
The Impacts of Regional Regulatory Policies on the Prevention and Control of Chronic Diseases in China: A Mediation Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
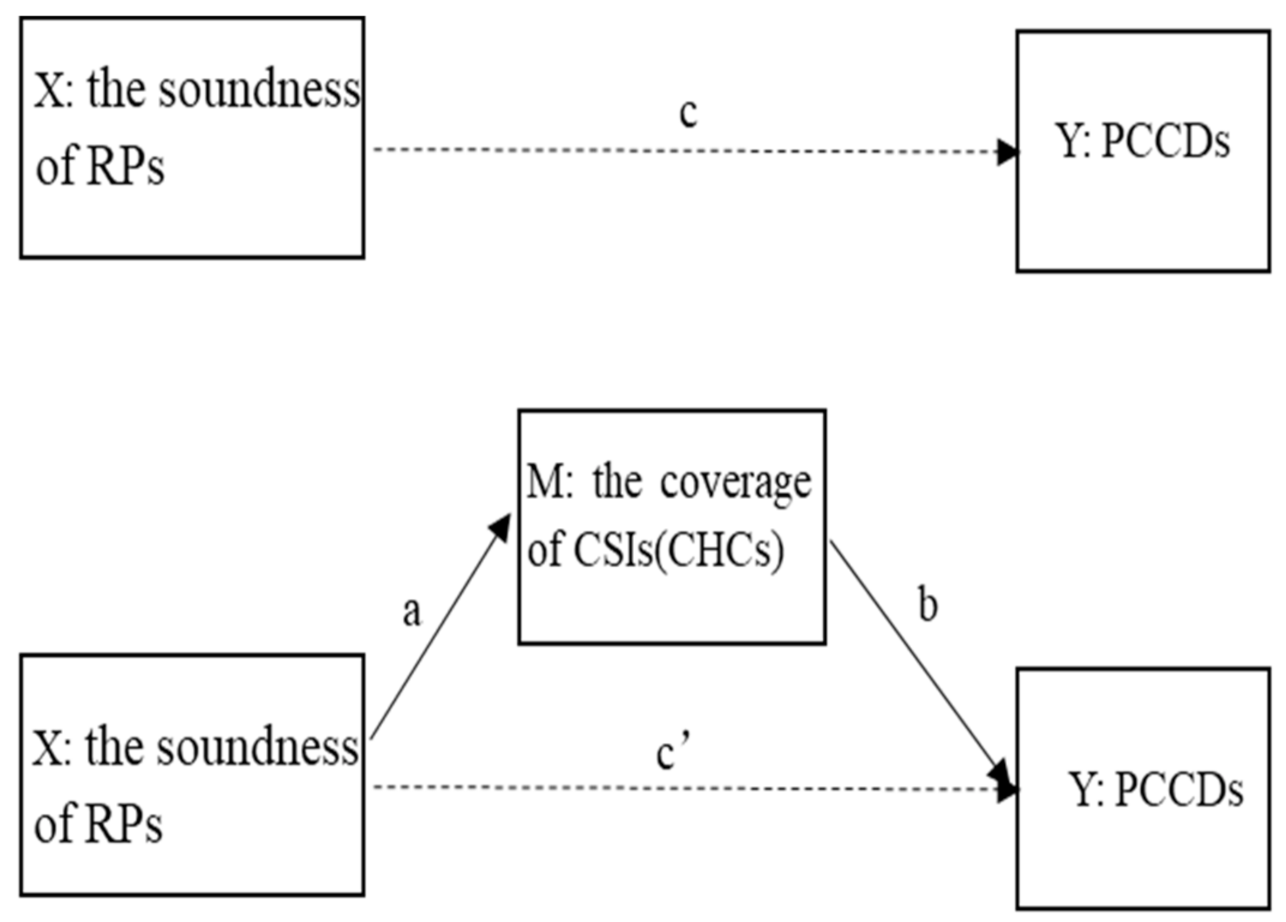
2.1. Study Design
2.2. Measurements
2.2.1. The Soundness of RPs
2.2.2. PCCDs
2.2.3. The Coverage of CSIs and CHCs
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Correlation Analysis
3.3. Regression Analysis
3.4. Mediation Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PCCDs | prevention and control of chronic diseases |
| RPs | regulatory policies |
| CSIs | community service institutions |
| CHCs | community health centres |
| SORM | soundness of the regulatory mechanism |
| RECR | regulatory element coverage rate |
| DPCR | departmental responsibilities clarity rate |
| RMAR | regulatory mechanism authority rate |
| AMCR | accountability mechanism clarity rate |
| NCDs | number of chronic diseases |
| ICC | intraclass correlation coefficient |
| CRCSI | coverage rate of the community service institutions |
| CRCHC | coverage rate of the community health centres |
| SD | standard deviation |
| IQR | interquartile range |
Appendix A

{kind=link}
| Name—ID | Description | Coding |
|---|---|---|
| Comprehensive coverage of regulatory elements—A1 | Record the content form involved in the file set | 1—long-term goal (over five years) 2—short-term goal (under five years) 3—put forward tasks and measure around the goal 4—policymaking 5—service (intervention) content 6—service (intervention) scope (region, population) 7—service process 8—operational norms 9—technical standards 10—institutional settings standards 11—personnel allocation standards 12—professional qualification standards 13—funding sources 14—funding standards 15—funds guarantee measures 16—material price standards 17—material supply management norms 18—information system construction standards 19—information monitoring standards 20—division of responsibility 21—monitoring and control mode 22—performance indexes and standards 23—reward and punishment measures 24—department coordination modes 25—evaluation indicators and standards |
| Well-defined responsibilities of stakeholders—A2 | A2-1: record department names | 1—provincial government 2—health commission 3—public health agencies 4—hospitals 5—primary health care institutions 6—finance bureau 7—human resources and social security bureau 8—policy security departments 9—health care security administration 10—education commission 11—civil affairs bureau 12—agriculture and rural affairs bureau 13—trading department 14—transportation commission 15—drug regulation administration 16—construction department 17—sports administration 18—environmental bureau 19—communication and news department 20—industrial information department 21—work safety administration 22—non-government organisations |
