
Incorrect Facemask-Wearing Detection Using Convolutional Neural Networks with Transfer Learning


Abstract
:1. Introduction
1.1. Motivation
1.2. The Aim of the Study
1.3. Related Work
2. Materials and Methods
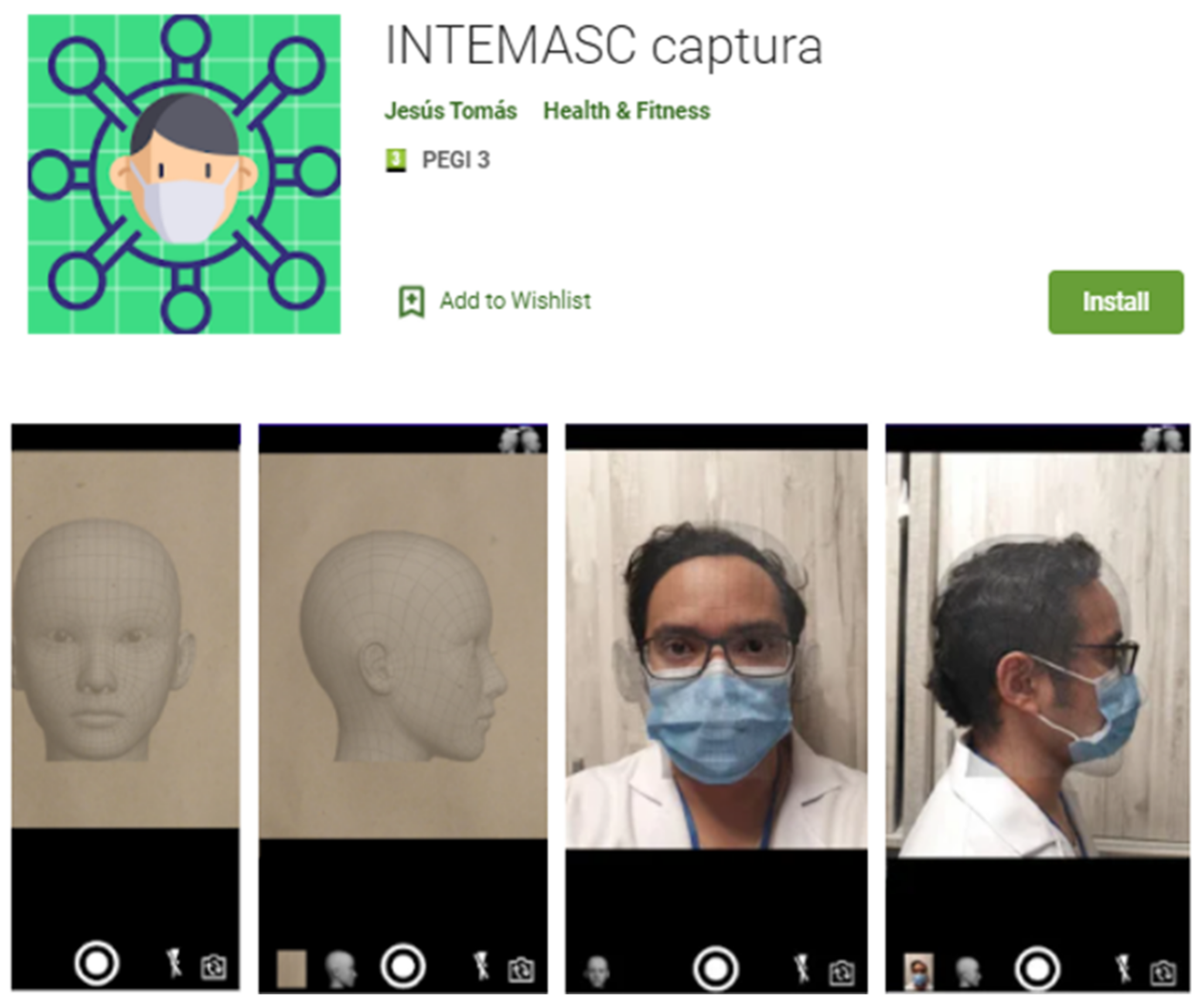
2.1. Obtaining the Data Set
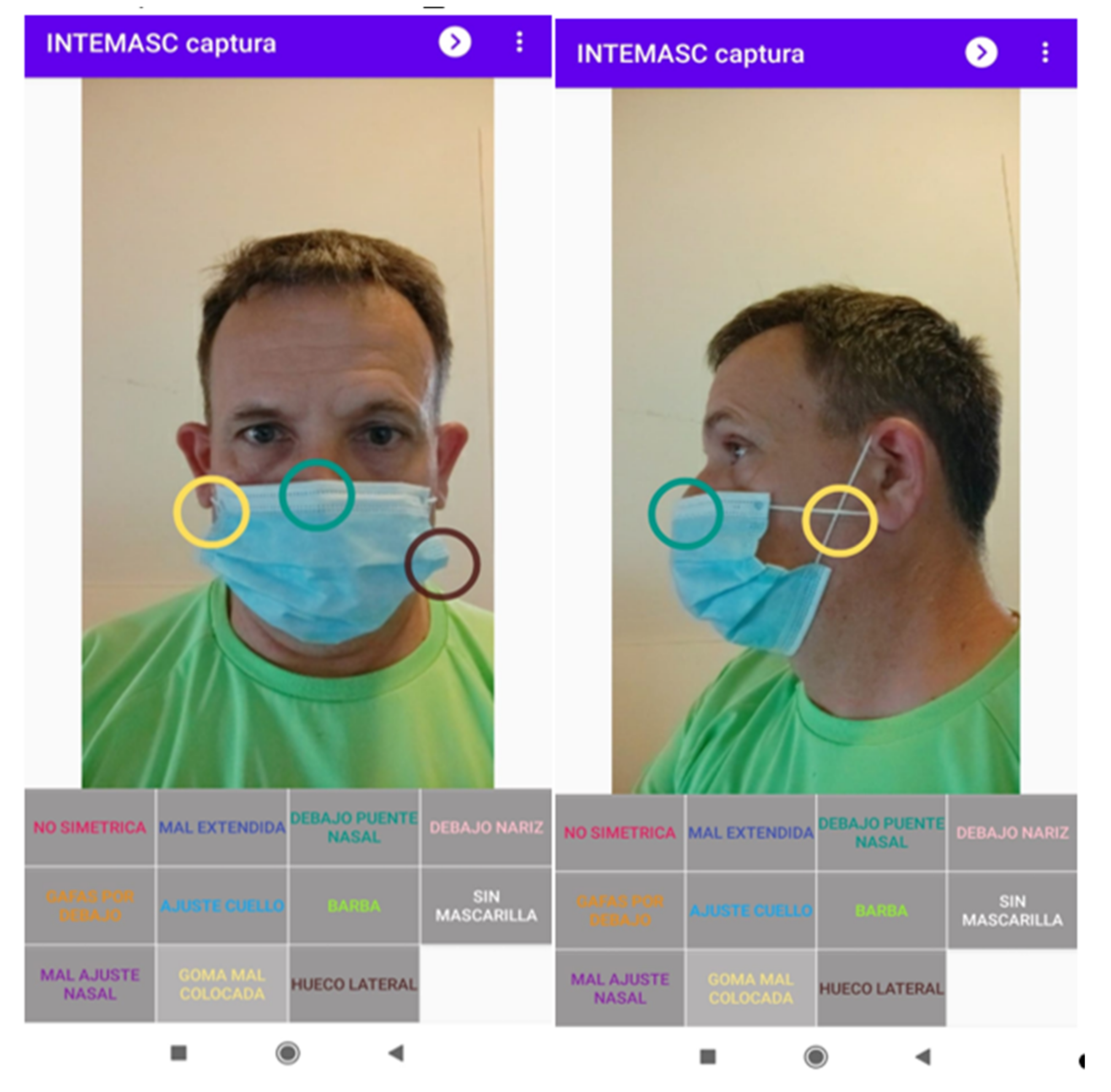
2.2. Labeling
2.3. Facial Detection and Cropping
2.4. Classification
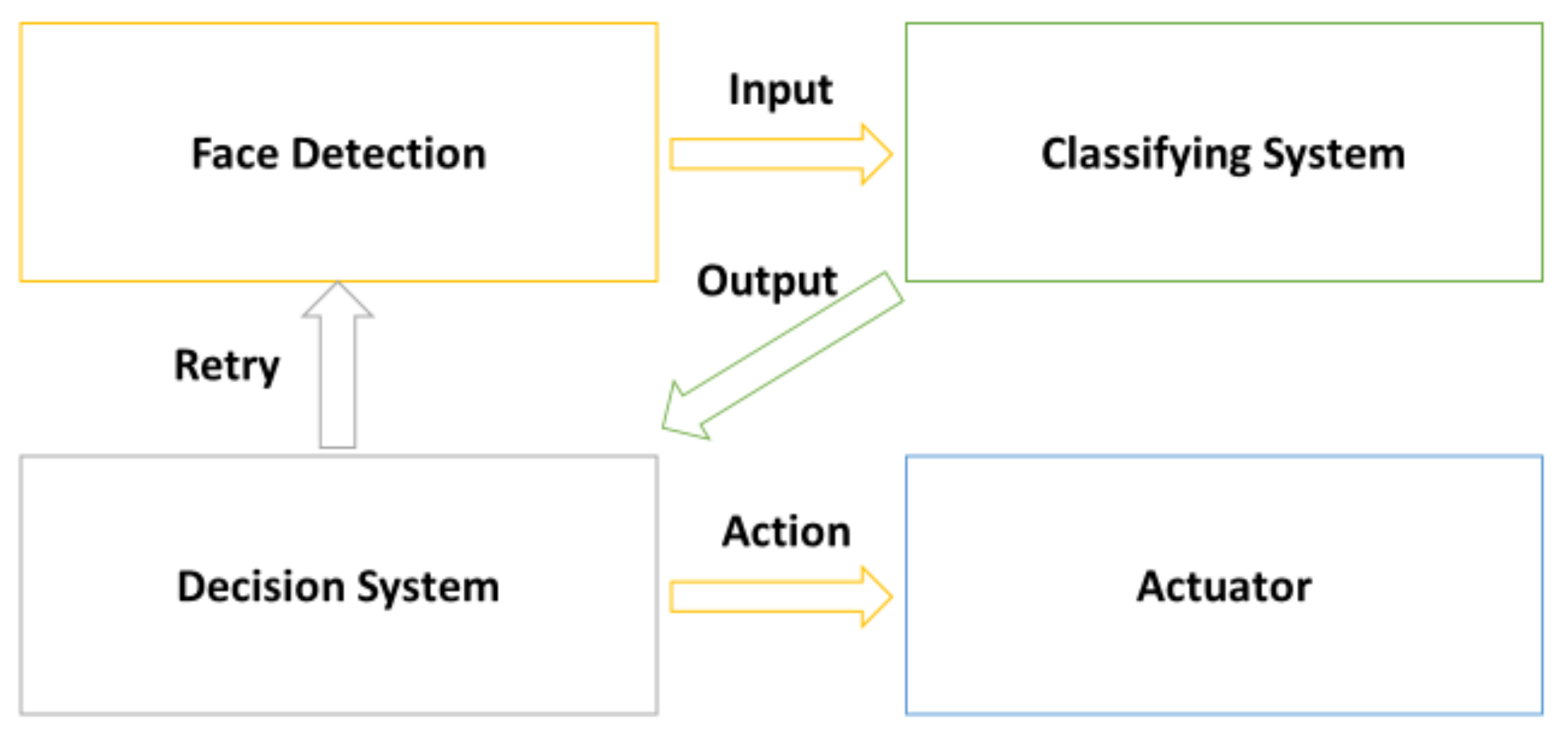
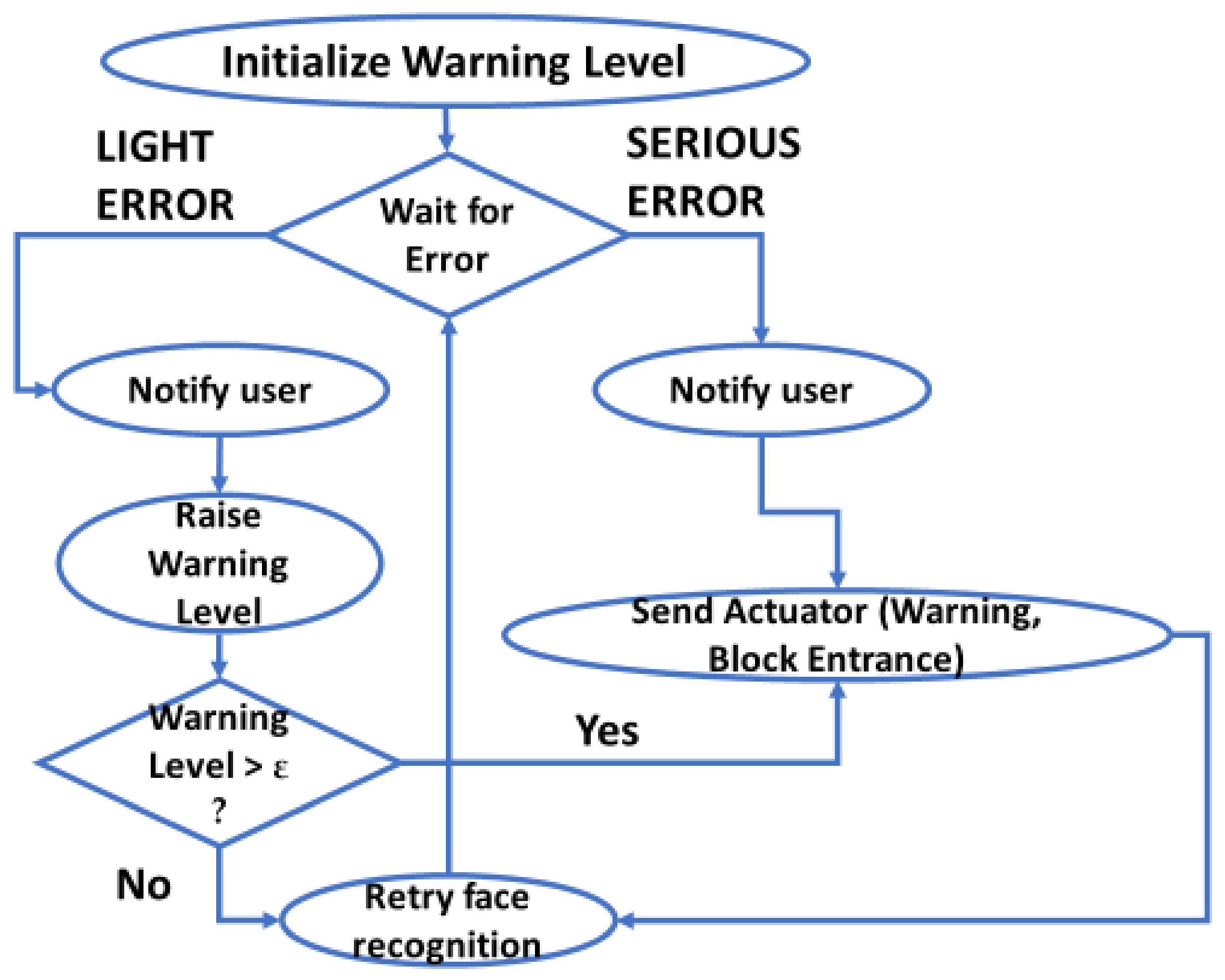
2.5. Decision System
2.6. System Validation
3. Results
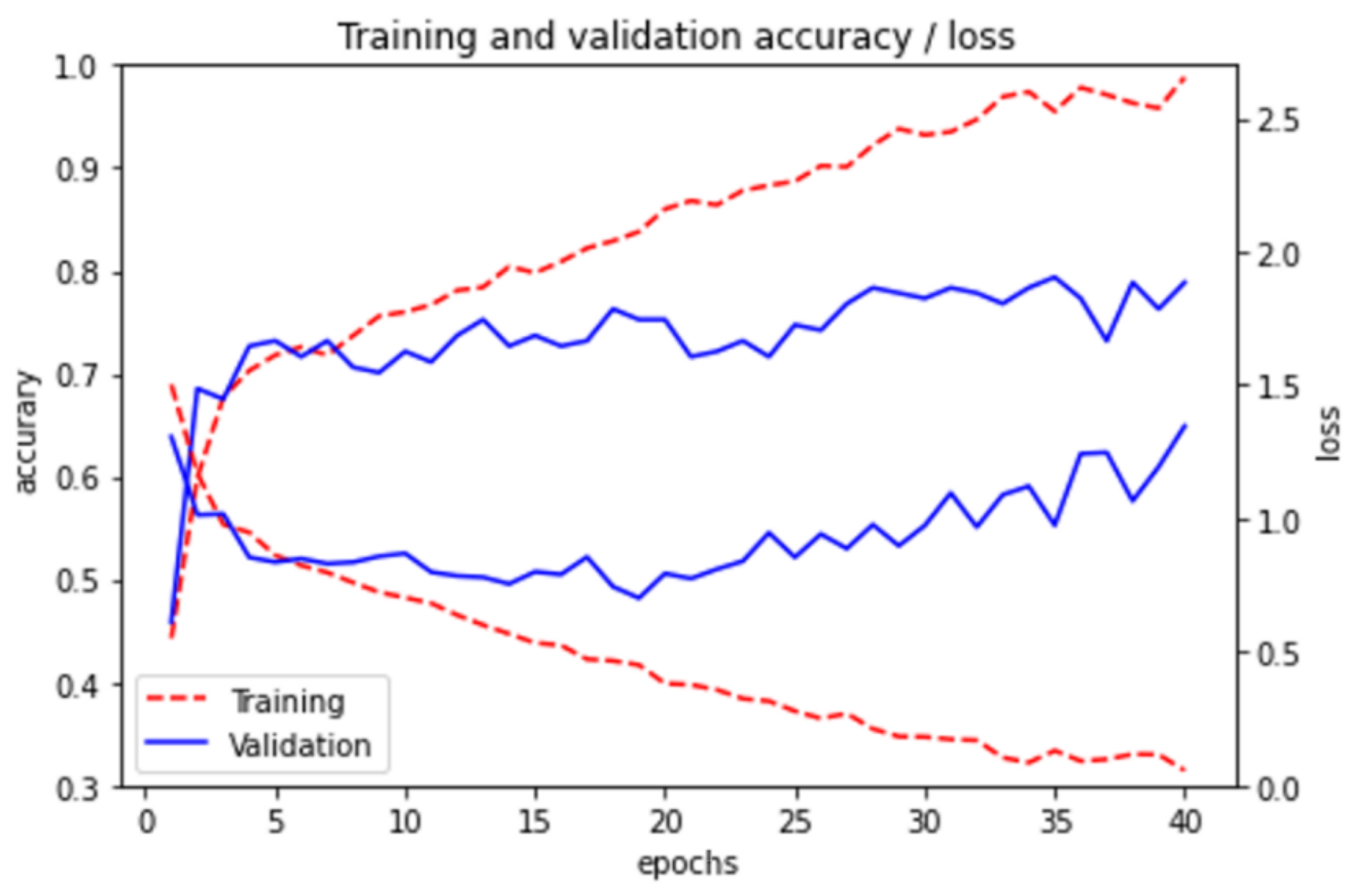
3.1. Convolutional Neural Networks
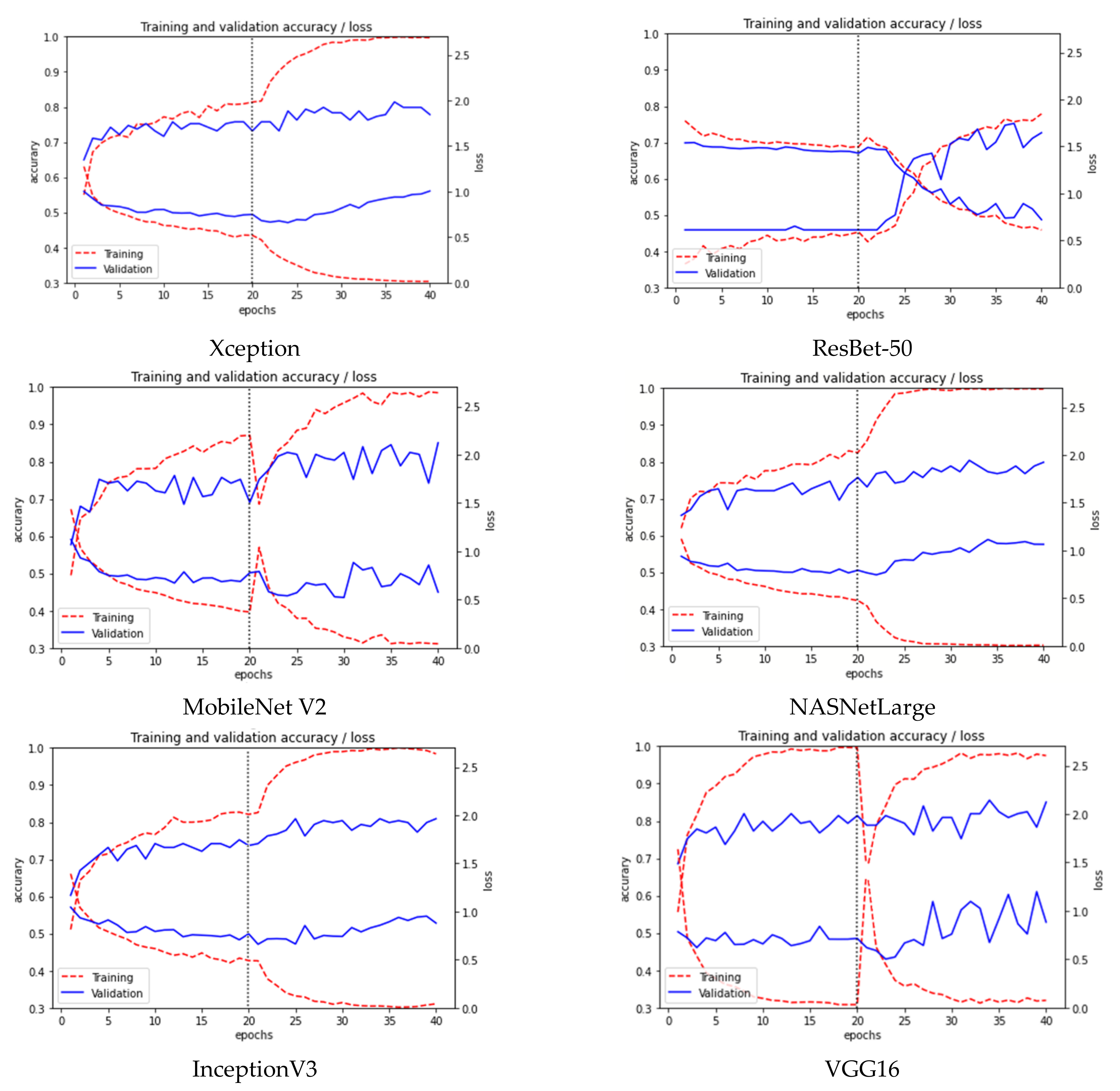
3.2. Transfer Learning
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Code Availability
References
- Nishiura, H.; Jung, S.M.; Linton, N.M.; Kinoshita, R.; Yang, Y.; Hayashi, K.; Kobayashi, T.; Yuan, B.; Akhmetzhanov, A.R. The extent of transmission of novel coronavirus in Wuhan, China, 2020. J. Clin. Med. 2020, 9, 330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, S.F.; Ho, Y.C. SARS-CoV-2: A storm is raging. J. Clin. Investig. 2020, 130, 2202–2205. [Google Scholar] [CrossRef]
- Dawson, P.; Rabold, E.M.; Laws, R.L.; Conners, E.E.; Gharpure, R.; Yin, S.; Buono, S.A.; Dasu, T.; Bhattacharyya, S.; Westergaard, R.P.; et al. Loss of taste and smell as distinguishing symptoms of coronavirus disease 2019. Clin. Infect. Dis. 2021, 72, 682–685. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; McKyer, E.L.J.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000Research 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.T.; Butler, J.C. Effectiveness of mask wearing to control community spread of SARS-CoV-2. JAMA 2021, 325, 998–999. [Google Scholar] [CrossRef]
