
Association between Insufficient Sleep and Dental Caries among Preschoolers in Japan: A Cross-Sectional Multicentre Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
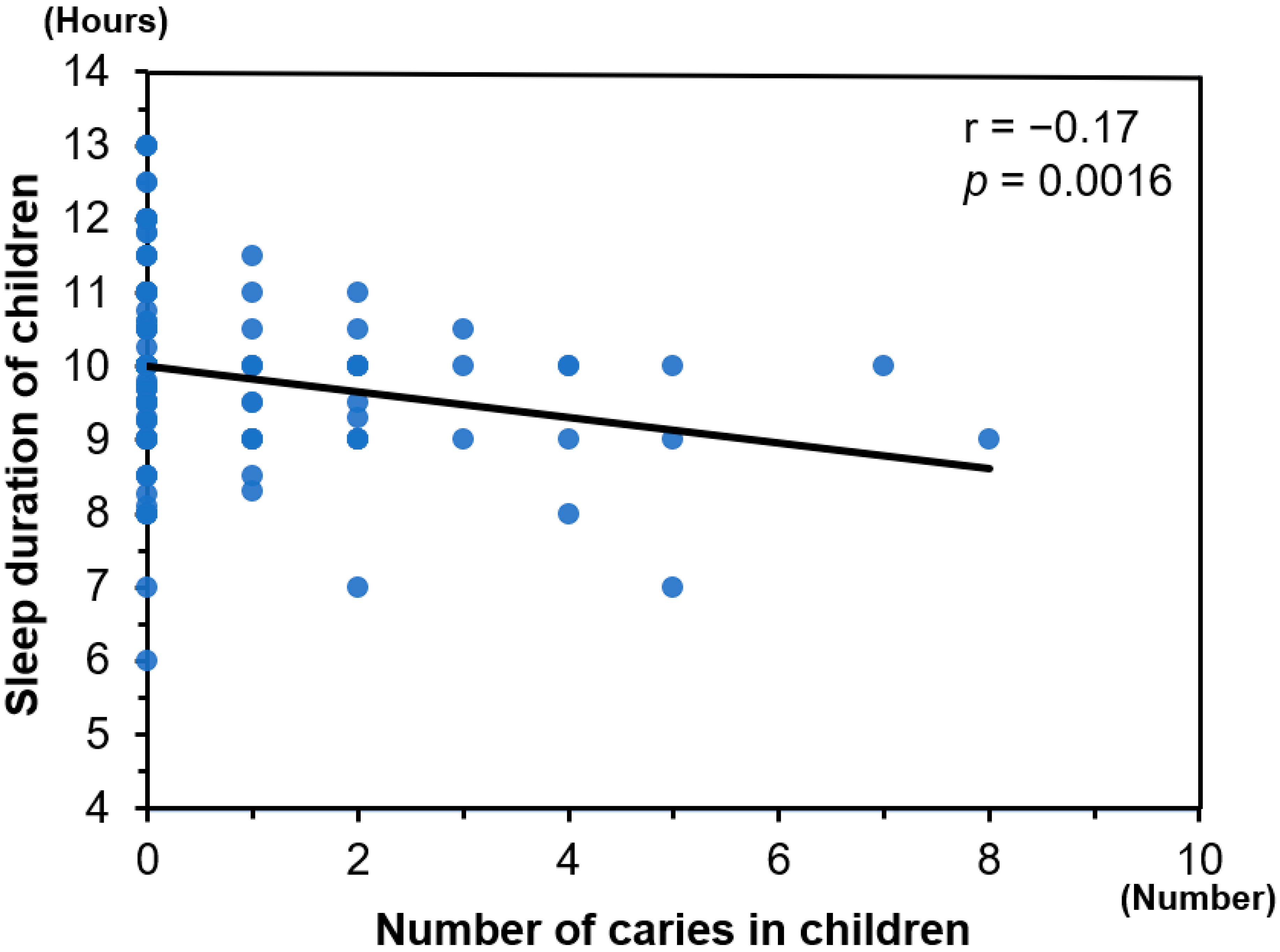
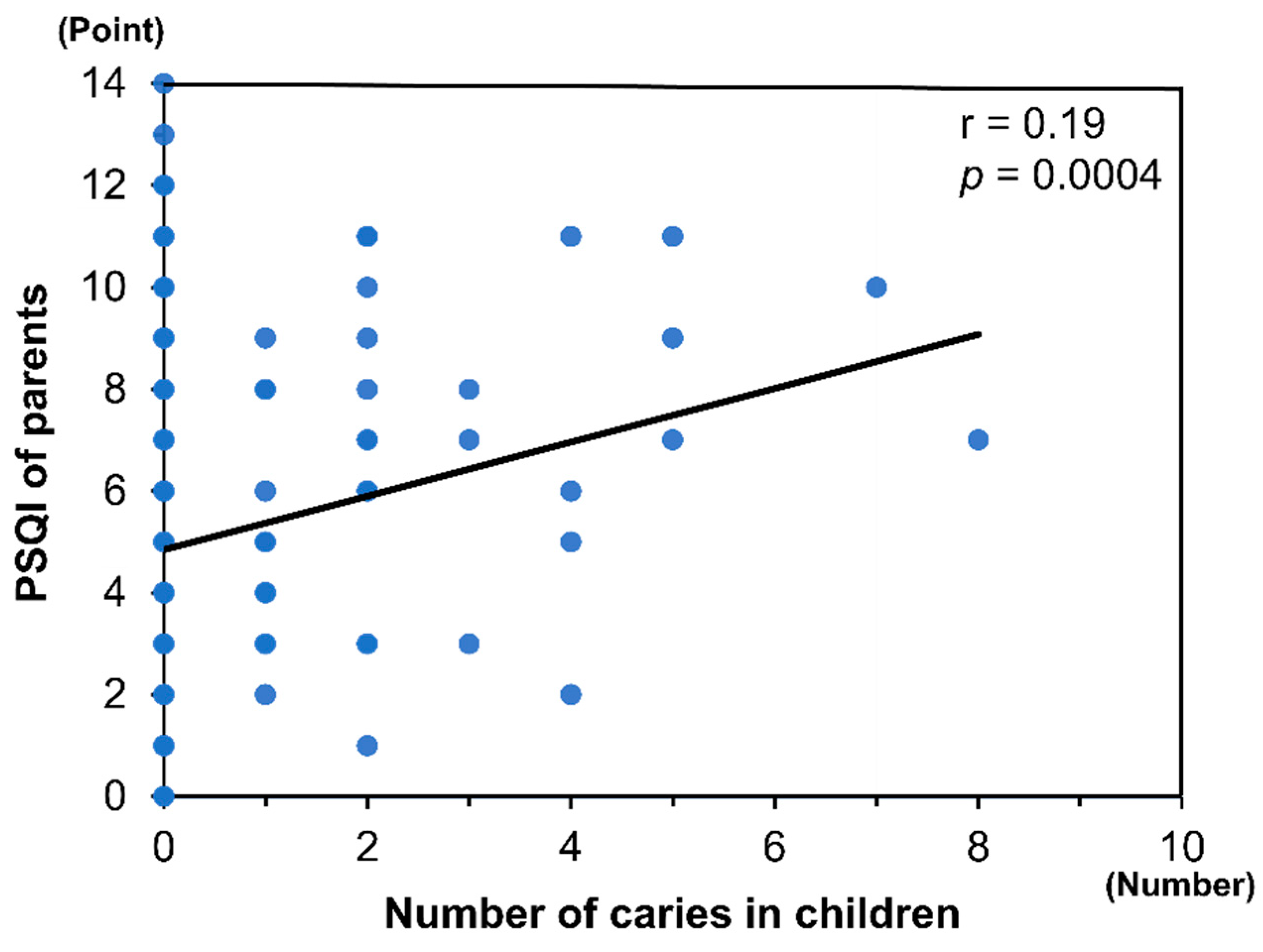
3. Results
4. Discussion
4.1. Main Findings of the Study
4.2. Findings of Previous Studies
4.3. What This Study Adds
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ayhan, H.; Suskan, E.; Yildirim, S. The effect of nursing or rampant caries on height, body weight and head circumference. J. Clin. Pediatr. Dent. 1996, 20, 209–212. [Google Scholar]
- Vinckier, F.; Gizani, S.; Declerck, D. Comprehensive dental care for children with rampant caries under general anaesthesia. Int. J. Paediatr. Dent. 2001, 11, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Greenwell, A.L.; Johnsen, D.; DiSantis, T.A.; Gerstenmaier, J.; Limbert, N. Longitudinal evaluation of caries patterns form the primary to the mixed dentition. Pediatr. Dent. 1990, 12, 278–282. [Google Scholar]
- Li, Y.; Wang, W. Predicting caries in permanent teeth from caries in primary teeth: An eight-year cohort study. J. Dent. Res. 2002, 81, 561–566. [Google Scholar] [CrossRef]
- Luzzi, V.; Fabbrizi, M.; Coloni, C.; Mastrantoni, C.; Mirra, C.; Bossù, M.; Vestri, A.; Polimeni, A. Experience of dental caries and its effects on early dental occlusion: A descriptive study. Ann. Stomatol. 2011, 2, 13–18. [Google Scholar]
- Kirthiga, M.; Murugan, M.; Saikia, A.; Kirubakaran, R. Risk factors for early childhood caries: A systematic review and meta-analysis of case control and cohort studies. Pediatr. Dent. 2019, 41, 95–112. [Google Scholar] [PubMed]
- Archer, S.N.; Oster, H. How sleep and wakefulness influence circadian rhythmicity: Effects of insufficient and mistimed sleep on the animal and human transcriptome. J. Sleep Res. 2015, 24, 476–493. [Google Scholar] [CrossRef]