| A2-2: record the responsibility description of each department | 0—not mentioned 1—department responsibility mentioned in the policy documents | |
| A2-3: record the measurable responsibility description of each department | 0—not mentioned 1—measurable department responsibility mentioned in the policy documents | |
| Authority of regulatory mechanism—B1 | B1-1: record the government level in charge of the coordination of relevant departments | 1—coordinate the government 2—coordinate the health commission 3—coordinate public health agencies 4—coordinate hospitals 5—coordinate primary health care institutions 6—coordinate the finance bureau 7—coordinate the human resources and social security bureau 8—coordinate policy security departments 9—coordinate the health care security administration 10—coordinate the education commission 11—coordinate the civil affairs bureau 12—coordinate the agriculture and rural affairs bureau 13—coordinate the trading department 14—coordinate the transportation commission 15—coordinate the drug regulation administration 16—coordinate the construction department 17—coordinate the sports administration 18—coordinate the environmental bureau 19—coordinate the communication and news department 20—coordinate the industrial information department 21—coordinate the work safety administration 22—coordinate non-government organisations |
| B1-2: record file publishing level | 1—documents issued by legislative institution 2—documents issued by government 3—documents issued by multisectoral combination 4—documents issued by health commission 5—documents issued by public health agencies | |
| Well-defined regulatory accountability mechanism—B2 | Record the accountability mechanisms | 0—not mentioned 1—regulator and accountability mentioned in the policy documents |
References
- Health China Action Promotion Committee. Healthy China Action (2019–2030). Available online: http://www.gov.cn/xinwen/2019-07/15/content_5409694.htm (accessed on 15 July 2019).
- Human Development Unit of East Asia and Pacific Region. Toward a Healthy and Harmonious Life in China: Stemming the Rising Tide of Non-Communicable Diseases; World Bank: Washington, DC, USA, 2011; pp. 1–8. [Google Scholar]
- Lv, L.T.; Deng, S.L. The current status and development strategies of chronic disease management in China. Chin. J. Health Policy 2016, 9, 1–7. [Google Scholar]
- World Health Organization. Transforming our World: The 2030 Agenda for Sustainable Development. Available online: https://sdgs.un.org/2030agenda (accessed on 21 October 2019).
