
Psychometric Properties of the Taiwanese Version of the Tilburg Frailty Indicator for Community-Dwelling Older Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. TFI
2.3. Translation and Cultural Adaptation of the TFI for Taiwan
2.4. Other Instruments
2.5. Analysis
2.6. Ethical Considerations
3. Results
3.1. Participant Characteristics
3.2. Reliability and Validity
3.2.1. Internal Consistency Reliability
3.2.2. Test–Retest Reliability
3.2.3. Content Validity
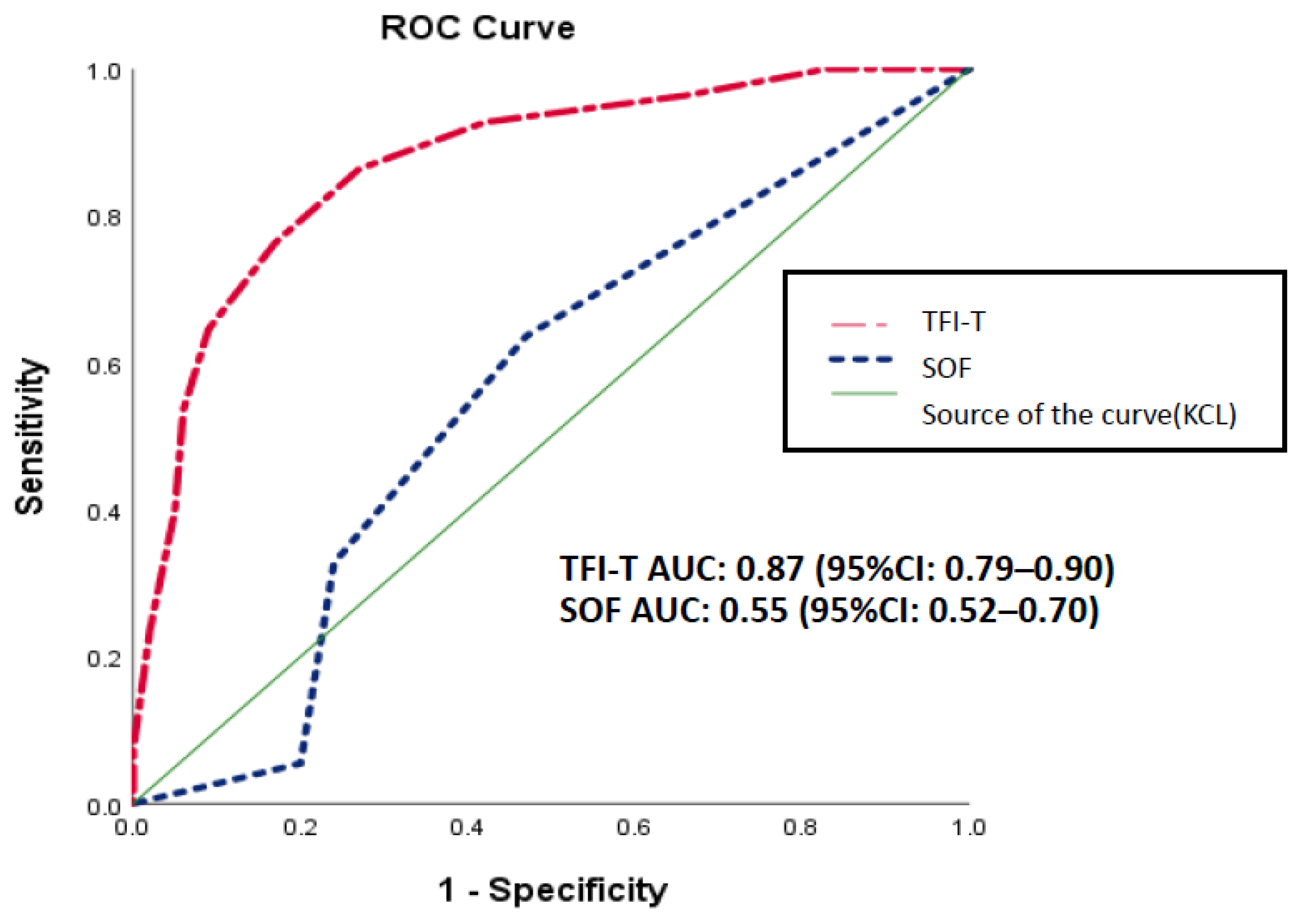
3.2.4. Criterion-Related Validity
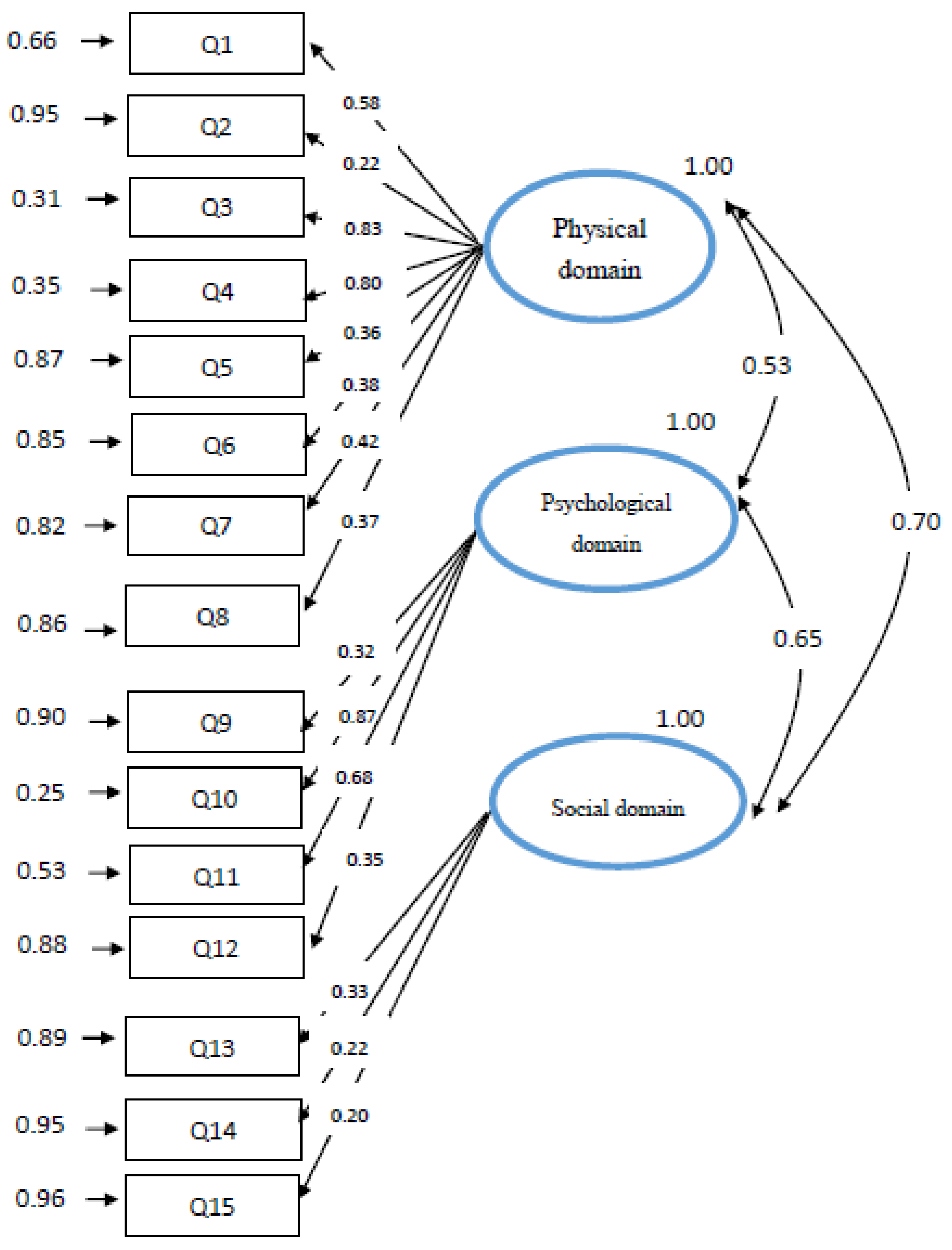
3.2.5. Construct Validity
4. Discussion
4.1. General Discussion
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Lee, W.J.; Lin, H.P.; Chen, R.C.; Lin, C.H.; Peng, L.N.; Chen, L.K. Epidemiology of frailty and associated factors among older adults living in rural communities in Taiwan. Arch. Gerontol. Geriatr. 2020, 87, 10398. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Chin, K.L.; Mazidi, M.; Zomer, E.; Ilomaki, J.; Zullo, A.R.; Gasevic, D.; Ademi, Z.; Korhonen, M.J.; LoGiudice, D.; et al. Global incidence of frailty and prefrailty among community-dwelling older adults: A systematic review and meta-analysis. JAMA Netw. Open 2019, 2, e198398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty in relation to the accumulation of deficits. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef] [Green Version]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.X.; Ding, G.; Yu, W.J.; Liu, T.F.; Yan, A.Y.; Chen, H.Y.; Zhang, A.H. Association between frailty and incident risk of disability in community-dwelling elder people: Evidence from a meta-analysis. Public Health 2019, 175, 90–100. [Google Scholar] [CrossRef]
- Persico, I.; Cesari, M.; Morandi, A.; Haas, J.; Mazzola, P.; Zambon, A.; Annoni, G.; Bellelli, G. Frailty and delirium in older adults: A systematic review and meta-analysis of the literature. J. Am. Geriatr. Soc. 2018, 66, 2022–2030. [Google Scholar] [CrossRef]