- Wang, J.; Pan, L.; Tang, S.; Ji, J.S.; Shi, X. Mask use during COVID-19: A risk adjusted strategy. Environ. Pollut. 2020, 266, 115099. [Google Scholar] [CrossRef]
- Joo, H.; Miller, G.F.; Sunshine, G.; Gakh, M.; Pike, J.; Havers, F.P.; Kim, L.; Weber, R.; Dugmeoglu, S.; Waston, C.; et al. Decline in COVID-19 hospitalization growth rates associated with statewide mask mandates—10 states, March–October 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 212. [Google Scholar] [CrossRef]
- Li, T.; Liu, Y.; Li, M.; Qian, X.; Dai, S.Y. Mask or no mask for COVID-19: A public health and market study. PLoS ONE 2020, 15, e0237691. [Google Scholar] [CrossRef]
- Leung, N.H.; Chu, D.K.; Shiu, E.Y.; Chan, K.H.; McDevitt, J.J.; Hau, B.J.; Yen, H.-L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food & Administration (FDA). N95 Respiradores Y Mascarillas Quirúrgicas (Mascarillas). Available online: https://www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-and-surgical-masks-face-masks (accessed on 11 March 2020).
- Centers for Disease Control and Prevention. CDC 24/7. Frequently Asked Questions about Personal Protective Equipment. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/respirator-use-faq.html (accessed on 14 August 2021).
- SANDETEL Junta de Andalucia. Estado del Arte: E-Salud & E-Inclusión Estudio de Las Tecnologías de la Información y la Comunicación Aplicadas a la Salud y a la Inclusión; Dandatel: Seville, Spain, 2011. [Google Scholar]
