
Characteristics of COVID-19-Related Free Telephone Consultations by Public Health Nurses in Japan: A Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
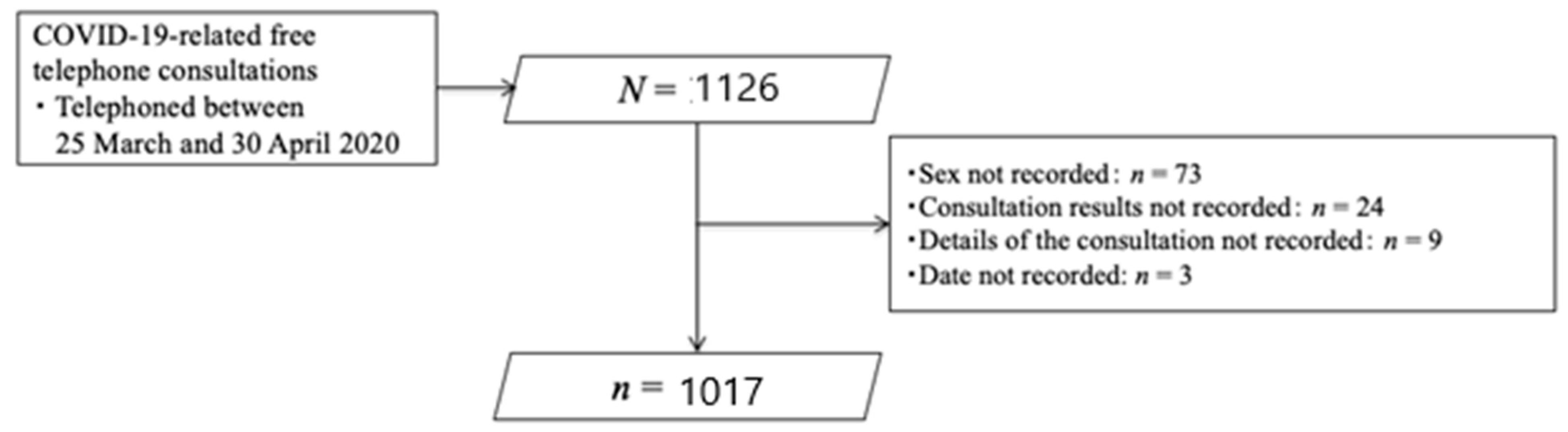
2.1. Study Sample
2.2. Variables on Telephone Consultation Sheets
2.3. Statistical Analysis
2.4. Ethical Statement
3. Results
3.1. Characteristics of COVID-19-Related Free Telephone Consultations
3.2. Characteristics of the Residents Group
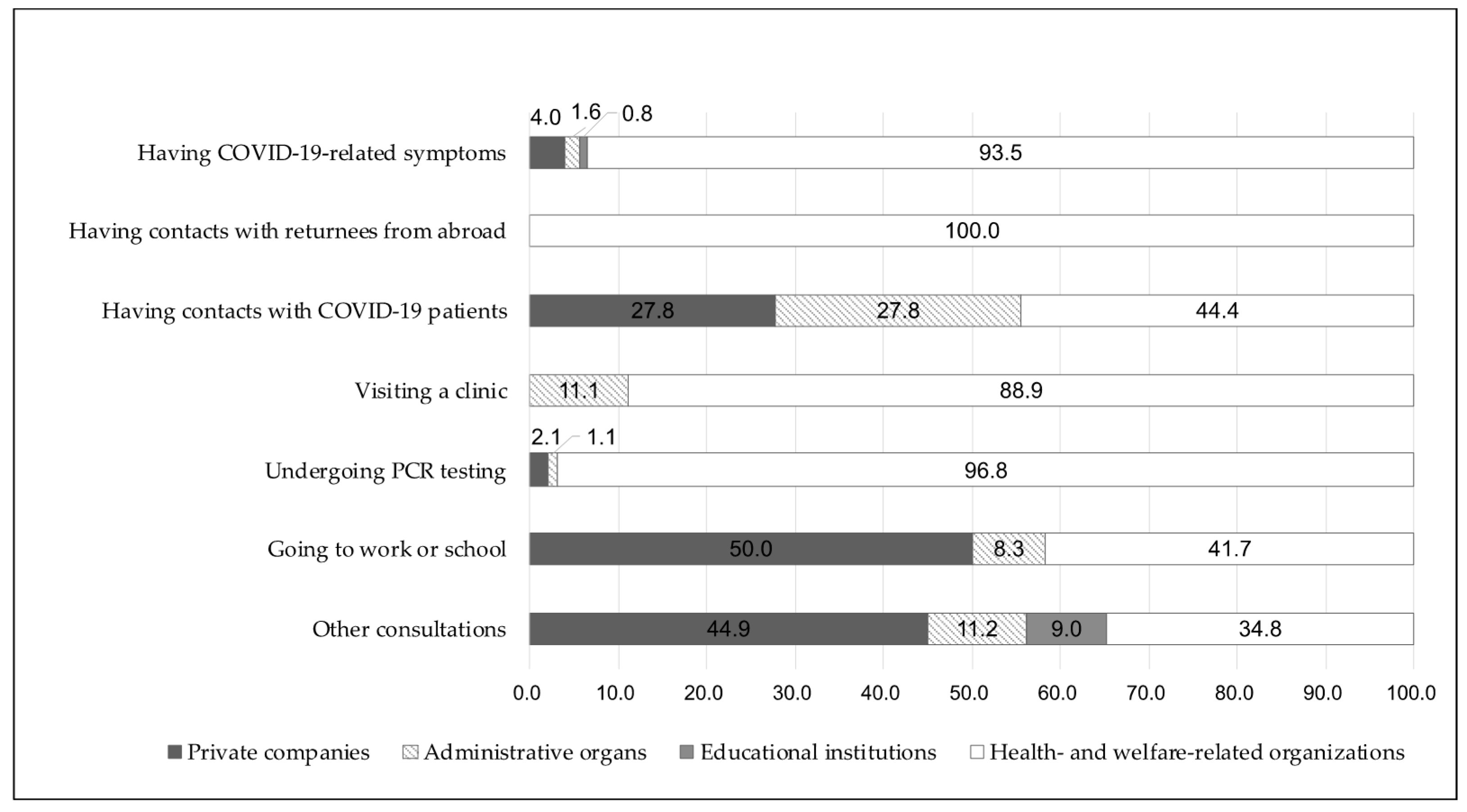
3.3. Reasons for Seeking Consultation by the Type of Organization
3.4. The Patterns of Both “Consultations Provided to Community People” and “Recommendations of the PHNs for Each Consultation”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Looking Back at a Year That Changed the World: WHO’s Response to Covid-19; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Shimizu, K.; Negita, M. Lessons Learned from Japan’s Response to the First Wave of Covid-19: A Content Analysis. Healthcare 2020, 8, 426. [Google Scholar] [CrossRef] [PubMed]
- Japan Cabinet Secretariat. Shingata Corona Virus Kansen Shou Kinkuu Jitai Sengen (Reiwa 3 Nen 4 Gatsu 7 Nichi Hasshutsu). 2020. Available online: https://corona.go.jp/news/pdf/kinkyujitai_sengen_0407.pdf (accessed on 3 March 2021).
- Ministry of Health, Labour, and Welfare. Community Health Act. 1994. Available online: https://elaws.e-gov.go.jp/document?law_unique_id=322AC0000000101_20190401_430AC0000000079 (accessed on 5 March 2021).
