
Factors Affecting the Initiation of a Shared Decision Making Program in Obstetric Practices

 , ,
, ,
Abstract
:1. Introduction
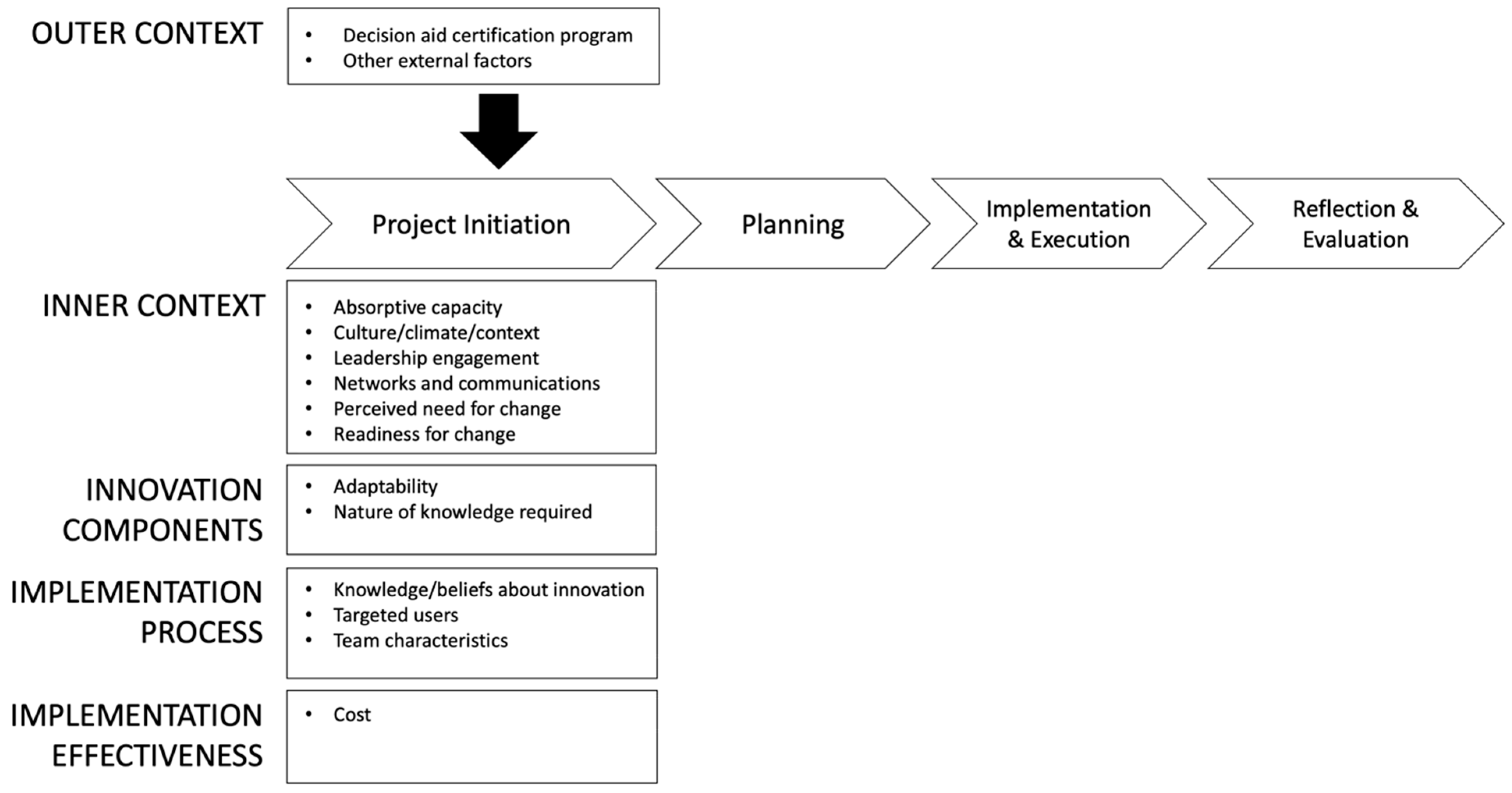
Conceptual Model
2. Material and Methods
2.1. Design
2.2. Study Setting
2.3. Data Sources
2.4. Data Management and Analyses
3. Results
3.1. Inner Context
3.2. Innovation Components
3.3. Implementation Process
3.4. Implementation Effectiveness
3.5. Outer Context
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

| Role | Responsibilities Related to SDM Project | Number of Participants (N = 18) | |||||
|---|---|---|---|---|---|---|---|
| Case Study Site A (n = 4) | Case Study Site B (n = 3) | Case Study Site C (n = 2) | State Government Sponsor (n = 4) | Certified Vendor (n = 4) | Non-Certified Vendor (n = 1) | ||
| Executive sponsor |
| 1 | 0 | 0 | 1 | 0 | 0 |
| Clinical champion |
| 1 | 2 | 1 | 1 | 1 | 0 |
| Project manager/business analyst |
| 1 | 1 | 1 | 1 | 2 | 1 |
| IT analyst/interface engine programmer |
| 1 | 0 | 0 | 0 | 0 | 0 |
| Provider |
| 0 | 0 | 0 | 0 | 0 | 0 |
| Subject matter expert consultant |
| 0 | 0 | 0 | 1 | 1 | 0 |
References
- National Learning Consortium. Shared Decision Making Fact Sheet; HealthIT.gov: Washington, DC, USA, 2013. [Google Scholar]
- Committee on Practice Bulletins-Obstetrics. ACOG Practice Bulletin No. 205. Delivery Vaginal Birth after Cesarean. Obstet. Gynecol. 2019, 133, e110–e127. [Google Scholar] [CrossRef]
- Scaffidi, R.M.; Padden-Denmead, M.L. Use of Shared Decision-Making in Response to Maternal Request for Elective Cesarean Birth. J. Midwifery Womens Health 2020, 65, 808–812. [Google Scholar] [CrossRef]
- Dartmouth-Hitchcock: Center for Shared Decision Making. Resources for Health Care Professionals. 2020. Available online: https://med.dartmouth-hitchcock.org/csdm_toolkits.html (accessed on 16 September 2020).
- Stacey, D.; Légaré, F.; Lewis, K.; Barry, M.J.; Bennett, C.L.; Eden, K.B.; Holmes-Rovner, M.; Llewellyn-Thomas, H.; Lyddiatt, A.; Thomson, R.; et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2017, 4, CD001431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenert, L.; Dunlea, R.; Del Fiol, G.; Hall, L.K. A Model to Support Shared Decision Making in Electronic Health Records Systems. Med Decis. Mak. 2014, 34, 987–995. [Google Scholar] [CrossRef] [Green Version]
- Melnick, E.R.; Lopez, K.; Hess, E.P.; Abujarad, F.; Brandt, C.A.; Shiffman, R.N.; Post, L.A. Back to the Bedside: Developing a Bedside Aid for Concussion and Brain Injury Decisions in the Emergency Department. eGEMs 2015, 3, 1136. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, A.M.; Stacey, D.; Entwistle, V.; Rovner, D.; Holmes-Rovner, M.; Tetore, J.; Llewelly-Thomas, H.; Entwistle, V.; Rostom, A.; Fiset, V.; et al. Decision Aids for People Facing Health Treatment or Screening Decisions. Cochrane Database Syst. Rev. 2001, 3, CD001431. [Google Scholar] [CrossRef] [Green Version]
- Senate House of Representatives. Patient Protection and Affordable Care Act; The 11th United States Congress: Washington, DC, USA, 2009. [Google Scholar]
- Légaré, F.; Adekpedjou, R.; Stacey, D.; Turcotte, S.; Kryworuchko, J.; Graham, I.D.; Lyddiatt, A.; Politi, M.C.; Thomson, R.; Elwyn, G.; et al. Interventions for increasing the use of shared decision making by healthcare professionals. Cochrane Database Syst. Rev. 2018, 2018, CD006732. [Google Scholar] [CrossRef]
- Schwalbe, K.; Furlong, D. Healthcare Project Management, 1st ed.; Schwalbe Publishing: Minneapolis, MN, USA, 2013. [Google Scholar]