- Aiello, A.E.; Perez, V.; Coulborn, R.M.; Davis, B.M.; Uddin, M.; Monto, A.S. Facemasks, Hand Hygiene, and Influenza among Young Adults: A Randomized Intervention Trial. PLoS ONE 2012, 7, e29744. [Google Scholar] [CrossRef]
- Chung, Y.; Chou, C.A.; Li, C.Y. Central Attention and a Dual Path Convolutional Neural Network in Real-World Tree Species Recognition. Int. J. Environ. Res. Public Health 2021, 18, 961. [Google Scholar] [CrossRef]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Nieto-Rodríguez, A.; Mucientes, M.; Brea, V.M. System for medical mask detection in the operating room through facial attributes. In Proceedings of the Iberian Conference on Pattern Recognition and Image Analysis, Santiago de Compostela, Spain, 17–19 July 2015; Springer: Cham, Switzerland, 2015; pp. 138–145. [Google Scholar]
- Chen, Y.; Hu, M.; Hua, C.; Zhai, G.; Zhang, J.; Li, Q.; Yang, S.X. Face mask assistant: Detection of face mask service stage based on mobile phone. IEEE Sens. J. 2021, 21, 11084–11093. [Google Scholar] [CrossRef]
- Nagrath, P.; Jain, R.; Madan, A.; Arora, R.; Kataria, P.; Hemanth, J. SSDMNV2: A real time DNN-based face mask detection system using single shot multibox detector and MobileNetV2. Sustain. Cities Soc. 2021, 66, 102692. [Google Scholar] [CrossRef]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv Prepr. 2017, arXiv:1704.04861. [Google Scholar]
- Mata, B.U. Face Mask Detection Using Convolutional Neural Network. J. Nat. Remedies 2021, 21, 14–19. [Google Scholar]