- Yoshioka-Maeda, K.; Iwasaki-Motegi, R.; Honda, C. Preventing the Dysfunction of Public Health Centres Responding to Covid-19 by Focusing on Public Health Nurses in Japan. J. Adv. Nurs. 2020, 76, 2215–2216. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Yoshioka-Maeda, K. Developing Sustainable Public Health Care Systems for Responding to Covid-19 in Japan. Public Health Nurs. 2021, 38, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Moguilner, S.; Pandya, S.; Schroeder, S.; et al. Telemedicine as the New Outpatient Clinic Gone Digital: Position Paper from the Pandemic Health System Resilience Program (Reprogram) International Consortium (Part 2). Front. Public Health 2020, 8, 410. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, W.; Gatto, A.; Pansini, V.; Curatola, A.; Capossela, L.; Currò, V.; Chiaretti, A. Telephone Consultation during Coronavirus Outbreak in a Pediatric Emergency Department: Methodological Approach of a Tertiary Care Center in a Covid-19 Hospital Setting. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 11440–11444. [Google Scholar] [PubMed]
- Iyengar, K.; Jain, V.K.; Vaishya, R. Pitfalls in Telemedicine Consultations in the Era of Covid 19 and How to Avoid Them. Diabetes Metab. Syndr. 2020, 14, 797–799. [Google Scholar] [CrossRef] [PubMed]
- Hasani, S.A.; Ghafri, T.A.; Al Lawati, H.; Mohammed, J.; Al Mukhainai, A.; Al Ajmi, F.; Anwar, H. The Use of Telephone Consultation in Primary Health Care during Covid-19 Pandemic, Oman: Perceptions from Physicians. J. Prim. Care Community Health 2020, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Koh, G.C.H.; Car, J. Covid-19: A Remote Assessment in Primary Care. BMJ 2020, 368, m1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour, and Welfare. Shingata Corona Virus Kansenshou Ni Taiou Sita Iryou Teikyou Taisei Ni Tsuite. 2020. Available online: https://www.mhlw.go.jp/content/10900000/000591991.pdf (accessed on 5 April 2021).
- Sumikawa, Y.; Honda, C.; Yoshioka-Maeda, K.; Yamamoto-Mitani, N. The University and Public Health Center Collaboration on the Verge of the COVID-19 Crisis: A Case of University Support via a Community Telephone Hotline in Japan. 2021. Available online: https://www.2020yearofthenurse.org/story/university-public-health-center-collaboration-during-covid-19/ (accessed on 5 May 2021).
- International Council on Archives, & the International Conference of Information Commissioners. Covid-19: The Duty to Document Does Not Cease in a Crisis, It Becomes More Essential. 2020. Available online: https://www.ica.org/en/covid-19-the-duty-to-document-does-not-cease-in-a-crisis-it-becomes-more-essential (accessed on 5 April 2021).
- Statistics of Tokyo. Tokyo Statistical Yearbook. Available online: https://www.toukei.metro.tokyo.lg.jp/juukiy/jy-index.htm (accessed on 1 June 2021).
- Cabinet Office Japan. Annual Report on the Aging Society [Summary] FY2020. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2020/pdf/2020.pdf (accessed on 5 May 2021).
- Isautier, J.M.; Copp, T.; Ayre, J.; Cvejic, E.; Meyerowitz-Katz, G.; Batcup, C.; Bonner, C.; Dodd, R.; Nickel, B.; Pickles, K.; et al. People’s Experiences and Satisfaction with Telehealth during the COVID-19 Pandemic in Australia: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e24531. [Google Scholar] [CrossRef] [PubMed]
- Eberly, L.A.; Kallan, M.J.; Julien, H.M.; Haynes, N.; Khatana, S.A.M.; Nathan, A.S.; Snider, C.; Chokshi, N.P.; Eneanya, N.D.; Takvorian, S.U.; et al. Patient characteristics associated with telemedicine access for primary and specialty ambulatory care during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2031640. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.L.; Zechel, A.; Carter, Y.H.; Abbott, S. Systematic review of recent innovations in service provision to improve access to primary care. Br. J. Gen. Pract. 2004, 54, 374–381. [Google Scholar] [PubMed]
- Abate, B.B.; Kassie, A.M.; Kassaw, M.W.; Aragie, T.G.; Masresha, S.A. Sex difference in coronavirus disease (COVID-19): A systematic review and meta-analysis. BMJ Open 2020, 10, e040129. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19—16 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---16-march-2020 (accessed on 23 July 2021).
