
Tailoring Can Improve Consumers’ Hygienic Food-Handling Behavior to Reduce the Transmission Risk of Antimicrobial-Resistant Bacteria through Food


Abstract
:1. Introduction
1.1. Tailored Intervention to Change Behavior
1.2. Relevant Theoretical Determinants
1.3. The Present Study
- Participants in the tailored intervention condition show higher levels of hygienic food-handling behavior, intention, self-efficacy, and risk perception at T2, T3, and T4, compared to that of participants in the generic intervention condition and the control condition.
- Participants in the tailored intervention show lower levels of negative outcome expectancies at T3 and T4, compared to that of participants in the generic intervention and the control condition.
- Participants in the tailored intervention show higher levels of coping planning and action control at T3 and T4, compared to that of participants in the generic intervention and the control condition.
- Hygienic food-handling behavior increases over time among participants in the tailored and generic interventions, whereas this behavior remains at the same level from T1 to T4 in the control group.
- The increase in hygienic food-handling behavior over time is higher for participants in the tailored intervention than in the generic intervention.
2. Materials and Methods
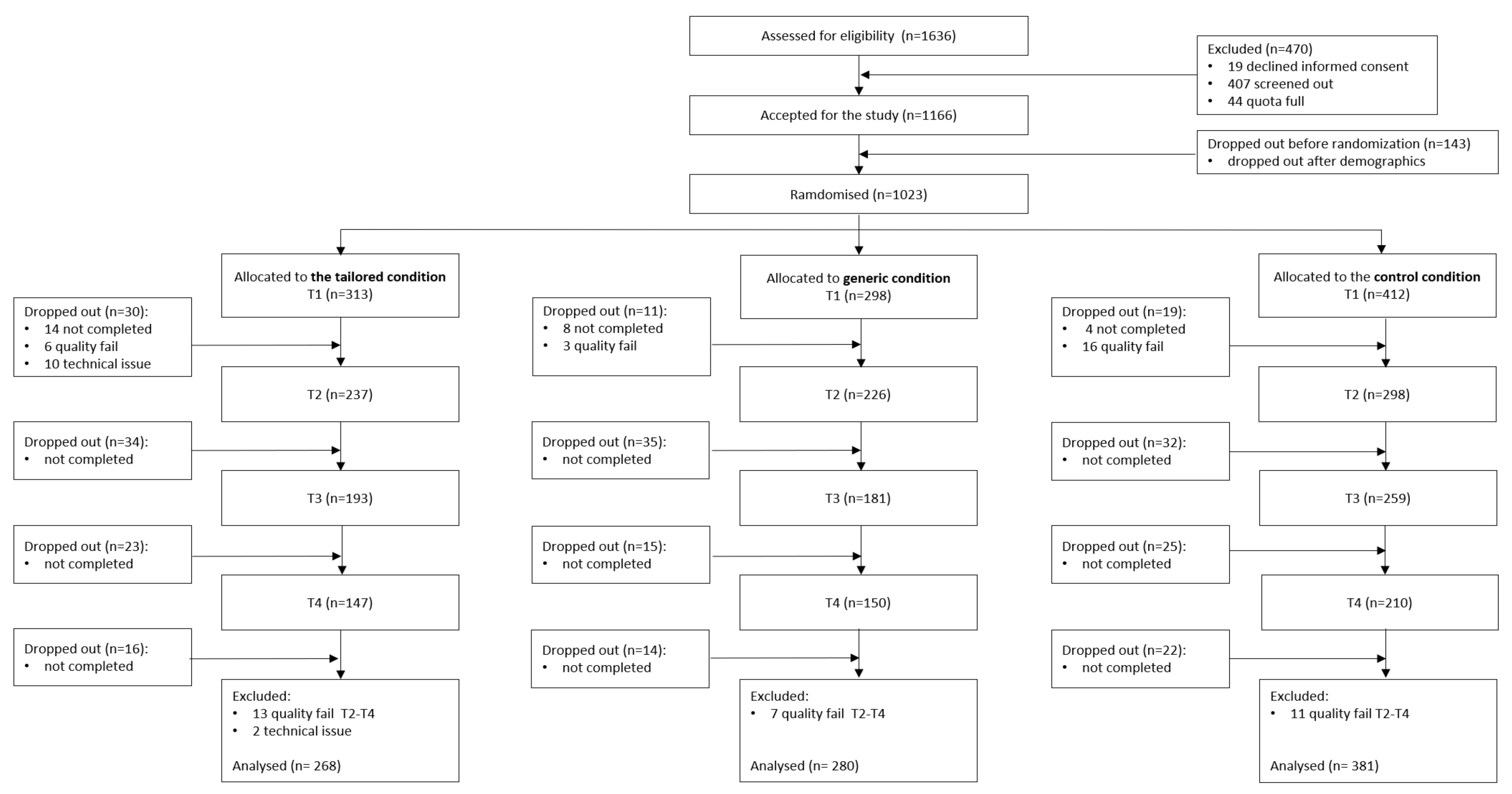
2.1. Procedure and Study Design
2.2. Measures
2.3. Intervention Descriptions
2.4. Participants
2.5. Statistical Analyses
3. Results
3.1. Sample
3.2. HAPA Variables at Baseline
3.3. MLM
3.3.1. Model Fit
3.3.2. Preintentional Determinants
Self-Efficacy
Risk Perception
Positive and Negative Outcome Expectancy
Summary of Preintentional Variables
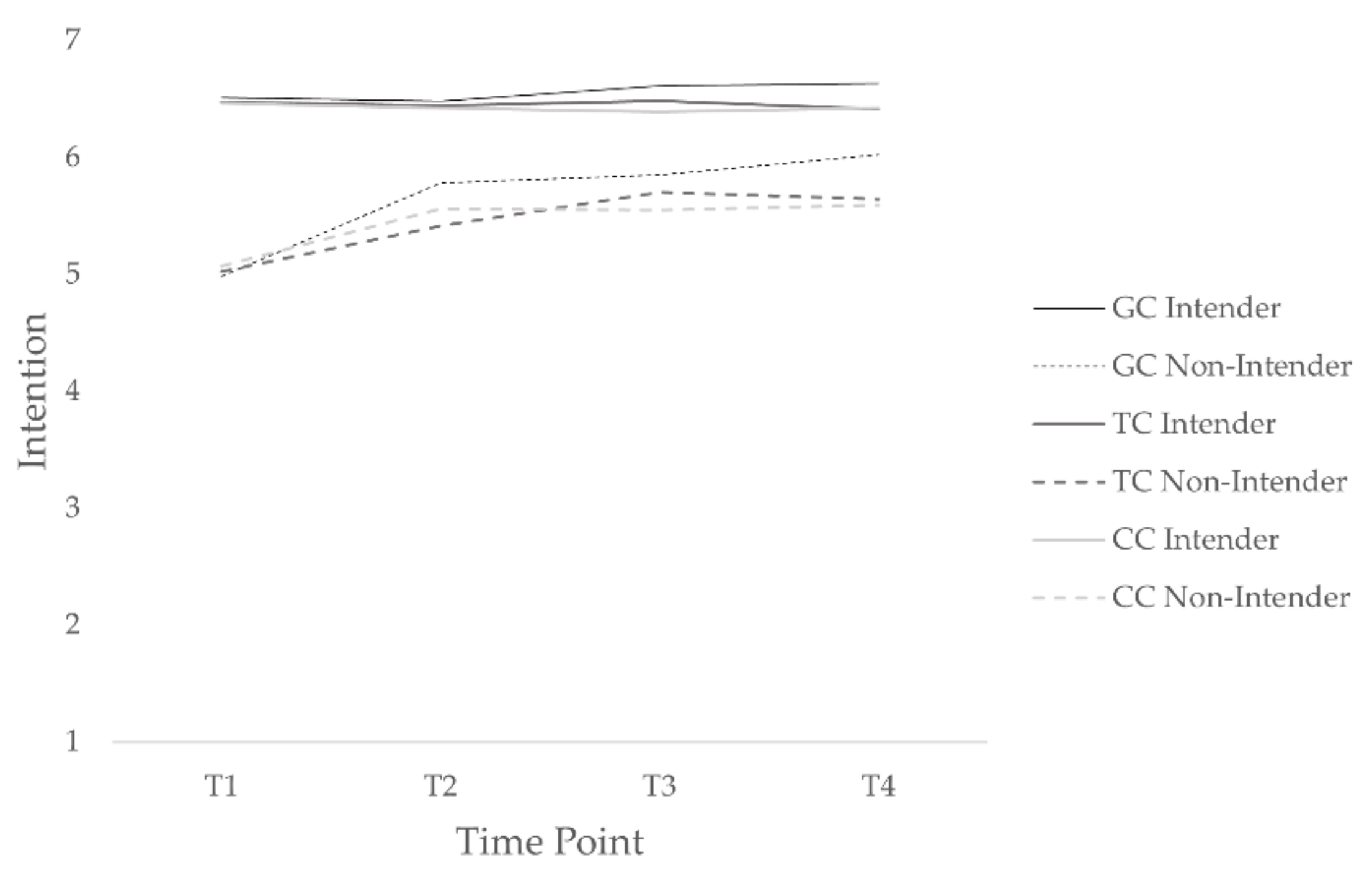
3.3.3. Intention
3.3.4. Postintentional Determinants
Coping Planning
Action Control
Habitual Behavior
Summary of Postintentional Variables
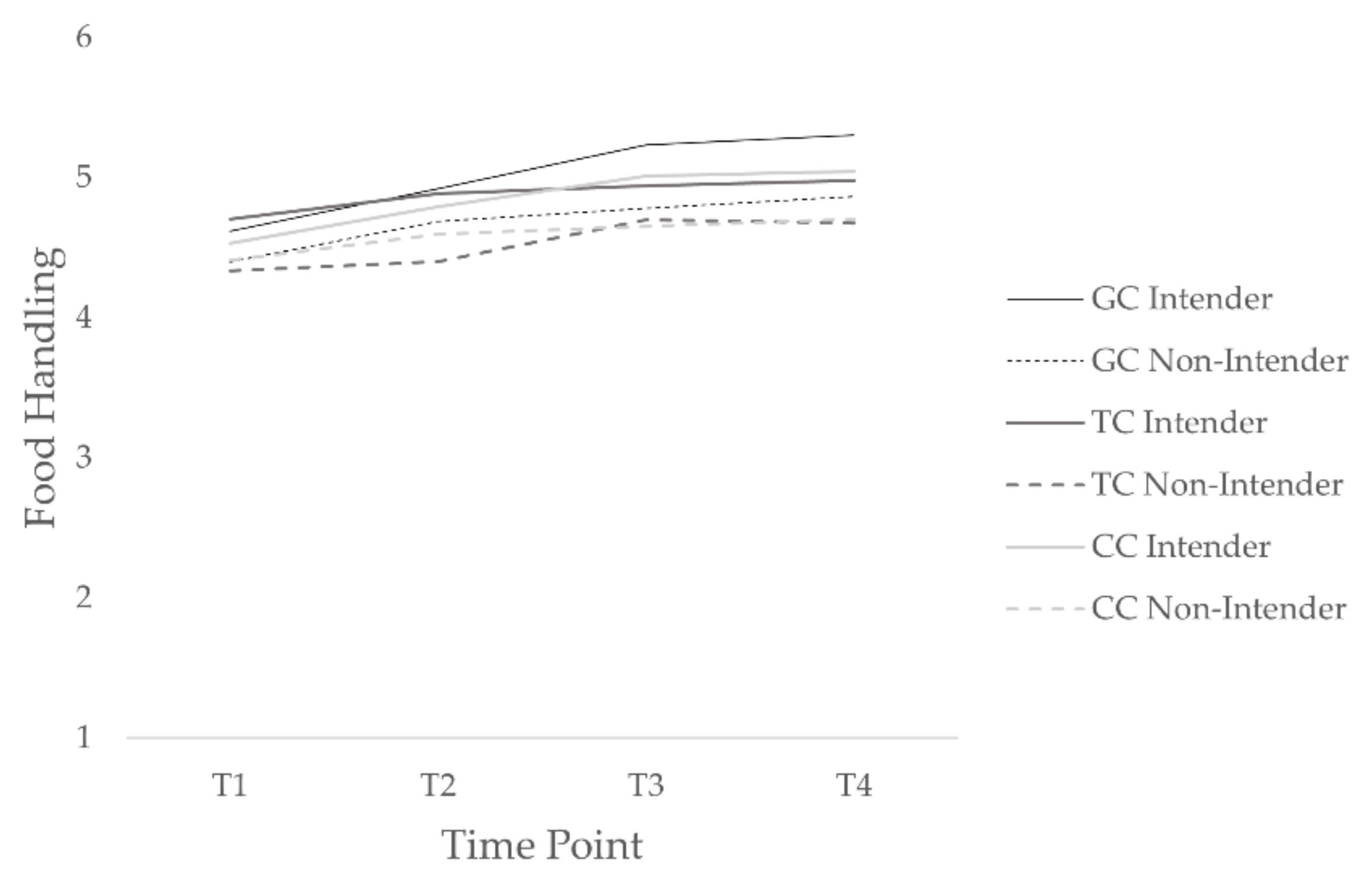
3.3.5. Self-Reported Behavior
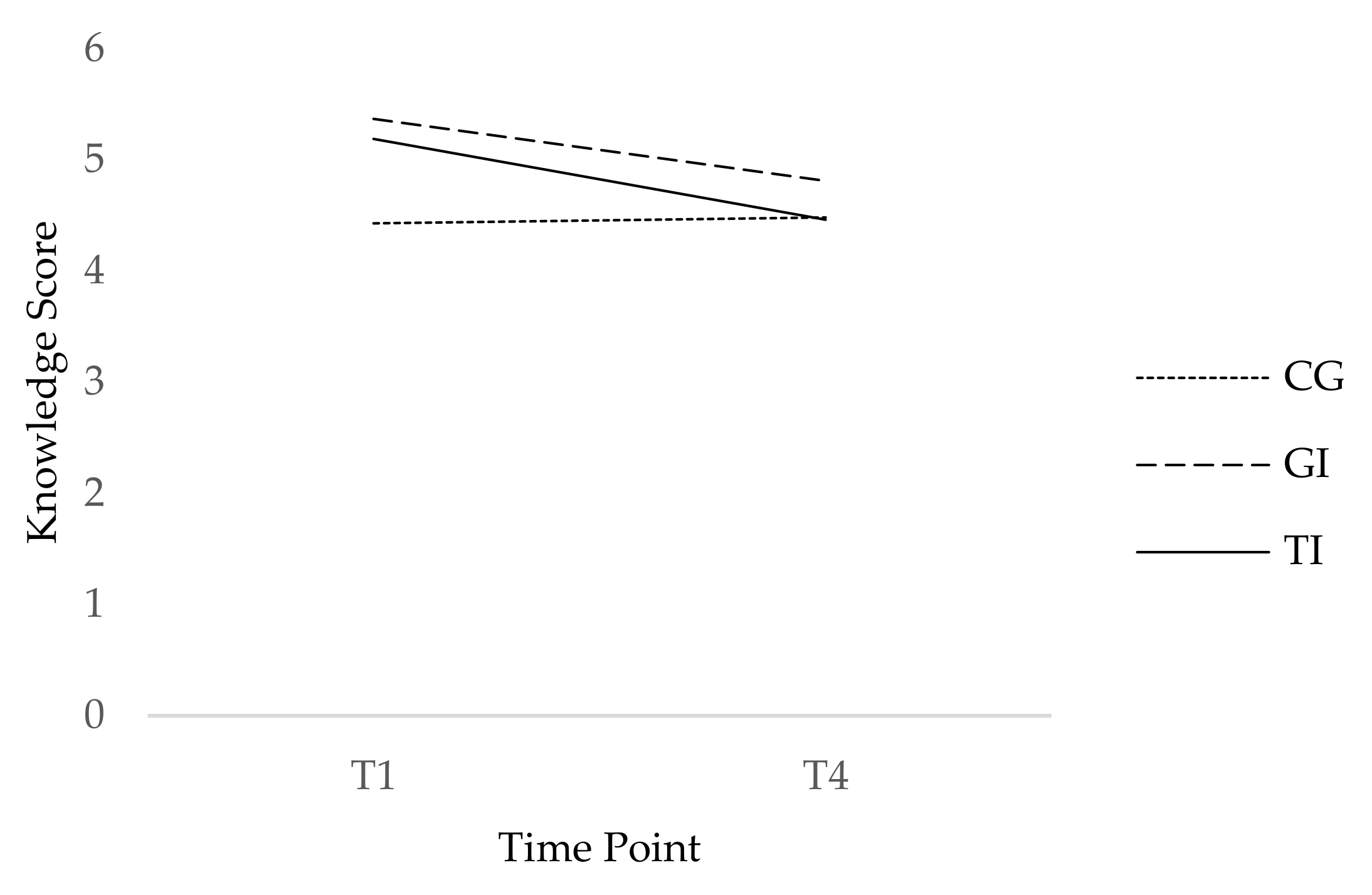
3.4. Knowledge
3.5. Evaluation
