-1586-5. [Google Scholar]
- Kompier, M.A.J. New systems of work organization and workers’ health. Scand. J. Work. Environ. Health 2006, 32, 421–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosa, H. Fremmedgørelse og Acceleration, 1st ed.; Hans Reitzels Forlag: Copenhagen, Denmark, 2014; ISBN 9788741257716. [Google Scholar]
- Becker, D. One Nation under Stress: Social Uses of the Stress Concept; Oxford University Press: New York, NY, USA, 2013; ISBN 9780199742912. [Google Scholar]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, T.C.; Epel, E.S. Stress, eating and the reward system. Physiol. Behav. 2007, 91, 449–458. [Google Scholar] [CrossRef]
- Epel, E.S.; Crosswell, A.D.; Mayer, S.E.; Prather, A.A.; Slavich, G.M.; Puterman, E.; Mendes, W.B. More than a feeling: A unified view of stress measurement for population science. Front. Neuroendocr. 2018, 49, 146–169. [Google Scholar] [CrossRef]
- Andersen, L.P. Arbejdsrelateret stress—Fra symptomer til et komplekst samspil. Tidsskr. Arb. 2007, 9, 11. [Google Scholar] [CrossRef]
- Cohen, S.; Gianaros, P.J.; Manuck, S.B. A Stage Model of Stress and Disease. Perspect. Psychol. Sci. 2016, 11, 456–463. [Google Scholar] [CrossRef]
- Cohen, S.; Murphy, M.L.; Prather, A.A. Ten Surprising Facts about Stressful Life Events and Disease Risk. Annu. Rev. Psychol. 2019, 70, 577–597. [Google Scholar] [CrossRef]
- McEwen, B.S. Protective and Damaging Effects of Stress Mediators. N. Engl. J. Med. 1998, 338, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef]
- Cohen, S.; Doyle, W.J.; Alper, C.M.; Janicki-Deverts, D.; Turner, R.B. Sleep Habits and Susceptibility to the Common Cold. Arch. Intern. Med. 2009, 169, 62–67. [Google Scholar] [CrossRef] [Green Version]
- Sinha, R.; Jastreboff, A.M. Stress as a Common Risk Factor for Obesity and Addiction. Biol. Psychiatry 2013, 73, 827–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomiyama, A.J. Stress and Obesity. Annu. Rev. Psychol. 2019, 70, 703–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Loughlin, I.; Newton-John, T.R. ‘Dis-comfort eating’: An investigation into the use of food as a coping strategy for the management of chronic pain. Appetite 2019, 140, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.L. Emotional influences on food choice: Sensory, physiological and psychological pathways. Physiol. Behav. 2006, 89, 53–61. [Google Scholar] [CrossRef]
- Wallis, D.; Hetherington, M. Emotions and eating. Self-reported and experimentally induced changes in food intake under stress. Appetite 2009, 52, 355–362. [Google Scholar] [CrossRef]
- Ans, A.H.; Anjum, I.; Satija, V.; Inayat, A.; Asghar, Z.; Akram, I.; Shrestha, B. Neurohormonal Regulation of Appetite and its Relationship with Stress: A Mini Literature Review. Cureus 2018, 10, e3032. [Google Scholar] [CrossRef] [Green Version]
- Epel, E.; Lapidus, R.; McEwen, B.; Brownell, K. Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology 2000, 26, 37–49. [Google Scholar] [CrossRef]
- Oliver, G.; Wardle, J. Perceived Effects of Stress on Food Choice. Physiol. Behav. 1999, 66, 511–515. [Google Scholar] [CrossRef]
- Finch, L.E.; Tiongco-Hofschneider, L.; Tomiyama, A.J. Stress-Induced Eating Dampens Physiological and Behavioral Stress Responses. In Nutrition in the Prevention and Treatment of Abdominal Obesity; Elsevier: Amsterdam, The Netherlands, 2019; pp. 175–187. ISBN 9780128160930. [Google Scholar]
- Finlayson, G.; King, N.; Blundell, J.E. Liking vs. wanting food: Importance for human appetite control and weight regulation. Neurosci. Biobehav. Rev. 2007, 31, 987–1002. [Google Scholar] [CrossRef] [Green Version]
- Berridge, K.C.; Kringelbach, M.L. Pleasure Systems in the Brain. Neuron 2015, 86, 646–664. [Google Scholar] [CrossRef] [Green Version]