- Li, A.L.; Zhang, Y.; Bai, Y.M.; Shao, Y.Q.; Yuan, H.; Zhang, Y.Y.; Xiang, F.; Sheng, Y.W.; Hu, Z.H.; Peng, H. Analysis on the development process of important policies related to community chronic disease prevention and control. Chin. J. Prev. Control Chronic Dis. 2017, 25, 305–308. [Google Scholar]
- Wang, R.Y.; He, Z.Y.; Zhao, W.W.; Wang, Y.Y.; Zhang, M.; Sun, M.M. Research progress of chronic disease management. Chin. Gen. Pract. 2016, 19, 1989–1993. [Google Scholar]
- Huang, J.M.; Hu, X.F. Prevention and control effect of community chronic disease monitoring and tracking management mode of community chronic disease monitoring and tracking management mode on hypertension patients. Qingdao Med. J. 2018, 50, 280–282. [Google Scholar]
- Locke, K.; Noseworthy, R.; Davies, A. Management of diabetes mellitus in nova-scotia Micmac communities. J. Can. Diet Assoc. 1993, 54, 92–96. [Google Scholar]
- Pozo, F.D.; Toledo, P.D.; Jiménez, S.; Hernando, M.E.; Micheli-Tzanakou, E. Chronic patient’s management: The Copd example. In M-Health; Springer: Boston, MA, USA, 2006. [Google Scholar]
- World Health Organization. Integrated Chronic Disease Prevention and Control. Available online: https://www.who.int/chp/about/integrated_cd (accessed on 15 July 2019).
- Wang, Z.X.; Shi, J.W.; Wu, Z.G.; Xie, H.L.; Yu, Y.F.; Li, P.; Liu, R.; Jing, L.M. Changes in chronic disease management among community health centers (CHCs) in China: Has health reform improved CHC ability? Int. J. Health Plan. Manag. 2017, 32, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Chen, X. Community health service and health management in the role of chronic diseases prevention and control analysis. Med. J. Liaoning 2017, 31, 41–42. [Google Scholar]
- Lin, M. Comparative Analysis of the Status of Community Service Organizations in China; Tianjin University Finance and Economics: Tianjin, China, 2017. [Google Scholar]
- Ling, Y. Ponderations on the development of promoting community health service based on health management of chronic disease. J. Anhui Univ. Technol. 2013, 30, 51–52. [Google Scholar]
- Wong, E.L.Y.; Woo, J.; Hui, E.; Chan, C.; Chan, W.L.S.; Cheung, A.W.L. Primary care for diabetes mellitus: Perspective from older patients. Patient Prefer. Adher. 2011, 5, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Mallawaarachchi, D.S.V.; Wickremasinghe, S.C.; Somatunga, L.C.; Siriwardena, V.T.; Gunawardena, N.S. Healthy lifestyle centres: A service for screening noncommunicable diseases through primary health-care institutions in Sri Lanka. WHO South East Asia J. Public Health 2016, 5, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.V.; Bochkareva, E.V.; Varakin, I.I.; Kokurina, E.V. Screening for chronic cerebrovascular diseases in primary health care facilities. Profil. Med. 2013, 16, 27–30. [Google Scholar]
- Sharma, A.; Patnaik, R.; Garg, S.; Ramachandran, P. Detection & management of anaemia in pregnancy in an urban primary health care institution. Indian J. Med. Res. 2008, 128, 45–51. [Google Scholar]
- Donabedian, A. The quality of care. How can it be assessed? JAMA 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Wang, L.; Wu, H.; Chang, L.J.; Lin, K.K.; Liu, X.Y.; Wei, X.J.; Jiang, Y.R.; Chen, Y. Emergency management strategies of community health service agencies in the joint prevention and control of COVID-19. Nurs. Integr. Tradit. Chin. West Med. 2020, 6, 58–61. [Google Scholar]
- Vedanthan, R.; Kamano, J.H.; DeLong, A.K.; Naanyu, V.; Binanay, C.A.; Bloomfield, G.S.; Chrysanthopoulou, S.A.; Finkelstein, E.A.; Hogan, J.W.; Horowitz, C.R.; et al. Community health workers improve linkage to hypertension care in Western Kenya. J. Am. Coll. Cardiol. 2019, 74, 1897–1906. [Google Scholar] [CrossRef]