- Matinheikki, J.; Artto, K.; Peltokorpi, A.; Rajala, R. Managing inter-organizational networks for value creation in the front-end of projects. Int. J. Proj. Manag. 2016, 34, 1226–1241. [Google Scholar] [CrossRef] [Green Version]
- Morris, P.W.G. Managing the front-end: How project managers shape business strategy and manage project definition. In Proceedings of the 2005 PMI Global Congress Proceedings, Edinburough, UK, 25 May 2005. [Google Scholar]
- Rojas-Meluk, J.F. Project initiation and measurement: Laying the foundation for better projects. In Proceedings of the 2006 PMI Global Congress Proceedings, Santiago, Chile, 6–8 November 2006. [Google Scholar]
- LeRouge, C.M.; Tulu, B.; Wood, S. Project initiation for telemedicine services. In E-Health and Telemedicine: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2016; pp. 1–24. [Google Scholar]
- Cortelyou-Ward, K.; Noblin, A.; Martin, J. Electronic Health Record Project Initiation and Early Planning in a Community Health Center. Health Care Manag. 2011, 30, 118–124. [Google Scholar] [CrossRef]
- Aarons, G.A.; Hurlburt, M.; Horwitz, S.M. Advancing a Conceptual Model of Evidence-Based Practice Implementation in Public Service Sectors. Adm. Policy Ment. Heal. Ment. Health Serv. Res. 2010, 38, 4–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damschroder, L.J.; Aron, D.C.; E Keith, R.; Kirsh, S.R.; A Alexander, J.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhalgh, T.; Robert, G.; Macfarlane, F.; Bate, P.; Kyriakidou, O. Diffusion of Innovations in Service Organizations: Systematic Review and Recommendations. Milbank Q. 2004, 82, 581–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimchi, J.; Polivka, B.; Stevenson, J.S. Triangulation: Operational Definitions. Nurs. Res. 1991, 40, 364–366. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.K.; Davis, D. Adding new dimensions to case study evaluations: The case of evaluating comprehensive reforms. New Dir. Evaluation 2007, 2007, 75–93. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeRouge, C.; Nguyen, A.M.; Bowen, D.J. Patient Decision Aid Selection for Shared Decision Making: A Multicase Qualitative Study. Med. Care Res. Rev. 2021. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis: A Methods Sourcebook, 3rd ed.; SAGE Publications: Southend Oaks, CA, USA, 2013. [Google Scholar]
- Denzin, N.K. The Research Act, 3rd ed.; McGraw Hill: New York, NY, USA, 1989. [Google Scholar]
- Lerouge, C.; Dickhut, K.; Lisetti, C.; Sangameswaran, S.; Malasanos, T. Engaging adolescents in a computer-based weight management program: Avatars and virtual coaches could help. J. Am. Med. Inform. Assoc. 2016, 23, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SocioCultural Research Consultants. Dedoose, 2019; Published Online.
- Légaré, F.; Witteman, H.O. Shared decision making: Examining key elements and barriers to adoption into routine clinical practice. Health Aff. (Millwood) 2013, 32, 276–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alston, C.; Mslgroup, Q.; Elwyn, G.; Fowler, F.; Hall, L.K.; Moulton, B.; Paget, L.; Shebel, B.H.; Berger, Z.; Brownlee, S.; et al. Shared Decision-Making Strategies for Best Care: Patient Decision Aids. NAM Perspect. 2014, 4. [Google Scholar] [CrossRef]
- Barr, P.J.; Elwyn, G. Measurement challenges in shared decision making: Putting the ‘patient’ in patient-reported measures. Health Expect. 2016, 19, 993–1001. [Google Scholar] [CrossRef]
