
Comparison of Dietary Behaviors and the Prevalence of Metabolic Syndrome in Single- and Multi-Person Households among Korean Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Household Types
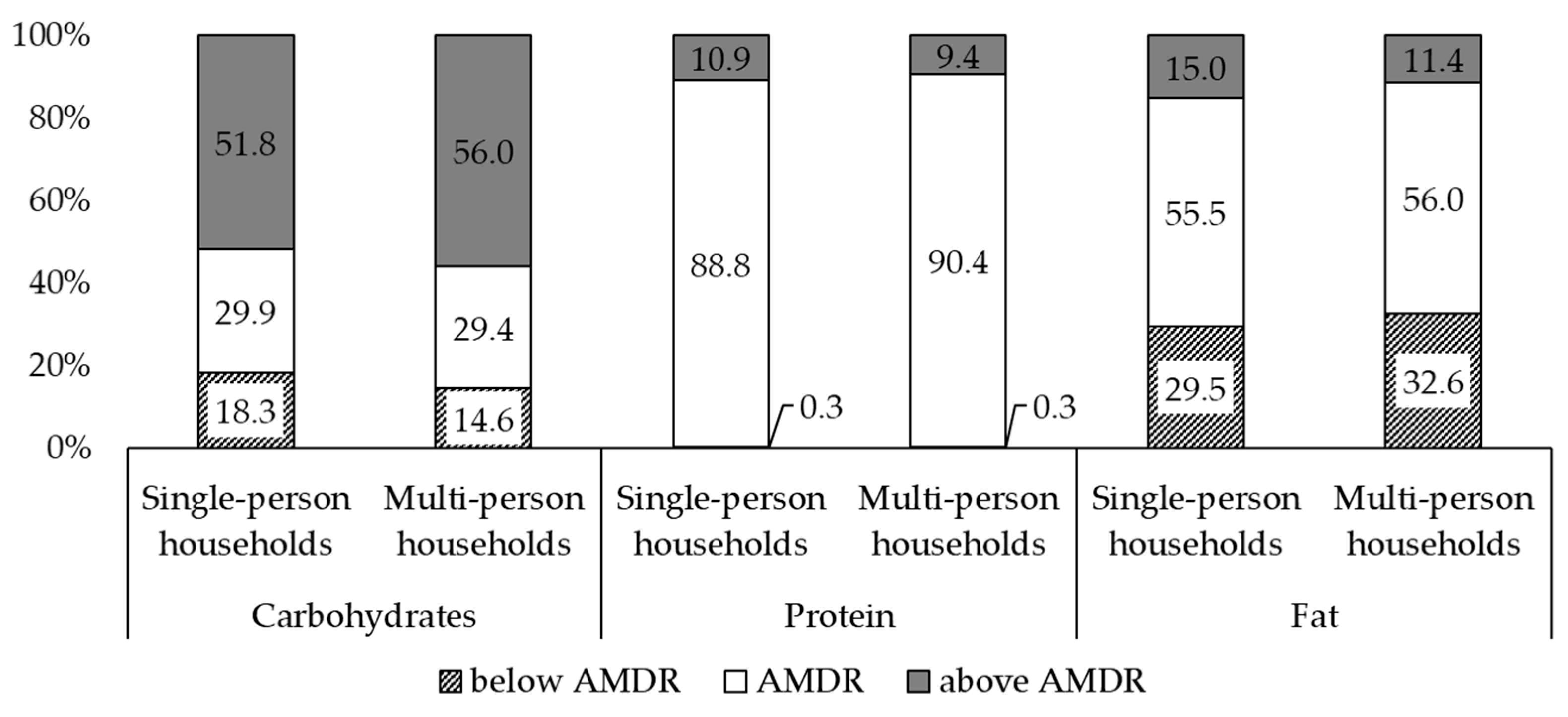
2.3. Nutrient Intake and Dietary Behaviors
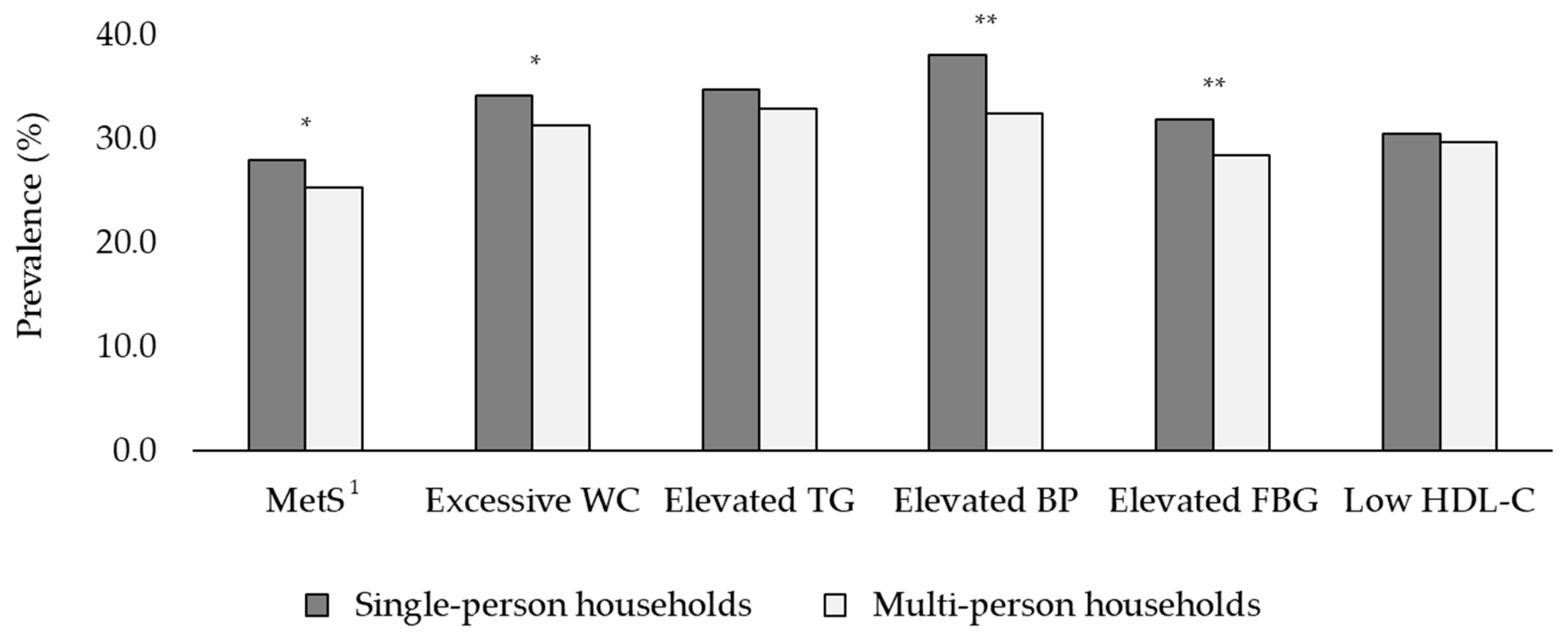
2.4. Definition of MetS and Its Components
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistics Korea. Status and Charateristics of Single-Person Households in Population and Housing Census. Available online: https://eiec.kdi.re.kr/policy/materialView.do?num=180908 (accessed on 1 September 2020).
- Yi, Y.H.; Kim, Y.J.; Cho, D.Y. Family type and health behaviors in elderly: Korean National Health and Nutrition Examination Survey (KNHANES), 2010–2012. Korean J. Health Serv. Manag. 2014, 8, 199–207. [Google Scholar] [CrossRef]
- Statistics Korea. Households Projections: 2017–2047. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/2/6/index.board (accessed on 1 September 2020).