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FSVO. Richtig Zubereiten-Sicher Geniessen (Cook Properly-Enjoy Safely). Available online: https://www.blv.admin.ch/blv/de/home/lebensmittel-und-ernaehrung/lebensmittelsicherheit/krankheitserreger-und-hygiene/hygiene.html (accessed on 23 February 2019).
- Regea, G. Review on antibiotics resistance and its economic impacts. J. Pharmacol. Clin. Res. 2018, 5, 555675. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E.; Stájer, A.; Baráth, Z. Antimicrobial resistance in the context of the sustainable development goals: A brief review. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 71–82. [Google Scholar] [CrossRef]
- Lechner, I.; Freivogel, C.; Stärk, K.D.; Visschers, V.H. Exposure pathways to antimicrobial resistance at the human-animal interface—A qualitative comparison of Swiss expert and consumer opinions. Front. Public Health 2020, 8, 345. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.W.; Redmond, E.C. Behavioral observation and microbiological analysis of older adult consumers’ cross-contamination practices in a model domestic kitchen. J. Food Prot. 2018, 81, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Maughan, C.; Chambers IV, E.; Godwin, S.; Chambers, D.; Cates, S.; Koppel, K. Food handling behaviors observed in consumers when cooking poultry and eggs. J. Food Prot. 2016, 79, 970–977. [Google Scholar] [CrossRef]
- Collineau, L.; Carmo, L.P.; Endimiani, A.; Magouras, I.; Müntener, C.; Schüpbach-Regula, G.; Stärk, K.D. Risk ranking of antimicrobial-resistant hazards found in meat in Switzerland. Risk Anal. 2018, 38, 1070–1084. [Google Scholar] [CrossRef] [PubMed]
- Jans, C.; Sarno, E.; Collineau, L.; Meile, L.; Stärk, K.D.; Stephan, R. Consumer exposure to antimicrobial resistant bacteria from food at Swiss retail level. Front. Microbiol. 2018, 9, 362. [Google Scholar] [CrossRef] [PubMed]
- Darlow, S.; Heckman, C. Results from a tailored SMS and behavior-tracking pilot study on sun-safe behaviors in young women. Health Educ. Behav. 2017, 44, 937–944. [Google Scholar] [CrossRef]
- Lustria, M.L.A.; Noar, S.M.; Cortese, J.; Van Stee, S.K.; Glueckauf, R.L.; Lee, J. A meta-analysis of web-delivered tailored health behavior change interventions. J. Health Commun. 2013, 18, 1039–1069. [Google Scholar] [CrossRef]
