
Investigation of the Excretion of Triamcinolone Acetonide and Its Metabolite


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Doses
2.2. Sample Collection before, during and after Substance Administration
2.3. Chemicals and Reagents
2.4. Urine Samples Preparation
2.5. Instrument Setups
2.5.1. Liquid Chromatography
2.5.2. Mass Spectrometry
3. Results
3.1. Method Validation
3.1.1. Linearity
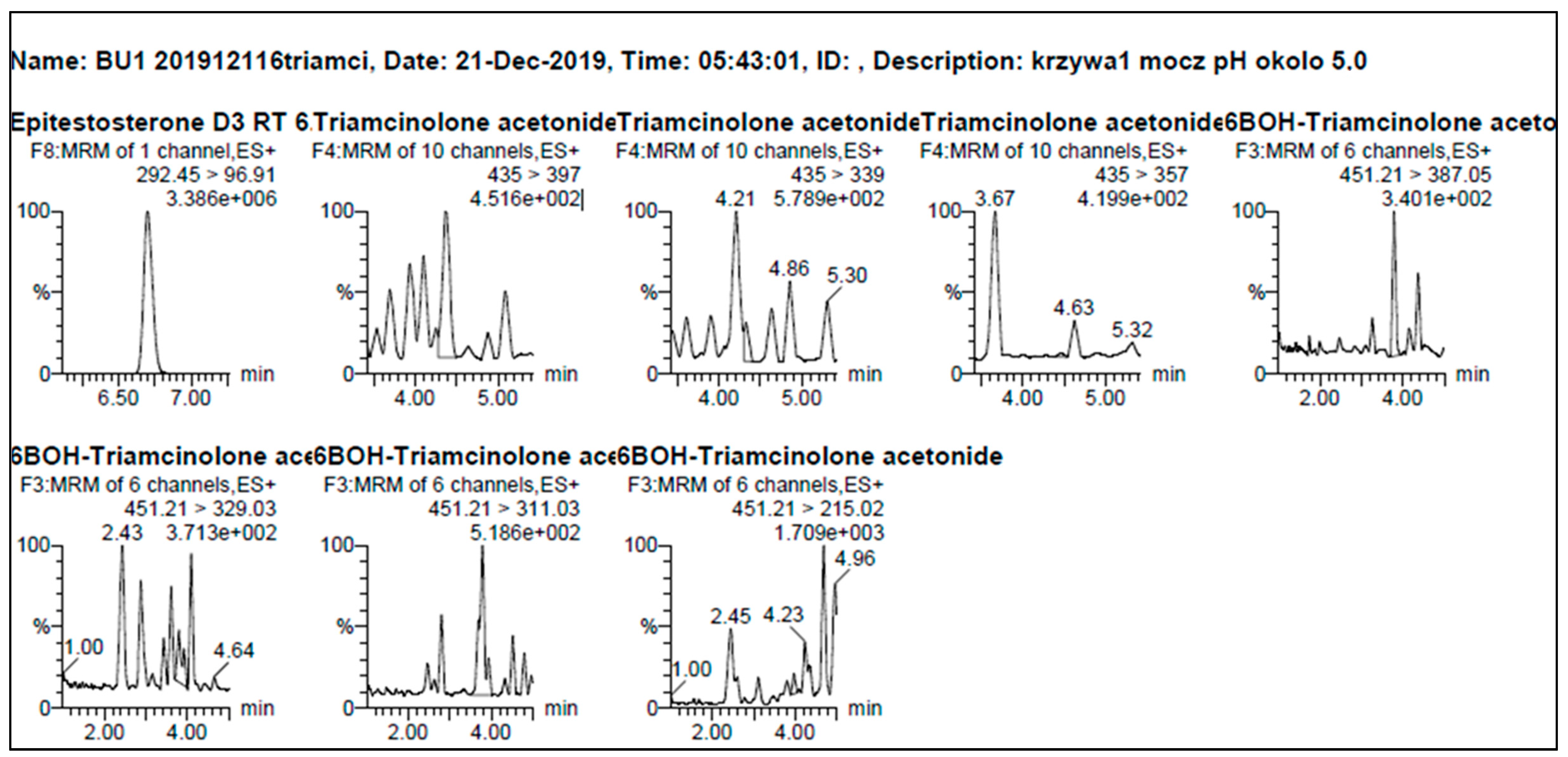
3.1.2. Selectivity and Limit of Detection (LOD)
3.1.3. Carry—Over Effect