- Lee, Y.B. One-person households and their policy implications. Health Welf. Forum 2017, 252, 64–77. [Google Scholar]
- Tak, Y.J.; Kim, Y.J.; Lee, S.Y.; Lee, J.G.; Jung, D.W.; Yi, Y.H.; Cho, Y.H.; Choi, E.J.; Nam, K.J. Health care behavior of people 60 years and older in Korea according to family type and sociodemographic factors-the 5th Korea National Health and Nutrition Examination Survey. J. Korean Geriatr. Soc. 2013, 17, 7–17. [Google Scholar] [CrossRef]
- Lee, M.; Choi, Y.; Lee, S. An exploratory study of the characteristics of one-person household and its social implication. Kookmin Soc. Sci. Rev. 2014, 27, 229–253. [Google Scholar]
- Park, J.H.; Min, S.; Eoh, Y.; Park, S.H. The elderly living in single-person households in South Korea: A latent profile analysis of self-esteem, life satisfaction, and depression. Qual. Life Res. 2021, 30, 1083–1092. [Google Scholar] [CrossRef]
- Kang, E.; Lee, M. Single-person households in South Korea and their policy implications. Health Welf. Policy Forum 2016, 234, 47–56. [Google Scholar]
- Kim, A. Effect of health behaviors, dietary habits, and psychological health on metabolic syndrome in one-person households among Korean young adults. J. Converg. Inf. Technol. 2018, 16, 493–509. [Google Scholar]
- Kim, M.A.; Choi, S.E.; Moon, J.H. Effect of heath behavior, physical health and mental health on heath-related quality of life in middle aged women: By using the 2014 Korea Health Panel Data. J. Korean Acad. Soc. Home Care Nurs. 2019, 26, 72–80. [Google Scholar]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the metabolic syndrome in the United States, 2003–2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.Y.; Lee, J.Y.; Song, J.; Lee, S.; Lee, J.; Lim, B.; Kim, H.; Huh, S. Cause-of-death statistics in the Republic of Korea, 2014. J. Korean Med. Assoc. 2016, 59, 221–232. [Google Scholar] [CrossRef] [Green Version]
- Korean Society of Cardiometabolic Syndrome. Metabolic Syndrome Fact Sheet in Korea 2021; Korean Society of CardioMetabolic Syndrome: Incheon, Korea, 2021. [Google Scholar]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Li, X.; Lin, H.; Fu, X.; Lin, W.; Li, M.; Zeng, X.; Gao, Q. Metabolic syndrome and stroke: A meta-analysis of prospective cohort studies. J. Clin. Neurosci. 2017, 40, 34–38. [Google Scholar] [CrossRef]
- Ju, S.Y.; Lee, J.Y.; Kim, D.H. Association of metabolic syndrome and its components with all-cause and cardiovascular mortality in the elderly: A meta-analysis of prospective cohort studies. Medicine 2017, 96, e8491. [Google Scholar] [CrossRef]
- Carnethon, M.R.; Loria, C.M.; Hill, J.O.; Sidney, S.; Savage, P.J.; Liu, K. Risk factors for the metabolic syndrome: The Coronary Artery Risk Development in Young Adults (CARDIA) study, 1985–2001. Diabetes Care 2004, 27, 2707–2715. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Liu, X.; Liu, Y.; Sun, X.; Wang, B.; Ren, Y.; Zhao, Y.; Zhou, J.; Han, C.; Yin, L. Leisure-time physical activity and incident metabolic syndrome: A systematic review and dose-response meta-analysis of cohort studies. Metabolism 2017, 75, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kang, M. Sedentary behavior and metabolic syndrome in physically active adults: National Health and Nutrition Examination Survey 2003–2006. Am. J. Hum. Biol. 2019, 31, e23225. [Google Scholar] [CrossRef] [PubMed]
