
Lipocalin, Resistin and Gut Microbiota-Derived Propionate Could Be Used to Predict Metabolic Bariatric Surgery Selected Outcomes

 , ,
, ,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
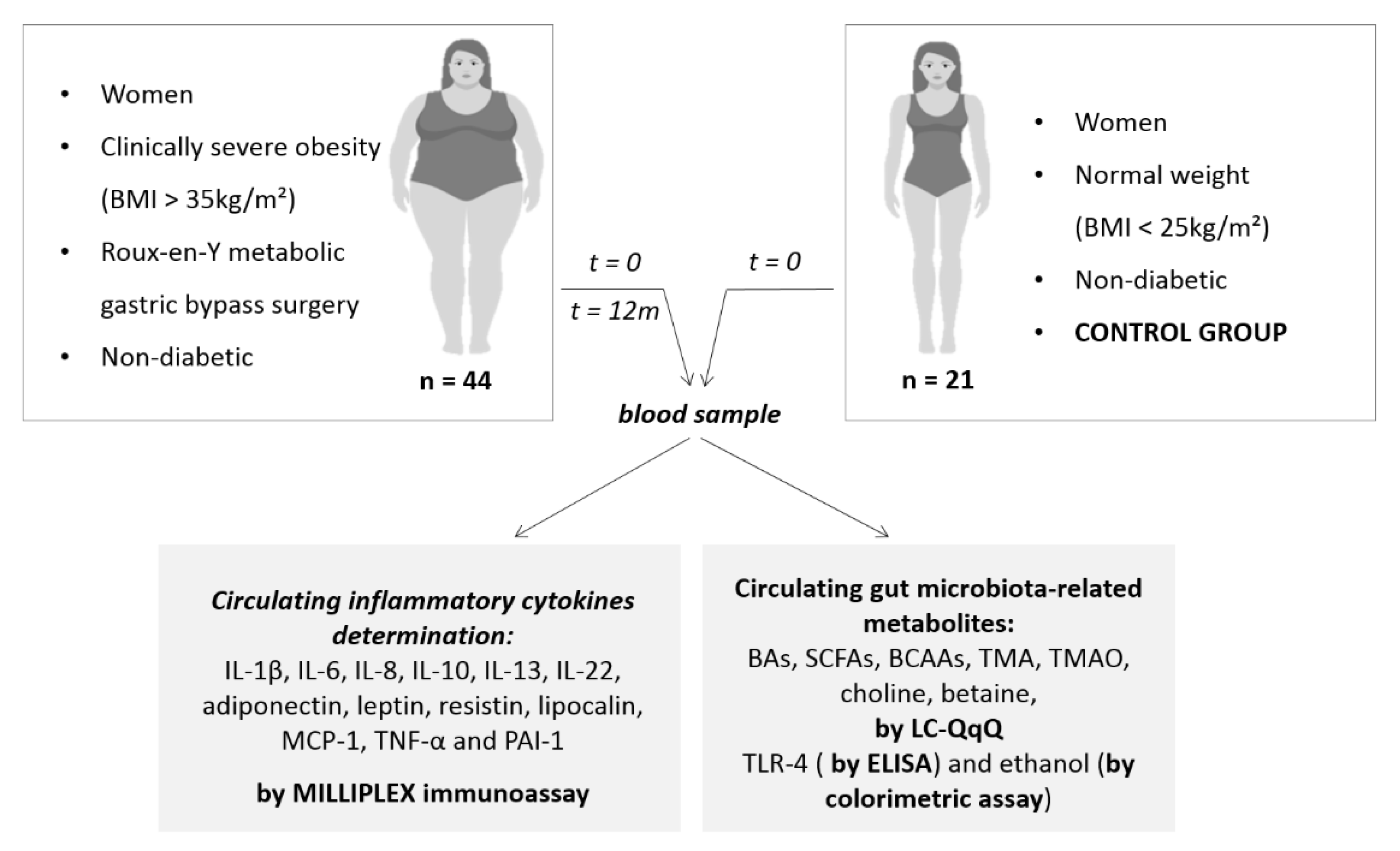
2.1. Subjects
2.2. Anthropometrical and Biochemical Analysis
2.3. Plasma Measurements
2.4. Statistical Analysis
3. Results
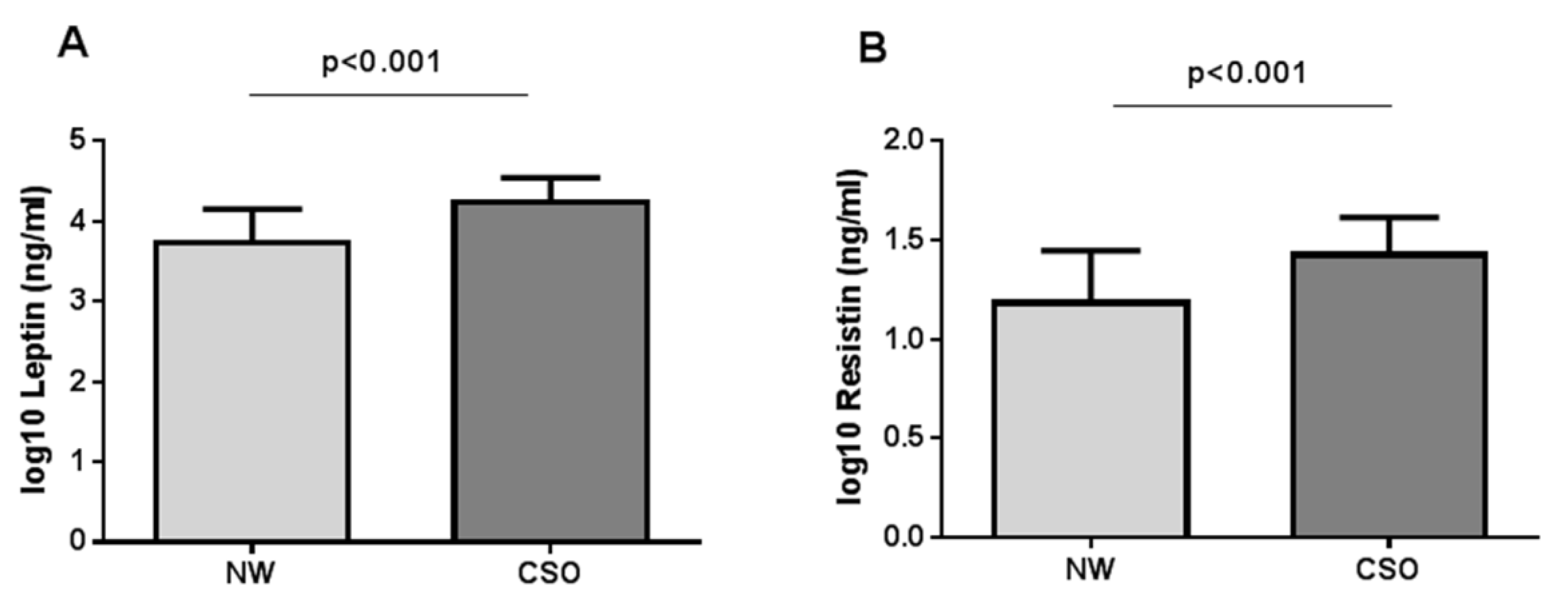
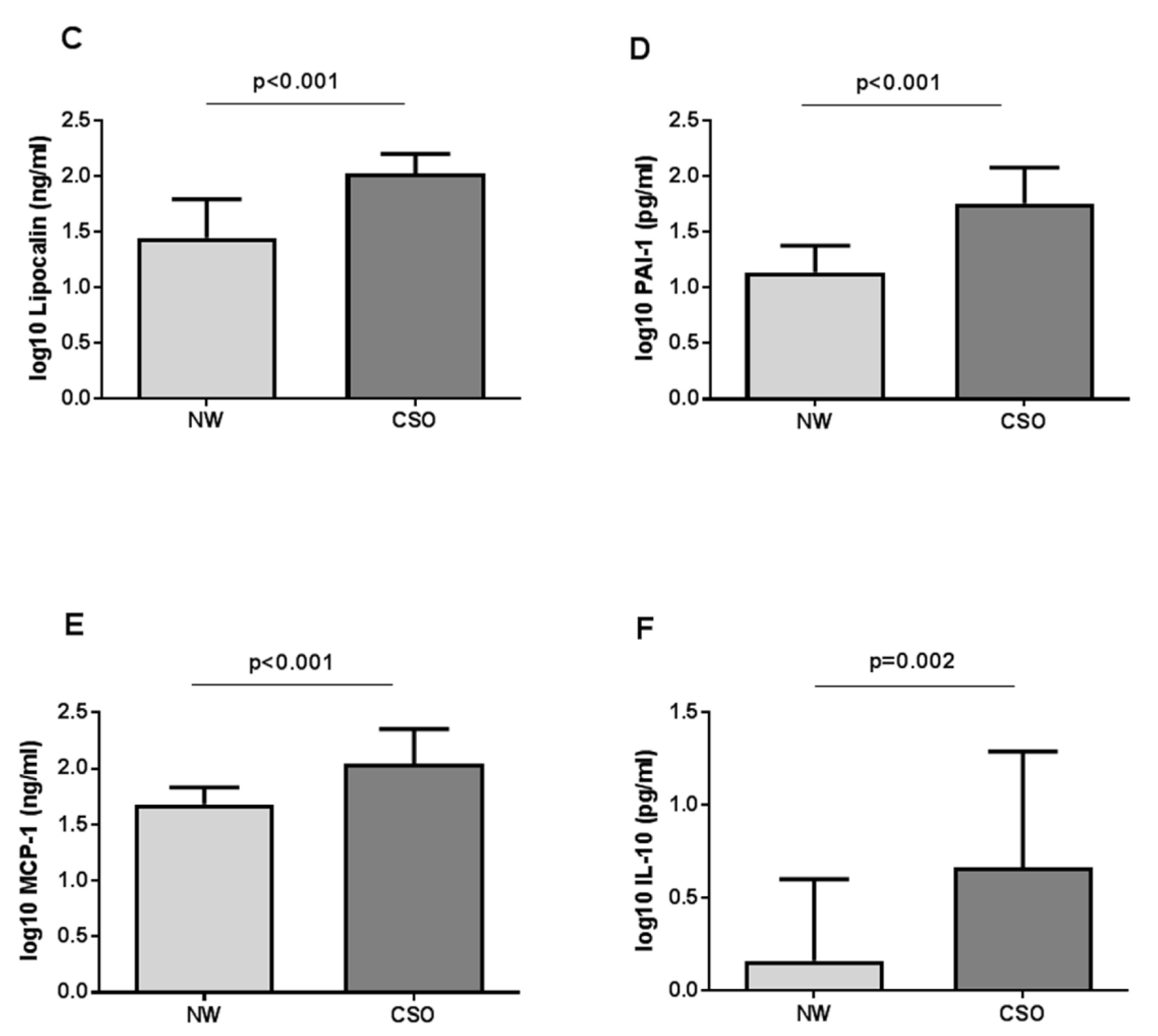
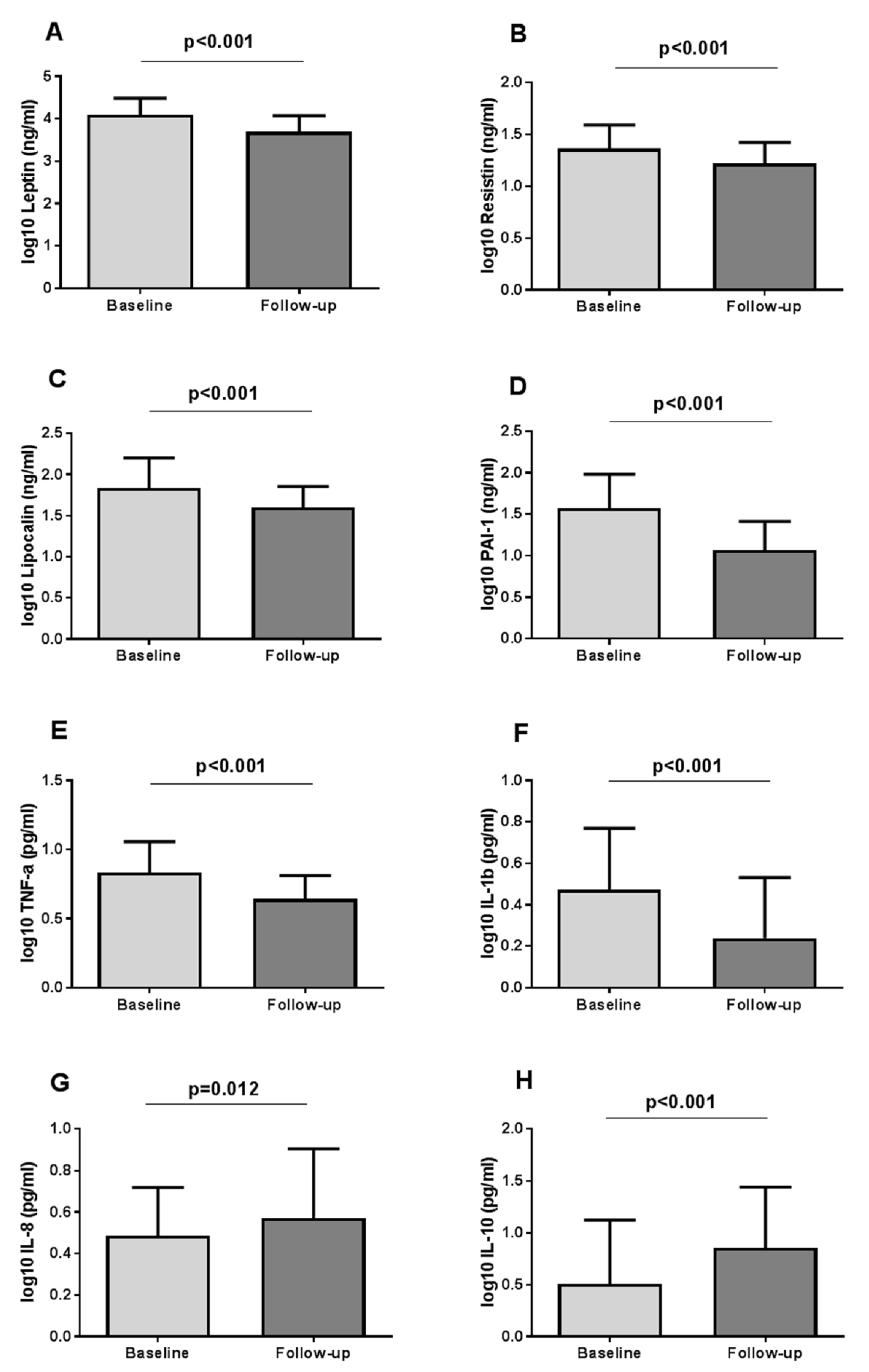
3.1. Characteristics of Patients and Adipocytokine Levels at Baseline and Postsurgery
3.2. Intestinal Microbiota-Derived Metabolites Levels in Serum Samples of the Population Studied
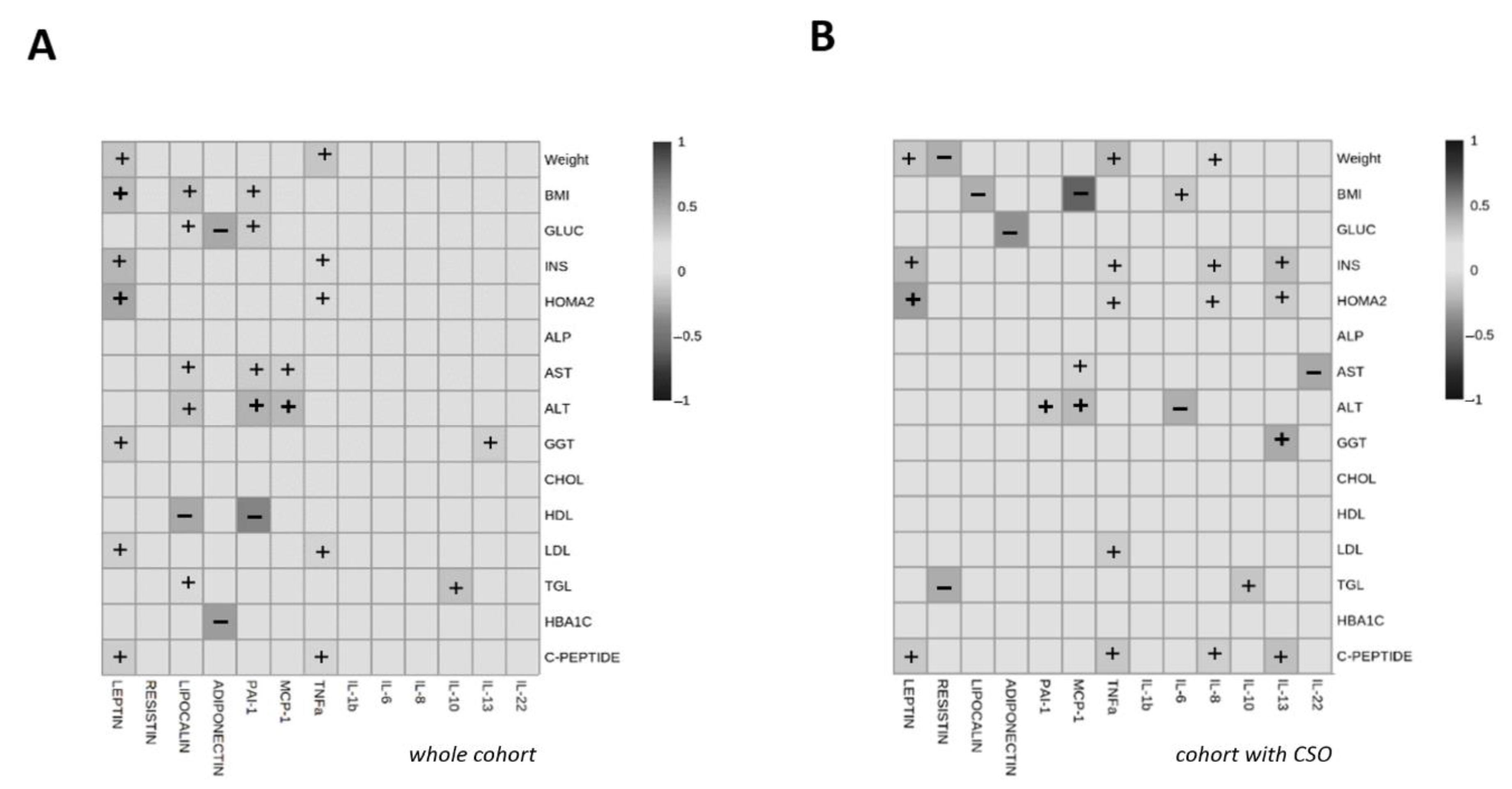
3.3. Correlations of Circulating Interleukin and Other Adipocytokine Levels with Anthropometrical Measures and with Metabolic Parameters
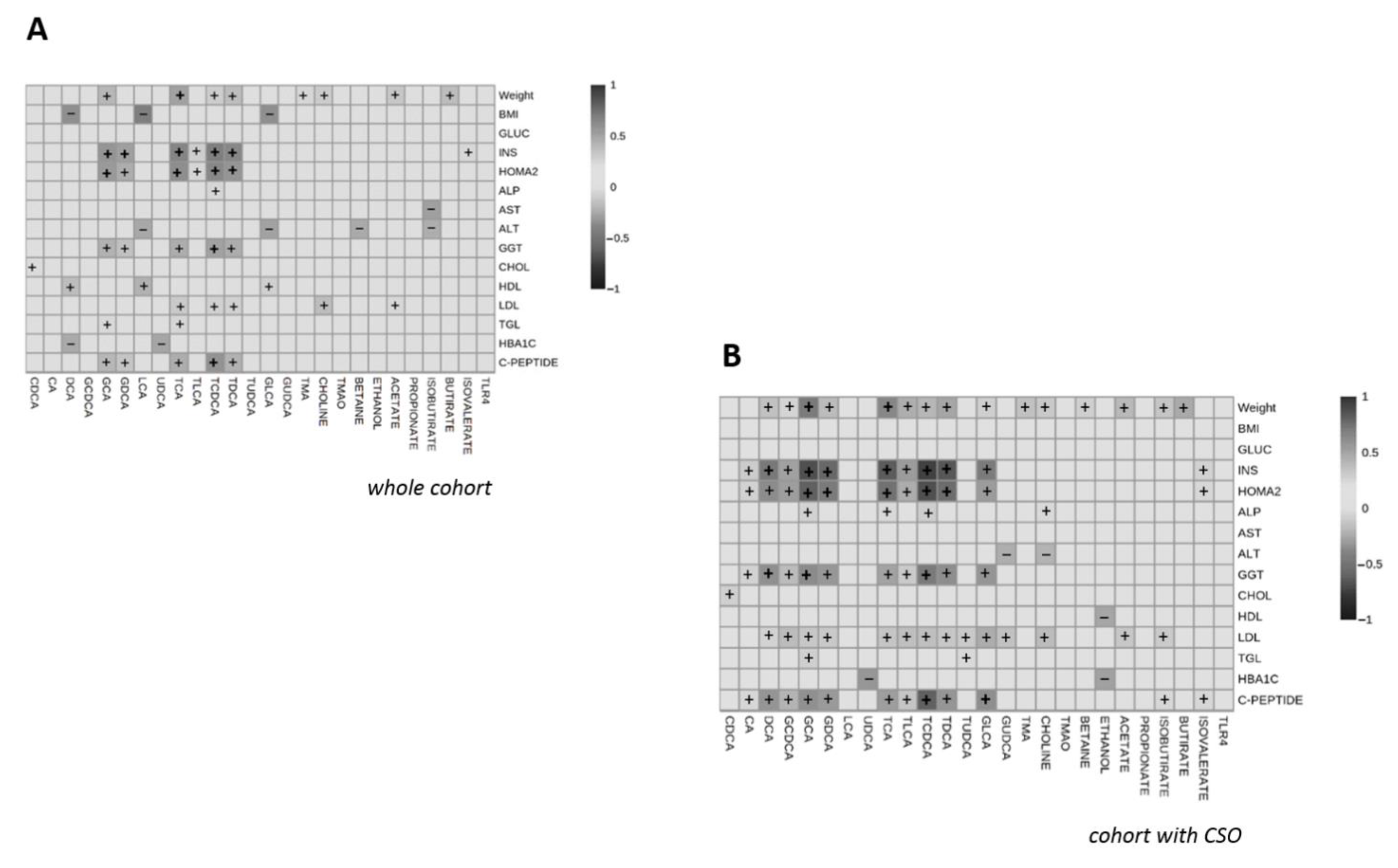
3.4. Correlations of Gut Microbiota Derived-Metabolites Levels with Anthropometrical Measures and with Metabolic Parameters Measures and with Metabolic Parameters
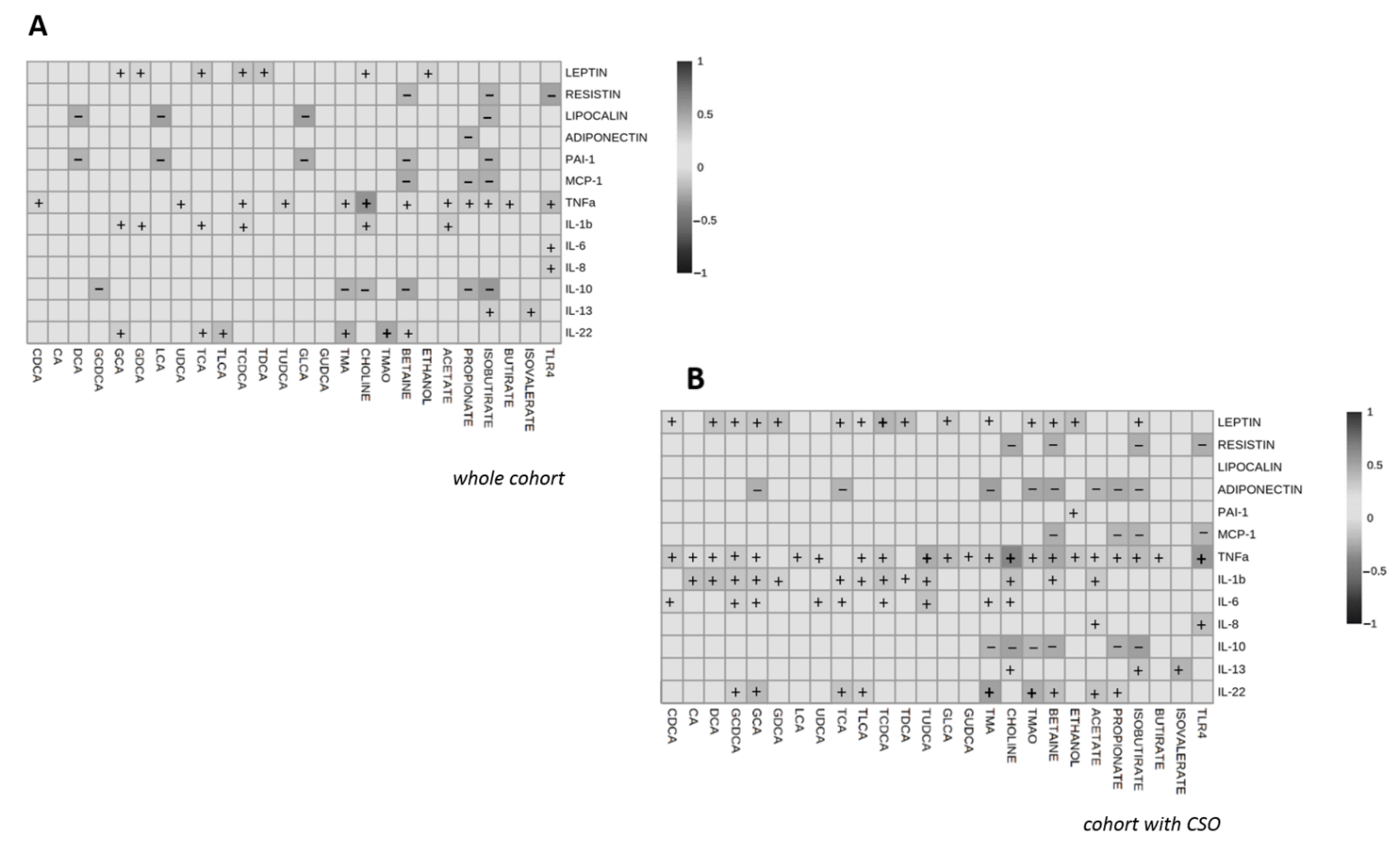
3.5. Correlations of Circulating Interleukin and Other Adipocytokine Levels with Gut Microbiota Derived-Metabolites Levels
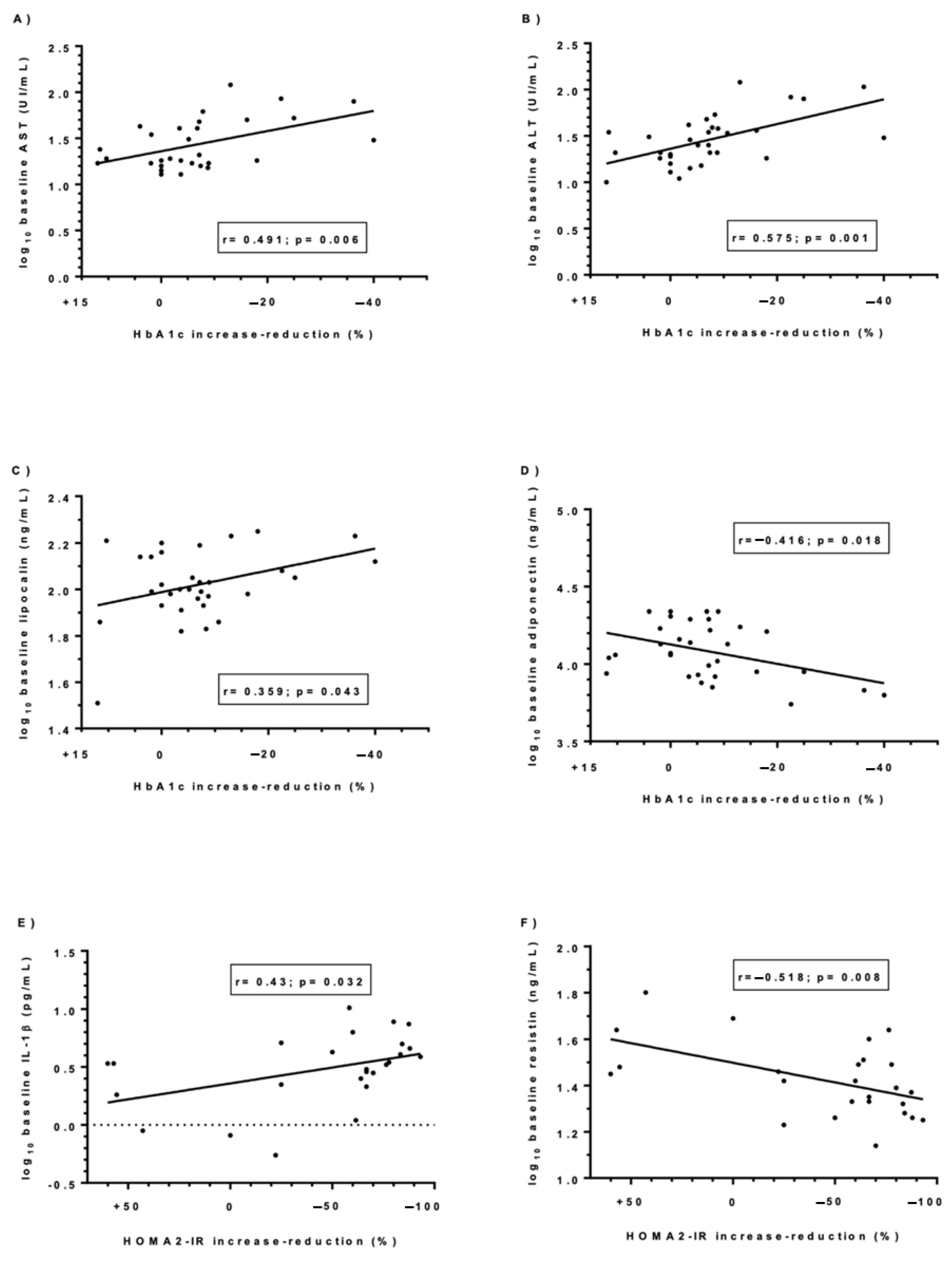
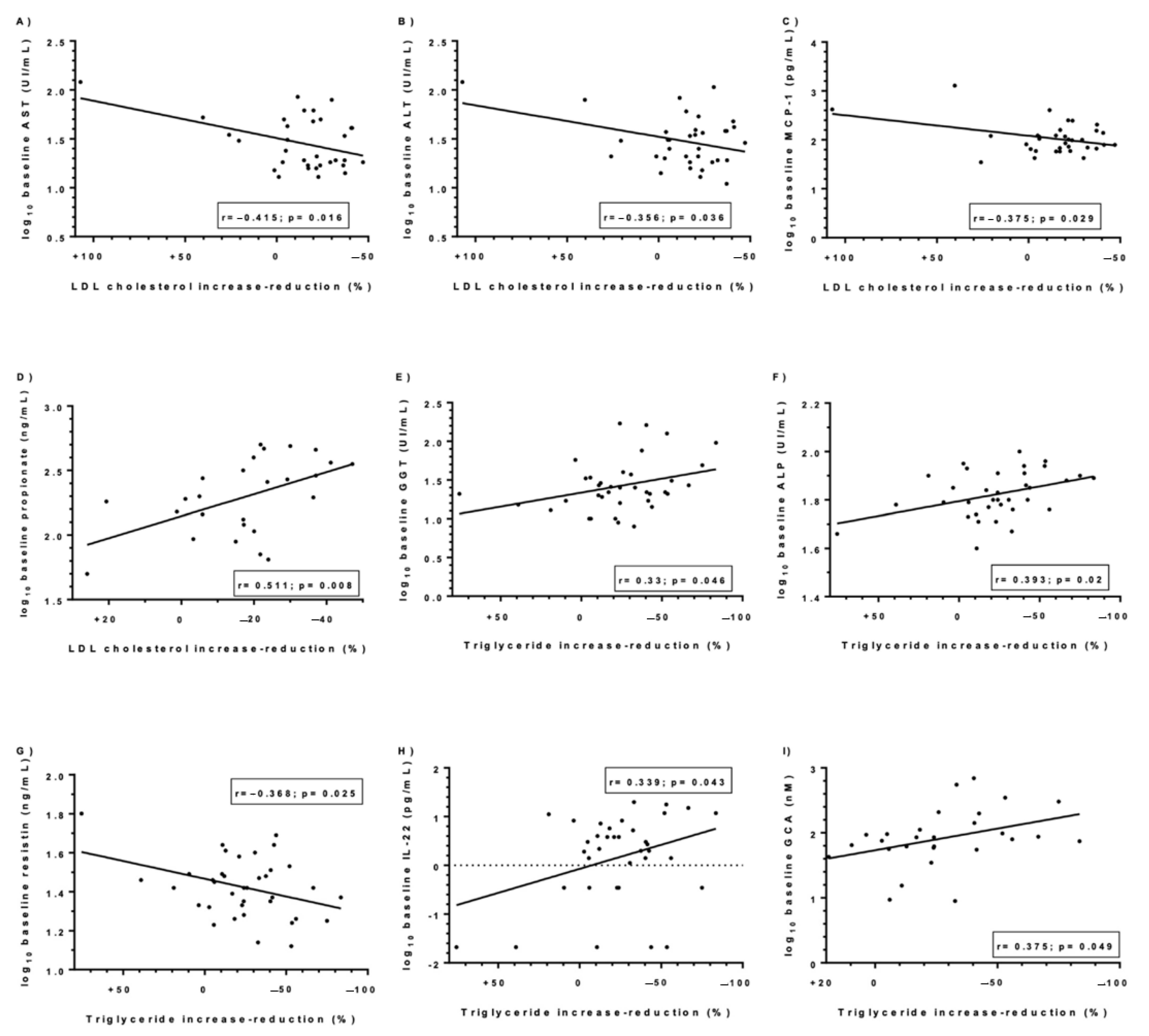
3.6. Predictive Value of Metabolic Parameters, the Preoperative Levels of Adipocytokines/Interleukins and Gut Microbiota-Derived Metabolites on the Changes of BMI and Metabolic Factors
3.7. Evaluation of the Change of the Glycemic Control Reached Postoperatively
3.8. Evaluation of the Lipid Profile Postoperatively
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Smith, C.J.; Perfetti, T.A.; Hayes, A.W.; Berry, S.C. Obesity as a Source of Endogenous Compounds Associated with Chronic Disease: A Review. Toxicol. Sci. 2020, 175, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Magee, C.J.; Barry, J.; Arumugasamy, M.; Javed, S.; Macadam, R.; Kerrigan, D.D. Laparoscopic Sleeve Gastrectomy for High-Risk Patients: Weight Loss and Comorbidity Improvement—Short-Term Results. Obes. Surg. 2011, 21, 547–550. [Google Scholar] [CrossRef]