- Reinhardt, É.L.; Fernandes, P.A.; Markus, R.P.; Fischer, F.M. Short sleep duration increases salivary IL-6 production. Chronobiol. Int. 2016, 33, 780–782. [Google Scholar] [CrossRef]
- Chen, H.; Tanaka, S.; Arai, K.; Yoshida, S.; Kawakami, K. Insufficient sleep and incidence of dental caries in deciduous teeth among children in Japan: A population-based cohort study. J. Pediatr. 2018, 198, 279–286.e5. [Google Scholar] [CrossRef] [Green Version]
- Adil, A.H.; Eusufzai, S.Z.; Kamruddin, A.; Wan Ahmad, W.; Jamayet, N.B.; Karobari, M.I.; Alam, M.K. Assessment of parents’ oral health literacy and its association with caries experience of their preschool children. Children 2020, 7, 101. [Google Scholar] [CrossRef]
- Asaka, Y.; Sekine, M.; Yamada, M.; Tatsuse, T.; Sano, M. Association of short sleep duration and long media use with caries in school children. Pediatr. Int. 2020, 62, 214–220. [Google Scholar] [CrossRef]
- Suka, M.; Odajima, T.; Kasai, M.; Igarashi, A.; Ishikawa, H.; Kusama, M.; Nakayama, T.; Sumitani, M.; Sugimori, H. The 14-item health literacy scale for Japanese adults (HLS-14). Environ. Health Prev. Med. 2013, 18, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Klein, H.; Carroll, C.E.; Knutson, J.W. Studies on dental caries: I. Dental status and dental needs of elementary school children. Public Health Rep. 1938, 53, 751–765. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Smyth, C.A. Evaluating sleep quality in older adults: The Pittsburgh Sleep Quality Index can be used to detect sleep disturbances or deficits. Am. J. Nurs. 2008, 108, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Suma Sogi, H.P.; Hugar, S.M.; Nalawade, T.M.; Sinha, A.; Hugar, S.; Mallikarjuna, R.M. Knowledge, attitude, and practices of oral health care in prevention of early childhood caries among parents of children in Belagavi city: A Questionnaire study. J. Family Med. Prim. Care 2016, 5, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Declerck, D.; Leroy, R.; Martens, L.; Lesaffre, E.; Garcia-Zattera, M.J.; Vanden Broucke, S.; Debyser, M.; Hoppenbrouwers, K. Factors associated with prevalence and severity of caries experience in preschool children. Community Dent. Oral Epidemiol. 