- Lemes, I.R.; Sui, X.; Fernandes, R.A.; Blair, S.N.; Turi-Lynch, B.C.; Codogno, J.S.; Monteiro, H.L. Association of sedentary behavior and metabolic syndrome. Public Health 2019, 167, 96–102. [Google Scholar] [CrossRef]
- Suliga, E.; Cieśla, E.; Rębak, D.; Kozieł, D.; Głuszek, S. Relationship between sitting time, physical activity, and metabolic syndrome among adults depending on body mass index (BMI). Med. Sci. Monit. 2018, 24, 7633. [Google Scholar] [CrossRef] [PubMed]
- Bazshahi, E.; Sheikhhossein, F.; Amini, M.R.; Shab-Bidar, S. The association of dietary energy density and the risk of obesity, type 2 diabetes and metabolic syndrome: A systematic review and meta-analysis of observational studies. Int. J. Clin. Pract. 2021, e14291. [Google Scholar] [CrossRef]
- Song, S.; Lee, J.E.; Song, W.O.; Paik, H.Y.; Song, Y. Carbohydrate intake and refined-grain consumption are associated with metabolic syndrome in the Korean adult population. J. Acad. Nutr. Diet. 2014, 114, 54–62. [Google Scholar] [CrossRef]
- Lee, K.W.; Shin, D. A healthy beverage consumption pattern is inversely associated with the risk of obesity and metabolic abnormalities in Korean adults. J. Med. Food 2018, 21, 935–945. [Google Scholar] [CrossRef]
- Aleixandre, A.; Miguel, M. Dietary fiber in the prevention and treatment of metabolic syndrome: A review. Crit. Rev. Food Sci. Nutr. 2008, 48, 905–912. [Google Scholar] [CrossRef]
- Wei, J.; Zeng, C.; Gong, Q.Y.; Li, X.X.; Lei, G.H.; Yang, T.B. Associations between dietary antioxidant intake and metabolic syndrome. PLoS ONE 2015, 10, e0130876. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.F.; Li, X.; Shi, M.; Li, D. n-3 polyunsaturated fatty acids and metabolic syndrome risk: A meta-analysis. Nutrients 2017, 9, 703. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Rodas, M.C.; Valenzuela, R.; Videla, L.A. Relevant aspects of nutritional and dietary interventions in non-alcoholic fatty liver disease. Int. J. Mol. Sci. 2015, 16, 25168–25198. [Google Scholar] [CrossRef] [Green Version]
- Heo, Y.K.; Sim, K.H. Dietary attitude of single households in metropolitan areas. Korean J. Food Nutr. 2016, 29, 735–745. [Google Scholar] [CrossRef] [Green Version]
- Chae, H.J.; Kim, M. Health behavior, health service use, and health related quality of life of adult women in one-person and multi-person households. Korean J. Women Health Nurs. 2019, 25, 299–314. [Google Scholar] [CrossRef]
- Kang, E.; Kim, H.; Kim, Y. Leisure activity types and depressive symptoms among middle aged people living alone. Health Social Welf. Rev. 2017, 37, 184–215. [Google Scholar]
- Kwak, J.H.; Choi, S.; Ju, D.J.; Lee, M.; Paik, J.K. An analysis of the association between chronic disease risk factors according to household type for the middle-aged: The Korea National Health and Nutrition Examination Survey (2013~2015). Korean J. Food Nutr. 2021, 34, 88–95. [Google Scholar]
- Kweon, S.; Kim, Y.; Jang, M.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Korea Centers for Disease Control and Prevention. User Guide for the Fourth Korea National Health and Nutrition Examination Survey (KNHANES V); Korea Centers for Disease Control and Prevention: Cheongwon, Korea, 2016. [Google Scholar]