- Schauer, P.R.; Mingrone, G.; Ikramuddin, S.; Wolfe, B. Clinical Outcomes of Metabolic Surgery: Efficacy of Glycemic Control, Weight Loss, and Remission of Diabetes. Diabetes Care 2016, 39, 902–911. [Google Scholar] [CrossRef] [Green Version]
- Peterli, R.; Wölnerhanssen, B.; Vetter, D.; Nett, P.; Gass, M.; Borbély, Y.; Peters, T.; Schiesser, M.; Schultes, B.; Beglinger, C.; et al. Laparoscopic Sleeve Gastrectomy Versus Roux-Y-Gastric Bypass for Morbid Obesity—3-Year Outcomes of the Prospective Randomized Swiss Multicenter Bypass or Sleeve Study (SM-BOSS). Ann. Surg. 2017, 265, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Higa, K.; Himpens, J.; Buchwald, H.; Scopinaro, N. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes. Surg. 2018, 28, 3783–3794. [Google Scholar] [CrossRef]
- Xu, G.; Song, M. Recent advances in the mechanisms underlying the beneficial effects of bariatric and metabolic surgery. Surg. Obes. Relat. Dis. 2021, 17, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Tham, J.C.; Howes, N.; Le Roux, C.W. The role of bariatric surgery in the treatment of diabetes. Ther. Adv. Chronic Dis. 2014, 5, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Courcoulas, A.P.; Yanovski, S.Z.; Bonds, D.; Eggerman, T.L.; Horlick, M.; Staten, M.A.; David, E. Long-Term Outcomes of Bariatric Surgery: A National Institutes of Health Symposium. JAMA Surg. 2017, 149, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Xanthakos, S.A. Nutritional Deficiencies in Obesity and After Bariatric Surgery. Pediatr. Clin. N. Am. 2009, 56, 1105–1121. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.T.; Varela, J.E. Bariatric surgery for obesity and metabolic disorders: State of the art. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Maggard, M.A.; Shugarman, L.R.; Suttorp, M.; Maglione, M.; Sugerman, H.J.; Livingston, E.H.; Nguyen, N.T.; Li, Z.; Mojica, W.A.; Hilton, L.; et al. Meta-Analysis: Surgical Treatment of Obesity. Ann. Intern. Med. 2005, 142, 547–559. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.-F.; Yan, Y.-X.; Xu, N.; Yin, D.; Hui, Y.; Zhang, J.-P.; Han, G.-J.; Ma, N.; Wu, Y.; Xu, J.-Z.; et al. Predictive Factors of Type 2 Diabetes Mellitus Remission Following Bariatric Surgery: A Meta-analysis. Obes. Surg. 2015, 25, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casajoana, A.; Pujol, J.; Garcia, A.; Elvira, J.; Virgili, N.; De Oca, F.J.; Duran, X.; Fernández-Veledo, S.; Vendrell, J.; Vilarrasa, N. Predictive Value of Gut Peptides in T2D Remission: Randomized Controlled Trial Comparing Metabolic Gastric Bypass, Sleeve Gastrectomy and Greater Curvature Plication. Obes. Surg. 2017, 27, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Ceperuelo-Mallafré, V.; Llauradó, G.; Keiran, N.; Benaiges, E.; Astiarraga, B.; Martínez, L.; Pellitero, S.; González-Clemente, J.M.; Rodríguez, A.; Fernández-Real, J.M.; et al. Preoperative Circulating Succinate Levels as a Biomarker for Diabetes Remission After Bariatric Surgery. Diabetes Care 2019, 42, 2347. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Brethauer, S.A.; Andalib, A.; Nowacki, A.S.; Jimenez, A.; Corcelles, R.; Hanipah, Z.N.; Punchai, S.; Bhatt, D.L.; Kashyap, S.R.; et al. Individualized Metabolic Surgery Score. Ann. Surg. 2017, 266, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Patimah, I.; KhazáAi, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2016, 13, 851–863. [Google Scholar] [CrossRef]
- Stolarczyk, E. Adipose tissue inflammation in obesity: A metabolic or immune response? Curr. Opin. Pharmacol. 2017, 37, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Saad, M.J.A.; Santos, A.; Prada, P.O. Linking Gut Microbiota and Inflammation to Obesity and Insulin Resistance. Physiology 2016, 31, 283–293. [Google Scholar] [CrossRef]