- Kojima, G. Increased healthcare costs associated with frailty among community-dwelling older people: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2019, 84, 103898. [Google Scholar] [CrossRef]
- Gobbens, R.J.; Boersma, P.; Uchmanowicz, I.; Santiago, L.M. The Tilburg Frailty Indicator (TFI): New evidence for its validity. Clin. Interv. Aging. 2020, 15, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: A review. Eur. J. Intern. Med. 2016, 31, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.W.; Kim, S.W.; Ahn, S.; Lim, J.Y.; Han, J.W.; Kim, T.H.; Kim, K.W.; Kim, K.I.; Kim, C.H. Prevalence and outcomes of frailty in Korean elderly population: Comparisons of a multidimensional frailty index with two phenotype models. PLoS ONE 2014, 9, e87958. [Google Scholar] [CrossRef]
- Hirai, K.; Tanaka, A.; Homma, T.; Kaneko, K.; Uno, T.; Sato, H.; Manabe, R.; Ohta, S.; Kusumoto, S.; Yamaguchi, F.; et al. Comparison of three frailty models and a sarcopenia model in elderly patients with chronic obstructive pulmonary disease. Geriatr. Gerontol. Int. 2019, 19, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Sewo Sampaio, P.Y.; Sampaio, R.A.; Yamada, M.; Arai, H. Systematic review of the Kihon Checklist: Is it a reliable assessment of frailty? Geriatr. Gerontol. Int. 2016, 16, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; Uchmanowicz, I. Assessing frailty with the Tilburg Frailty Indicator (TFI): A review of reliability and validity. Clin. Interv. Aging. 2021, 16, 863–875. [Google Scholar] [CrossRef]
- Gobbens, R.J.; van Assen, M.A.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. The Tilburg Frailty Indicator: Psychometric properties. J. Am. Med. Dir. Assoc. 2010, 11, 344–355. [Google Scholar] [CrossRef]