- Martinez-Montilla, J.M.; Mercken, L.; de Vries, H.; Candel, M.; Lima-Rodríguez, J.S.; Lima-Serrano, M. A web-based, computer-tailored intervention to reduce alcohol consumption and binge drinking among Spanish adolescents: Cluster randomized controlled trial. J. Med. Internet Res. 2020, 22, e15438. [Google Scholar] [CrossRef] [Green Version]
- Tong, H.L.; Quiroz, J.C.; Kocaballi, A.B.; Fat, S.C.M.; Dao, K.P.; Gehringer, H.; Chow, C.K.; Laranjo, L. Personalized mobile technologies for lifestyle behavior change: A systematic review, meta-analysis, and meta-regression. Prev. Med. 2021, 148, 106532. [Google Scholar] [CrossRef]
- Afonso, L.; Rodrigues, R.; Castro, J.; Parente, N.; Teixeira, C.; Fraga, A.; Torres, S. A mobile-based tailored recommendation system for parents of children with overweight or obesity: A new tool for health care centers. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 779–794. [Google Scholar] [CrossRef]
- De Cocker, K.; De Bourdeaudhuij, I.; Cardon, G.; Vandelanotte, C. The effectiveness of a web-based computer-tailored intervention on workplace sitting: A randomized controlled trial. J. Med. Internet Res. 2016, 18, e96. [Google Scholar] [CrossRef] [Green Version]
- Tzelepis, F.; Mitchell, A.; Wilson, L.; Byrnes, E.; Haschek, A.; Leigh, L.; Oldmeadow, C. The Long-Term Effectiveness of Internet-Based Interventions on Multiple Health Risk Behaviors: Systematic Review and Robust Variance Estimation Meta-analysis. J. Med. Internet Res. 2021, 23, e23513. [Google Scholar] [CrossRef]
- Von Lengerke, T.; Ebadi, E.; Schock, B.; Krauth, C.; Lange, K.; Stahmeyer, J.T.; Chaberny, I.F. Impact of psychologically tailored hand hygiene interventions on nosocomial infections with multidrug-resistant organisms: Results of the cluster-randomized controlled trial PSYGIENE. Antimicrob. Resist. Infect. Control 2019, 8, 56. [Google Scholar] [CrossRef]
- Wang, L.; Miller, L.C. Just-in-the-moment adaptive interventions (JITAI): A meta-analytical review. Health Commun. 2020, 35, 1531–1544. [Google Scholar] [CrossRef]