- Bhagwandin, C.; Ashbeck, E.L.; Whalen, M.; Bandola-Simon, J.; Roche, P.; Szajman, A.; Truong, S.M.; Wertheim, B.C.; Klimentidis, Y.C.; Ishido, S.; et al. The E3 ubiquitin ligase MARCH1 regulates glucose-tolerance and lipid storage in a sex-specific manner. PLoS ONE 2018, 13, 1–14. [Google Scholar] [CrossRef]
- Asare, G.; Santa, S.; Ngala, R.; Asiedu, B.; Afriyie, D.; Amoah, A.G. Effect of hormonal contraceptives on lipid profile and the risk indices for cardiovascular disease in a Ghanaian community. Int. J. Women’s Health 2014, 6, 597. [Google Scholar] [CrossRef] [Green Version]
- Askarpour, M.; Alizadeh, S.; Hadi, A.; Symonds, M.E.; Miraghajani, M.; Sheikhi, A.; Ghaedi, E. Effect of Bariatric Surgery on the Circulating Level of Adiponectin, Chemerin, Plasminogen Activator Inhibitor-1, Leptin, Resistin, and Visfatin: A Systematic Review and Meta-Analysis. Horm. Metab. Res. 2020, 52, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.A.; Abdallah, A.; Mikhail, H.; Abdelsalam, A.; Ibrahim, A.H.; Sultan, A.A.E.A.; El-Ghobary, M.; Ismail, A.A.M.; Abouelregal, T.E.; Omar, M.; et al. Long-term Impact of Mini-Gastric Bypass on Inflammatory Cytokines in Cohort of Morbidly Obese Patients: A Prospective Study. Obes. Surg. 2020, 30, 2338–2344. [Google Scholar] [CrossRef] [PubMed]
- Askarpour, M.; Khani, D.; Sheikhi, A.; Ghaedi, E.; Alizadeh, S. Effect of Bariatric Surgery on Serum Inflammatory Factors of Obese Patients: A Systematic Review and Meta-Analysis. Obes. Surg. 2019, 29, 2631–2647. [Google Scholar] [CrossRef] [PubMed]
- Aron-Wisnewsky, J.; Prifti, E.; Belda, E.; Ichou, F.; Kayser, B.D.; Dao, M.C.; Verger, E.; Hedjazil, L.; Bouillot, J.-L.; Chevallier, J.-M.; et al. Major microbiota dysbiosis in severe obesity: Fate after bariatric surgery. Physiol. Behav. 2017, 176, 139–148. [Google Scholar] [CrossRef]
- Aragonès, G.; Colom-Pellicer, M.; Aguilar, C.; Guiu-Jurado, E.; Martínez, S.; Sabench, F.; Porras, J.A.; Riesco, D.; Del Castillo, D.; Richart, C.; et al. Circulating microbiota-derived metabolites: A “liquid biopsy”? Int. J. Obes. 2019, 44, 875–885. [Google Scholar] [CrossRef] [Green Version]
