Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Interventions and Outcomes
2.4. Sample Size
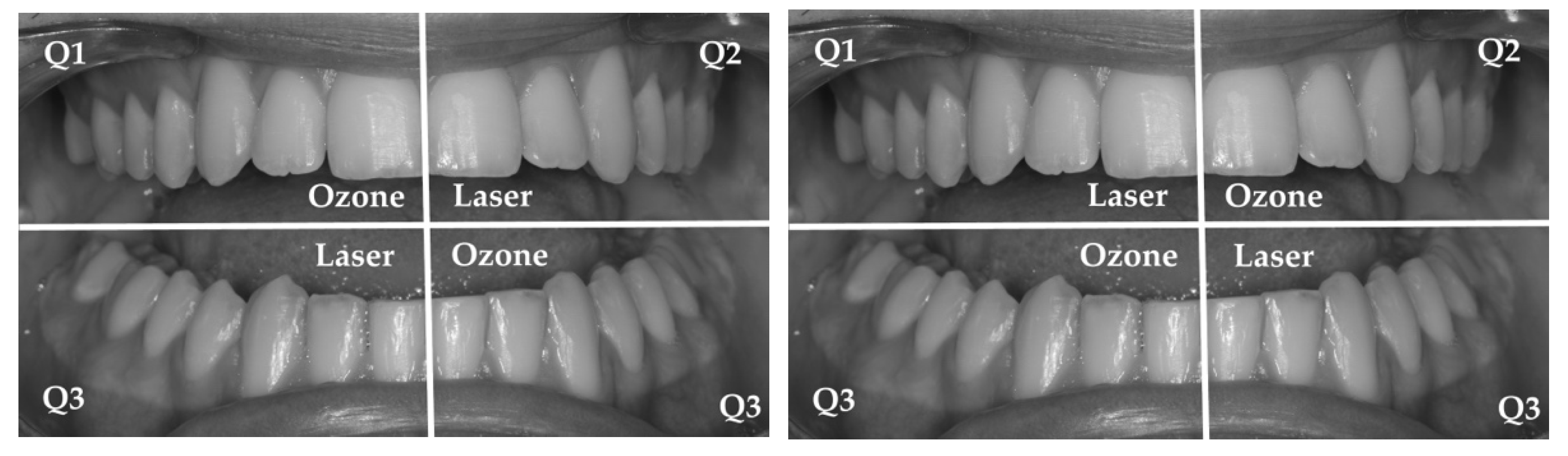
2.5. Randomization and Blinding
2.6. Statistical Methods
3. Results
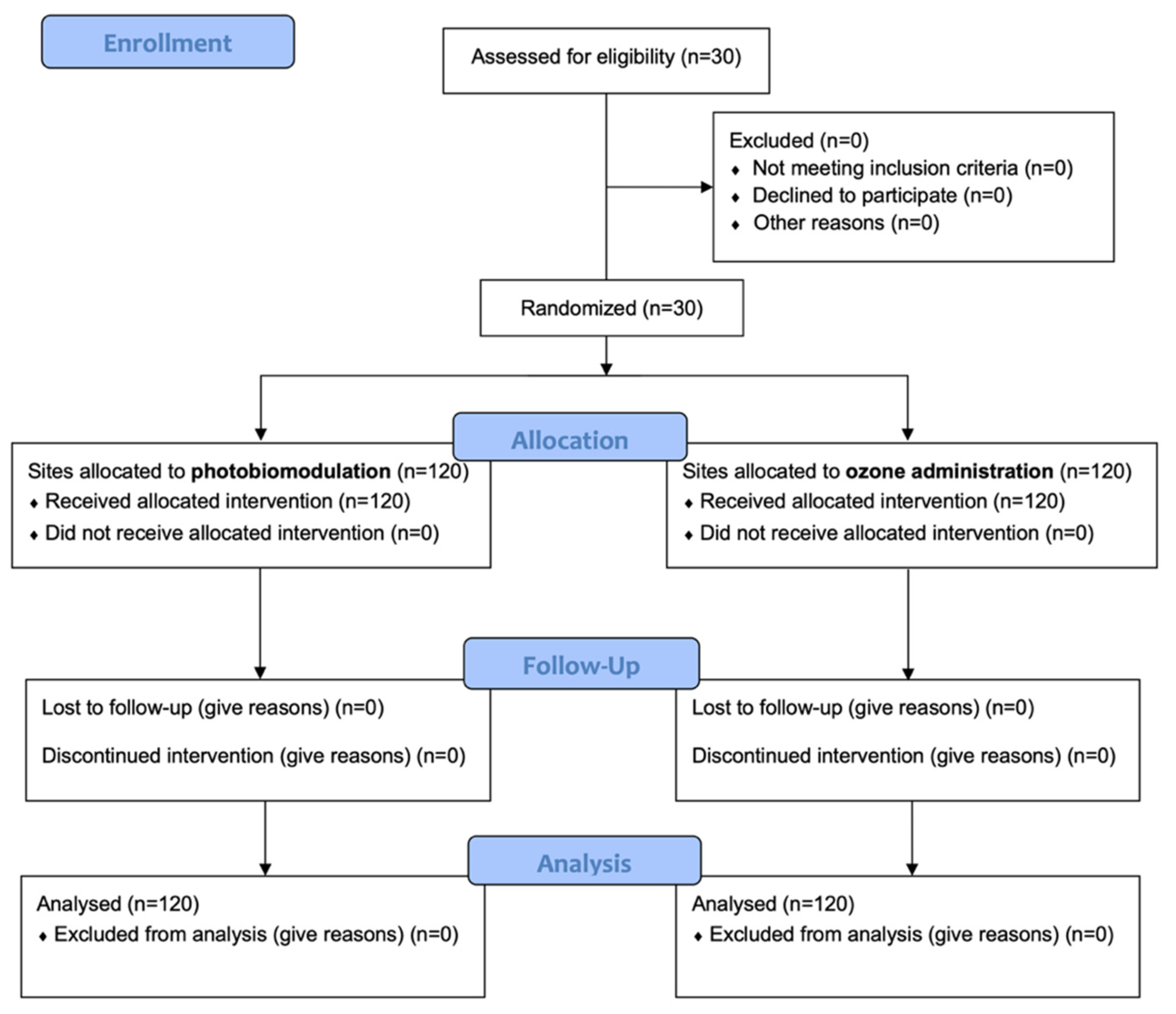
3.1. Participant Flow and Baseline Data
3.2. Probing Pocket Depth (PPD)
3.3. Plaque Index (PI%)
3.4. Bleeding on Probing (BoP)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [Green Version]
- Kinane, D.F.; Chestnutt, I.G. Smoking and periodontal disease. Crit. Rev. Oral Biol. Med. 2000, 11, 356–365. [Google Scholar]
- Taba, M., Jr.; Souza, S.L.; Mariguela, V.C. Periodontal disease: A genetic perspective. Braz. Oral Res. 2012, 26, 32–38. [Google Scholar] [CrossRef]
- Pólvora, T.L.S.; Nobre, Á.V.V.; Tirapelli, C.; Taba, M., Jr.; Macedo, L.D.; Santana, R.C.; Pozzetto, B.; Lourenço, A.G.; Motta, A.C.F. Relationship between human immunodeficiency virus (HIV-1) infection and chronic periodontitis. Expert Rev. Clin. Immunol. 2018, 14, 315–327. [Google Scholar] [CrossRef]
- Shapira, L.; Wilensky, A.; Kinane, D.F. Effect of genetic variability on the inflammatory response to periodontal infection. J. Clin. Periodontol. 2005, 32, 72–86. [Google Scholar] [CrossRef]
- Marsh, P.D. Dental plaque: Biological significance of a biofilm and community life-style. J. Clin. Periodontol. 2005, 32, 7–15. [Google Scholar] [CrossRef]
- Berezow, A.B.; Darveau, R.P. Microbial shift and periodontitis. Periodontology 2000 2011, 55, 36–47. [Google Scholar] [CrossRef]
- Mombelli, A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontology 2000 2018, 76, 85–96. [Google Scholar] [CrossRef]
- Feres, M. Antibiotics in the treatment of periodontal diseases: Microbiological basis and clinical applications. Ann. R. Australas. Coll. Dent. Surg. 2008, 19, 37–44. [Google Scholar]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Meimandi, M.; Talebi Ardakani, M.R.; Esmaeil Nejad, A.; Yousefnejad, P.; Saebi, K.; Tayeed, M.H. The Effect of Photodynamic Therapy in the Treatment of Chronic Periodontitis: A Review of Literature. J. Lasers Med. Sci. 2017, 8, S7–S11. [Google Scholar] [CrossRef]
- Sechi, L.A.; Lezcano, I.; Nunez, N.; Espim, M.; Duprè, I.; Pinna, A.; Molicotti, P.; Fadda, G.; Zanetti, S. Antibacterial activity of ozonized sunflower oil (Oleozon). J. Appl. Microbiol. 2001, 90, 279–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lezcano, I.; Nuñez, N.; Espino, M.; Gómez, M. Antibacterial activity of ozonized sunflower oil, oleozon, against Staphylococcus aureus and Staphylococcus epidermidis. Ozone Sci. Eng. 2000, 22, 207–214. [Google Scholar] [CrossRef]