- Sutton, J.L.; Gould, R.L.; Daley, S.; Coulson, M.C.; Ward, E.V.; Butler, A.M.; Nunn, S.P.; Howard, R.J. Psychometric properties of multicomponent tools designed to assess frailty in older adults: A systematic review. BMC Geriatr. 2016, 16, 55. [Google Scholar] [CrossRef] [Green Version]
- Dong, L.; Liu, N.; Tian, X.; Qiao, X.; Gobbens, R.J.J.; Kane, R.L.; Wang, C. Reliability and validity of the Tilburg Frailty Indicator (TFI) among Chinese community-dwelling older people. Arch. Gerontol. Geriatr. 2017, 73, 21–28. [Google Scholar] [CrossRef]
- Freitag, S.; Schmidt, S.; Gobbens, R.J. Tilburg frailty indicator. German translation and psychometric testing. Z. Gerontol. Geriatr. 2016, 49, 86–93. [Google Scholar] [CrossRef]
- Mulasso, A.; Roppolo, M.; Gobbens, R.J.; Rabaglietti, E. The Italian version of the Tilburg Frailty Indicator: Analysis of psychometric properties. Res. Aging 2016, 38, 842–863. [Google Scholar] [CrossRef] [PubMed]
- Santiago, L.M.; Luz, L.L.; Mattos, I.E.; Gobbens, R.J.; van Assen, M.A. Psychometric properties of the Brazilian version of the Tilburg frailty indicator (TFI). Arch. Gerontol. Geriatr. 2013, 57, 39–45. [Google Scholar] [CrossRef]
- Uchmanowicz, I.; Jankowska-Polańska, B.; Uchmanowicz, B.; Kowalczuk, K.; Gobbens, R.J. Validity and reliability of the Polish version of the Tilburg Frailty Indicator (TFI). J. Frailty. Aging 2016, 5, 27–32. [Google Scholar] [CrossRef]
- Coelho, T.; Santos, R.; Paúl, C.; Gobbens, R.J.; Fernandes, L. Portuguese version of the Tilburg Frailty Indicator: Transcultural adaptation and psychometric validation. Geriatr. Gerontol. Int. 2015, 15, 951–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, P.; Chen, J.L.; Liu, N. Sample size estimation of quantitative research in nursing research. Chin. J. Nurs. 2010, 45, 378–380. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toba, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp.: Armonk, NY, USA, 2018. [Google Scholar]
- Jöreskog, K.G.; Sörbom, D. LISREL 8.80; Scientific Software International Inc.: Lincolnwood, IL, USA, 2006. [Google Scholar]