- Heianza, Y.; Sun, D.; Smith, S.R.; Bray, G.A.; Sacks, F.M.; Qi, L. Changes in Gut Microbiota–Related Metabolites and Long-term Successful Weight Loss in Response to Weight-Loss Diets: The POUNDS Lost Trial. Diabetes Care 2018, 41, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Canfora, E.E.; Meex, R.C.R.; Venema, K.; Blaak, E.E. Gut microbial metabolites in obesity, NAFLD and T2DM. Nat. Rev. Endocrinol. 2019, 15, 261–273. [Google Scholar] [CrossRef]
- Belizário, J.E.; Faintuch, J.; Garay-Malpartida, H.M. Gut Microbiome Dysbiosis and Immunometabolism: New Frontiers for Treatment of Metabolic Diseases. Mediat. Inflamm. 2018, 2018, 1–12. [Google Scholar] [CrossRef]
- Rathinam, V.A.; Fitzgerald, K.A. Inflammasome Complexes: Emerging Mechanisms and Effector Functions. Cell 2016, 165, 792–800. [Google Scholar] [CrossRef] [Green Version]
- Dalmas, E.; Rouault, C.; Abdennour, M.; Rovere, C.; Rizkalla, S.; Bar-Hen, A.; Nahon, J.-L.; Bouillot, J.-L.; Guerre-Millo, M.; Clément, K.; et al. Variations in circulating inflammatory factors are related to changes in calorie and carbohydrate intakes early in the course of surgery-induced weight reduction. Am. J. Clin. Nutr. 2013, 94, 450–458. [Google Scholar] [CrossRef]
- Lee, W.-J.; Almulaifi, A.; Tsou, J.J.; Ser, K.-H.; Lee, Y.-C.; Chen, S.-C. Laparoscopic sleeve gastrectomy for type 2 diabetes mellitus: Predicting the success by ABCD score. Surg. Obes. Relat. Dis. 2015, 11, 991–996. [Google Scholar] [CrossRef]
- Still, C.D.; Wood, G.C.; Benotti, P.; Petrick, A.T.; Gabrielsen, J.; Strodel, W.E.; Ibele, A.; Seiler, J.; Irving, B.; Celaya, M.; et al. Preoperative prediction of type 2 diabetes remission after Roux-en-Y gastric bypass surgery: A retrospective cohort study. Lancet Diabetes Endocrinol. 2013, 2, 38–45. [Google Scholar] [CrossRef] [Green Version]
- Aron-Wisnewsky, J.; Sokolovska, N.; Liu, Y.; Comaneshter, D.S.; Vinker, S.; Pecht, T.; Poitou, C.; Oppert, J.-M.; Bouillot, J.-L.; Genser, L.; et al. The advanced-DiaRem score improves prediction of diabetes remission 1 year post-Roux-en-Y gastric bypass. Diabetologia 2017, 60, 1892–1902. [Google Scholar] [CrossRef]