- Diplock, K.J.; Dubin, J.A.; Leatherdale, S.T.; Hammond, D.; Jones-Bitton, A.; Majowicz, S.E. Observation of high school students’ food handling behaviors: Do they improve following a food safety education intervention? J. Food Prot. 2018, 81, 917–925. [Google Scholar] [CrossRef]
- Prestwich, A.; Webb, T.L.; Conner, M. Using theory to develop and test interventions to promote changes in health behaviour: Evidence, issues, and recommendations. Curr. Opin. Psychol. 2015, 5, 1–5. [Google Scholar] [CrossRef]
- Young, I.; Waddell, L.A.; Wilhelm, B.J.; Greig, J. A systematic review and meta-regression of single group, pre-post studies evaluating food safety education and training interventions for food handlers. Food Res. Int. 2020, 128, 108711. [Google Scholar] [CrossRef]
- Schwarzer, R. Self-efficacy in the adoption and maintenance of health behaviors: Theoretcial approaches and a new mode. In Self-Efficacy: Thought Control of Action; Hemisphere: Washington, DC, USA, 1992; pp. 217–243. [Google Scholar]
- Chow, S.; Mullan, B. Predicting food hygiene. An investigation of social factors and past behaviour in an extended model of the health action process approach. Appetite 2010, 54, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Freivogel, C.; Visschers, V.H. Understanding the underlying psychosocial determinants of safe food handling among consumers to mitigate the transmission risk of antimicrobial-resistant bacteria. Int. J. Environ. Res. Public Health 2020, 17, 2546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nisbet, E.K.; Gick, M.L. Can health psychology help the planet? Applying theory and models of health behaviour to environmental actions. Can. Psychol./Psychol. Can. 2008, 49, 296. [Google Scholar] [CrossRef]
- Schüz, B.; Sniehotta, F.F.; Mallach, N.; Wiedemann, A.U.; Schwarzer, R. Predicting transitions from preintentional, intentional and actional stages of change. Health Educ. Res. 2008, 24, 64–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullan, B.; Wong, C.; O’Moore, K. Predicting hygienic food handling behaviour: Modelling the health action process approach. Br. Food J. 2010, 112, 1216–1229. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Gardner, B.; Rebar, A.L. Habit formation and behavior change In Oxford Research Encyclopedia of Psychology; Oxford University Press: New York, NY, USA, 2019; pp. 1–29. [Google Scholar]