- Jauhari, A.; Anamisa, D.R.; Negara, Y.D.P. Detection system of facial patterns with masks in new normal based on the Viola Jones method. J. Phys. Conf. Ser. 2021, 1836, 012035. [Google Scholar] [CrossRef]
- Sen, S.; Sawant, K. Face mask detection for covid_19 pandemic using pytorch in deep learning. In IOP Conference Series: Materials Science and Engineering; IOP Publishing: Bristol, UK, 2021; Volume 1070, p. 012061. [Google Scholar]
- Balaji, S.; Balamurugan, B.; Kumar, T.A.; Rajmohan, R.; Kumar, P.P. A brief Survey on AI Based Face Mask Detection System for Public Places. Ir. Interdiscip. J. Sci. Res. IIJSR 2021, 5, 108–117. [Google Scholar]
- Kurlekar, M.S. Face Mask Detection System Using Deep Learning. Turk. J. Comput. Math. Educ. Turcomat 2021, 12, 1327–1332. [Google Scholar]
- Sakshi, S.; Gupta, A.K.; Yadav, S.S.; Kumar, U. Face Mask Detection System using CNN. In Proceedings of the 2021 IEEE International Conference on Advance Computing and Innovative Technologies in Engineering (ICACITE), Greater Noida, India, 4–5 March 2021; pp. 212–216. [Google Scholar]
- Cheng, G.; Li, S.; Zhang, Y.; Zhou, R. A Mask Detection System Based on Yolov3-Tiny. Front. Soc. Sci. Technol. 2020, 2, 33–41. [Google Scholar] [CrossRef]
- Loey, M.; Manogaran, G.; Taha, M.H.N.; Khalifa, N.E.M. A hybrid deep transfer learning model with machine learning methods for face mask detection in the era of the COVID-19 pandemic. Measurement 2021, 167, 108288. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Rudraraju, S.R.; Suryadevara, N.K.; Negi, A. Face Mask Detection at the Fog Computing Gateway. In Proceedings of the 2020 IEEE 15th Conference on Computer Science and Information Systems (FedCSIS), Sofia, Bulgaria, 6–9 September 2020; pp. 521–524. [Google Scholar]
- Wang, B.; Zhao, Y.; Chen, C.P. Hybrid Transfer Learning and Broad Learning System for Wearing Mask Detection in the COVID-19 Era. IEEE Trans. Instrum. Meas. 2021, 70, 1–12. [Google Scholar]
- Hussain, S.; Yu, Y.; Ayoub, M.; Khan, A.; Rehman, R.; Wahid, J.A.; Hou, W. IoT and Deep Learning Based Approach for Rapid Screening and Face Mask Detection for Infection Spread Control of COVID-19. Appl. Sci. 2021, 11, 3495. [Google Scholar] [CrossRef]
- Qin, B.; Li, D. Identifying Facemask-Wearing Condition Using Image Super-Resolution with Classification Network to Prevent COVID-19. Sensors 2020, 20, 5236. [Google Scholar] [CrossRef]
- Cabani, A.; Hammoudi, K.; Benhabiles, H.; Melkemi, M. MaskedFace-Net—A dataset of correctly/incorrectly masked face images in the context of COVID-19. Smart Health 2021, 19, 100144, ISSN 2352-6483. [Google Scholar] [CrossRef] [PubMed]
- “Intemasc Captura” Application. Available online: https://play.google.com/store/apps/details?id=es.upv.mastermoviles.intemasc.captura (accessed on 13 July 2021).
- Media Dissemination. Available online: http://mmoviles.upv.es/intemasc/stiker_difusion.mp4 (accessed on 13 July 2021).