- Ciudin, A.; Fidilio, E.; Ortiz, A.; Pich, S.; Salas, E.; Mesa, J.; Hernández, C.; Simó-Servat, O.; Lecube, A.; Simó, R. Genetic Testing to Predict Weight Loss and Diabetes Remission and Long-Term Sustainability after Bariatric Surgery: A Pilot Study. J. Clin. Med. 2019, 8, 964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ke, Z.; Li, F.; Gao, Y.; Tan, D.; Sun, F.; Zhou, X.; Chen, J.; Lin, X.; Zhu, Z.; Tong, W. The Use of Visceral Adiposity Index to Predict Diabetes Remission in Low BMI Chinese Patients After Bariatric Surgery. Obes. Surg. 2021, 31, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Al Assal, K.; Prifti, E.; Belda, E.; Sala, P.; Clément, K.; Dao, M.-C.; Doré, J.; Levenez, F.; Taddei, C.R.; Fonseca, D.C.; et al. Gut Microbiota Profile of Obese Diabetic Women Submitted to Roux-en-Y Gastric Bypass and Its Association with Food Intake and Postoperative Diabetes Remission. Nutrients 2020, 12, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genua, I.; Ramos, A.; Caimari, F.; Balagué, C.; Sánchez-Quesada, J.L.; Pérez, A.; Miñambres, I. Effects of Bariatric Surgery on HDL Cholesterol. Obes. Surg. 2020, 30, 1793–1798. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | NW (n = 21) | CSO (n = 44) | p-Value |
|---|---|---|---|
| Age (years) | 44.48 ± 8.69 | 49.02 ± 8.18 | 0.060 |
| Weight (kg) | 57.56 ± 7.01 | 112.13 ± 13.27 | <0.001 * |
| BMI (kg/m2) | 21.97 ± 2.03 | 42.89 ± 5.14 | <0.001 * |
| Glucose (Log10 mg/dL) | 1.90 ± 0.04 | 1.97 ± 0.14 | 0.006 * |
| Insulin (Log10 mU/L) | 0.76 ± 0.13 | 0.98 ± 0.33 | 0.003 * |
| A1C (Log10 %) | 0.73 ± 0.03 | 0.76 ± 0.07 | 0.222 |
| HOMA2-IR (Log10) | −0.14 ± 0.13 | 0.10 ± 0.33 | 0.002 * |
| Cholesterol (Log10 mg/dL) | 2.26 ± 0.08 | 2.24 ± 0.10 | 0.526 |
| HDL-C (Log10 mg/dL) | 1.84 ± 0.09 | 1.64 ± 0.10 | <0.001 * |
| LDL-C (Log10 mg/dL) | 1.98 ± 0.13 | 2.01 ± 0.13 | 0.463 |
| Triglycerides (Log10 mg/dL) | 1.80 ± 0.19 | 2.06 ± 0.21 | <0.001 * |