- Carden, L.; Wood, W. Habit formation and change. Curr. Opin. Behav. Sci. 2018, 20, 117–122. [Google Scholar] [CrossRef]
- Mergelsberg, E.L.; Mullan, B.A.; Allom, V.; Scott, A. An intervention designed to investigate habit formation in a novel health behaviour. Psychol. Health 2020, 36, 405–426. [Google Scholar] [CrossRef]
- Lally, P.; Gardner, B. Promoting habit formation. Health Psychol. Rev. 2013, 7, S137–S158. [Google Scholar] [CrossRef]
- EFS. Questback EFS Survey; Questback: Oslo, Norway, 2018. [Google Scholar]
- Rebar, A.L.; Gardner, B.; Rhodes, R.E.; Verplanken, B. The measurement of habit. In The Psychology of Habit; Springer: Berlin/Heidelberg, Germany, 2018; pp. 31–49. [Google Scholar]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27, 379. [Google Scholar] [CrossRef] [Green Version]
- Kok, G.; Gottlieb, N.H.; Peters, G.-J.Y.; Mullen, P.D.; Parcel, G.S.; Ruiter, R.A.; Fernández, M.E.; Markham, C.; Bartholomew, L.K. A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychol. Rev. 2016, 10, 297–312. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.; Cane, J.; Wood, C.E. The behaviour change techniques taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behaviour change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Ojo, S.O.; Bailey, D.P.; Brierley, M.L.; Hewson, D.J.; Chater, A.M. Breaking barriers: Using the behavior change wheel to develop a tailored intervention to overcome workplace inhibitors to breaking up sitting time. BMC Public Health 2019, 19, 1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freivogel, C.; Visschers, V.H. Antimicrobial-resistant bacteria in food: Which behaviour change strategies increase consumers’ risk awareness and preventive food-handling behaviour? Health Psychol. Behav. Med. 2021, 9, 350–379. [Google Scholar] [CrossRef] [PubMed]
