
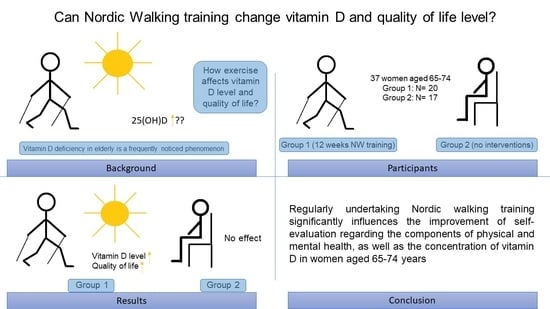
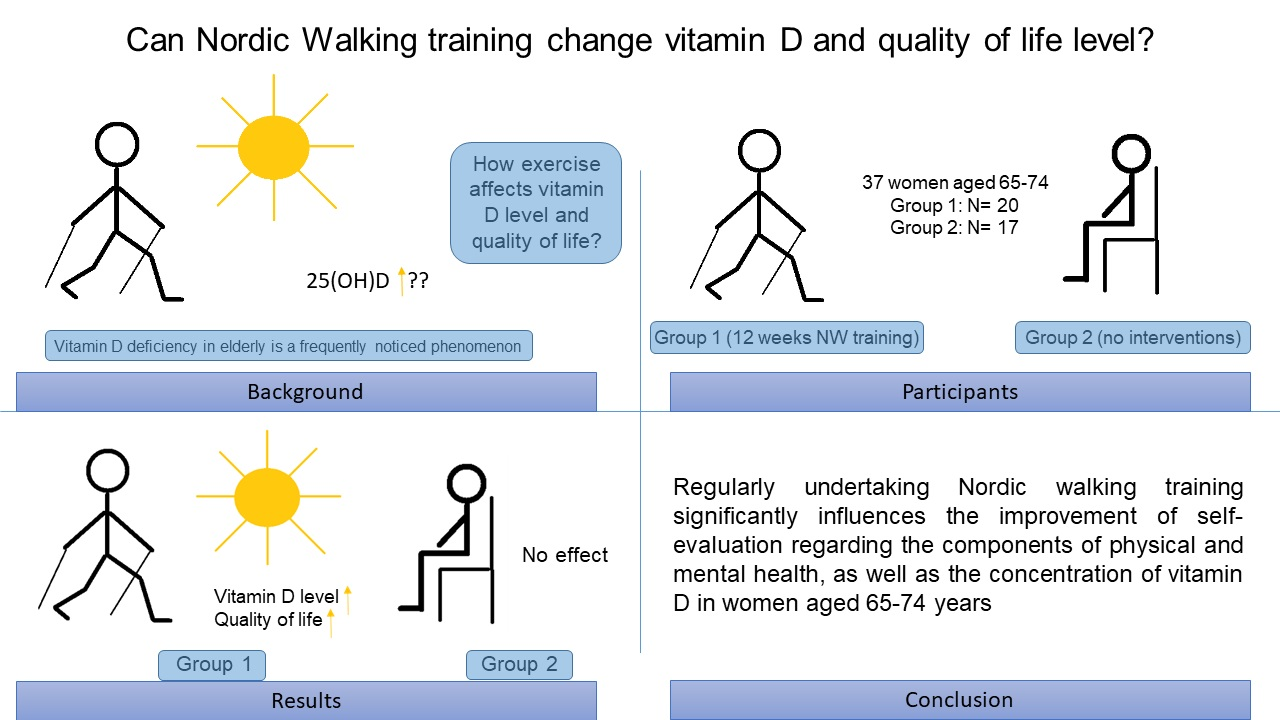
Influence of Nordic Walking Training on Vitamin D Level in the Blood and Quality of Life among Women Aged 65–74

 , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Characteristics of the Study Group
2.3. Research Methods
2.4. Determination of Vitamin D Levels
2.5. Evaluating Quality of Life
2.6. Description of Intervention
2.7. Statistical Analysis
3. Results
3.1. Vitamin D Levels
3.2. Quality of Life Assessment
4. Discussion
5. Conclusions
- The 12-week Nordic walking training programme had a positive effect on the self-reported level of physical and mental health among older women.