- Havermans, R.C. “You Say it’s Liking, I Say it’s Wanting …”. On the difficulty of disentangling food reward in man. Appetite 2011, 57, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Berridge, K.C. ‘Liking’ and ‘wanting’ food rewards: Brain substrates and roles in eating disorders. Physiol. Behav. 2009, 97, 537–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berridge, K.C.; Ho, C.-Y.; Richard, J.M.; DiFeliceantonio, A.G. The tempted brain eats: Pleasure and desire circuits in obesity and eating disorders. Brain Res. 2010, 1350, 43–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.J.; Beilharz, J.E.; Maniam, J.; Reichelt, A.C.; Westbrook, R.F. Why is obesity such a problem in the 21st century? The intersection of palatable food, cues and reward pathways, stress, and cognition. Neurosci. Biobehav. Rev. 2015, 58, 36–45. [Google Scholar] [CrossRef]
- Ruddock, H.K.; Hardman, C.A. Guilty pleasures: The effect of perceived overeating on food addiction attributions and snack choice. Appetite 2018, 121, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomsen, K.R.; Whybrow, P.C.; Kringelbach, M.L. Reconceptualizing anhedonia: Novel perspectives on balancing the pleasure networks in the human brain. Front. Behav. Neurosci. 2015, 9, 49. [Google Scholar] [CrossRef] [Green Version]
- Gard, D.E.; Gard, M.G.; Kring, A.M.; John, O.P. Anticipatory and consummatory components of the experience of pleasure: A scale development study. J. Res. Pers. 2006, 40, 1086–1102. [Google Scholar] [CrossRef]
- Stanton, C.H.; Holmes, A.J.; Chang, S.W.; Joormann, J. From Stress to Anhedonia: Molecular Processes through Functional Circuits. Trends Neurosci. 2018, 42, 23–42. [Google Scholar] [CrossRef]
- Pizzagalli, D.A.; Bogdan, R.; Ratner, K.G.; Jahn, A.L. Increased perceived stress is associated with blunted hedonic capacity: Potential implications for depression research. Behav. Res. Ther. 2007, 45, 2742–2753. [Google Scholar] [CrossRef] [Green Version]
- Fawcett, J.; Clark, D.C.; Scheftner, W.A.; Gibbons, R.D. Assessing Anhedonia in Psychiatric Patients. Arch. Gen. Psychiatry 1983, 40, 79–84. [Google Scholar] [CrossRef]
- Chapman, L.J.; Chapman, J.P.; Raulin, M.L. Scales for physical and social anhedonia. J. Abnorm. Psychol. 1976, 85, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Snaith, R.P.; Hamilton, M.; Morley, S.; Humayan, A.; Hargreaves, D.; Trigwell, P. A Scale for the Assessment of Hedonic Tone the Snaith–Hamilton Pleasure Scale. Br. J. Psychiatry 1995, 167, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Hyldelund, N.B.; Worck, S.; Olsen, A. Convenience may increase vegetable intake among young consumers. Food Qual. Prefer. 2020, 83, 103925. [Google Scholar] [CrossRef]
- Andersen, B.V.; Chan, R.C.K.; Byrne, D.V. A Conceptual Framework for Multi-Dimensional Measurements of Food Related Pleasure—The Food Pleasure Scale. Foods 2021, 10, 2044. [Google Scholar] [CrossRef] [PubMed]
- Hyldelund, N.B.; Dalgaard, V.L.; Byrne, D.V.; Andersen, B.V. Why Being ‘Stressed’ Is ‘Desserts’ in Reverse—The Effect of Acute Psychosocial Stress on Food Pleasure and Food Choice. Foods 2022, 11, 1756. [Google Scholar] [CrossRef] [PubMed]
- Finch, L.E.; Cummings, J.R.; Tomiyama, A.J. Cookie or clementine? Psychophysiological stress reactivity and recovery after eating healthy and unhealthy comfort foods. Psychoneuroendocrinology 2019, 107, 26–36. [Google Scholar] [CrossRef]
- Masih, T.; Dimmock, J.; Epel, E.S.; Guelfi, K. Stress-induced eating and the relaxation response as a potential antidote: A review and hypothesis. Appetite 2017, 118, 136–143. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Eskildsen, A.; Dalgaard, V.L.; Nielsen, K.J.; Andersen, J.H.; Zachariae, R.; Olsen, L.R.; Jã¸rgensen, A.; Christiansen, D. Cross-cultural adaptation and validation of the Danish consensus version of the 10-item Perceived Stress Scale. Scand. J. Work. Environ. Health 2015, 41, 486–490. [Google Scholar] [CrossRef]
- Franken, I.H.; Rassin, E.; Muris, P. The assessment of anhedonia in clinical and non-clinical populations: Further validation of the Snaith–Hamilton Pleasure Scale (SHAPS). J. Affect. Disord. 2007, 99, 83–89. [Google Scholar] [CrossRef]
- Rizvi, S.J.; Quilty, L.C.; Sproule, B.A.; Cyriac, A.; Bagby, R.M.; Kennedy, S.H. Development and validation of the Dimensional Anhedonia Rating Scale (DARS) in a community sample and individuals with major depression. Psychiatry Res. 2015, 229, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Compusense Inc. Compusense20. Available online: www.compusense.com (accessed on 20 April 2022).