- Chambers, D.; Chambers, E.; Godwin, S.; Doan, A.; Cates, S. Developing a messaging graphic for storage times of refrigerated ready to eat (RTE) foods for a consumer food safety health campaign. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 859–875. [Google Scholar] [CrossRef]
- Ashford, S.; Edmunds, J.; French, D.P. What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. Br. J. Health Psychol. 2010, 15, 265–288. [Google Scholar] [CrossRef] [Green Version]
- Knittle, K.; Nurmi, J.; Crutzen, R.; Hankonen, N.; Beattie, M.; Dombrowski, S.U. How can interventions increase motivation for physical activity? A systematic review and meta-analysis. Health Psychol. Rev. 2018, 12, 211–230. [Google Scholar] [CrossRef]
- Bishop, F.M. Self-guided change: The most common form of long-term, maintained health behavior change. Health Psychol. Open 2018, 5, 1–14. [Google Scholar] [CrossRef]
- Carey, R.N.; Connell, L.E.; Johnston, M.; Rothman, A.J.; de Bruin, M.; Kelly, M.P.; Michie, S. Behavior change techniques and their mechanisms of action: A synthesis of links described in published intervention literature. Ann. Behav. Med. 2019, 53, 693–707. [Google Scholar] [CrossRef] [Green Version]
- Garssen, B. Repression: Finding our way in the maze of concepts. J. Behav. Med. 2007, 30, 471–481. [Google Scholar] [CrossRef] [Green Version]
- Locke, E.A.; Latham, G.P. The development of goal setting theory: A half century retrospective. Motiv. Sci. 2019, 5, 93. [Google Scholar] [CrossRef]
- Phillips, L.A.; Gardner, B. Habitual exercise instigation (vs. execution) predicts healthy adults’ exercise frequency. Health Psychol. 2016, 35, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwasnicka, D.; Presseau, J.; White, M.; Sniehotta, F.F. Does planning how to cope with anticipated barriers facilitate health-related behaviour change? A systematic review. Health Psychol. Rev. 2013, 7, 129–145. [Google Scholar] [CrossRef]
- FSO. Bevölkerungsstand und -Entwicklung (Population Size and Developement). Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/bevoelkerung/stand-entwicklung.html (accessed on 23 February 2020).