- The 12-week Nordic walking intervention increased vitamin D levels in older women.
- Regular physical activity and the prevention of vitamin D deficiency can be key factors in maintaining independence among seniors.
- Nordic walking exercise should be routinely undertaken by older adults.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tosato, M.; Zamboni, V.; Ferrini, A.; Cesari, M. The aging proces and potential interventions to extend life expectancy. Clin. Interv. Aging 2007, 2, 401–412. [Google Scholar] [PubMed]
- Blagosklonny, M.V. Why human lifespan is rapidly increasing: Solving “longevity riddle” with “revealed-slow-aging” hypothesis. Aging 2010, 2, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, Z.; Bowling, A. Quality of life from the perspectives of older people. Ageing Soc. 2004, 24, 675–691. [Google Scholar] [CrossRef] [Green Version]
- Cybulski, M.; Krajewska-Kulak, E.; Jamiolkowski, J. Preferred health behaviors and quality of life of the elderly people in Poland. Clin. Interv. Aging 2015, 10, 1555–1564. [Google Scholar] [CrossRef] [Green Version]
- Informacji Ministra Zdrowia na Temat Wpływu Zmian Demograficznych i Starzenia się Społeczeństwa na Organizację Systemu Ochrony Zdrowia i Narodowy Program Zdrowia. Available online: http://www.stat.gov.pl (accessed on 2 September 2021).
- Rottermund, J.; Knapik, A.; Szyszka, M. Aktywność fizyczna a jakość życia osób starszych. Społeczeństwo i Rodz. 2015, 42, 78–98. [Google Scholar]
- Weening-Dijksterhuis, E.; de Greed, M.H.; Krijnen, W.; van der Schans, C. Self-reported physical fitness in frail older persons: Reliability and validity of the self-assessment of physical fitness (SAPF). Percept. Mot. Skills 2012, 115, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Yuta, N.; Ryota, S.; Susumu, O.; Kazushi, M.; Yoshinori, F. Effects of an unsupervised Nordic walking intervention on cognitive and physical function among older women engaging in volunteer activity. J. Exerc. Sci. Fit. 2021, 19, 209–215. [Google Scholar]
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayama, M.; Furuya, T.; Inoue, E.; Tanaka, E.; Ikari, K.; Yamanaka, H.; Harigai, M. Vitamin D deficiency is a risk factor for new fractures in Japanese postmenopausal women with rheumatoid arthritis: Results from the IORRA cohort study. Arch. Osteoporos. 2021, 3, 119. [Google Scholar] [CrossRef]
- Halicki, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatmentand prevention. Rev. Endocr Metab Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Lips, P. The prevalence of vitamin D inadequacy amongst women with osteoporosis: An international epidemiological investigation. J. Inter. Med. 2006, 260, 245–254. [Google Scholar] [CrossRef]
- Minda, M.; Kukuła, D. Proces starzenia się a aktywność fizyczna osób starszych. Probl. Med. Nauk. Zdrowiu 2017, 2, 43–51. [Google Scholar]
- Touvier, M.; Deschasaux, M.; Montourcy, M.; Sutton, A.; Charnaux, N.; Kesse-Guyot, E.; Assmann, K.E.; Fezeu, L.; Latino-Martel, P.; Druesne-Pecollo, N.; et al. Determinants of vitamin D status in Caucasian adults: Influence of sun exposure, dietary intake, sociodemographic, lifestyle, anthropometric, and genetic factors. J. Invest. Dermatol. 2015, 135, 378–388. [Google Scholar] [CrossRef] [Green Version]