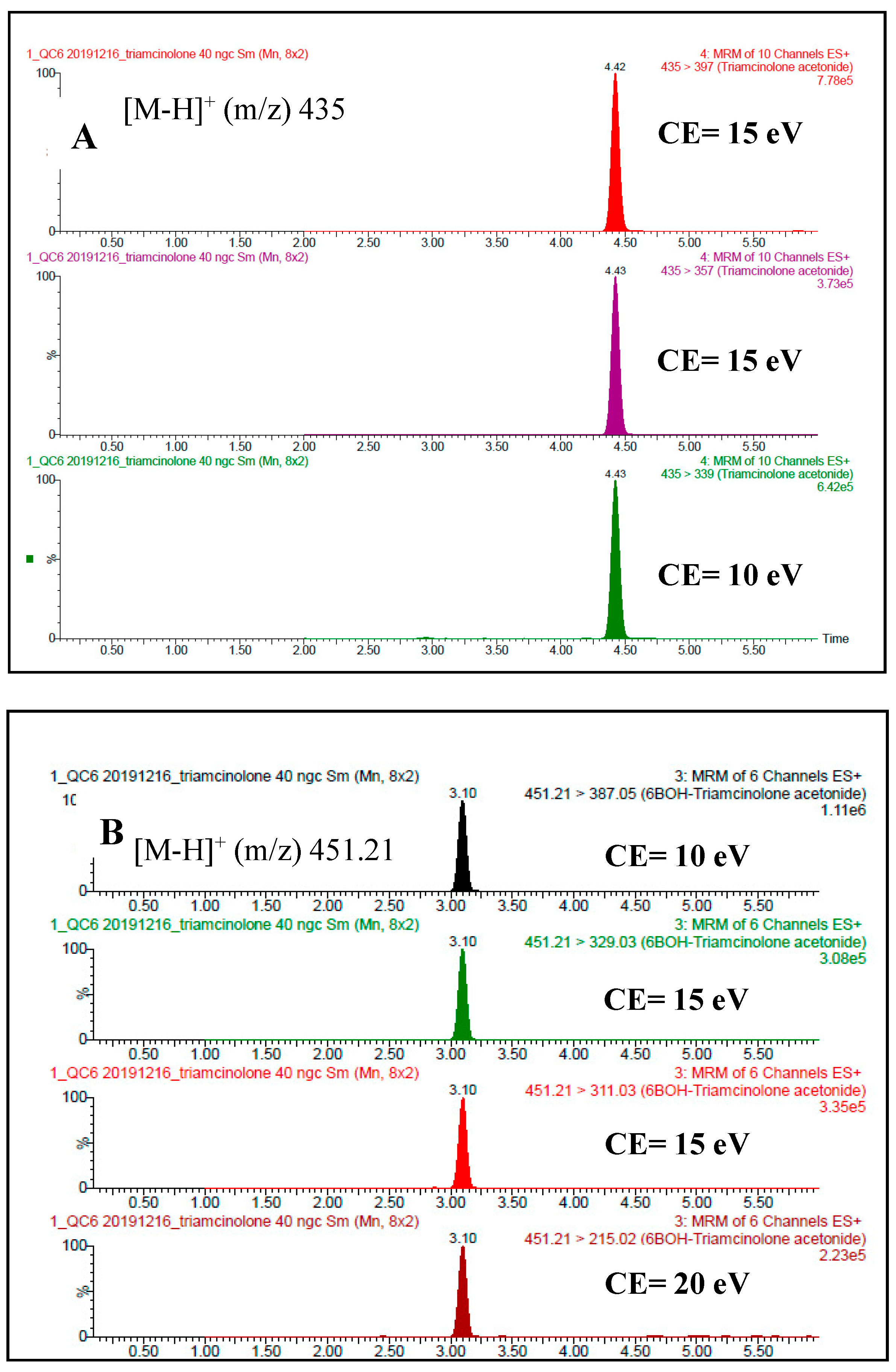
3.1.4. Repeatability of Retention Times
3.1.5. Real Anti-Doping Samples Testing
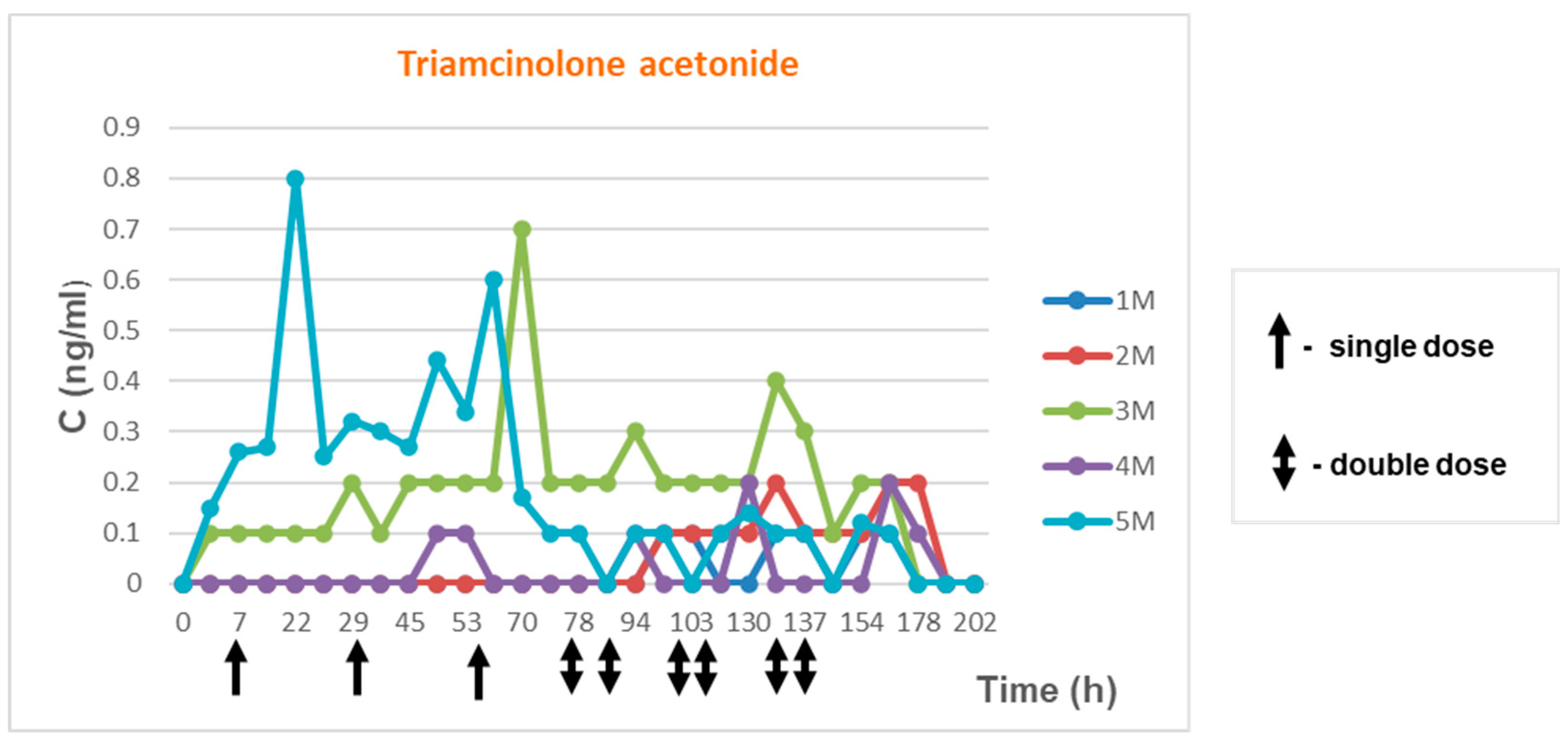
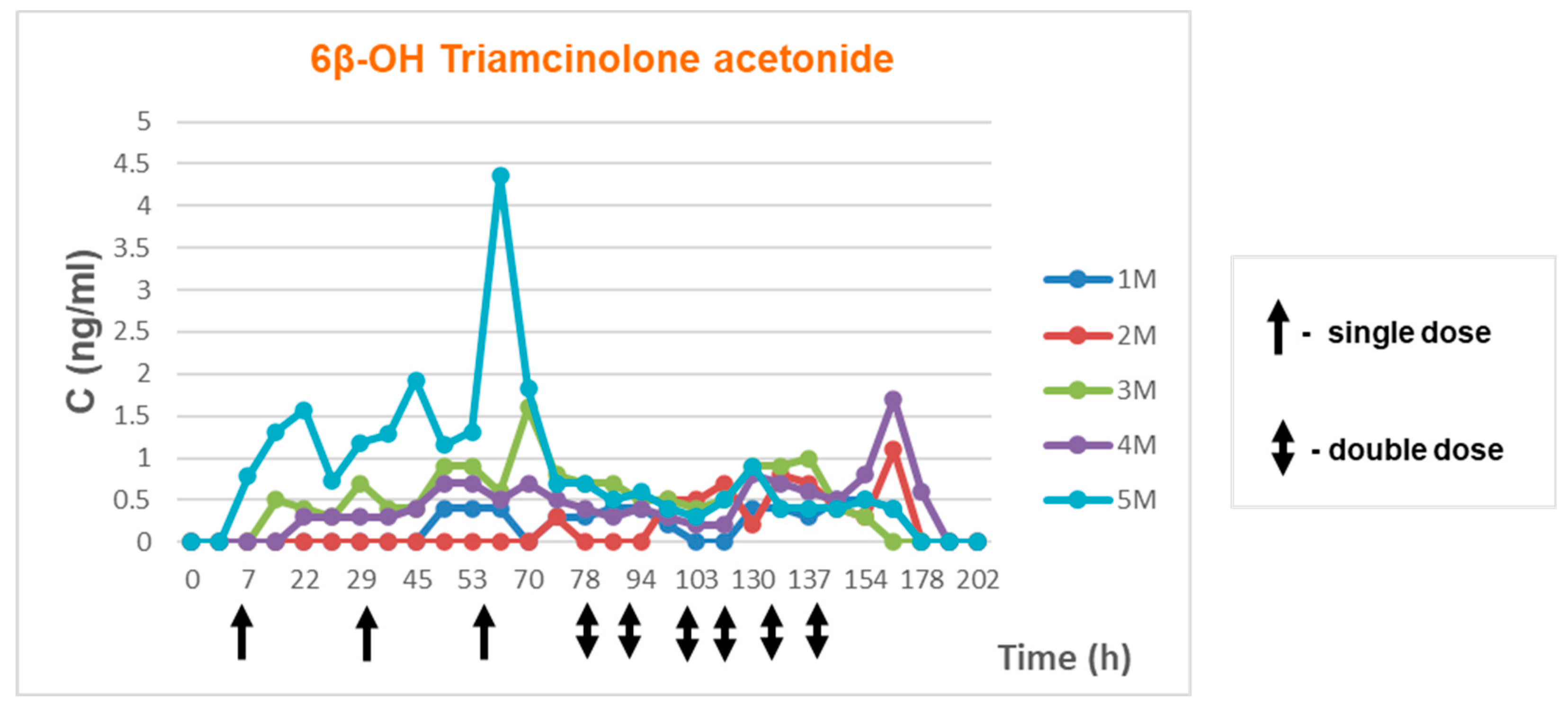
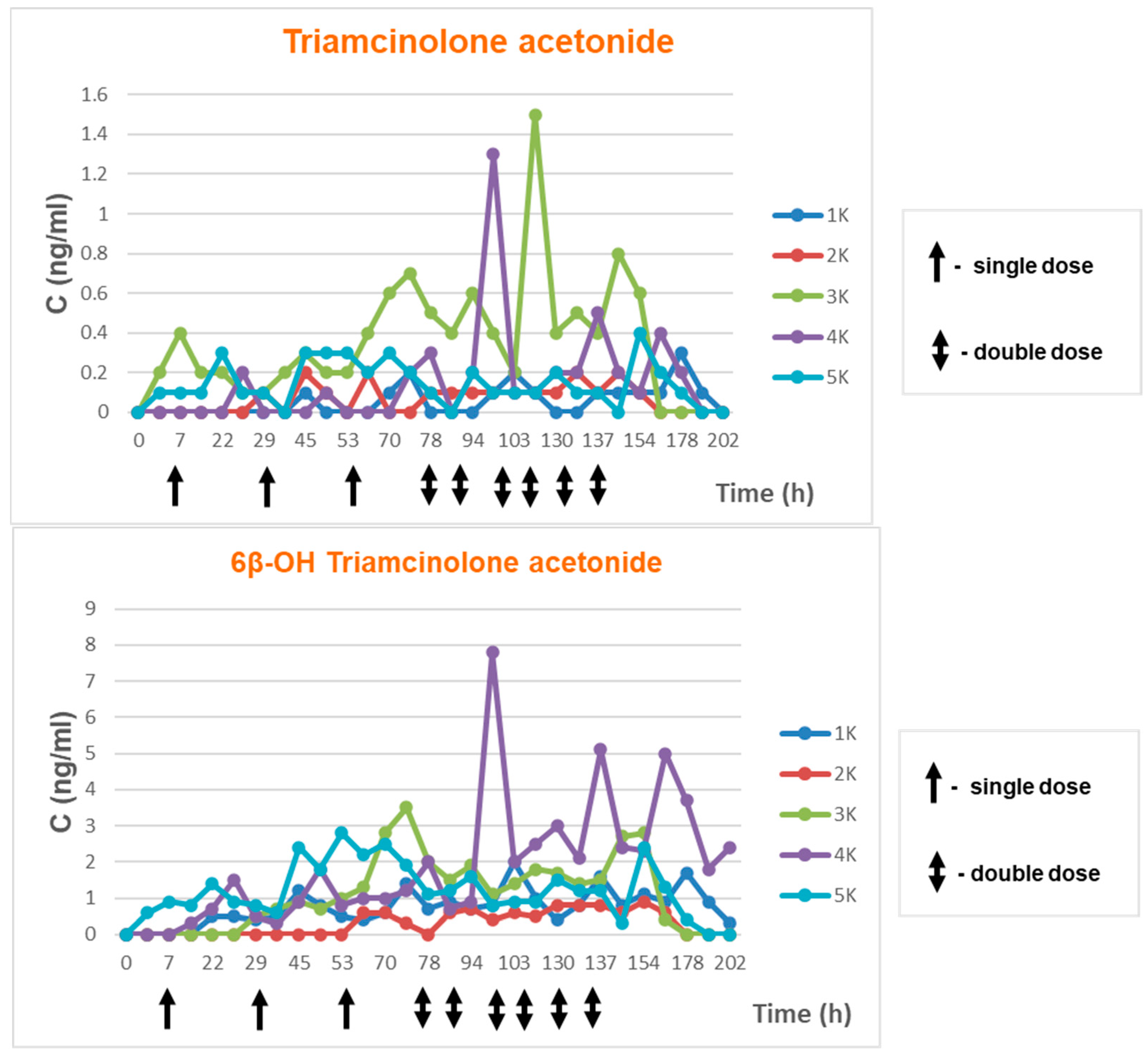
3.1.6. Excretion Study after Transdermal TA Administration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pharmindex. Available online: https://pharmindex.pl/listalekow# (accessed on 15 December 2022).