| AST (Log10 UI/L) | 1.27 ± 0.10 | 1.41 ± 0.25 | 0.002 * |
| ALT (Log10 UI/L) | 1.22 ± 0.16 | 1.44 ± 0.25 | 0.001 * |
| GGT (Log10 UI/L) | 1.14 ± 0.14 | 1.40 ± 0.31 | <0.001 * |
| ALP (Log10 UI/L) | 1.75 ± 0.10 | 1.82 ± 0.09 | 0.012 * |
| C-Peptide (Log10 ng/mL) | 0.05 ± 0.11 | 0.27 ± 0.20 | 0.002 * |
| Variables | Baseline | Follow-Up | p-Value |
|---|---|---|---|
| Weight (kg) | 112.13 ± 13.27 | 78.54 ± 14.13 | <0.001 * |
| BMI (kg/m2) | 42.89 ± 5.14 | 30.04 ± 5.34 | <0.001 * |
| Glucose (Log10 mg/dL) | 1.97 ± 0.14 | 1.91 ± 0.05 | 0.003 * |
| Insulin (Log10 mU/L) | 0.96 ± 0.29 | 0.55 ± 0.27 | <0.001 * |
| HbA1C (Log10 %) | 0.76 ± 0.07 | 0.72 ± 0.05 | 0.002 * |
| HOMA2-IR (Log10) | 0.07 ± 0.29 | −0.33 ± 0.27 | <0.001 * |
| Cholesterol (Log10 mg/dL) | 2.24 ± 0.10 | 2.22 ± 0.06 | 0.139 |
| HDL-C (Log10 mg/dL) | 1.64 ± 0.10 | 1.78 ± 0.08 | <0.001 * |
| LDL-C (Log10 mg/dL) | 2.01 ± 0.13 | 1.93 ± 0.12 | <0.001 * |
| Triglycerides (Log10 mg/dL) | 2.06 ± 0.21 | 1.90 ± 0.14 | <0.001 * |
| AST (Log10 UI/L) | 1.41 ± 0.25 | 1.29 ± 0.12 | 0.002 * |
| ALT (Log10 UI/L) | 1.43 ± 0.25 | 1.25 ± 0.20 | <0.001 * |
| GGT (Log10 UI/L) | 1.40 ± 0.31 | 1.06 ± 0.21 | <0.001 * |
| ALP (Log10 UI/L) | 1.82 ± 0.09 | 1.93 ± 0.09 | <0.001 * |
| C-Peptide (Log10 ng/mL) | 0.24 ± 0.15 | 0.07 ± 0.21 | 0.001 * |
| Variables | NW (n = 21) | CSO (n = 44) | p-Value |
|---|---|---|---|
| Choline (Log 10 µM) | 0.98 ± 0.09 | 1.23 ± 0.18 | <0.001 * |
| TMA (Log 10 nM) | 1.77 ± 0.10 | 1.65 ± 0.32 | 0.077 |
| TMAO (Log 10 µM) | 0.46 ± 0.33 | 0.46 ± 0.32 | 0.973 |
| Betaine (Log 10 µM) | 1.52 ± 0.11 | 1.42 ± 0.15 | 0.011 * |
| TLR4 (Log 10 ng/mL) | 0.44 ± 0.18 | 0.31 ± 0.34 | 0.141 |
| Short chain fatty acids | |||
| Acetate (Log 10 ng/mL) | 3.20 ± 0.24 | 3.20 ± 0.38 | 0.975 |
| Propionate (Log 10 ng/mL) | 2.27 ± 0.07 | 2.31 ± 0.28 | 0.459 |
| Isobutyrate (Log 10 ng/mL) | 1.59 ± 0.80 | 1.52 ± 0.17 | 0.037 * |
| Butyrate (Log 10 ng/mL) | 1.67 ± 0.25 | 1.82 ± 0.27 | 0.053 |
| Isovalerate (Log 10 ng/mL) | 1.42 ± 0.24 | 1.29 ± 0.41 | 0.211 |