- Retsinformation.dk Act on Research Ethics Review of Health Research Projects. Available online: https://www.retsinformation.dk/eli/lta/2017/1083 (accessed on 20 April 2022).
- Rstudio Team. RStudio: Integrated Development for R 2022; RStudio, Inc.: Boston, MA, USA, 2015. [Google Scholar]
- Jensen, H.A.R.; Davidsen, M.; Møller, S.R.; Román, J.E.I.; Kragelund, K.; Christensen, A.I.; Ekholm, O. Danskernes Sundhed—Den Nationale Sundhedsprofil 2021; Statens Institut for Folkesundhed: København, Denmark, 2022; Available online: https://www.sst.dk/-/media/Udgivelser/2022/Sundhedsprofil/Sundhedsprofilen.ashx?sc_lang=da&hash=5C9A9A81483F6C987D5651976B72ECB2 (accessed on 10 June 2022).
- World Health Organization (WHO). Depression and Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Hatzigiakoumis, D.S.; Martinotti, G.; Di Giannantonio, M.; Janiri, L. Anhedonia and Substance Dependence: Clinical Correlates and Treatment Options. Front. Psychiatry 2011, 2, 10. [Google Scholar] [CrossRef] [Green Version]
- Nakonezny, P.A.; Morris, D.W.; Greer, T.L.; Byerly, M.J.; Carmody, T.J.; Grannemann, B.D.; Bernstein, I.H.; Trivedi, M.H. Evaluation of anhedonia with the Snaith–Hamilton Pleasure Scale (SHAPS) in adult outpatients with major depressive disorder. J. Psychiatr. Res. 2015, 65, 124–130. [Google Scholar] [CrossRef]
- Andersen, B.V.; Brockhoff, P.B.; Hyldig, G. The importance of liking of appearance, -odour, -taste and -texture in the evaluation of overall liking. A comparison with the evaluation of sensory satisfaction. Food Qual. Prefer. 2018, 71, 228–232. [Google Scholar] [CrossRef] [Green Version]
- Cardello, A.V.; Schutz, H.; Snow, C.; Lesher, L. Predictors of food acceptance, consumption and satisfaction in specific eating situations. Food Qual. Prefer. 2000, 11, 201–216. [Google Scholar] [CrossRef]
- Köster, E.P. Diversity in the determinants of food choice: A psychological perspective. Food Qual. Prefer. 2009, 20, 70–82. [Google Scholar] [CrossRef]
- Andersen, B.; Hyldig, G. Food satisfaction: Integrating feelings before, during and after food intake. Food Qual. Prefer. 2015, 43, 126–134. [Google Scholar] [CrossRef]
- Duerlund, M.; Andersen, B.V.; Alexi, N.; Peng, M.; Byrne, D.V. Subjective Sensations related to Food as Determinants of Snack Choice. Foods 2020, 9, 336. [Google Scholar] [CrossRef] [Green Version]
- Hyldelund, N.B.; Byrne, D.V.; Chan, R.C.; Andersen, B.V. Food pleasure across nations: A comparison of the drivers between Chinese and Danish populations. Food Qual. Prefer. 2021, 97, 104493. [Google Scholar] [CrossRef]
- Hyldelund, N.B.; Byrne, D.V.; Andersen, B.V. Food Pleasure Profiles—An Exploratory Case Study of the Relation between Drivers of Food Pleasure and Lifestyle and Personality Traits in a Danish Consumer Segment. Foods 2022, 11, 718. [Google Scholar] [CrossRef]
- Lawless, H.T.; Heymann, H. Introduction. In Sensory Evaluation of Food: Principles and Practices, 2nd ed.; Lawless, H.T., Heymann, H., Eds.; Springer Science and Business Media: New York, NY, USA, 2010; pp. 1–2. ISBN 978-1-4419-6487-8. [Google Scholar]
- Maslow, A.H. Motivation and Personality, 2nd ed.Harper & Row: New York, NY, USA, 1970; ISBN 0060442417 9780060442415. [Google Scholar]