- Service of Professional Information about Medicines (Serwis Fachowej Informacji o Lekach). Available online: https://www.lekinfo24.pl/wyniki-wyszukiwania?qh=triamcinolone+aceton&q=triamcinolone+aceton (accessed on 15 December 2022).
- Encyclopedia of Medicines (Encyklopedia Leków). Available online: http://medycyna.anauk.net/101-0-1443-Triamcinolone+acetonide.Encyklopedia.Lekow.htmL (accessed on 15 December 2022).
- Practical Medicine for Doctors (Medycyna Praktyczna dla Lekarzy). Available online: https://www.mp.pl/szukaj?q=triamcinolone+acetonide (accessed on 15 December 2022).
- World Anti-Doping Agency. The 2004 Prohibited List. Available online: https://www.wada-ama.org/sites/default/files/resources/files/WADA_Prohibited_List_2004_EN.pdf (accessed on 15 December 2022).
- World Anti-Doping Agency. The 2023 Prohibited List. Available online: https://www.wada-ama.org/sites/default/files/2022-09/2023list_en_final_9_september_2022.pdf (accessed on 3 February 2023).
- World Anti-Doping Agency. WADA Technical Document-TD2019MRPL-Minimum Required Performance Levels For Detection and Identification of Non-Threshold Substances. Available online: https://www.wada-ama.org/sites/default/files/resources/files/td2019mrpl_eng.pdf (accessed on 15 December 2022).
- World Anti-Doping Agency. WADA Technical Document-TD2022MRPL-Minimum Required Performance Levels For Detection and Identification of Non-Threshold Substances. Available online: https://www.wada-ama.org/sites/default/files/2022-01/td2022mrpl_v1.1_eng_0.pdf (accessed on 15 December 2022).