- Im, J.G.; Kim, S.H.; Lee, G.Y.; Joung, H.; Park, M.J. Inadequate calcium intake is highly prevalent in Korean children and adolescents: The Korea National Health and Nutrition Examination Survey (KNHANES) 2007–2010. Public Health Nutr. 2014, 17, 2489–2495. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.W.; Cho, W. The consumption of dairy products is associated with reduced risks of obesity and metabolic syndrome in Korean women but not in men. Nutrients 2017, 9, 630. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult treatment panel III). Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Alberti, K.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- Bae, C.Y.; Piao, M.; Kim, M.; Im, Y.; Kim, S.; Kim, D.; Choi, J.; Cho, K.H. Biological age and lifestyle in the diagnosis of metabolic syndrome: The NHIS health screening data, 2014–2015. Sci. Rep. 2021, 11, 1–11. [Google Scholar]
- Laaksonen, D.E.; Niskanen, L.; Punnonen, K.; Nyyssönen, K.; Tuomainen, T.P.; Valkonen, V.P.; Salonen, R.; Salonen, J.T. Testosterone and sex hormone–binding globulin predict the metabolic syndrome and diabetes in middle-aged men. Diabetes Care 2004, 27, 1036–1041. [Google Scholar] [CrossRef] [Green Version]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.R.; Han, K.; Choi, J.Y.; Ersek, J.; Liu, J.; Jo, S.J.; Lee, K.S.; Yim, H.W.; Lee, W.C.; Park, Y.G.; et al. Age-and sex-specific relationships between household income, education, and diabetes mellitus in Korean adults: The Korea National Health and Nutrition Examination Survey, 2008–2010. PLoS ONE 2015, 10, e0117034. [Google Scholar] [CrossRef]
- Kim, E.; Park, S. Comparison of health behaviors, disease prevalence between one-person women and multiple households women in Korea. J. Korean Public Health Nurs. 2016, 30, 483–494. [Google Scholar] [CrossRef] [Green Version]
- Shang, X.; Scott, D.; Hodge, A.; English, D.R.; Giles, G.G.; Ebeling, P.R.; Sanders, K.M. Dietary protein from different food sources, incident metabolic syndrome and changes in its components: An 11-year longitudinal study in healthy community-dwelling adults. Clin Nutr. 2017, 36, 1540–1548. [Google Scholar] [CrossRef]
- Malik, V.S.; Li, Y.; Tobias, D.K.; Pan, A.; Hu, F.B. Dietary protein intake and risk of type 2 diabetes in US men and women. Am. J. Epidemiol. 2016, 183, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Beunza, J.J.; Bes-Rastrollo, M.; Pajares, R.M.; Martínez-González, M.Á. Vegetable protein and fiber from cereal are inversely associated with the risk of hypertension in a Spanish cohort. Arch. Med. Res. 2006, 37, 778–786. [Google Scholar] [CrossRef]
- Julibert, A.; del Mar Bibiloni, M.; Tur, J.A. Dietary fat intake and metabolic syndrome in adults: A systematic review. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 887–905. [Google Scholar] [CrossRef]
- Jeon, Y.; Ahn, B. Food consumption behaviors according to household types. J. Rural Dev. 2016, 39, 73–95. [Google Scholar]
- Lee, K.; Hwang, Y.; Ban, H.; Lim, S.; Jin, H.; Lee, H. Impact of the growth of single-person households on the food market and policy tasks. Korea Rural Econ. Inst. 2015, 10, 1–241. [Google Scholar]
- Kang, N.Y.; Jung, B.M. Analysis of the difference in nutrients intake, dietary behaviors and food intake frequency of single-and non single-person households: The Korea National Health and Nutrition Examination Survey (KNHANES), 2014–2016. Korean J. Community Nutr. 2019, 24, 1–17. [Google Scholar] [CrossRef]