2008, 36, 168–178. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, M.; Patel, D.K.; Vyas, A.; Khan, A.J.; McGrady, M.G.; Boothman, N.; Pretty, I.A. Sugar before bed: A simple dietary risk factor for caries experience. Community Dent. Health 2017, 34, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Shantinath, S.D.; Breiger, D.; Williams, B.J.; Hasazi, J.E. The relationship of sleep problems and sleep-associated feeding to nursing caries. Pediatr. Dent. 1996, 18, 375–378. [Google Scholar]
- Martinez, D.; Lenz Mdo, C. Circadian rhythm sleep disorders. Indian J. Med. Res. 2010, 131, 141–149. [Google Scholar]
- Arvidsson, L.; Birkhed, D.; Hunsberger, M.; Lanfer, A.; Lissner, L.; Mehlig, K.; Mårild, S.; Eiben, G. BMI, eating habits and sleep in relation to salivary counts of mutans streptococci in children—The IDEFICS Sweden study. Public Health Nutr. 2016, 19, 1088–1092. [Google Scholar] [CrossRef] [Green Version]
- McEwen, B.S.; Karatsoreos, I.N. Sleep deprivation and circadian disruption: Stress, allostasis, and allostatic load. Sleep Med. Clin. 2015, 10, 1–10. [Google Scholar] [CrossRef]
- Opydo-Szymaczek, J.; Borysewicz-Lewicka, M.; Andrysiak, K.; Witkowska, Z.; Hoffmann-Przybylska, A.; Przybylski, P.; Walicka, E.; Gerreth, K. Clinical Consequences of Dental Caries, Parents’ Perception of Child’s Oral Health and Attitudes towards Dental Visits in a Population of 7-Year-Old Children. Int. J. Environ. Res. Public Health 2021, 18, 5844. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ministry of Health, Labor and Welfare: Japan. Result of the Dental Disease Survey. 2016. Available online: https://www.mhlw.go.jp/toukei/list/dl/62-28-02.pdf (accessed on 5 December 2020).