- Mascarenhas, L.A.B.; Oliveira, F.O.; da Silva, E.S.; dos Santos, L.M.C.; de Alencar Pereira Rodrigues, L.; Neves, P.R.F.; Santos, A.Á.B.; Moreira, G.A.F.; Lobato, G.M.; Nascimento, C.; et al. Technological Advances in Ozone and Ozonized Water Spray Disinfection Devices. Appl. Sci. 2021, 11, 3081. [Google Scholar] [CrossRef]
- Giuroiu, C.L.; Andrian, S.; Stoleriu, S.; Scurtu, M.; Țănculescu, O.; Poroch, V.; Sălceanu, M. The Combination of Diode Laser and Ozonated Water in the Treatment of Complicated Pulp Gangrene. Appl. Sci. 2020, 10, 4203. [Google Scholar] [CrossRef]
- Silva, V.; Peirone, C.; Capita, R.; Alonso-Calleja, C.; Marques-Magallanes, J.A.; Pires, I.; Maltez, L.; Pereira, J.E.; Igrejas, G.; Poeta, P. Topical Application of Ozonated Oils for the Treatment of MRSA Skin Infection in an Animal Model of Infected Ulcer. Biology. 2021, 10, 372. [Google Scholar] [CrossRef]
- Di Mauro, R.; Cantarella, G.; Bernardini, R.; Di Rosa, M.; Barbagallo, I.; Distefano, A.; Longhitano, L.; Vicario, N.; Nicolosi, D.; Lazzarino, G.; et al. The Biochemical and Pharmacological Properties of Ozone: The Smell of Protection in Acute and Chronic Diseases. Int. J. Mol. Sci. 2019, 20, 634. [Google Scholar] [CrossRef] [Green Version]
- Monzillo, V.; Lallitto, F.; Russo, A.; Poggio, C.; Scribante, A.; Arciola, C.R.; Bertuccio, F.R.; Colombo, M. Ozonized Gel Against Four Candida Species: A Pilot Study and Clinical Perspectives. Materials 2020, 13, 1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, S.; Scribante, A. Ozone therapy in dentistry: From traditional applications towards innovative ones. A review of the literature. IOP Conf. Ser. Earth Environ. Sci. 2021, 707, 012001. [Google Scholar] [CrossRef]
- Colombo, M.; Gallo, S.; Garofoli, A.; Poggio, C.; Arciola, C.R.; Scribante, A. Ozone Gel in Chronic Periodontal Disease: A Randomized Clinical Trial on the Anti-Inflammatory Effects of Ozone Application. Biology 2021, 10, 625. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G.; Mansi, B. Ozone therapy in periodontics. J. Med. Life 2012, 5, 59–67. [Google Scholar]
- Merigo, E.; Rocca, J.P.; Pinheiro, A.L.B.; Fornaini, C. Photobiomodulation Therapy in Oral Medicine: A Guide for the Practitioner with Focus on New Possible Protocols. Photobiomodul. Photomed. Laser Surg. 2019, 37, 669–680. [Google Scholar] [CrossRef]