- Viola, P.; Jones, M. Rapid object detection using a boosted cascade of simple features. In Proceedings of the 2001 IEEE Computer Society Conference on Computer Vision and Pattern Recognition. CVPR 2001, Kauai, HI, USA, 8–14 December 2001; pp. 511–518. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops (CVPRW), Honolulu, HI, USA, 21–26 July 2017; pp. 1800–1807. [Google Scholar]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- “Mask Detect” Application. Available online: https://play.google.com/store/apps/details?id=es.upv.mastermoviles.intemasc.rec (accessed on 14 August 2021).
- Code Used in the Present Work. Available online: https://github.com/jesus-tomas-girones/Mask_Detect (accessed on 13 July 2021).
- ImageNet Task. Available online: https://keras.io/api/applications (accessed on 13 July 2021).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Author [ref] | Date | Type of Detection | Face Detector | Classification Model | Software Library | Best Accuracy |
|---|---|---|---|---|---|---|
| Nagrath [18] | March 2021 | mask/ no mask | Single shot multibox | MobileNetV2 | TensorFlow, OpenCV | 92.64% |
| Mata [20] | April 2021 | mask/ no mask | Image Data Generator | CNN | TensorFlow, OpenCV | 60% |
| Jauhari [21] | March 2021 | mask/ no mask | Cascade Viola Jones | AdaBoost | Python | 90.9% |
| Sen [22] | February 2021 | mask/ no mask | - | MobileNetV2 | PyTorch, OpenCV | 79.2% |
| Balaji [23] | 2021 | mask/ no mask | Viola-Jones detector | VGG-16 CNN | TensorFlow, OpenCV | 96% |
| Kurlekar [24] | April 2021 | mask/ no mask | - | CNN | TensorFlow, OpenCV, Caffe | - |
| Sakshi [25] | March 2021 | mask/ no mask | - | MobileNetV2 | TensorFlow, Keras | 99% |