- Souza, A.C.; Alexandre, N.M.C.; Guirardello, E.B. Psychometric properties in instruments evaluation of reliability and validity. Epidemiol. Serv. Saude. 2017, 26, 649–659. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, S.E.; Cole, D.A. Bias in cross-sectional analyses of longitudinal mediation. Psychol. Methods 2007, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- Köksal, M.S.; Ertekin, P.; Çolakoglu, Ö.M. How differences among data collectors are reflected in the reliability and validity of data collected by Likert-type scales? Educ. Sci. Theory Pract. 2014, 14, 2206–2212. [Google Scholar]



{kind=link}
{kind=link}
| Variable | n(%) |
| Age (years) | |
| 60–69 | 61 (29.0%) |
| 70–79 | 68 (32.4%) |
| 80–94 | 81 (38.6%) |
| Gender (female) | 159 (75.7%) |
| Marital status | |
| Married or remarried 100 | (48%) |
| Widowed | 97 (46%) |
| Divorced and unmarried | |
| ≤6 | 53 (25%) |
| 7–9 | 54 (26%) |
| ≥10 | 103 (49%) |
| Monthly income | (Taiwan Dollars) |
| No income 29 | (14%) |
| <10,000 | 100 (47%) |
| 10,001–50,000 | 81 (39%) |
| Variable | Mean ± SD |
| SOF total index (0–3) | 0.97 ± 1.05 |
| KCL total score (0–25) | 7.27 ± 4.49 |
| KCL sub-domain: | |
| ADL | 1.10 ± 1.49 |
| physical strength | 1.87 ± 1.48 |
| Nutrition | 0.25 ± 0.48 |
| oral function | 1.24 ± 0.92 |
| Isolation | 0.34 ± 0.55 |
| Memory | 1.23 ± 0.88 |
| Mood | 1.25 ± 1.36 |
| TFI-T total score (0–15) | 5.69 ± 3.22 |
| TFI-T sub-domain: | |
| Physical domain score (0–8) | 3.19 ± 2.18 |
| Psychological domain score (0–4) | 1.18 ± 1.19 |
| Social domain score (0–3) | 1.32 ± 0.64 |
| Variable | 1 | 2 | 3 |
|---|---|---|---|
| 1. SOF | 1 | - | - |
| 2. KCL | 0.13 | 1 | - |
| 3. TFI-T | 0.11 | 0.74 *** | 1 |
| Criterion | Cutoff | Sensitivity (True Positive Rate) (%) | Specificity (True Negative Rate) (%) | DI | Youden’s Index |
|---|---|---|---|---|---|
| KCL | TFI-T ≥ 4.5 | 86.4 | 73 | 1.59 | 0.59 |