- Légaré, F.; Ratté, S.; Gravel, K.; Graham, I.D. Barriers and facilitators to implementing shared decision-making in clinical practice: Update of a systematic review of health professionals’ perceptions. Patient Educ. Couns. 2008, 73, 526–535. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Project Site A | Project Site B | Project Site C | |
|---|---|---|---|
| Healthcare System Type | Academic, Voluntary Nonprofit | Governmental Hospital District | Voluntary Nonprofit |
| Location | Urban | Urban | Urban |
| FQHC Status | No | No | No |
| # of Obstetric Clinics in Project | 2 | 5 | 1 |
| # of Clinicians in Project | 17 (9 OBGYNs, 8 midwives) | 40 (all OBGYNs) | 3 (2 OBGYNs, 1 midwife) |
| Decision Aid Vendor | Non-Certified Vendor | Non-Certified Vendor | Certified Vendor |
| Decision Aid Modality | Paper | In-Person Class | Paper |
| EHR System | Epic© | Different system at each clinic | Epic© |
| Theme | Source | Representative Supporting Evidence (Quote or Supporting Document Comment) |
|---|---|---|
| Inner Context | ||
| Absorptive Capacity | Interview | “We were just coming out of a huge, Epic© upgrade, and IT was quite busy. Our physicians were happy to at least have something that they can start working on [the paper version of the decision aid]. We can potentially see an electronic decision aid implemented some time down the line or maybe next year once we have our resources back in place.” (Project Site C) |
| EHR documentation protocol | Early versions of some EHR documentation protocols were for an electronic version of the decision aid but were then updated to documentation of a paper-based or classroom version. | |
| Culture/Climate/Context | Interview | “[There is] a very activated obstetrical community around obstetrical quality improvement, especially with respect to active management of labor.” (State) |
| Leadership Engagement | Interview | “Part of the initial conversations with the [State] was alongside our Director for the Clinical Integrated Network. Both of them were on initial conversations. and we felt that it would be great for [Health System] to start this project.” (Project Site C) |
| Project management plans provided by project sites | Project management plans noted who was involved in the initial meetings from each project site and healthcare system. | |
| Network and Communications | Interview | “The willingness to share [information] with each other, even amongst organizations that are competing with each other, is probably stronger than average.” (Certified Vendor) |
| Implementation plans provided by the vendor | Each project site received an implementation plan (i.e., roadmap) from the vendor, and the roadmaps had similar components. | |
| Perceived Need for Change | Interview | “If [the patient] has all the information, it’s possible that they would pick the less expensive option.” (Vendor) |
| Readiness for Change | Interview | “SDM is the right thing to do for our patients and families.” (Project Site A) |
| Innovation Components | ||
| Adaptability | Interview | “The IT build is one of our major time obstacles. We don’t have an IT department that’s going to prioritize this as number one, and so we needed something fairly simple for them to be able to get it done in less than a year, really.” (Project Site A) |
| Training modules provided by project sites | Training modules indicated that the decision aid could be presented to the patient at several possible timepoints. | |