- Krebs, P.; Prochaska, J.O.; Rossi, J.S. A meta-analysis of computer-tailored interventions for health behavior change. Prev. Med. 2010, 51, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twisk, J.W. Applied Multilevel Analysis: A Practical Guide for Medical Researchers; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- IBM. SPSS Statistics for Windows, 25.0; IBM: Endicott, NY, USA, 2017. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Dima, A.L. Scale validation in applied health research: Tutorial for a 6-step R-based psychometrics protocol. Health Psychol. Behav. Med. 2018, 6, 136–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Ark, L.A. Mokken scale analysis in R. J. Stat. Softw. 2007, 20, 1–19. [Google Scholar] [CrossRef]
- Van der Ark, L.A. New developments in Mokken scale analysis in R. J. Stat. Softw. 2012, 48, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Sijtsma, K.; Molenaar, I.W. Introduction to Nonparametric Item Response Theory; Sage: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Peters, G.-J. The alpha and the omega of scale reliability and validity: Why and how to abandon Cronbach’s alpha and the route towards more comprehensive assessment of scale quality. Eur. Health Psychol. 2018, 16, 56–69. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I.M. The health belief model and preventive health behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D. Nlme: Linear and Nonlinear Mixed Effects Models; R Package 3.1-151; R Development Core Team: New York, NY, USA, 2020. [Google Scholar]
- Field, A.P.; Miles, J.; Field, Z. Discovering Statistics Using R; Sage: London, UK, 2012. [Google Scholar]
- Aiken, L.S.; West, S.G.; Reno, R.R. Multiple Regression: Testing and Interpreting Interactions; Sage: New York, NY, USA, 1991. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics, 6th ed.; Pearson: Boston, MA, USA, 2007. [Google Scholar]
- Chyung, S.Y.; Hutchinson, D.; Shamsy, J.A. Evidence-Based Survey Design: Ceiling Effects Associated with Response Scales. Perform. Improv. 2020, 59, 6–13. [Google Scholar] [CrossRef]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211. [Google Scholar] [CrossRef] [Green Version]
- Maas, C.J.; Hox, J.J. Sufficient sample sizes for multilevel modeling. Methodology 2005, 1, 86–92. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | ||||||||
|---|---|---|---|---|---|---|---|---|
| Tailored(n = 268) | Generic(n = 280) | Control(n = 381) | ||||||
| n | % | n | % | n | % | χ2 (df) | p | |
| Gender | 0.43 | 0.81 | ||||||
| Male | 118 | 44.0 | 116 | 41.4 | 160 | 42.0 | ||
| Female | 150 | 56.0 | 164 | 58.6 | 221 | 58.0 | ||
| Education level1 | 2.62 | 0.62 | ||||||
| Primary or secondary school | 14 | 5.2 | 19 | 6.8 | 19 | 5.0 | ||
| Vocational or higher secondary school | 156 | 58.2 | 150 | 53.6 | 225 | 59.1 | ||
| College/University degree | 97 | 36.2 | 111 | 39.6 | 137 | 36.0 | ||
| Household composition1 | 11.57 | 0.07 | ||||||
| Single-person household | 67 | 25.0 | 52 | 18.6 | 89 | 23.4 | ||
| With partner | 77 | 28.7 | 99 | 35.4 | 139 | 36.5 | ||
| With children | 91 | 34.0 | 108 | 38.6 | 123 | 32.3 | ||
| Another household composition | 32 | 11.9 | 21 | 7.5 | 30 | 7.9 | ||
| M | (SD) | M | (SD) | M | (SD) | F (df) | p | |
| Age | 43.52 | (14.27) | 43.80 | (13.52) | 45.90 | (13.50) | 3.01 (2, 926) | 0.05 |
| Frequency of preparing… | ||||||||
| Raw red meat | 3.60 | (1.08) | 3.67 | (1.05) | 3.64 | (1.14) | 0.26 (2, 926) | 0.77 |
| Raw poultry | 3.36 | (1.10) | 3.26 | (1.12) | 3.39 | (1.16) | 1.03 (2, 926) | 0.36 |
| Raw fish/seafood | 2.49 | (1.09) | 2.35 | (1.21) | 2.50 | (1.23) | 1.52 (2, 926) | 0.22 |
| Self-Efficacy | Likelihood | Severity | Positive Outcome Expectancy | Negative Outcome Expectancy | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| γ | 95% CI | γ | 95% CI | γ | 95% CI | γ | 95% CI | γ | 95% CI | |
| Fixed effects level 1 | ||||||||||
| Intercept | 5.55 | 5.41; 5.69 | 3.12 | 2.94; 3.29 | 4.77 | 4.58; 4.96 | 5.67 | 5.51; 5.83 | 3.14 | 2.98; 3.31 |
| Time | 0.18 | −0.01; 0.36 | 0.18 | 0.07; 0.29 | −0.12 | −0.28; 0.03 | 0.06 | −0.20; 0.31 | −0.08 | −0.17; 0.01 |