- Sfondrini, M.F.; Vitale, M.; Pinheiro, A.L.B.; Gandini, P.; Sorrentino, L.; Iarussi, U.M.; Scribante, A. Photobiomodulation and Pain Reduction in Patients Requiring Orthodontic Band Application: Randomized Clinical Trial. Biomed. Res. Int. 2020, 2020, 7460938. [Google Scholar] [CrossRef]
- Sun, G.; Tunér, J. Low-level laser therapy in dentistry. Dent. Clin. N. Am. 2004, 48, 1061–1076. [Google Scholar] [CrossRef]
- Caruso, U.; Nastri, L.; Piccolomini, R.; d’Ercole, S.; Mazza, C.; Guida, L. Use of diode laser 980 nm as adjunctive therapy in the treatment of chronic periodontitis. A randomized controlled clinical trial. New Microbiol. 2008, 31, 513–518. [Google Scholar] [PubMed]
- Saygun, I.; Nizam, N.; Ural, A.U.; Serdar, M.A.; Avcu, F.; Tözüm, T.F. Low-level laser irradiation affects the release of basic fibroblast growth factor (bFGF), insulin-like growth factor-I (IGF-I), and receptor of IGF-I (IGFBP3) from osteoblasts. Photomed. Laser Surg. 2012, 30, 149–154. [Google Scholar] [CrossRef]
- Özberk, S.S.; Gündoğar, H.; Özkaya, M.; Taner, İ.L.; Erciyas, K. The effect of photobiomodulation therapy on nonsurgical periodontal treatment in patients with type 2 diabetes mellitus: A randomized controlled, single-blind, split-mouth clinical trial. Lasers Med. Sci. 2020, 35, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Karkhanechi, M.; Chow, D.; Sipkin, J.; Sherman, D.; Boylan, R.J.; Norman, R.G.; Craig, R.G.; Cisneros, G.J. Periodontal status of adult patients treated with fixed buccal appliances and removable aligners over one year of active orthodontic therapy. Angle Orthod. 2013, 83, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Lesaffre, E.; Philstrom, B.; Needleman, I.; Worthington, H. The design and analysis of split-mouth studies: What statisticians and clinicians should know. Stat. Med. 2009, 28, 3470–3482. [Google Scholar] [CrossRef] [PubMed]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Converti, I.; Grassi, F.R.; Santacroce, L.; Topi, S.; Gnoni, A.; Scacco, S.; Scarano, A.; et al. The Effect of Gaseous Ozone Therapy in Conjunction with Periodontal Treatment on Glycated Hemoglobin Level in Subjects with Type 2 Diabetes Mellitus: An Unmasked Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 5467. [Google Scholar] [CrossRef] [PubMed]
- Fernandes-Dias, S.B.; de Marco, A.C.; Santamaria, M., Jr.; Kerbauy, W.D.; Jardini, M.A.; Santamaria, M.P. Connective tissue graft associated or not with low laser therapy to treat gingival recession: Randomized clinical trial. J. Clin. Periodontol. 2015, 42, 54–61. [Google Scholar] [CrossRef]