- Nagyova, I.; Jendrichovsky, M.; Kucinsky, R.; Lachytova, M.; Rus, V. Effects of Nordic walking on cardiovascular performance and quality of life in coronary artery disease. Eur. J. Phys. Rehabil. Med. 2020, 56, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Krysiuk, O.B.; Deineko, V.V.; Kantemirova, R.K.; Sukhonos, Y.A.; Arutiunov, V.A. Nordic walking in an integrated approach to improving the quality of live of the elderly. Adv. Gerontol. 2020, 33, 590–594. [Google Scholar]
- Enko, D.; Kriegshauser, G.; Stolba, R.; Worf, E.; Halwachs-Baumann, G. Method evaluation study of a new generation of vitamin D assays. Biochem. Med. 2015, 25, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Tylka, J.; Piotrowicz, R. Kwestionariusz oceny jakości życia SF- 36- wersja polska. Kardiol. Pol. 2009, 67, 1166–1169. [Google Scholar] [PubMed]
- Cieślik, B.; Podbielska, H. Przegląd wybranych kwestionariuszy oceny jakości życia. Acta Bio-Opt. Infom. Med. 2015, 21, 102–135. [Google Scholar]
- Kozdroń, E. Aktywność rekreacyjna w procesie pomyślnego starzenia się. Zeszyty Naukowe WSKFiT 2014, 9, 78–80. [Google Scholar]
- Mansour, K.B.; Gorce, P.; Rezzoug, N. The impact of Nordic walking training on the gait of the elderly. J. Sports Sci. 2018, 36, 2368–2374. [Google Scholar] [CrossRef]
- Gomeñuka, N.A.; Oliveira, H.B.; Silva, E.S.; Costa, R.R.; Kanitz, A.C.; Liedtke, G.V.; Schuch, F.B.; Peyré-Tartaruga, L.A. Effects of Nordic walking training on quality of live, balance and functional mobility in elderly: A randomized clinical trial. PLoS ONE 2019, 14, e0211472. [Google Scholar] [CrossRef]
- Sun, Q.; Townsend, M.K.; Okereke, O.I.; Franco, O.H.; Hu, F.B.; Grodstein, F. Physical activity at midlife in relations to sucsessful survival in women at age 70 years or older. Arch. Inter. Med. 2010, 170, 194–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabia, S.; Singh-Manoux, A.; Hagger-Johnson, G.; Cambois, E.; Brunner, E.J.; Kivimaki, M. Influence of individual and combined healthy behaviours on successful aging. Can. Med. Assoc. J. 2012, 184, 1985–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bashkireva, A.S.; Bogdanova, D.Y.; Bilyk, A.Y.; Shishko, A.V.; Kachan, E.Y.; Arutyunov, V.A. Quality of life and physical activity among elderly and old people. Adv. Gerontol. 2018, 31, 743–750. [Google Scholar] [CrossRef]
- Hagner- Derengowska, M.; Kałużna, A.; Czamara, A.; Kałużny, K.; Budzyński, J. Wpływ treningu Nordic Walking na parametry chodu i sprawność fizyczną u kobiet w wieku pomenopauzalnym. Polish J. Sport Med. 2015, 4, 179–186. [Google Scholar]
- Figueiredo, S.; Finch, L.; Mai, J.; Ahmed, S.; Huang, A.; Mayo, N.E. Nordic walking for geriatric rehabilitation: A randomized pilot trial. Disabil. Rehabil. 2013, 35, 968–975. [Google Scholar] [CrossRef]