- Lee, J.; Shin, A. Vegetable and fruit intake in one person household: The Korean National Health and Nutrition Examination Survey (2010~2012). J. Nutr. Health 2015, 48, 269–276. [Google Scholar] [CrossRef]
- Berge, J.M.; MacLehose, R.F.; Loth, K.A.; Eisenberg, M.E.; Fulkerson, J.A.; Neumark-Sztainer, D. Family meals. Associations with weight and eating behaviors among mothers and fathers. Appetite 2012, 58, 1128–1135. [Google Scholar] [CrossRef] [Green Version]
- Larson, N.I.; Nelson, M.C.; Neumark-Sztainer, D.; Story, M.; Hannan, P.J. Making time for meals: Meal structure and associations with dietary intake in young adults. J. Am. Diet. Assoc. 2009, 109, 72–79. [Google Scholar] [CrossRef]
- Newman, S.L.; Tumin, R.; Andridge, R.; Anderson, S.E. Family meal frequency and association with household food availability in United States multi-person households: National Health and nutrition examination survey 2007–2010. PLoS ONE 2015, 10, e0144330. [Google Scholar] [CrossRef] [Green Version]
- Choi, M.K.; Park, E.S.; Kim, M.H. Home meal replacement use and eating habits of adults in one-person households. Korean J. Community Nutr. 2019, 24, 476–484. [Google Scholar] [CrossRef]
- Vesnaver, E.; Keller, H.H. Social influences and eating behavior in later life: A review. J. Nutr. Gerontol. Geriatr. 2011, 30, 2–23. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Shin, D. Relationships of dietary factors with obesity, hypertension, and diabetes by regional type among single-person households in Korea. Nutrients 2021, 13, 1218. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Park, A.; Kim, K. Food insecurity and depressive symptoms of older adults living alone in South Korea. Ageing Soc. 2019, 39, 2042–2058. [Google Scholar] [CrossRef]
- Han, H.; Oh, E.; Joung, S. An analysis on variables related to the financial satisfaction of one-person households. Financ. Plan. Rev. 2014, 7, 173. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Household Type | p-Value 1 | ||
|---|---|---|---|---|
| Single-Person Households | Multi-Person Households | |||
| n (Wt’d %) | n (Wt’d %) | n (Wt’d %) | ||
| Total | 21,944 (100.00) | 2522 (9.19) | 19,422 (90.81) | |
| Mean number of household members | 3.09 ± 0.02 2 | 1.00 ± 0.00 | 3.30 ± 0.01 | |
| Sex | 0.3528 | |||
| Men | 9143 (49.64) | 945 (50.82) | 8198 (49.53) | |
| Women | 12,801 (50.36) | 1577 (49.18) | 11,224 (50.47) | |
| Age (years) | <0.0001 | |||
| 19–29 | 2498 (18.19) | 239 (19.92) | 2259 (18.01) | |
| 30–49 | 7465 (39.29) | 422 (26.38) | 7043 (40.60) | |
| 50–64 | 6371 (26.52) | 616 (21.88) | 5755 (27.00) | |
| ≥65 | 5610 (16.00) | 1245 (31.82) | 4365 (14.39) | |
| Education level | <0.0001 | |||
| ≤Middle school | 6990 (22.76) | 1402 (38.22) | 5588 (21.20) | |
| High school | 7100 (36.13) | 572 (28.70) | 6528 (36.88) | |
| ≥College | 7854 (41.11) | 548 (33.08) | 7306 (41.92) | |
| Income | <0.0001 | |||
| Lowest | 4058 (14.21) | 1279 (40.27) | 2779 (11.57) | |
| Lower middle | 5397 (23.44) | 592 (23.19) | 4805 (23.46) | |
| Upper middle | 6105 (29.95) | 361 (20.52) | 5744 (30.90) | |
| Highest | 6384 (32.41) | 290 (16.03) | 6094 (34.06) | |
| Marital status | <0.0001 | |||
| Married | 18,530 (76.71) | 1864 (55.17) | 16,666 (78.89) | |