- Yılmaz, S.; Algan, S.; Gursoy, H.; Noyan, U.; Kuru, B.E.; Kadir, T. Evaluation of the clinical and antimicrobial effects of the Er:YAG laser or topical gaseous ozone as adjuncts to initial periodontal therapy. Photomed. Laser Surg. 2013, 31, 293–298. [Google Scholar] [CrossRef]
- Piepho, H.P. An Algorithm for a Letter-Based Representation of All-Pairwise Comparisons. J. Comput. Graph. Stat. 2004, 13, 456–466. [Google Scholar] [CrossRef]
- Scribante, A.; Poggio, C.; Gallo, S.; Riva, P.; Cuocci, A.; Carbone, M.; Arciola, C.R.; Colombo, M. In Vitro Re-Hardening of Bleached Enamel Using Mineralizing Pastes: Toward Preventing Bacterial Colonization. Materials 2020, 13, 818. [Google Scholar] [CrossRef] [Green Version]
- Deng, Z.L.; Szafrański, S.P.; Jarek, M.; Bhuju, S.; Wagner-Döbler, I. Dysbiosis in chronic periodontitis: Key microbial players and interactions with the human host. Sci. Rep. 2017, 7, 3703–3715. [Google Scholar] [CrossRef] [Green Version]
- Huth, K.C.; Quirling, M.; Lenzke, S.; Paschos, E.; Kamereck, K.; Brand, K.; Hickel, R.; Ilie, N. Effectiveness of ozone against periodontal pathogenic microorganisms. Eur. J. Oral Sci. 2011, 119, 204–210. [Google Scholar] [CrossRef]
- Gandhi, K.K.; Cappetta, E.G.; Pavaskar, R. Effectiveness of the adjunctive use of ozone and chlorhexidine in patients with chronic periodontitis. BDJ Open. 2019, 5, 17. [Google Scholar] [CrossRef] [Green Version]
- Talmaç, A.C.; Çalişir, M. Efficacy of gaseous ozone in smoking and non-smoking gingivitis patients. Ir. J. Med. Sci. 2021, 190, 325–333. [Google Scholar] [CrossRef]
- Convissar, R.; Ross, G. Photobiomodulation Lasers in Dentistry. Semin. Orthod. 2020, 26, 102–106. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Topi, S.; Gnoni, A.; Dipalma, G.; Mancini, A.; Di Domenico, M.; Tartaglia, G.M.; Scarano, A.; et al. The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 985. [Google Scholar] [CrossRef]
- Dompe, C.; Moncrieff, L.; Matys, J.; Grzech-Leśniak, K.; Kocherova, I.; Bryja, A.; Bruska, M.; Dominiak, M.; Mozdziak, P.; Skiba, T.H.I.; et al. Photobiomodulation—Underlying Mechanism and Clinical Applications. J. Clin. Med. 2020, 9, 1724. [Google Scholar] [CrossRef] [PubMed]
- Al-Rabiah, M.; Al-Hamoudi, N.; Al-Aali, K.A.; Slapar, L.; AlHelal, A.; Al Deeb, M.; Mokeem, S.A.; Vohra, F.; Abduljabbar, T. Efficacy of Scaling and Root Planing with Photobiomodulation for Treating Periodontitis in Gutka Chewers: A Randomized Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2020, 38, 545–551. [Google Scholar] [CrossRef]