- Chen, W.L.; Zhang, C.G.; Cui, Z.Y.; Wang, J.Y.; Zhao, J.; Wang, J.W.; Wang, X.; Yu, J.M. The impact of social capital on physical activity and nutrition in China: The mediating effect of health literacy. BMC Public Health 2019, 19, 1713. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, C.Y.; Zhou, Q.Y.; Wang, X.; Gao, X.; Tian, Z.; Chen, R.; Xu, T.Q.; Hao, C.; Chen, Z.; et al. Comprehensive analysis of maternal health management and monitoring mechanisms in Beijing and Shanghai. Chin. Health Serv. Manag. 2019, 36, 466–469. [Google Scholar]
- Yan, Y.Y.; Pu, Y.; Zhang, Q.M.; Zhang, Y.Y.; Chen, C.Y.; Yang, X.; Li, L.; Hao, M.; Pu, C.; Chen, F. Degree of perfection in the management mechanism of infectious diseases prevention in Yunnan and Guangxi—A quantitative evaluation from the perspective of policy documents. Chin. Manag. Health Serv. Adm. 2020, 40, 53–58. [Google Scholar]
- Li, L.; Li, C.Y.; Zhou, Q.Y.; Pu, C.; Xu, L.Z.; Xu, T.Q.; Hao, C.; Hu, Z.; Hao, M. Differences of maternal mortality rate between Shanghai and New York city from the perspective of regulatory policy. Chin. Med. J. 2020, 133, 792–799. [Google Scholar] [CrossRef] [Green Version]
- Hao, M. Pursuing Excellence—Building an Appropriate Public Health System; CPC Central Party School Press: Beijing, China, 2021. [Google Scholar]
- World Health Organization. Noncommunicable_Diseases. Available online: https://www.who.int/health-topics/noncommunicable-diseases#tab=tab_1 (accessed on 25 July 2019).
- World Health Organization. ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS). Available online: https://icd.who.int/browse11/l-m/en (accessed on 12 February 2020).
- Regan, S.; Macdonald, M.; Allan, D.E.; Martin, C.; Peroff-Johnston, N. Public health human resources: A comparative analysis of policy documents in two Canadian provinces. Hum. Resour. Health 2014, 12, 13. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.H.; John, S.; Chen, X.X.; Wang, Y.F.; Gong, J.Q.; Meng, Q.Q.; Wang, G.W.; Wang, H.L. China Health and Retirement Longitudinal Study Wave 4 User’s Guide; National School of Development, Peking University: Beijing, China, 2020. [Google Scholar]
- China Health and Retirement Longitudinal Survey, CHARLS. Available online: http://charls.pku.edu.cn/pages/about/charls/zh-cn.html (accessed on 13 September 2019).
- Yuan, Y.Y.; Li, H.F. A study on the gender difference of falls among the elderly in urban and rural China: Based on CHARLS 2015 data. Popul. Soc. 2020, 36, 46–57. [Google Scholar] [CrossRef]
- Zhang, L.Y.; Zhang, H.N. Financial constraints and family entrepreneurship—urban and rural differences in China. J. Financ. Res. 2013, 09, 123–135. [Google Scholar]
- Qiu, Y.D.; Li, H.; Yang, Z.Y.; Liu, Q.; Wang, K.; Li, R.J.; Xing, D.; Hou, Y.F.; Lin, J.H. The prevalence and economic burden of pain on middle-aged and elderly Chinese people: Results from the China health and retirement longitudinal study. BMC Health Serv. Res. 2020, 20, 600. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Methodology in the social sciences. In Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Efron, B.; Tibshirani, R.J. An Introduction to the bootstrap. J. Am. Stat. Assoc. 1993, 89, 436. [Google Scholar]
- Kong, L.Z. Thoughts on chronic diseases prevention and control in China. Chin. Health Serv. Manag. 2012, 5, 2–5. [Google Scholar]
- General Office of the State Council of the People’s Republic of China. The General Office of the State Council on Printing and Distributing China’s Medium- and Long-Term Plan for the Prevention and Treatment of Chronic Diseases (2017–2025). Available online: http://www.gov.cn/zhengce/content/2017-02/14/content_5167886.htm (accessed on 14 February 2017).