- Tomiyama, A.J.; Finch, L.E.; Cummings, J.R. Did That Brownie Do Its Job? Stress, Eating, and the Biobehavioral Effects of Comfort Food. Emerg. Trends Soc. Behav. Sci. 2015, 1–15. [Google Scholar] [CrossRef]
- Pelizza, L.; Ferrari, A. Anhedonia in schizophrenia and major depression: State or trait? Ann. Gen. Psychiatry 2009, 8, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucas, M. Coffee, Caffeine, and Risk of Depression among Women. Arch. Intern. Med. 2011, 171, 1571–1578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, T.L.; Vickers, R.R.; Ward, H.W.; Rahe, R.H. Occupational Stress and Variation in Cigarette, Coffee, and Alcohol Consumption. J. Health Soc. Behav. 1981, 22, 155. [Google Scholar] [CrossRef]
- Schreiber, G.B.; Robins, M.; Maffeo, C.E.; Masters, M.N.; Bond, A.P.; Morganstein, D. Confounders contributing to the reported associations of coffee or caffeine with disease. Prev. Med. 1988, 17, 295–309. [Google Scholar] [CrossRef]
- Alasmari, F. Caffeine induces neurobehavioral effects through modulating neurotransmitters. Saudi Pharm. J. 2020, 28, 445–451. [Google Scholar] [CrossRef]
- Garrett, B.E.; Griffiths, R.R. The Role of Dopamine in the Behavioral Effects of Caffeine in Animals and Humans. Pharmacol. Biochem. Behav. 1997, 57, 533–541. [Google Scholar] [CrossRef]
- van der Valk, E.S.; Savas, M.; van Rossum, E.F.C. Stress and Obesity: Are There More Susceptible Individuals? Curr. Obes. Rep. 2018, 7, 193–203. [Google Scholar] [CrossRef] [Green Version]
- Fadnes, L.; Taube, A. How to identify information bias due to self-reporting in epidemiological research. Internet J. Epidemiol. 2009, 7, 28–38. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Title |
|---|---|
| ntotal | 190 |
| Males/females (%) | 35 (18%)/155 (82%) |
| Age (years) * | 44.61 ± 11.31 (23–67) |
| Educational level | |
| Primary school (%) | 5 (3%) |
| High school (%) | 12 (6%) |
| Vocational education (%) | 43 (22%) |
| Short higher Education (%) | 28 (14%) |
| Medium higher Education (%) | 68 (36%) |
| Long higher Education (%) | 33 (17%) |
| PhD | 1 (1%) |
| BMI (kg/m2) 1,* | 28.00 ± 6.40 (18–53) |
| Perceived Stress Scale (PSS-10) 2 | |
| Moderate stress (%) | 116 (61%) |
| High stress (%) | 74 (39%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyldelund, N.B.; Frederiksen, C.; Byrne, D.V.; Andersen, B.V. Is Stress Taking the Pleasure Out of Food?—A Characterization of the Food Pleasure Profiles, Appetite, and Eating Behaviors of People with Chronic Stress. Foods 2022, 11, 1980. https://doi.org/10.3390/foods11131980
Hyldelund NB, Frederiksen C, Byrne DV, Andersen BV. Is Stress Taking the Pleasure Out of Food?—A Characterization of the Food Pleasure Profiles, Appetite, and Eating Behaviors of People with Chronic Stress. Foods. 2022; 11(13):1980. https://doi.org/10.3390/foods11131980
Chicago/Turabian StyleHyldelund, Nikoline Bach, Chanette Frederiksen, Derek Victor Byrne, and Barbara Vad Andersen. 2022. "Is Stress Taking the Pleasure Out of Food?—A Characterization of the Food Pleasure Profiles, Appetite, and Eating Behaviors of People with Chronic Stress" Foods 11, no. 13: 1980. https://doi.org/10.3390/foods11131980