- Park, S.K.; Yang, D.J.; Kang, Y.H.; Kim, J.H.; Uhm, Y.H.; Lee, Y.S. Effects of Nordic walking and walking on spatiotemporal gait parameters and ground reaction force. J. Phy. Ther. Sci. 2015, 27, 2891–2893. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Soriano, P.; Encarnación-Martínez, A.; Aparicio-Aparicio, I.; Giménez, J.V.; Llana-Belloch, S. Nordic walking: A systematic review. Eur. J. Hum. Mov. 2014, 33, 26–45. [Google Scholar]
- Sharma, P.; Agarwal, M.; Tiwari, S. Nordic Walking: A novel exercise regimen for cardio-metabolic health. A brief review. J. Physiol. 2017, 16, 25–30. [Google Scholar]
- Pellegrini, B.; Boccia, G.; Zoppirolli, C.; Rosa, R.; Stella, F.; Bortolan, L.; Rainoldi, A.; Schena, F. Muscular and metabolic responses to different Nordic walking techniques, when style matters. PLoS ONE 2018, 13, e0195438. [Google Scholar] [CrossRef] [Green Version]
- Pellegrini, B.; Peyré-Tartaruga, L.A.; Zoppirolli, C.; Bortolan, L.; Bacchi, E.; Figard-Fabre, H.; Schena, F. Exploring Muscle Activation during Nordic Walking: A Comparison between Conventional and Uphill Walking. PLoS ONE 2015, 10, e0138906. [Google Scholar] [CrossRef] [Green Version]
- Tschentscher, M.; Niederseer, D. Niebauer. J, Health Benefits of Nordic Walking A Systematic Review. Am. J. Prev Med. 2013, 44, 76–84. [Google Scholar] [CrossRef]
- Gougeon, M.A.; Zhou, L.; Nantel, J. Nordic walking improves trunk stability and gait spatial-temporal characteristics in people with Parkinson disease. NeuroRehabilitation 2017, 41, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Knapik, A.; Saulicz, E.; Plinta, R.; Kuszewski, M. Aktywność fizyczna a zdrowie kobiet w starszym wieku. J. Clin. Orthop. Trauma. 2011, 6, 27–33. [Google Scholar]
- Saulicz, M.; Saulicz, E.; Myśliwiec, A.; Wolny, T.; Linek, P.; Knapik, A.; Rottermund, J. Effect of a 4-week Nordic walking training on the physical fitness and self-assessment of the quality of health of women on the perimenopausal age. Menopause Rev. 2015, 14, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Lipowski, M.; Walczak-Kozłowska, T.; Lipowska, M.; Kortas, J.; Antosiewicz, J.; Falcioni, G.; Ziemann, E. Improvement of attention executive finctions and processing speed in elderly women as a result of involvement in the nordic walking training program and vitamin D supplementation. Nutrients 2019, 11, 1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilch, W.; Tyka, A.; Cebula, A.; Śliwicka, E.; Pilaczyńska-Szcześniak, Ł. Effects of a 6-week Nordic walking training on changes in 25(OH)D blood concentration in women aged over 55. J. Sports Med. Phys. Fitness. 2017, 57, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Wanner, M.; Richard, A.; Martin, B.; Linseisen, J.; Rohrmann, S. Associations between objective and self-reported physical activity and vitamin D serum levels in the US population. Cancer Causes Control. 2015, 26, 881–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villacis, D.; Yi, A.; Jahn, R.; Kephart, C.J.; Charlton, T.; Gamradt, S.C.; Romano, R.; Tibone, J.E.; Hatch, G.F.R., III. Prevalence of abnormal vitamin D levels among division I NCAA athletes. Sports Health 2014, 6, 340–347. [Google Scholar] [CrossRef]