- Kaliszewski, P.; Kończak, D.; Chołbiński, P.; Wicka, M.; Michalak, D.; Kwiatkowska, D.; Lewandowska-Pachecka, S.; Namieśnik, J.; Pokrywka, A. Budesonide treatment of professional athletes and anti-doping testing-case studies. Acta Pol. Pharm.-Drug Res. 2016, 73, 229–237. [Google Scholar]
- Matabosch, X.; Pozo, O.J.; Pérez-Mña, C.; Farré, M.; Marcos, J.; Segura, J.; Ventura, R. Discrimination of prohibited oral use from authorized inhaled treatment of budesonide in sports. Ther. Drug Monit. 2013, 35, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Matabosch, X.; Pozo, O.J.; Papaseit, E.; Farré, M.; Marcos, J.; Segura, J.; Ventura, R. Detection and characterization of triamcinolone acetonide metabolites in human urine by liquid chromatography/tandem mass spectrometry after intramuscular administration. Rapid Commun. Mass Spectrom. 2014, 28, 1829–1839. [Google Scholar] [CrossRef]
- Matabosch, X.; Pozo, O.J.; Pérez-Mañá, C.; Papaseit, E.; Marcos, J.; Segura, J.; Ventura, R. Evaluation of the reporting level to detect triamcinolone acetonide misuse in sports. J. Steroid Biochem. Mol. Biol. 2015, 145, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.W.; Huang, T.Y.; Tseng, Y.C.; Chang-Chien, G.P.; Lin, S.F.; Hsu, M.C. Positive doping results caused by the single-dose local injection of triamcinolone acetonide. Forensic Sci. Int. 2014, 244, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coll, S.; Monfort, N.; Alechaga, É.; Matabosch, X.; Pérez-Mañá, C.; Ventura, R. Additional studies on triamcinolone acetonide use and misuse in sports: Elimination profile after intranasal and high-dose intramuscular administrations. Steroids 2019, 151, 108464. [Google Scholar] [CrossRef] [PubMed]
- Coll, S.; Matabosch, X.; Llorente-Onaindia, J.; Carbó, M.L.; Pérez-Mañá, C.; Monfort, N.; Monfort, J.; Ventura, R. Elimination profile of triamcinolone hexacetonide and its metabolites in human urine and plasma after a single intra-articular administration. Drug Test Anal. 2019, 11, 1589–1600. [Google Scholar] [CrossRef] [PubMed]
- Knych, H.K.; Vidal, M.A.; Casbeer, H.C.; McKemie, D.S. Pharmacokinetics of triamcinolone acetonide following intramuscular and intra-articular administration to exercised Thoroughbred horse. Equine Vet J. 2013, 45, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Allado, E.; Poussel, M.; Gambier, N.; Saunier, V.; Starck, M.; Buisson, C.; Cinquetti, G.; Albuisson, E.; Chenuel, B. SporTRIA study-a multicentre trial protocol for excretion kinetics of triamcinolone acetonide following sport-related intra-articular injections in knees: Definitions of the washout periods. BMJ Open 2021, 11, e047548. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, D.; Grucza, K.; Chajewska, K.; Konarski, P.; Wojtkowiak, K.; Drapała, A.; Wicka, M. Ecdysterone: Possible sources of origin in urine. Drug Test Anal. 2022. [Google Scholar] [CrossRef] [PubMed]
- World Anti-Doping Agency Anti-Doping Testing Figures Report. Available online: https://www.wada-ama.org/en/resources/laboratories/anti-doping-testing-figures-report (accessed on 15 December 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medication/Manufacturing Company | Drug/Medication Formulation | Active Substance | Intended Use |
|---|---|---|---|