| Fixed effects level 2 | ||||||||||
| Control condition # | 0.18 | −0.00; 0.37 | 0.17 | −0.05; 0.40 | 0.05 | −0.20; 0.30 | 0.06 | −0.15; 0.26 | −0.06 | −0.27; 0.16 |
| Generic condition # | 0.10 | −0.10; 0.30 | 0.24 | −0.01; 0.48 | 0.16 | −0.11; 0.43 | 0.08 | −0.14; 0.30 | −0.07 | −0.30; 0.16 |
| HAPA phase † | 0.60 | 0.41; 0.79 | 0.21 | −0.03; 0.44 | 0.40 | 0.13; 0.67 | 0.47 | 0.24; 0.70 | −0.37 | −0.59; −0.16 |
| Cross-level interaction | ||||||||||
| Time * control condition | −0.13 | −0.23; −0.02 | −0.20 | −0.34; −0.06 | −0.01 | −0.16; 0.14 | −0.12 | −0.24; 0.01 | 0.11 | −0.00; 0.22 |
| Time * generic condition | 0.07 | −0.04; 0.17 | −0.06 | −0.21; 0.08 | 0.09 | −0.06; 0.25 | −0.02 | −0.15; 0.11 | 0.06 | −0.05; 0.18 |
| Time * HAPA phase * control condition | 0.21 | 0.07; 0.34 | 0.11 | −0.07; 0.29 | 0.05 | −0.14; 0.25 | 0.13 | −0.04; 0.30 | −0.26 | −0.42; −0.11 |
| Time * HAPA phase * generic condition | −0.02 | −0.16; 0.13 | 0.04 | −0.15; 0.23 | −0.09 | −0.30; 0.12 | 0.01 | −0.08; 0.27 | −0.26 | −0.41; −0.10 |
| Random effect variances | ||||||||||
| Intercept | 0.72 | 0.92 | 0.94 | 0.57 | 0.91 | |||||
| Time | 0.02 | 0.05 | ||||||||
| Residuals | 0.32 | 0.57 | 0.88 | 0.65 | 0.48 | |||||
| Corr § | −0.14 | −0.12 | ||||||||
| AIC | 6034.87 | 7358.03 | 7867.48 | 6996.59 | 6746.83 | |||||
| Intention | Coping Planing | Action Control | Habit | Behavior | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| γ | 95% CI | γ | 95% CI | γ | 95% CI | γ | 95% CI | γ | 95% CI | |
| Fixed effects level 1 | ||||||||||
| Intercept | 5.06 | 4.92; 5.20 | 4.01 | 3.80; 4.23 | 4.62 | 4.41; 4.84 | 5.10 | 4.92; 5.29 | 4.39 | 4.27; 4.51 |
| Time | 0.63 | 0.43; 0.82 | 0.57 | 0.23; 0.92 | −0.07 | −0.37 0.21 | 0.07 | −0.15; 0.30 | 0.28 | 0.19; 0.38 |
| Fixed effects level 2 | ||||||||||
| Control condition # | 0.11 | −0.07; 0.30 | 0.18 | −0.10; 0.46 | 0.08 | −0.20; 0.36 | 0.06 | −0.17; 0.30 | 0.11 | −0.04; 0.27 |
| Generic condition # | 0.06 | −0.14; 0.26 | 0.21 | −0.09; 0.52 | 0.17 | −0.13; 0.48 | 0.08 | −0.17; 0.34 | 0.10 | −0.07; 0.27 |
| HAPA phase † | 1.29 | 1.10; 1.48 | 0.74 | 0.43; 1.04 | 0.64 | 0.35; 0.93 | 0.42 | 0.18; 0.65 | 0.19 | 0.02; 0.35 |
| Cross-level interactions | ||||||||||
| Time * control condition | −0.09 | −0.19; 0.02 | −0.09 | −0.27; 0.09 | −0.12 | −0.26; 0.05 | −0.02 | −0.13; 0.10 | −0.09 | −0.19; 0.00 |
| Time * generic condition | 0.09 | −0.02; 0.20 | −0.02 | −0.22; 0.17 | 0.02 | −0.14; 0.20 | 0.02 | −0.10; 0.15 | 0.00 | −0.10; 0.11 |
| Time * HAPA phase * control condition | 0.14 | 0.00; 0.27 | 0.24 | 0.00; 0.48 | 0.23 | 0.01; 0.42 | 0.11 | −0.04; 0.27 | 0.17 | 0.05; 0.30 |
| Time * HAPA phase * generic condition | −0.03 | −0.17; 0.11 | 0.24 | −0.01; 0.50 | 0.15 | −0.09; 0.36 | 0.08 | −0.09; 0.24 | 0.11 | −0.02; 0.24 |
| Random effect variances | ||||||||||
| Intercept | 0.64 | 1.20 | 1.39 | 1.27 | 0.42 | |||||
| Time | 0.01 | 0.05 | 0.00 | 0.03 | 0.01 | |||||
| Residuals | 0.37 | 1.09 | 0.95 | 0.46 | 0.30 | |||||
| Corr § | −0.19 | 0.13 | −0.15 | −0.29 | 0.55 | |||||
| AIC | 6132.07 | 8568.97 | 8116.87 | 7024.09 | 5454.27 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freivogel, C.; Lehmann, S.H.; Visschers, V.H.M. Tailoring Can Improve Consumers’ Hygienic Food-Handling Behavior to Reduce the Transmission Risk of Antimicrobial-Resistant Bacteria through Food. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 169-192. https://doi.org/10.3390/ejihpe12020014
Freivogel C, Lehmann SH, Visschers VHM. Tailoring Can Improve Consumers’ Hygienic Food-Handling Behavior to Reduce the Transmission Risk of Antimicrobial-Resistant Bacteria through Food. European Journal of Investigation in Health, Psychology and Education. 2022; 12(2):169-192. https://doi.org/10.3390/ejihpe12020014
Chicago/Turabian StyleFreivogel, Claudia, Sarah H. Lehmann, and Vivianne H. M. Visschers. 2022. "Tailoring Can Improve Consumers’ Hygienic Food-Handling Behavior to Reduce the Transmission Risk of Antimicrobial-Resistant Bacteria through Food" European Journal of Investigation in Health, Psychology and Education 12, no. 2: 169-192. https://doi.org/10.3390/ejihpe12020014