| Cheng [26] | 2020 | mask/ no mask | YOLO v3 -tiny | CNN + SVM | - | - |
| Loey [27] | January 2021 | mask/ no mask | YOLO v3 | Resnet50 + SVM | - | 99.5% |
| Rudraraju [29] | September 2020 | mask/ no mask/ nose out | Haar cascade classifier | MobileNet | OpenCV, Keras | 90% |
| Wang [30] | January 2021 | mask/ no mask/ nose out | Fast RCNN | InceptionV2 | OpenCV, Matlab | 91.1% |
| Hussain [31] | April 2021 | mask/ no mask/ nose out | YOLO v3 | VGG-16, MobileNetV2, InceptionV3, ResNet50 | Keras | 99.8% |
| Qin [32] | September 2020 | mask/ no mask/ nose out | Multitask Cascaded CNN | SRCNet | Matlab | 98.7% |
| Front Image | Side Image | |||||
|---|---|---|---|---|---|---|
| 1st Error | 2nd Error | 3rd Error | 1st Error | 2nd Error | 3rd Error | |
| Correct | 518 | 0 | 0 | 476 | 0 | 0 |
| without a mask | 350 | 0 | 0 | 328 | 0 | 0 |
| adjusted below the bridge of the nose | 284 | 74 | 12 | 261 | 67 | 12 |
| mask incorrectly extended | 247 | 192 | 58 | 210 | 104 | 21 |
| exposed nose | 245 | 1 | 0 | 218 | 2 | 0 |
| non-symmetrical placement | 108 | 54 | 15 | 56 | 10 | 0 |
| lateral gap greater than 1 cm | 85 | 21 | 0 | 92 | 24 | 1 |
| glasses placed under the mask | 82 | 10 | 1 | 77 | 9 | 0 |
| incorrectly placed rubber band | 81 | 40 | 6 | 98 | 47 | 6 |
| incorrectly bent in the nasal part | 71 | 11 | 1 | 68 | 8 | 0 |
| neck adjustment greater than 1 cm | 25 | 9 | 2 | 34 | 12 | 2 |
| with a beard, mask is not recommended | 12 | 0 | 0 | 11 | 0 | 0 |
| Model | Size | Parameters | Depth | Accuracy | ImageNet Accuracy |
