
SARS-CoV-2 in Pediatric Inpatient Care: Management, Clinical Presentation and Utilization of Healthcare Capacity

 and
and
Abstract
:1. Introduction
2. Materials and Methods
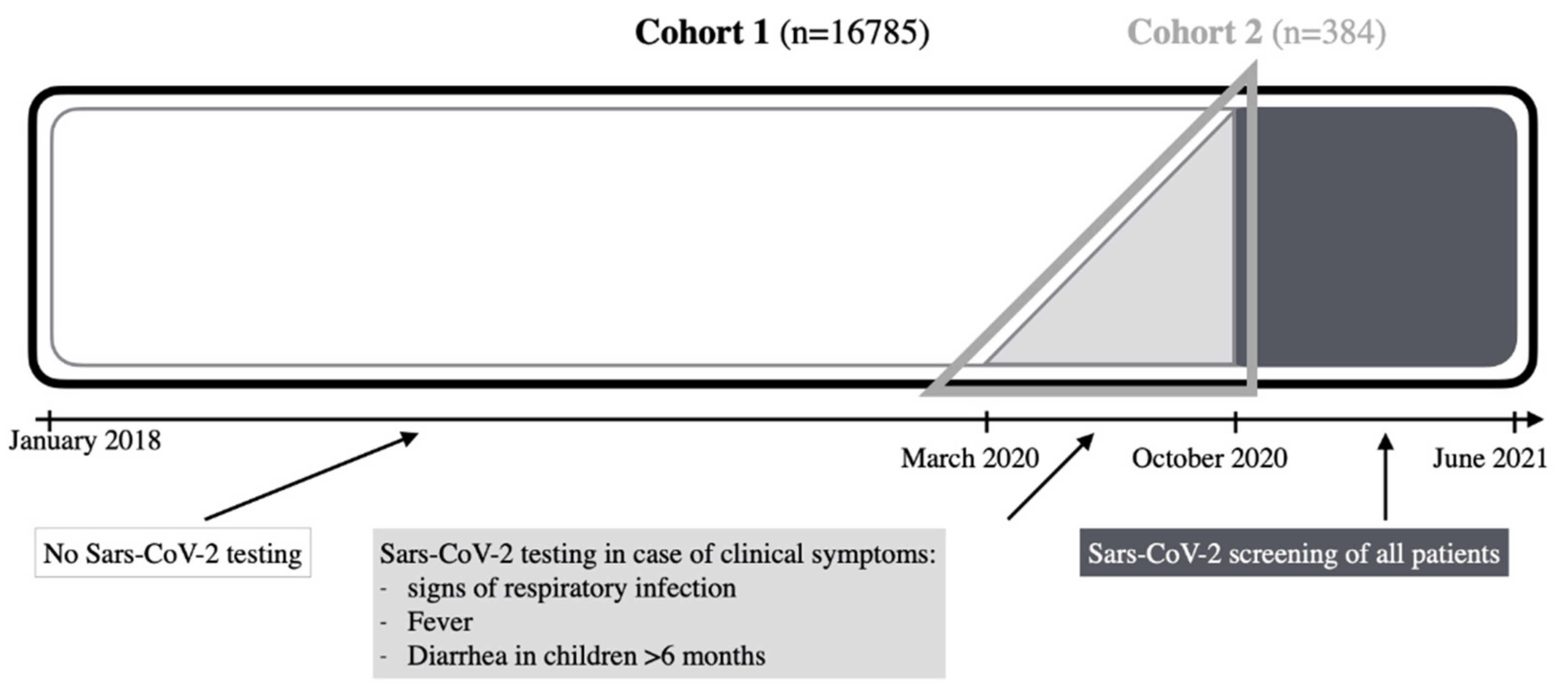
2.1. Study Design and Patient Cohort
2.2. Statistical Analysis
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- WHO. Available online: https://www.who.int (accessed on 2 July 2020).