| Pevisone/Karo Pharma | Cream, ointment | Econazole nitrate 10 mg/g Triamcinolone acetonide 1 mg/g | Fungal infection of the skin accompanied by pruritus and inflammation |
| Triacomb/Teva Canada | Cream | Gramicidin 0.25 mg/g Neomycin sulphate 2.5 mg/g Nystatin 100,000 j.m./g Triamcinolone acetonide 1 mg/g | anti-inflammatory, antiprurital, antibacterial and antifungal |
| Polcortolon TC/Polfa Tarchomin | Skin aerosol suspension | Tetracycline hydrochloride 23.12 mg/g Triamcinolone acetonide 0.58 mg/g | Allergic skin conditions, first degree burns and frostbites, lower leg ulceration |
| Polcortolon TC/Polfa Tarchomin | Injections | Triamcinolone acetonide 40 mg/mL | joint inflammation and degeneration, rheumatic conditions, allergy-related skin conditions, asthma |
| Monacort/Polfa Tarchomin | Aerosol | Dichlorohydroxyquinoline Triamcinolone acetonide | Seborrheic dermatitis, first degree burns and frostbites, radiation dermatitis |
| Kenalog/BRISTOL MYERS SQUIBB CO. | Injections | Triamcinolone acetonide 40 mg/mL | joint inflammation and degeneration, rheumatic conditions, allergy-related skin conditions, asthma |
| Nasacort/Aventis Pharma | Areosol | Triamcinolone acetonide 55 µg/dose | Allergy, nose conditions |
| Triamhexal/Hexal AG. | Injections | Triamcinolone acetonide 0.04 g/mL | Asthma, rhinitis, adrenal insufficiency, collagen disorders, skin conditions, rheumatic conditions, hemolitic disorders, leukemia, lymphomas, kidney conditions |
| Time Lapsed | % of Acetonitrile/Water |
|---|---|
| 0 min | 5% |
| 2 min | 35% |
| 8 min | 50% |
| 9 min | 100% |
| 10 min | 100% |
| 11 min | 5% |
| Compound | Precursor Ion | Daughter Ions | Cone [V] | CE [V] |
|---|---|---|---|---|
| Triamcinolone acetonide | 435 | 397 | 25 | 15 |
| 339 | 15 | |||
| 357 | 10 | |||
| 6β-hydroxy Triamcinolone acetonide | 451.21 | 387.05 | 10 | 10 |
| 329.03 | 15 | |||
| 311.03 | 15 | |||
| 215.02 | 20 | |||
| D3-Testosterone | 292.45 | 99.78 | 35 | 25 |
| D3-Epitestosterone | 292.45 | 96.91 | 35 | 25 |
| Calibration Curve—Urine Item | pH | Specific Gravity | r2 for TA | |
|---|---|---|---|---|
| r2 for 6β-OH TA | ||||
| Curve 1 | 4.93 | 1.005 | r2 = 0.992589 y = 0.00695683*x + 0.00448783 | |
| r2 = 0.992273 y = 0.01041*x + 0.0139676 | ||||
| Curve 2 | 5.33 | 1.022 | r2 = 0.992421 y = 0.00739297*x + 0.00364649 | |
| r2 = 0.995764 y = 0.00677963*x + 0.00083371 | ||||
| Curve 3 | 5.57 | 1.018 | r2 = 0.992421 y = 0.00739297*x + 0.00364649 | |
| r2 = 0.998375 y = 0.00640535*x + 0.000668843 | ||||
| Curve 4 | 6.80 | 1.003 | r2 = 0.990605 y = 0.00681797*x + 0.00513173 | |
| r2 = 0.990098 y = 0.0117811*x + 0.0251488 | ||||
| Curve 5 | 6.32 | 1.008 | r2 = 0.991373 y = 0.00711099*x + 0.0200535 | |
| r2 = 0.987084 y = 0.00988865*x + 0.0204793 | ||||
| Curve 6 | 7.42 | 1.015 | r2 = 0.996764 y = 0.00791197*x + 0.00320253 | |
| r2 = 0.997698 y = 0.00833508*x + 0.00636717 | ||||
| Compound | Linearity Range [ng/mL] | Linear Regression Equation b | (r) c | LOQ d [ng/mL] |
|---|---|---|---|---|
| Triamcinolone acetonide | 0.5–100 | y = 0.01x + 0.02 | 0.999 | 0.5 |
| 6β-hydroxy triamcinolone acetonide | 0.5–100 | y = 0.01x + 0.01 | 0.998 | 0.5 |
| Item | Compound Tested | Retention Time | |
|---|---|---|---|
| [min] | RSD [%] | ||
| 1 | Triamcinolone acetonide | 4.42 | 0.12 |
| 2 | 6β-hydroxy Triamcinolone acetonide | 3.10 | 0.15 |