- Julihn, A.; Soares, F.C.; Hammarfjord, U.; Hjern, A.; Dahllöf, G. Birth order is associated with caries development in young children: A register-based cohort study. BMC Public Health 2020, 20, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marjoribanks, K. Sibling dilution hypothesis: A regression surface analysis. Psychol. Rep. 2001, 89, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, M.; Momma, H.; Sekiguchi, T.; Kuroki, K.; Kanazawa, K.; Watanabe, M.; Hagiwara, Y.; Nagatomi, R. Excessive game playing is associated with poor toothbrushing behavior among athletic children: A cross-sectional study in Miyagi, Japan. Tohoku J. Exp. Med. 2017, 241, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gokhale, N.; Nuvvula, S. Influence of socioeconomic and working status of the parents on the incidence of their children’s dental caries. J. Nat. Sci. Biol. Med. 2016, 7, 127–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanioka, T.; Nakamura, E.; Ojima, M.; Tanaka, K.; Aoyama, H. Dental caries in 3-year-old children and smoking status of parents. Paediatr. Perinat. Epidemiol. 2008, 22, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, D.; Ogawa, M.; Nakamura, T.; Izawa, K.P. Impact of Parents’ Comprehensive Health Literacy on BMI in Children: A Multicenter Cross-Sectional Study in Japan. J. Sch. Health. 2018, 88, 910–916. [Google Scholar] [CrossRef]
- Ogi, H.; Nakamura, D.; Ogawa, M.; Nakamura, T.; Izawa, K.P. Associations between parents’ health literacy and sleeping hours in children: A cross-sectional study. Healthcare 2018, 6, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, S.; Ogi, H.; Ogawa, M.; Nakamura, D.; Nakamura, T.; Izawa, K.P. Relationship between parents’ health literacy and children’s sleep problems in Japan. BMC Public Health 2021, 21, 791. [Google Scholar] [CrossRef]
- Ogi, H.; Nakamura, D.; Ogawa, M.; Nakamura, T.; Izawa, K.P. Association between parents’ social capital and physical status in preschool children in Japan: A cross-sectional multicentre study. Matern. Child. Health J. 2021, 25, 1607–1614. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 332) | with Caries Experience (n = 42) | without Caries Experience (n = 290) | p Value | |
|---|---|---|---|---|
| Child | ||||
| Age, months | 64.4 ± 10.1 | 66.9 ± 9.1 | 64.1 ± 10.2 | 0.089 |
| Sex, female, n (%) | 154 (46.4) | 15 (35.7) | 139 (47.9) | 0.896 |
| BMI, kg/m2 | 15.6 ± 1.5 | 15.9 ± 1.7 | 15.6 ± 1.5 | 0.158 |
| Birth weight, g | 3015.3 ± 435.5 | 3021.6 ± 370.8 | 3014.4 ± 444.6 | 0.920 |
| Number of siblings, n | 2.3 ± 0.8 | 2.5 ± 1.2 | 2.2 ± 0.8 | 0.094 |
| Breakfast, every day, n (%) | 311 (93.7) | 36 (85.7) | 275 (94.8) | 0.023 |
| Extracurricular activities, yes, n (%) | 145 (43.7) | 12 (28.6) | 133 (45.9) | 0.003 |
| Sleep duration, h | 9.9 ± 1.0 | 9.5 ± 0.9 | 10.0 ± 1.0 | 0.002 |