| Primary bile acids | |||
| CDCA (Log 10 nM) | 2.04 ± 0.44 | 1.75 ± 0.62 | 0.047 * |
| CA (Log 10 nM) | 1.82 ± 0.60 | 1.70 ± 0.54 | 0.535 |
| GCDCA (Log 10 nM) | 2.52 ± 0.45 | 2.20 ± 0.40 | 0.012 * |
| GCA (Log 10 nM) | 1.93 ± 0.38 | 1.88 ± 0.44 | 0.705 |
| TCA (Log 10 nM) | 1.18 ± 0.33 | 1.32 ± 0.51 | 0.334 |
| TCDCA (Log 10 nM) | 1.72 ± 0.48 | 1.74 ± 0.44 | 0.869 |
| Secondary bile acids | |||
| DCA (Log 10 nM) | 2.38 ± 0.52 | 1.97 ± 0.41 | 0.003 * |
| GDCA (Log 10 nM) | 2.05 ± 0.40 | 1.70 ± 0.45 | 0.006 * |
| LCA (Log 10 nM) | 1.12 ± 0.22 | 1.07 ± 0.19 | 0.460 |
| UDCA (Log 10 nM) | 1.41 ± 0.38 | 1.49 ± 0.63 | 0.656 |
| TLCA (Log 10 nM) | 0.41 ± 0.38 | 0.15 ± 0.45 | 0.045 * |
| TDCA (Log 10 nM) | 1.49 ± 0.43 | 1.07 ± 0.65 | 0.019 * |
| TUDCA (Log 10 nM) | 0.36 ± 0.30 | 0.58 ± 0.32 | 0.022 * |
| GLCA (Log 10 nM) | 1.82 ± 0.30 | 1.29 ± 0.37 | <0.001 * |
| GUDCA (Log 10 nM) | 2.49 ± 0.40 | 2.44 ± 0.51 | 0.755 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auguet, T.; Lopez-Dupla, M.; Ramos, J.; Bertran, L.; Riesco, D.; Aguilar, C.; Ardévol, A.; Pinent, M.; Sabench, F.; Del Castillo, D.; et al. Lipocalin, Resistin and Gut Microbiota-Derived Propionate Could Be Used to Predict Metabolic Bariatric Surgery Selected Outcomes. Processes 2022, 10, 143. https://doi.org/10.3390/pr10010143
Auguet T, Lopez-Dupla M, Ramos J, Bertran L, Riesco D, Aguilar C, Ardévol A, Pinent M, Sabench F, Del Castillo D, et al. Lipocalin, Resistin and Gut Microbiota-Derived Propionate Could Be Used to Predict Metabolic Bariatric Surgery Selected Outcomes. Processes. 2022; 10(1):143. https://doi.org/10.3390/pr10010143
Chicago/Turabian StyleAuguet, Teresa, Miguel Lopez-Dupla, Jessica Ramos, Laia Bertran, David Riesco, Carmen Aguilar, Anna Ardévol, Montserrat Pinent, Fàtima Sabench, Daniel Del Castillo, and et al. 2022. "Lipocalin, Resistin and Gut Microbiota-Derived Propionate Could Be Used to Predict Metabolic Bariatric Surgery Selected Outcomes" Processes 10, no. 1: 143. https://doi.org/10.3390/pr10010143