| Item | Gender | Concentration of Triamcinolone Acetonide [ng/mL] | Concentration of 6β-Hydroxy-Triamcinolone Acetonide [ng/mL] | pH | Specific Gravity [g/mL] | Sport|Discipline | Other Substances Detected in Samples |
|---|---|---|---|---|---|---|---|
| 1. | F | 29.63 | 49.99 | 5.55 | 1.026 | Athletics | Race Walk | Cathine < 5 ug/mL Pseudoephedrine < 150 ng/mL |
| 2. | M | 13.12 | 68.00 | 5.23 | 1.018 | Cycling | Road | -- |
| 3. | F | 23.75 | 145.30 (estimated concentration beyond calibration curve) | 5.20 | 1.025 | Athletics | Throws | -- |
| 4. | M | 7.56 | 20.31 | 7.40 | 1.008 | Athletics | Long Distance 3000 m or greater | -- |
| 5. | M | <1 | <1 | 5.60 | 1.006 | Cycling | Road | Codeine < 50 ng/mL/morphine < 1000 ng/mL |
| 6. | M | 3.02 | 11.73 | 5.81 | 1.024 | Canoe/Kayak | Long Distance 1000 m | -- |
| 7. | F | 2.53 | 15.44 | 5.93 | 1.013 | Volleyball | Volleyball | Etg > 5 µg/mL |
| 8. | M | 2.73 | 29.43 | 5.79 | 1.023 | Modern Pentathlon | Modern Pentathlon | -- |
| 9. | F | 2.10 | 6.09 | 5.34 | 1.018 | Athletics | Sprint 400 m or less | -- |
| 10. | M | <1 | 3.65 | 5.59 | 1.012 | Athletics | Sprint 400 m or less | -- |
| 11. | M | 2.45 | 11.14 | 6.81 | 1.018 | Modern Pentathlon | Modern Pentathlon | -- |
| 12. | M | 5.72 | 23.34 | 5.19 | 1.023 | Athletics | Throws | -- |
| 13. | M | 1.98 | 7.30 | 5.57 | 1.027 | Athletics | Jumps | -- |
| 14. | F | <1 | 8.60 | 5.77 | 1.018 | Basketball | Basketball | -- |
| 15. | M | 18.86 | 92.05 | 5.36 | 1.019 | Aquatics | Swimming Middle Distance 200–400 m | Salbutamol < 1000 ng/mL |
| 16. | M | - | <1 | 5.46 | 1.016 | Athletics | Long Distance 3000 m or greater | -- |
| 17. | F | <1 | 2.16 | 5.53 | 1.020 | Athletics | Sprint 400 m or less | -- |
| 18. | M | 1.89 | 10.57 | 5.68 | 1.027 | Football | Football | -- |
| Item | Age | Height | Weight | BMI |
|---|---|---|---|---|
| 1M | 28 | 179 | 84 | 26.22 |
| 2M | 29 | 175 | 67 | 21.88 |
| 3M | 41 | 178 | 83 | 26.20 |
| 4M | 51 | 173 | 89 | 29.74 |
| 5M | 60 | 178 | 90 | 28.41 |
| Item | Age | Height | Weight | BMI |
|---|---|---|---|---|
| 1K | 29 | 162 | 67 | 25.33 |
| 2K | 30 | 152 | 48 | 20.78 |
| 3K | 32 | 171 | 68 | 23.26 |
| 4K | 36 | 172 | 60 | 20.28 |
| 5K | 48 | 168 | 56 | 19.84 |
| Year | Number of Samples with TA Presence Reported as AAF | % AAF for Glucocorticoids Group |
|---|---|---|
| 2004 | 246 | 44.9% |
| 2005 | 25 | 7.7% |
| 2006 | 18 | 6.4% |
| 2007 | 18 | 6.3% |
| 2008 | 16 | 5.1% |
| 2009 | 1 | 0.4% |
| 2010 | 7 | 3.0% |
| 2011 | 16 | 5.8% |
| 2012 | 16 | 4.4% |
| 2013 | 12 | 3.6% |
| 2014 | 16 | 6% |
| 2015 | 17 | 8% |
| 2016 | 18 | 10% |
| 2017 | 31 | 14% |
| 2018 | 72 | 25% |
| 2019 | 44 | 19% |
| 2020 | 16 | 23% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwiatkowska, D.; Wicka, M.; Bulska, E.; Kaliszewski, P. Investigation of the Excretion of Triamcinolone Acetonide and Its Metabolite. Separations 2023, 10, 164. https://doi.org/10.3390/separations10030164
Kwiatkowska D, Wicka M, Bulska E, Kaliszewski P. Investigation of the Excretion of Triamcinolone Acetonide and Its Metabolite. Separations. 2023; 10(3):164. https://doi.org/10.3390/separations10030164
Chicago/Turabian StyleKwiatkowska, Dorota, Mariola Wicka, Ewa Bulska, and Pawel Kaliszewski. 2023. "Investigation of the Excretion of Triamcinolone Acetonide and Its Metabolite" Separations 10, no. 3: 164. https://doi.org/10.3390/separations10030164