|---|---|---|---|---|---|
| CNN without data aug | 32 MB | 8.5 M | 15 | 0.763 | - |
| CNN | 32 MB | 8.5 M | 15 | 0.797 | - |
| MobileNet V2 | 14 MB | 3.5 M | 88 | 0.812 | 0.713 |
| Xception | 88 MB | 22.9 M | 126 | 0.802 | 0.790 |
| InceptionV3 | 92 MB | 23.9 M | 159 | 0.819 | 0.779 |
| ResNet-50 | 98 MB | 25.6 M | - | 0.742 | 0.749 |
| NASNetLarge | 343 MB | 88,9 M | - | 0.799 | 0.825 |
| VGG16 | 528 MB | 138.4 M | 23 | 0.834 | 0.713 |
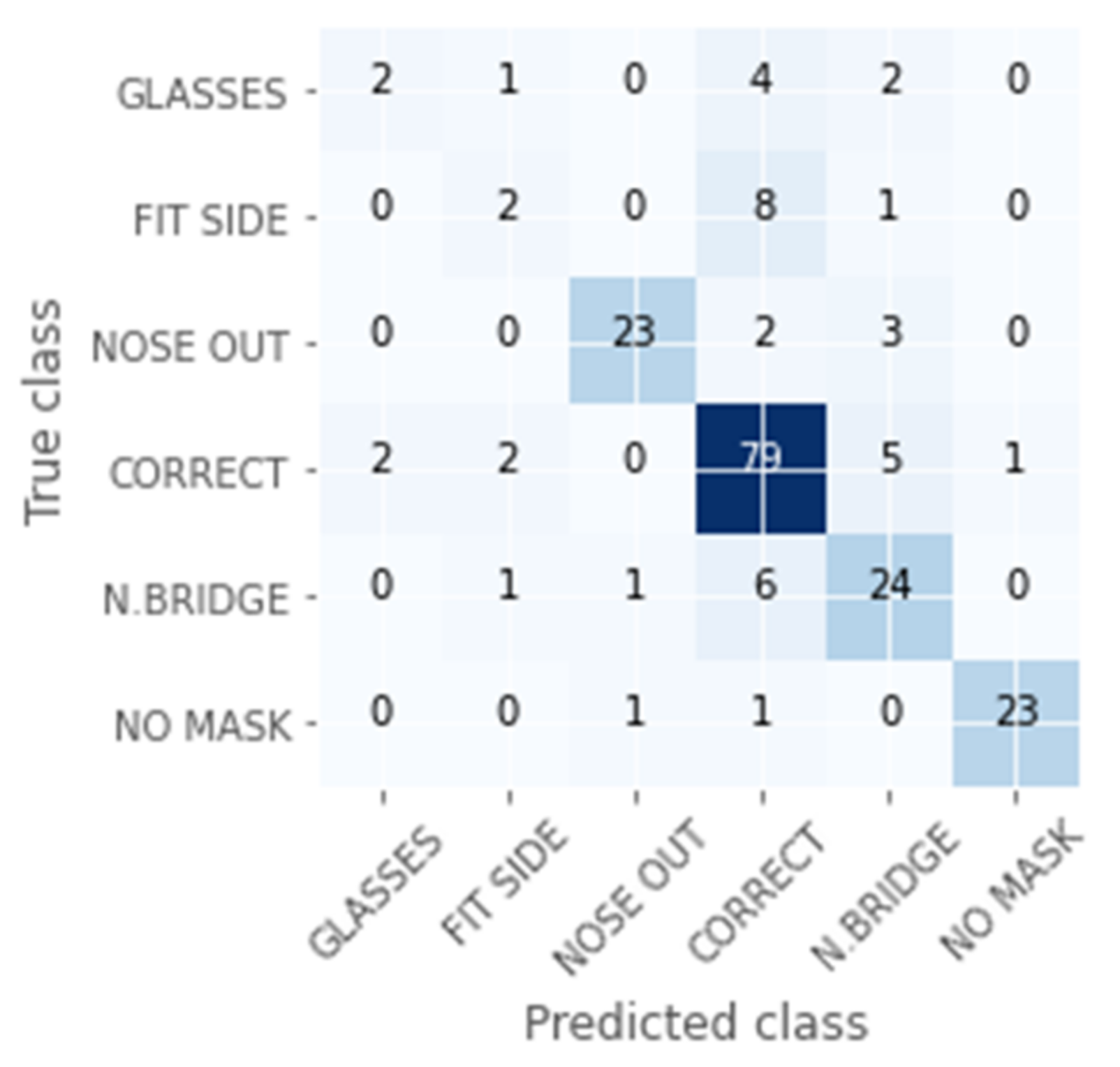
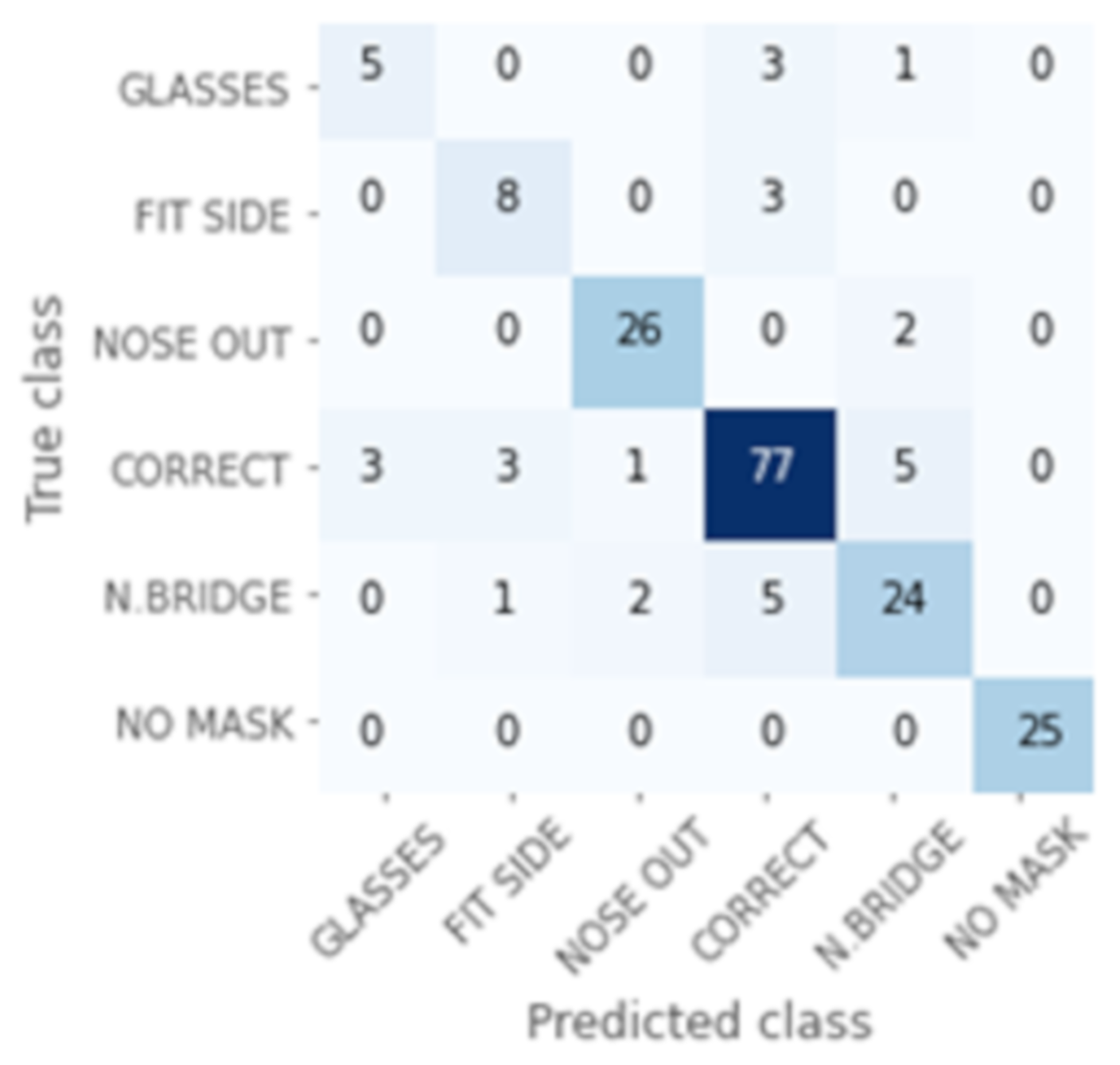
| Precision | Recall | F1-Score | |
|---|---|---|---|
| GLASSES | 0.56 | 0.63 | 0.59 |
| FIT SIDE | 0.73 | 0.67 | 0.70 |
| NOSE OUT | 0.93 | 0.90 | 0.91 |
| CORRECT | 0.87 | 0.88 | 0.87 |
| N.BRIDGE | 0.75 | 0.75 | 0.75 |
| NO MASK | 1.00 | 1.00 | 1.00 |
| total | 0.84 | 0.85 | 0.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomás, J.; Rego, A.; Viciano-Tudela, S.; Lloret, J. Incorrect Facemask-Wearing Detection Using Convolutional Neural Networks with Transfer Learning. Healthcare 2021, 9, 1050. https://doi.org/10.3390/healthcare9081050
Tomás J, Rego A, Viciano-Tudela S, Lloret J. Incorrect Facemask-Wearing Detection Using Convolutional Neural Networks with Transfer Learning. Healthcare. 2021; 9(8):1050. https://doi.org/10.3390/healthcare9081050
Chicago/Turabian StyleTomás, Jesús, Albert Rego, Sandra Viciano-Tudela, and Jaime Lloret. 2021. "Incorrect Facemask-Wearing Detection Using Convolutional Neural Networks with Transfer Learning" Healthcare 9, no. 8: 1050. https://doi.org/10.3390/healthcare9081050