- Peiris, J.S.; Lai, S.T.; Poon, L.L.; Guan, Y.; Yam, L.Y.; Lim, W.; Nicholls, J.; Yee, W.K.; Yan, W.W.; Cheung, M.T.; et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet 2003, 361, 1319–1325. [Google Scholar] [CrossRef] [Green Version]
- Wool, G.D.; Miller, J.L. The Impact of COVID-19 Disease on Platelets and Coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Niazkar, H.R.; Zibaee, B.; Nasimi, A.; Bahri, N. The neurological manifestations of COVID-19: A review article. Neurol. Sci. 2020, 41, 1667–1671. [Google Scholar] [CrossRef] [PubMed]
- Streng, A.; Hartmann, K.; Armann, J.; Berner, R.; Liese, J.G. COVID-19 in hospitalized children and adolescents. Monatsschr Kinderheilkd 2020, 1–12. [Google Scholar] [CrossRef]
- Team, C.C.-R. Coronavirus Disease 2019 in Children—United States, 12 February–2 April 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 422–426. [Google Scholar]
- Brinkmann, F.; Schlegtendal, A.; Hoffmann, A.; Theile, K.; Hippert, F.; Strodka, R.; Timmesfeld, N.; Diebner, H.H.; Lucke, T.; Maier, C. SARS-CoV-2 Infections Among Children and Adolescents with Acute Infections in the Ruhr Region. Dtsch. Arztebl. Int. 2021, 118, 363–364. [Google Scholar]
- Donath, H.; Zielen, S.; Wittekindt, B.; Klingebiel, T.; Graf, J.; Eckrich, M.; Walter, C.; Blumchen, K. Effects of the SARS-CoV2-Lockdown on Pediatric Care in the Rhine-Main Area. Klin. Padiatr. 2021, 233, 31–36. [Google Scholar]
- SurvStat@RKI, Abfrage der Meldedaten nach dem Infektionsschutzgesetz (IfSG). Available online: https://survstat.rki.de/ (accessed on 1 July 2020).
- Castagnoli, R.; Votto, M.; Licari, A.; Brambilla, I.; Bruno, R.; Perlini, S.; Rovida, F.; Baldanti, F.; Marseglia, G.L. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents: A Systematic Review. JAMA Pediatr. 2020, 174, 882–889. [Google Scholar] [CrossRef] [Green Version]
- Patel, N.A. Pediatric COVID-19: Systematic review of the literature. Am. J. Otolaryngol. 2020, 41, 102573. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pediatric Hospital Admissions | SARS-CoV-2 Tests (Total) | SARS-CoV-2 Positive (Total; %) | Among These: Typical Clinical Signs Present as Previously Defined (Total; %) | Approximate Test Positive Rate in Germany (all Age Groups) | ||||
|---|---|---|---|---|---|---|---|---|
| January | 2020 | 466 | ||||||
| February | 2020 | 418 | 0 | |||||
| March | 2020 | 345 | 2 | 2 | 100.0% | 2 | 100.0% | 7.7% |
| April | 2020 | 271 | 4 | 3 | 75.0% | 1 | 33.3% | 6.6% |
| May | 2020 | 314 | 25 | 0 | 0.0% | 2.1% | ||
| June | 2020 | 377 | 100 | 1 | 1.0% | 1 | 100.0% | 0.9% |
| July | 2020 | 388 | 118 | 0 | 0.0% | 0.7% | ||
| August | 2020 | 404 | 87 | 0 | 0.0% | 0.9% | ||
| September | 2020 | 414 | 112 | 2 | 1.8% | 2 | 100.0% | 1.2% |
| October | 2020 | 361 | 190 | 9 | 4.7% | 5 | 55.6% | 4.4% |
| November | 2020 | 339 | 263 | 5 | 1.9% | 3 | 60.0% | 8.4% |
| December | 2020 | 310 | 246 | 5 | 2.0% | 4 | 80.0% | 11.8% |
| January | 2021 | 303 | 242 | 1 | 0.4% | 1 | 100.0% | 9.9% |
| February | 2021 | 326 | 270 | 1 | 0.4% | 0 | 0.0% | 6.3% |
| March | 2021 | 374 | 295 | 2 | 0.7% | 2 | 100,0% | 9.3% |
| April | 2021 | 328 | 259 | 3 | 1.2% | 2 | 66.7% | 11.7% |
| May | 2021 | 370 | 299 | 2 | 0.7% | 2 | 100.0% | 6.6% |
| SARS-CoV-2 Negative (n = 378) | SARS-CoV-2 Positive (n = 6) | Σ | SARS-CoV-2 Positive | |
|---|---|---|---|---|
| male | 219 | 4 | 223 | 1.8% |
| female | 159 | 2 | 161 | 1.2% |
| age 0–6 months | 96 | 2 | 98 | 2.0% |
| age 7–24 months | 127 | 2 | 129 | 1.6% |
| age 2–12 years | 119 | 1 | 120 | 0.8% |
| age >12 years | 36 | 1 | 37 | 2.7% |