- Ren, C.; McGrath, C.; Jin, L.; Zhang, C.; Yang, Y. The effectiveness of low-level laser therapy as an adjunct to non-surgical periodontal treatment: A meta-analysis. J. Periodontal. Res. 2017, 52, 8–20. [Google Scholar] [CrossRef] [Green Version]
- Dalvi, S.; Benedicenti, S.; Hanna, R. Effectiveness of Photobiomodulation as an Adjunct to Nonsurgical Periodontal Therapy in the Management of Periodontitis- A Systematic Review of in vivo Human Studies. Photochem. Photobiol. 2021, 97, 223–242. [Google Scholar] [CrossRef] [PubMed]
- Cronshaw, M.; Parker, S.; Anagnostaki, E.; Mylona, V.; Lynch, E.; Grootveld, M. Photobiomodulation and Oral Mucositis: A Systematic Review. Dent. J. 2020, 8, 87. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Instrument | Manufacturer | Parameters |
|---|---|---|
| Ozone DTA generator | Sweden & Martina, Due Carrare, PD, Italy | Power: 6 Probe type: 3 Usage: 1 min/cm2 |
| Giotto diode laser | Dental Medical Technologies, Lissone, MB, Italy | λ = 980 nm Frequency: 200 Hz Semiconductor: AlGaInAs Spot diameter of the optical fiber: 200 nm Power: 1.5 W Pulsation: ON 20 ms, OFF 30 ms Usage: 1 min per site Power density (irradiance): 100 mW/cm2 |
| Appointment | Procedures |
|---|---|
| |
| |
| Baseline (T0) |
|
| |
| Group A: ozone administration | |
| Group B: photobiomodulation (PBM) administration | |
| After 1 month (T1) After 2 months (T2) After 3 months (T3) After 4 months (T4) After 5 months (T5) After 6 months (T6) |
|
Group A: ozone administration Group B: photobiomodulation (PBM) administration |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Ozone | T0 | 5.11 | 1.07 | 4.00 | 5.00 | 9.00 | A |
| T1 | 4.62 | 0.96 | 3.00 | 4.00 | 9.00 | B | |
| T2 | 4.46 | 0.86 | 3.00 | 4.00 | 7.00 | B,C | |
| T3 | 4.07 | 0.87 | 3.00 | 4.00 | 7.00 | D | |
| T4 | 3.82 | 0.76 | 2.00 | 4.00 | 6.00 | D,F | |
| T5 | 3.62 | 0.72 | 2.00 | 4.00 | 6.00 | F | |
| T6 | 3.54 | 0.72 | 2.00 | 3.00 | 6.00 | F | |
| PBM | T0 | 5.31 | 1.02 | 4.00 | 5.00 | 9.00 | A |
| T1 | 4.51 | 0.90 | 3.00 | 4.00 | 7.00 | B,C | |
| T2 | 4.18 | 0.85 | 2.00 | 4.00 | 7.00 | C,D | |
| T3 | 3.85 | 0.89 | 2.00 | 4.00 | 6.00 | D,E | |
| T4 | 3.37 | 0.75 | 2.00 | 3.00 | 6.00 | E,F | |
| T5 | 2.85 | 0.66 | 1.00 | 3.00 | 5.00 | G | |
| T6 | 2.43 | 0.62 | 1.00 | 2.00 | 3.00 | H |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Ozone | T0 | 71.67 | 23.54 | 30.00 | 80.00 | 100.00 | A |