- Sela, V.M.; Sela, F.E.R. A academia da terceira idade como um projeto do governo municipal de Maringá-PR para solucionar as falhas de mercado. Cad. Adm. 2012, 20, 82–90. [Google Scholar]

{kind=link}
| NW Group (x ± SD) | C Group (x ± SD) | NW Group vs. C Group | ||||||
|---|---|---|---|---|---|---|---|---|
| Trial 1 | Trial 2 | p(t-Test) ≤ 0.05 * | Trial 1 | Trial 2 | p(t-Test) ≤ 0.05 * | p(t-Test) ≤ 0.05 * Trial 1 | p(t-Test) ≤ 0.05 * Trial 2 | |
| Vitamin D level | 25.38 ± 10.73 | 29.52 ± 9.59 | 0.000 * | 24.06 ± 10.29 | 23.24 ± 8.12 | 0.291 | 0.311 | 0.040 * |
| Health Components and Factors | NW Group (x ± SD) | C Group (x ± SD) | NW Group vs. C Group | |||||
|---|---|---|---|---|---|---|---|---|
| Trial 1 | Trial 2 | p(t-Test) ≤ 0.05 * | Trial 1 | Trial 2 | p(t-Test) ≤ 0.05 * | p(t-Test) ≤ 0.05 * Trial 1 | p(t-Test) ≤ 0.05 * Trial 2 | |
| Physical Component Summary (PCS) | 59.25 ± 3.28 | 72.18 ± 4.23 | 0.000 * | 58.62 ± 4.62 | 58.39 ± 2.87 | 0.520 | 0.833 | 0.000 * |
| Physical Functioning (PF) | 66.42 ± 4.18 | 76.45 ± 5.41 | 0.000 * | 63.13 ± 3.76 | 62.66 ± 3.87 | 0.503 | 0.467 | 0.000 * |
| Role-physical (RF) | 51.82 ± 5.11 | 64.61 ± 3.28 | 0.000 * | 53.46 ± 5.35 | 53.76 ± 4.56 | 0.765 | 0.376 | 0.000 * |
| Bodily Pain (BP) | 59.35 ± 4.75 | 71.52 ± 3.16 | 0.000 * | 62.00 ± 3.87 | 62.85 ± 5.01 | 0.381 | 0.401 | 0.002 * |
| General Health (GH) | 59.45 ± 3.11 | 76.15 ± 5.55 | 0.000 * | 55.76 ± 4.99 | 54.24 ± 4.62 | 0.053 | 0.501 | 0.000 * |
| Mental Component Summary (MCS) | 63.39 ± 5.85 | 76.14 ± 4.37 | 0.000 * | 61.87 ± 5.63 | 62.54 ± 3.98 | 0.353 | 0.748 | 0.000 * |
| Vitality (VT) | 60.80 ± 4.16 | 75.60 ± 3.56 | 0.000 * | 64.88 ± 4,21 | 64.71 ± 5.33 | 0.907 | 0.433 | 0.000 * |
| Social Functioning (SF) | 75.96 ± 4.77 | 86.16 ± 5.88 | 0.000 * | 69.49 ± 3.54 | 67.72 ± 4.21 | 0.055 | 0.282 | 0.000 * |
| Role-emotional (RE) | 62.74 ± 3.87 | 74.80 ± 4.97 | 0.025 * | 57.59 ± 5.29 | 59.76 ± 3.66 | 0.155 | 0.401 | 0.000 * |
| Mental Health (MH) | 54.05 ± 5.21 | 68.00 ± 4.65 | 0.000 * | 52.94 ± 5.47 | 55.82 ± 4.87 | 0.027 * | 0.318 | 0.000 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podsiadło, S.; Skiba, A.; Kałuża, A.; Ptaszek, B.; Stożek, J.; Skiba, A.; Marchewka, A. Influence of Nordic Walking Training on Vitamin D Level in the Blood and Quality of Life among Women Aged 65–74. Healthcare 2021, 9, 1146. https://doi.org/10.3390/healthcare9091146
Podsiadło S, Skiba A, Kałuża A, Ptaszek B, Stożek J, Skiba A, Marchewka A. Influence of Nordic Walking Training on Vitamin D Level in the Blood and Quality of Life among Women Aged 65–74. Healthcare. 2021; 9(9):1146. https://doi.org/10.3390/healthcare9091146
Chicago/Turabian StylePodsiadło, Szymon, Agnieszka Skiba, Anna Kałuża, Bartłomiej Ptaszek, Joanna Stożek, Amadeusz Skiba, and Anna Marchewka. 2021. "Influence of Nordic Walking Training on Vitamin D Level in the Blood and Quality of Life among Women Aged 65–74" Healthcare 9, no. 9: 1146. https://doi.org/10.3390/healthcare9091146