| comorbidities present | 121 | 1 | 122 | 0.8% |
| neurological | 15 | 15 | ||
| psychiatric (e.g., ADHS, depression) | 1 | 1 | ||
| pulmonary (e.g., Asthma bronchiale, BPD, previous obstructive bronchitis or pneumonia) | 53 | 53 | ||
| congenital heart defect | 7 | 7 | ||
| urogenital | 7 | 7 | ||
| syndromal (e.g., trisomy 21) | 9 | 9 | ||
| preterm birth | ||||
| - <30 weeks of gestation | 7 | 7 | ||
| - >30 weeks of gestation | 15 | 1 | 16 | 6.3% |
| weight percentile | ||||
| <3 | 10 | 1 | 11 | 9.1% |
| 3–9 | 25 | 25 | ||
| 10–24 | 56 | 56 | ||
| 25–74 | 184 | 2 | 186 | 1.1% |
| 75–89 | 59 | 1 | 60 | 1.7% |
| 90–96 | 20 | 20 | ||
| >97 | 20 | 1 | 21 | 4.8% |
| no information | 4 | 1 | 5 | 20.0% |
| height percentile | ||||
| <3 | 15 | 1 | 16 | 6.3% |
| 3–9 | 23 | 23 | ||
| 10–24 | 44 | 44 | ||
| 25–74 | 169 | 2 | 171 | 1.2% |
| 75–89 | 54 | 1 | 55 | 1.8% |
| 90–96 | 38 | 1 | 39 | 2.6% |
| >97 | 20 | 20 | ||
| no information | 15 | 1 | 16 | 6.3% |
| SARS-CoV-2 Negative (n = 378) | SARS-CoV-2 Positive (n = 6) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0–6 Months | 7–24 Months | 2–12 Years | >12 Years | 0–6 Months | 7–24 Months | 2–12 Years | >12 Years | Σ | SARS-CoV-2 Positive | |
| fever | 57 | 101 | 67 | 16 | 2 | 1 | 1 | 245 | 1.63% | |
| cough | 30 | 39 | 70 | 5 | 1 | 1 | 1 | 1 | 148 | 2.7% |
| dyspnea or tachypnea | 26 | 46 | 61 | 11 | 1 | 145 | 0.7% | |||
| - respiratory symptoms >2 weeks | 2 | 1 | 1 | 1 | 1 | 6 | 33.3% | |||
| rhinitis | 29 | 46 | 43 | 2 | 1 | 121 | 0.8% | |||
| sore throat | 1 | 7 | 17 | 4 | 29 | |||||
| headache | 5 | 10 | 15 | |||||||
| diarrhea | 20 | 20 | 12 | 5 | 57 | |||||
| vomiting | 6 | 14 | 26 | 5 | 51 | |||||
| epileptic seizure | 4 | 20 | 9 | 2 | 1 | 36 | 2.8% | |||
| abdominal pain | 2 | 4 | 15 | 8 | 29 | |||||
| ear pain | 2 | 2 | 1 | 1 | 6 | |||||
| neurological problems | 2 | 1 | 4 | 1 | 8 | |||||
| 0–6 Months | 7–24 Months | 2–12 Years | >12 Years | |||||
|---|---|---|---|---|---|---|---|---|
| upper airway infection | 28 | 32.6% | 30 | 21.4% | 8 | 7.2% | 5 | 31.3% |
| obstructive bronchitis | 10 | 11.6% | 33 | 23.6% | 50 | 45.0% | 1 | 6.3% |
| pseudocroup | 2 | 2.3% | 4 | 2.9% | 2 | 1.8% | ||
| pneumonia | 2 | 2.3% | 13 | 9.3% | 18 | 16.2% | 3 | 18.8% |
| - radiological diagnosis | 1 | 4 | 9 | 1 | 5.3% | |||
| - clinical diagnosis | 1 | 9 | 9 | 2 | 10.5% | |||
| gastroenteritis | 11 | 12.8% | 12 | 8.6% | 15 | 13.5% | 6 | 37.5% |
| sepsis | 4 | 4.7% | 2 | 1.4% | ||||
| newborn infection | 10 | 11.6% | ||||||
| febrile seizure | 2 | 2.3% | 25 | 17.9% | 8 | 7.2% | ||
| urinary tract infection | 12 | 14.0% | 10 | 7.1% | 7 | 6.3% | 1 | 6.3% |
| tonsillitis | 7 | 5.0% | 2 | 1.8% | ||||
| otitis media | 3 | 3,5% | 3 | 2.1% | ||||
| meningitis | 2 | 2,3% | 1 | 0.7% | 1 | 0.9% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busch, C.; Blickle, M.; Schmidt, B.; Sievers, L.K.; Pfitzer, C. SARS-CoV-2 in Pediatric Inpatient Care: Management, Clinical Presentation and Utilization of Healthcare Capacity. Healthcare 2021, 9, 1190. https://doi.org/10.3390/healthcare9091190
Busch C, Blickle M, Schmidt B, Sievers LK, Pfitzer C. SARS-CoV-2 in Pediatric Inpatient Care: Management, Clinical Presentation and Utilization of Healthcare Capacity. Healthcare. 2021; 9(9):1190. https://doi.org/10.3390/healthcare9091190
Chicago/Turabian StyleBusch, Christine, Maximilian Blickle, Beatrix Schmidt, Laura Katharina Sievers, and Constanze Pfitzer. 2021. "SARS-CoV-2 in Pediatric Inpatient Care: Management, Clinical Presentation and Utilization of Healthcare Capacity" Healthcare 9, no. 9: 1190. https://doi.org/10.3390/healthcare9091190