| TV time, h | 2.1 ± 1.2 | 2.6 ± 1.4 | 2.0 ± 1.2 | 0.003 |
| Game time, h | 0.5 ± 0.7 | 0.8 ± 0.9 | 0.5 ± 0.7 | 0.027 |
| Screen time, h | 2.6 ± 1.5 | 3.3 ± 1.9 | 2.5 ± 1.4 | 0.000 |
| Parent | ||||
| Age, year | 36.1 ± 5.3 | 35.4 ± 6.5 | 36.2 ± 5.1 | 0.387 |
| Sex, female | 311 (93.7) | 41 (97.6) | 270 (93.1) | 0.261 |
| BMI, kg/m2 | 21.5 ± 3.3 | 21.7 ± 4.4 | 21.4 ± 3.1 | 0.609 |
| Smoking, yes, n (%) | 44 (13.2) | 13 (30.7) | 31 (10.7) | 0.003 |
| Drinking, every day, n (%) | 37 (11.1) | 4 (9.5) | 33 (11.4) | 0.721 |
| Marital status, married, n (%) | 313 (94.2) | 38 (85.7) | 277 (95.0) | 0.011 |
| Working, yes, n (%) | 233 (70.2) | 30 (71.4) | 203 (70.0) | 0.850 |
| Education, years | 13.4 ± 1.6 | 12.7 ± 1.7 | 13.5 ± 1.6 | 0.003 |
| Household income, >6 million, n (%) | 119 (36.2) | 11 (26.2) | 108 (37.6) | 0.1495 |
| PSQI, points | 5.0 ± 2.7 | 6.0 ± 2.8 | 4.9 ± 2.7 | 0.010 |
| Health literacy, points | 54.8 ± 7.3 | 53.5 ± 7.2 | 56.0 ± 7.8 | 0.040 |
| Variables | Univariate Model | Multivariate Model | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Child | ||||
| Sleep duration | 0.58 (0.41–0.82) | 0.0018 | 0.54 (0.36–0.80) | 0.0012 |
| Screen time | 1.40 (1.15–1.70) | 0.0010 | 1.35 (1.09–1.66) | 0.0051 |
| Age | 1.03 (1.00–1.06) | 0.0910 | ||
| Sex, female | 0.60 (0.31–1.18) | 0.1407 | ||
| Breakfast, not every day | 3.06 (1.11–8.38) | 0.0436 | ||
| Extracurricular activities | 0.47 (0.23–0.96) | 0.0314 | ||
| Parent | ||||
| Age | 0.97 (0.92–1.03) | 0.0274 | ||
| Sex, female | 0.33 (0.04–2.52) | 0.2847 | ||
| PSQI | 1.16 (1.03–1.30) | 0.014 | 1.06 (0.94–1.21) | 0.344 |
| Smoking, no | 3.75 (1.76–7.95) | 0.0011 | 3.91 (1.72–8.89) | 0.0017 |
| Marital status, no | 3.55 (1.27–9.92) | 0.0157 | ||
| Health literacy | 1.05 (1.00–1.11) | 0.0335 | ||
| Education | 0.75 (0.62–0.91) | 0.0039 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogawa, M.; Ogi, H.; Nakamura, D.; Nakamura, T.; Izawa, K.P. Association between Insufficient Sleep and Dental Caries among Preschoolers in Japan: A Cross-Sectional Multicentre Study. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1-10. https://doi.org/10.3390/ejihpe12010001
Ogawa M, Ogi H, Nakamura D, Nakamura T, Izawa KP. Association between Insufficient Sleep and Dental Caries among Preschoolers in Japan: A Cross-Sectional Multicentre Study. European Journal of Investigation in Health, Psychology and Education. 2022; 12(1):1-10. https://doi.org/10.3390/ejihpe12010001
Chicago/Turabian StyleOgawa, Masato, Hiroto Ogi, Daisuke Nakamura, Teruo Nakamura, and Kazuhiro P. Izawa. 2022. "Association between Insufficient Sleep and Dental Caries among Preschoolers in Japan: A Cross-Sectional Multicentre Study" European Journal of Investigation in Health, Psychology and Education 12, no. 1: 1-10. https://doi.org/10.3390/ejihpe12010001