- Zhang, H.; Xiong, J.Y.; Guan, W.B.; Jiang, M.Z.; Shen, X.; Ma, J. Analyzing the management effects of chronic diseases: Taking national demonstration zone of chronic diseases comprehensive prevention and control as an example. Chin. Hosp. 2019, 23, 15–17. [Google Scholar]
- Zhang, L. Evaluation on Diabetes Mellitus Management in Community Health Service; Jinan University: Jinan, China, 2015. [Google Scholar]
- Chen, S.L. Research on the role of community health service agencies in the prevention and treatment of chronic diseases. Pract. J. Card. Cereb. Pneumal Vasc. Dis. 2011, 19, 514–515. [Google Scholar]
- Wang, S.Z.; Luo, F.P. Grassroots policy mobilization: A new way to facilitate residents’ participation. Nanjing J. Soc. Sci. 2020, 4, 63–71. [Google Scholar]
- Feng, J.J.; Liu, Y.F.; Jing, R.F. International experience of chronic disease management and enlightenment. China Pharm. 2017, 28, 1009–1012. [Google Scholar]
- Wu, Z.J.; Jian, W.Y. Availability of community health management services for elderly patients with chronic diseases and its social determinants. Chin. Gen. Pract. 2015, 18, 3469–3472. [Google Scholar]
- Zhao, Y.R. Social Work Methods in the Social Support Network Construction for the Elderly—Taking the Practice of F Community Service Center in SHENZHEN as the Study Case; Suzhou University: Suzhou, China, 2014. [Google Scholar]
- Li, J.L.; Li, J.J.; Jin, R.R.; Zhang, J.; Su, X.W.; Ma, S.; Deng, G.J.; Shen, Z.Z.; Bian, F.; Jiang, Y. Studying the difficulty degree of related activities in communities of the national demonstration areas for comprehensive prevention and control of non-communicable diseases. Chin. J. Prev. Control Chronic Dis. 2018, 26, 283–286. [Google Scholar]
- Wang, J.; Li, N.X. The Influence of the elderly home care in community on the management of chronic diseases in the elderly. J. Prev. Med. Inf. 2017, 33, 1174–1177. [Google Scholar]
- Li, L.Q. Analysis on the current situation of Dong zhangmeng rural health library. Chin. J. Clin. Ration Drug Use 2011, 4, 164–165. [Google Scholar]
- Deng, Q.; Liu, W. Physical exercise, social interaction, access to care, and community service: Mediators in the relationship between socioeconomic status and health among older patients with diabetes. Front. Public Health 2020, 8, 589742. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Follow-up to the Political Declaration of the Third High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases. Available online: https://apps.who.int/iris/handle/10665/328411 (accessed on 23 October 2019).

| Characteristics | Quantitative Indicators | Definition of Indicators |
|---|---|---|
| Comprehensiveness | RECR (%) | The proportion of the number of regulatory elements covered in a city’s chronic disease health policy document collection to the 25 required elements |
| DPCR (%) | The proportion of the number of departments with clear and measurable responsibilities to the 22 departments that should be included in PCCDs | |
| Authority | RMAR (%) | The proportion of the number of authority of government branches and regulatory mechanism document sets to the total required |
| Implementation | AMCR (%) | The proportion of the number of departments with clearly defined monitoring agencies and accountabilities to the 22 departments that should be included in PCCDs |
| Indicators | Mean Value/Median Value | SD/IQR |
|---|---|---|
| SORM (%) | 9.70 | 3.67 |
| RECR (%) | 37.84 | 10.32 |
| DPCR (%) | 4.92 | 4.29 |
| RMAR (%) | 23.55 | 6.91 |
| AMCR (%) 1 | 0.55 | (0, 1.85) |
| Community service | ||
| CRCHC (%) | 6.72 | 6.20 |
| CRCSI (%) | 58.46 | 54.00 |
| Economic and aging level | ||
| GDP per capita (thousand yuan) | 54.61 | 24.00 |