| Nature of Knowledge Required | Interview | “The VBAC [Vaginal Birth After Cesarean] booklet is part of just a bigger education campaign.” (Non-Certified Vendor) |
| Implementation plans provided by the vendor | The implementation plans laid out multiple components of the SDM program, including implementation of the TOLAC decision aid, provider SDM training, and process for recording SDM in patient records. | |
| Implementation Process | ||
| Knowledge/Beliefs about Innovation | Interview | “It used to be called informed consent. To tell you the truth, most physicians find it kind of amusing that somebody decided to rename it, which is what they do with everything every few years. In theory, it’s different, but it’s not in practice.” (Project Site B) |
| Interview | “To me, shared decision making is following a very prescriptive process that documents key milestones in the conversation that unravels with the patient and the family, being able to point them to the risks and the benefits of a chosen treatment option, being able to document that, being able to then arrive at a decision and to measure its impact and evaluation.” (Project Site A) | |
| Targeted Users | Interview | “Honestly, I think if we can get 60 to 70% [of eligible patients through the class], that would be a huge win. You just can’t make everybody can go to the class. There are people who can’t make it or are not going to. I don’t think that will ever have 100%. That’s a dream. I would be really happy if we got 60 to 70. I feel like 75% would be an absolutely stellar result.” (Project Site B) |
| Training materials | Training materials described the types of users. | |
| Team Characteristics | Interview | “The non-physician leaders [at Project Site] were pretty much on board, ready to go, but there were some physician doubts on it about whether or not this was worthwhile, how exactly it would work.” (Certified Vendor) |
| Project management plans provided by project sites | Project management plans listed the team members. | |
| Implementation Effectiveness | ||
| Cost | Interview | “My sense is that organizations are doing as much as they can to cut cost, and I think SDM is one because, it’s really hard to show the return-on-investment of a program like this. I imagine that the growth in the momentum will continue to be slow unfortunately.” (State) |
| Outer Context | ||
| Decision Aid Certification Program and Other External Factors | Interview | “I think in the end that external environmental driver that has in Washington State that this reduces your medical malpractice liability is the big opportunity for us push things in the right direction. And eventually we’re going to go there.” (Certified Vendor) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowen, D.J.; Nguyen, A.M.; LeRouge, C.; LePoire, E.; Sheng Kwan-Gett, T. Factors Affecting the Initiation of a Shared Decision Making Program in Obstetric Practices. Healthcare 2021, 9, 1217. https://doi.org/10.3390/healthcare9091217
Bowen DJ, Nguyen AM, LeRouge C, LePoire E, Sheng Kwan-Gett T. Factors Affecting the Initiation of a Shared Decision Making Program in Obstetric Practices. Healthcare. 2021; 9(9):1217. https://doi.org/10.3390/healthcare9091217
Chicago/Turabian StyleBowen, Deborah J., Ann M. Nguyen, Cynthia LeRouge, Erin LePoire, and Tao Sheng Kwan-Gett. 2021. "Factors Affecting the Initiation of a Shared Decision Making Program in Obstetric Practices" Healthcare 9, no. 9: 1217. https://doi.org/10.3390/healthcare9091217