| TFI-T ≥ 5.5 | 76.4 | 83 | 1.59 | 0.59 | |
| TFI-T ≥ 6.5 | 65.0 | 91 | 1.56 | 0.56 | |
| TFI-T ≥ 7.5 | 53.6 | 94 | 1.47 | 0.49 |
| Three-Factor Model | X2/df | GFI | CFI | AGFI | RMR | NFI | RMSEA | NFI |
|---|---|---|---|---|---|---|---|---|
| Scale | 174.3/87 | 0.98 | 0.91 | 0.83 | 0.04 | 0.84 | 0.0054 | 0.89 |
| Domains of TFI-T | Domains of KCL | r | p-Value |
|---|---|---|---|
| Physical domain (Q1–Q8) | ADL (Q1–Q5) | 0.43 | <0.01 |
| physical strength (Q6–Q10) | 0.61 | <0.01 | |
| Nutrition (Q11–Q12) | 0.14 | <0.05 | |
| oral function (Q13–Q15) | 0.37 | <0.01 | |
| Psychological domain (Q9–Q11) | Memory (Q18–Q20) | 0.39 | <0.01 |
| Mood (Q21–Q25) | 0.45 | <0.01 | |
| Social domain (Q12–Q15) | Isolation (Q16–Q17) | 0.30 | <0.01 |
| Variable | TFI-T | t | p-Value | |
|---|---|---|---|---|
| <5.5 robust group (n = 109) (mean ± SD) | ≥5.5 frail group (n = 101) (mean ± SD) | |||
| SOF scale | 0.85 ± 1.15 | 1.09 ± 0.91 | −1.63 | 0.10 |
| KCL score | 4.59 ± 2.86 | 10.17 ± 4.12 | −11.29 | <0.001 |
| TFI-T Physical domain | 1.49 ± 1.05 | 5.02 ± 1.49 | −19.60 | <0.001 |
| Psychological domain | 0.44 ± 1.97 | 1.97 ± 1.12 | −11.77 | <0.001 |
| Social domain | 1.14 ± 0.56 | 1.52 ± 0.65 | −4.54 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-H.; Liu, C.-Y.; Rong, J.-R. Psychometric Properties of the Taiwanese Version of the Tilburg Frailty Indicator for Community-Dwelling Older Adults. Healthcare 2021, 9, 1193. https://doi.org/10.3390/healthcare9091193
Lin C-H, Liu C-Y, Rong J-R. Psychometric Properties of the Taiwanese Version of the Tilburg Frailty Indicator for Community-Dwelling Older Adults. Healthcare. 2021; 9(9):1193. https://doi.org/10.3390/healthcare9091193
Chicago/Turabian StyleLin, Chia-Hui, Chieh-Yu Liu, and Jiin-Ru Rong. 2021. "Psychometric Properties of the Taiwanese Version of the Tilburg Frailty Indicator for Community-Dwelling Older Adults" Healthcare 9, no. 9: 1193. https://doi.org/10.3390/healthcare9091193