| Single | 3414 (23.29) | 658 (44.83) | 2756 (21.11) | |
| Occupation | 0.0011 | |||
| No | 8775 (35.76) | 1259 (39.76) | 7516 (35.36) | |
| Yes | 13,169 (64.24) | 1263 (60.24) | 11,906 (64.64) | |
| Region | 0.0209 | |||
| Urban | 17,845 (86.10) | 1924 (83.31) | 15,921 (86.38) | |
| Rural | 4099 (13.90) | 598 (16.69) | 3501 (13.62) | |
| Drinking status | 0.3283 | |||
| Never/rarely | 10,309 (41.38) | 1353 (42.23) | 8956 (52.95) | |
| ≤1 time/month | 7017 (35.71) | 677 (33.94) | 6340 (19.81) | |
| >1 time/month | 4618 (22.91) | 492 (23.83) | 4126 (27.24) | |
| Smoking status | <0.0001 | |||
| Never | 13,695 (57.86) | 1551 (52.95) | 12,144 (58.36) | |
| Former smoker | 4647 (21.67) | 461 (19.81) | 4186 (21.86) | |
| Current smoker | 3602 (20.47) | 510 (27.24) | 3092 (19.78) | |
| Regular physical activity 3 | 0.6259 | |||
| Yes | 9856 (46.66) | 1082 (47.27) | 8774 (46.60) | |
| No | 12,088 (53.34) | 1440 (52.73) | 10,648 (53.40) | |
| Household Type | p-Value 1 | ||
|---|---|---|---|
| Single-Person Households | Multi-Person Households | ||
| Mean ± SE | Mean ± SE | ||
| Total energy, kcal | 2021 ± 23 | 1963 ± 13 | 0.0165 |
| Plant sources 2, % of energy | 81.70 ± 0.34 | 82.70 ± 0.19 | 0.2247 |
| Animal sources 2, % of energy | 18.30 ± 0.34 | 17.30 ± 0.19 | 0.0063 |
| Carbohydrates, % of energy | 64.83 ± 0.30 | 65.80 ± 0.17 | 0.0019 |
| Proteins, % of energy | 14.85 ± 0.13 | 14.73 ± 0.07 | 0.3662 |
| Plant proteins 2, % of energy | 7.62 ± 0.06 | 7.84 ± 0.04 | 0.0004 |
| Animal proteins 2, % of energy | 7.23 ± 0.15 | 6.88 ± 0.08 | 0.0244 |
| Total fats, % of energy | 20.32 ± 0.24 | 19.47 ± 0.14 | 0.0014 |
| Saturated fats, % of energy | 6.40 ± 0.10 | 6.05 ± 0.05 | 0.0008 |
| Monounsaturated fats, % of energy | 6.35 ± 0.11 | 6.06 ± 0.06 | 0.0126 |
| Polyunsaturated fats, % of energy | 5.26 ± 0.08 | 5.05 ± 0.04 | 0.0125 |
| Household Type | p-Value 1 | ||
|---|---|---|---|
| Single-Person Households | Multi-Person Households | ||
| Mean ± SE | Mean ± SE | ||
| Grains and associated products | 285.96 ± 4.32 | 283.70 ± 2.55 | 0.6376 |
| Starchy vegetables | 38.56 ± 2.77 | 37.02 ± 1.54 | 0.5867 |
| Sugar and sweets | 10.33 ± 0.50 | 9.85 ± 0.29 | 0.3636 |
| Legumes | 40.11 ± 2.32 | 37.26 ± 1.27 | 0.2668 |
| Nuts and seeds | 6.42 ± 0.57 | 7.75 ± 0.50 | 0.0544 |
| Vegetables and mushrooms | 295.75 ± 4.88 | 310.76 ± 3.36 | 0.0064 |
| Fruits | 151.61 ± 6.35 | 168.33 ± 3.66 | 0.0160 |
| Seaweed | 18.05 ± 1.60 | 28.28 ± 1.51 | <0.0001 |
| Meat | 109.36 ± 4.31 | 102.62 ± 2.72 | 0.1283 |
| Eggs | 27.54 ± 1.60 | 24.72 ± 0.76 | 0.0660 |
| Fish and shellfish | 86.80 ± 3.93 | 97.73 ± 2.71 | 0.0121 |
| Milk and dairy products | 95.01 ± 5.29 | 74.74 ± 2.25 | 0.0001 |
| Alcoholic and non-alcoholic beverages | 356.67 ± 12.89 | 326.45 ± 7.31 | 0.0217 |
| Oils and fats | 7.93 ± 0.34 | 6.72 ± 0.15 | 0.0003 |
| Others | 37.30 ± 1.26 | 34.13 ± 0.67 | 0.0170 |
| Total DVS | 10.10 ± 0.07 | 10.43 ± 0.04 | <0.0001 |
| Household Types | p-Value 1 | ||
|---|---|---|---|
| Single-Person Households | Multi-Person Households | ||
| Mean ± SE | Mean ± SE | ||
| Total eating episodes | 5.32 ± 0.05 | 5.37 ± 0.03 | 0.3192 |
| Total main meal episodes | 2.54 ± 0.01 | 2.58 ± 0.01 | 0.0099 |
| Total snacking episodes | 2.77 ± 0.05 | 2.79 ± 0.03 | 0.7960 |
| Energy from foods prepared at home, % | 37.09 ± 0.73 | 46.06 ± 0.46 | <0.0001 |