| T1 | 57.33 | 18.13 | 20.00 | 60.00 | 80.00 | B | |
| T2 | 50.87 | 16.13 | 20.00 | 52.50 | 75.00 | B,C | |
| T3 | 44.77 | 15.33 | 20.00 | 45.00 | 70.00 | C,D | |
| T4 | 41.60 | 11.97 | 20.00 | 41.00 | 60.00 | C,D,E | |
| T5 | 37.60 | 11.03 | 20.00 | 38.00 | 60.00 | C,D,E,F | |
| T6 | 35.13 | 10.41 | 20.00 | 35.00 | 60.00 | D,E,F | |
| Photobiomodulation | T0 | 73.17 | 21.35 | 40.00 | 80.00 | 100.00 | A |
| T1 | 57.33 | 18.13 | 20.00 | 60.00 | 80.00 | B | |
| T2 | 50.67 | 15.85 | 20.00 | 52.50 | 75.00 | B,C | |
| T3 | 43.17 | 13.93 | 20.00 | 42.50 | 70.00 | C,D,E | |
| T4 | 37.33 | 11.50 | 20.00 | 32.50 | 55.00 | D,E,F | |
| T5 | 30.20 | 10.48 | 15.00 | 30.00 | 55.00 | E,F | |
| T6 | 25.17 | 7.43 | 13.00 | 25.00 | 45.00 | F |
| Group | Time | Mean | St Dev | Min | Median | Max | Significance * |
|---|---|---|---|---|---|---|---|
| Ozone | T0 | 71.67 | 23.54 | 30.00 | 80.00 | 100.00 | A |
| T1 | 57.33 | 18.13 | 20.00 | 60.00 | 80.00 | B | |
| T2 | 50.87 | 16.13 | 20.00 | 52.50 | 75.00 | B,C | |
| T3 | 44.77 | 15.33 | 20.00 | 45.00 | 70.00 | C,D | |
| T4 | 41.60 | 11.97 | 20.00 | 41.00 | 60.00 | C,D,E | |
| T5 | 37.60 | 11.03 | 20.00 | 38.00 | 60.00 | C,D,E,F | |
| T6 | 35.13 | 10.41 | 20.00 | 35.00 | 60.00 | D,E,F | |
| Photobiomodulation | T0 | 73.17 | 21.35 | 40.00 | 80.00 | 100.00 | A |
| T1 | 57.33 | 18.13 | 20.00 | 60.00 | 80.00 | B | |
| T2 | 50.67 | 15.85 | 20.00 | 52.50 | 75.00 | B,C | |
| T3 | 43.17 | 13.93 | 20.00 | 42.50 | 70.00 | C,D,E | |
| T4 | 37.33 | 11.50 | 20.00 | 32.50 | 55.00 | D,E,F | |
| T5 | 30.20 | 10.48 | 15.00 | 30.00 | 55.00 | E,F | |
| T6 | 25.17 | 7.43 | 13.00 | 25.00 | 45.00 | F |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scribante, A.; Gallo, S.; Pascadopoli, M.; Soleo, R.; Di Fonso, F.; Politi, L.; Venugopal, A.; Marya, A.; Butera, A. Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial. Photonics 2022, 9, 138. https://doi.org/10.3390/photonics9030138
Scribante A, Gallo S, Pascadopoli M, Soleo R, Di Fonso F, Politi L, Venugopal A, Marya A, Butera A. Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial. Photonics. 2022; 9(3):138. https://doi.org/10.3390/photonics9030138
Chicago/Turabian StyleScribante, Andrea, Simone Gallo, Maurizio Pascadopoli, Riccardo Soleo, Fabio Di Fonso, Luca Politi, Adith Venugopal, Anand Marya, and Andrea Butera. 2022. "Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial" Photonics 9, no. 3: 138. https://doi.org/10.3390/photonics9030138