| Proportion of population over 65 years of age (%) | 10.35 | 1.70 |
| Variables | Category | Mean (Median)/n | SD (IQR)/% |
|---|---|---|---|
| NCDs | 0 | 4567 | 27.36 |
| 1 | 4481 | 26.84 | |
| 2 | 3379 | 20.24 | |
| 3 | 2023 | 12.12 | |
| 4 | 1162 | 6.96 | |
| ≥5 | 1081 | 6.48 | |
| Control variables | |||
| Age (years) | 61 | 10.01 | |
| Sex | Male = 1 | 8037 | 48.15 |
| Female = 2 | 8656 | 51.85 | |
| Registered residence | Town = 1 | 3547 | 21.25 |
| Rural = 0 | 13,146 | 78.75 | |
| Marital status | Married = 1 | 13,349 | 79.97 |
| Other = 0 | 3344 | 20.03 | |
| Education attainment | Elementary school and below = 1 | 4900 | 29.35 |
| Junior high school = 2 | 5665 | 33.94 | |
| Senior high school and above = 3 | 6128 | 36.71 | |
| Medical insurance | Yes = 1 | 15,234 | 91.26 |
| No = 0 | 1459 | 8.74 | |
| Pension insurance | Yes = 1 | 14,696 | 88.04 |
| No = 0 | 1997 | 11.96 | |
| Drinking | Yes = 1 | 7733 | 46.33 |
| No = 0 | 8960 | 53.68 | |
| Smoking | Yes = 1 | 6912 | 41.41 |
| No = 0 | 9781 | 58.59 | |
| Annual household income per capita(yuan) 1 | 6993.50 | (2470, 17,000) |
| Variables | SORM | CRCHC | CRCSI |
|---|---|---|---|
| CRCHC | 0.331 *** | ||
| CRCSI | 0.473 *** | 0.396 *** | |
| NCD per capita | −0.029 *** | −0.049 *** | −0.059 *** |
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| β | SE | β | SE | |
| SORM | −0.014 *** | 0.002 | −0.010 *** | 0.003 |
| Control variables (individual level) | ||||
| Age | 0.019 *** | 0.001 | 0.019 *** | 0.001 |
| Sex | 0.211 *** | 0.023 | 0.213 *** | 0.023 |
| Registered residence | 0.136 *** | 0.019 | 0.139 *** | (0.019) |
| Marital status | 0.011 | 0.019 | 0.011 | (0.019) |
| Education attainment (Reference group: elementary school and below) | ||||
| Junior high school | 0.082 *** | 0.019 | 0.081 *** | 0.019 |
| Senior high school and above | 0.028 | 0.022 | 0.031 | 0.022 |
| Log Annual household income per capita | −0.016 *** | 0.004 | −0.015 *** | 0.005 |
| Medical insurance | 0.139 *** | 0.028 | 0.136 *** | 0.028 |
| Pension insurance | 0.049 * | 0.025 | 0.045 * | 0.025 |
| Drinking | 0.037 ** | 0.017 | 0.028 * | 0.017 |
| Smoking | 0.057 *** | 0.021 | 0.065 *** | 0.021 |
| Control variables (provincial level) | ||||
| Log GDP per capita | −0.094 *** | 0.026 | ||
| Proportion of population over 65 years of age | 0.028 *** | 0.005 | ||
| alpha 95% CI | (0.270, 0.311) | (0.267, 0.308) | ||
| Model | Path | β | SE | 95% CI | Promotion Mediated |
|---|---|---|---|---|---|
| Total effect | −0.014 *** | 0.004 | −0.022, −0.006 | ||
| A: CRCHC | Direct effect | −0.012 *** | 0.004 | −0.021, −0.004 | 11.31% |
| Indirect effect | −0.002 *** | 0.001 | −0.003, −0.001 | ||
| B: CRCSI | Direct effect | −0.008 * | 0.004 | −0.016, 0.001 | 45.42% |
| Indirect effect | −0.006 *** | 0.001 | −0.008, −0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huangfu, H.; Yu, Q.; Shi, P.; Shen, Q.; Zhang, Z.; Chen, Z.; Pu, C.; Xu, L.; Hu, Z.; Ma, A.; et al. The Impacts of Regional Regulatory Policies on the Prevention and Control of Chronic Diseases in China: A Mediation Analysis. Healthcare 2021, 9, 1058. https://doi.org/10.3390/healthcare9081058
Huangfu H, Yu Q, Shi P, Shen Q, Zhang Z, Chen Z, Pu C, Xu L, Hu Z, Ma A, et al. The Impacts of Regional Regulatory Policies on the Prevention and Control of Chronic Diseases in China: A Mediation Analysis. Healthcare. 2021; 9(8):1058. https://doi.org/10.3390/healthcare9081058
Chicago/Turabian StyleHuangfu, Huihui, Qinwen Yu, Peiwu Shi, Qunhong Shen, Zhaoyang Zhang, Zheng Chen, Chuan Pu, Lingzhong Xu, Zhi Hu, Anning Ma, and et al. 2021. "The Impacts of Regional Regulatory Policies on the Prevention and Control of Chronic Diseases in China: A Mediation Analysis" Healthcare 9, no. 8: 1058. https://doi.org/10.3390/healthcare9081058