| Energy from foods prepared outside the home, % | 47.60 ± 1.17 | 43.35 ± 0.92 | <0.0001 |
| Report skipping breakfast, % | 21.81 ± 1.10 | 17.09 ± 0.42 | <0.0001 |
| Report eating all three main meals, % | 65.59 ± 1.30 | 70.30 ± 0.49 | 0.0007 |
| Report eating all main meals alone, % | 21.88 ± 1.08 | 4.00 ± 0.20 | <0.0001 |
| Report eating out at least 1 time per week, % | 29.02 ± 1.66 | 18.05 ± 0.46 | <0.0001 |
| Mild/moderate or severe food insecurity, % | 48.10 ± 1.39 | 44.65 ± 0.67 | 0.0202 |
| Household Type | ||
|---|---|---|
| Single-Person Households | Multi-Person Households | |
| AOR (95% CI) 1 | AOR (95% CI) | |
| Sex | ||
| Men | 0.87 (0.65–1.17) | 0.67 (0.60–0.75) |
| Women | 1.00 (ref.) | 1.00 (ref.) |
| Age (years) | ||
| 19–29 | 1.00 (ref.) | 1.00 (ref.) |
| 30–49 | 3.48 (2.09–5.80) | 3.89 (3.02–5.00) |
| 50–64 | 6.10 (3.40–10.94) | 7.15 (5.50–9.29) |
| ≥65 | 8.17 (4.46–14.97) | 10.79 (8.18–14.22) |
| Education level | ||
| ≤Middle school | 1.53 (1.08–2.17) | 1.78 (1.58–2.01) |
| High school | 1.15 (0.81–1.63) | 1.26 (1.14–1.39) |
| ≥College | 1.00 (ref.) | 1.00 (ref.) |
| Income | ||
| Lowest | 1.23 (0.81–1.89) | 1.29 (1.12–1.48) |
| Lower middle | 1.06 (0.68–1.65) | 1.11 (1.00–1.24) |
| Upper middle | 0.76 (0.50–1.15) | 1.08 (0.97–1.20) |
| Highest | 1.00 (ref.) | 1.00 (ref.) |
| Marital status | ||
| Married | 1.00 (ref.) | 1.00 (ref.) |
| Single | 1.03 (0.68–1.56) | 1.01 (0.83–1.25) |
| Occupation | ||
| Unemployed | 1.31 (1.04–1.65) | 1.09 (1.01–1.19) |
| Employed | 1.00 (ref.) | 1.00 (ref.) |
| Region | ||
| Urban | 1.01 (0.79–1.30) | 1.07 (0.94–1.20) |
| Rural | 1.00 (ref.) | 1.00 (ref.) |
| Drinking status | ||
| Never/rarely | 1.00 (ref.) | 1.00 (ref.) |
| ≤1 time/month | 0.77 (0.60–1.01) | 0.93 (0.85–1.02) |
| >1 time/month | 0.83 (0.60–1.14) | 1.20 (1.08–1.34) |
| Smoking status | ||
| Never | 1.00 (ref.) | 1.00 (ref.) |
| Former smoker | 0.80 (0.57–1.13) | 1.00 (0.88–1.13) |
| Current smoker | 1.13 (0.77–1.66) | 1.24 (1.08–1.42) |
| Regular physical activity 2 | ||
| Yes | 1.00 (ref.) | 1.00 (ref.) |
| No | 1.29 (1.04–1.60) | 1.05 (0.97–1.13) |
| Household Type | p-Value | ||
|---|---|---|---|
| Multi-Person Households | Single-Person Households | ||
| AOR (95% CI) 1 | |||
| MetS 2 | 1.00 (ref.) | 1.14 (1.02–1.29) | 0.0244 * 3 |
| Excessive WC | 1.00 (ref.) | 1.14 (1.01–1.28) | 0.0279 * |
| Elevated TG | 1.00 (ref.) | 1.09 (0.97–1.22) | 0.1684 |
| Elevated BP | 1.00 (ref.) | 1.28 (1.12–1.47) | 0.0003 ** |
| Elevated FBG | 1.00 (ref.) | 1.18 (1.05–1.33) | 0.0072 ** |
| Low HDL-C | 1.00 (ref.) | 1.04 (0.92–1.17) | 0.5177 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.W.; Shin, D. Comparison of Dietary Behaviors and the Prevalence of Metabolic Syndrome in Single- and Multi-Person Households among Korean Adults. Healthcare 2021, 9, 1116. https://doi.org/10.3390/healthcare9091116
Lee KW, Shin D. Comparison of Dietary Behaviors and the Prevalence of Metabolic Syndrome in Single- and Multi-Person Households among Korean Adults. Healthcare. 2021; 9(9):1116. https://doi.org/10.3390/healthcare9091116
Chicago/Turabian StyleLee, Kyung Won, and Dayeon Shin. 2021. "Comparison of Dietary Behaviors and the Prevalence of Metabolic Syndrome in Single- and Multi-Person Households among Korean Adults" Healthcare 9, no. 9: 1116. https://doi.org/10.3390/healthcare9091116