- Furuse, Y.; Sando, E.; Tsuchiya, N.; Miyahara, R.; Yasuda, I.; Ko, Y.K.; Saito, M.; Morimoto, K.; Imamura, T.; Shobugawa, Y.; et al. Clusters of Coronavirus Disease in Communities, Japan, January–April 2020. Emerg. Infect. Dis. 2020, 26, 2176–2179. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour, and Welfare. Basic Policy for Countermeasures against SARS-Cov-2 Infection. 25 February 2020. Available online: https://www.mhlw.go.jp/content/10200000/000603610.pdf (accessed on 23 July 2021).
- Shirai, C.; Fujiyama, R.; Uchino, E.; Irie, F.; Takatoriges, T.; Iso, H. Evaluation of the flu call center and medical system data on pandemic (H1N1) 2009 influenza. Comparison of cases in Kobe city and Ibaraki prefecture. J. Public Health 2012, 59, 684–692. [Google Scholar]
- Ministry of Health, Labour, and Welfare. Tsugino Infuluenza Ryuukou Ni Sonaeta Taisei Seibi Ni Tuite. 2020. Available online: https://www.mhlw.go.jp/content/10601000/000670438.pdf (accessed on 15 March 2021).



{kind=link}
{kind=link}
| Variables | Total (N = 1017) N (%) or Mean ± SD (Min–Max) | The Resident Group (n = 799) n (%) or Mean ± SD (Min–Max) | The Organization Group (n = 218) n (%) or Mean ± SD (Min–Max) | p |
|---|---|---|---|---|
| Sex | ||||
| Male | 471 (46.3) | 343 (42.9) | 128 (58.7) | <0.001 * |
| Age (n = 662) | ||||
| <60 years old | 498 (75.2) | 408 (76.7) | 90 (69.2) | 0.077 * |
| ≥60 years | 164 (24.8) | 124 (23.3) | 40 (30.8) | |
| Consultation time | ||||
| 9 a.m. to 11 a.m. | 508 (50.0) | 387 (48.4) | 121 (55.5) | 0.045 * |
| 12 p.m. to 14 p.m. | 261 (25.7) | 219 (27.4) | 42 (19.3) | |
| 15 p.m. to 17 p.m. | 248 (24.4) | 193 (24.2) | 55 (25.2) | |
| Duration of consultation: min (n = 622) | 6.8 ± 4.7 (1–50) | 6.9 ± 4.8 (1–50) | 6.6 ± 4.1 (1–20) | 0.716 § |
| Categories of organizations | ||||
| Private companies | - | - | 47 (21.6) | - |
| Administrative organs | - | - | 14 (6.4) | |
| Educational institutions | - | - | 9 (4.1) | |
| Health- and welfare-related organizations | - | - | 148 (67.9) | |
| Variables | Male (n = 343) n (%) or Mean ± SD (Min–Max) | Female (n = 456) n (%) or Mean ± SD (Min–Max) | p |
|---|---|---|---|
| Age (n = 532) | |||
| <60 years old | 182 (81.6) | 226 (73.1) | 0.023 * |
| ≥60 years old | 41 (18.4) | 83 (26.9) | |
| Consultation time | |||
| 9 a.m. to 11 a.m. | 172 (50.1) | 215 (47.1) | 0.644 * |
| 12 p.m. to 14 p.m. | 93 (27.1) | 126 (27.6) | |
| 15 p.m. to 17 p.m. | 78 (22.7) | 115 (25.2) | |
| Duration of consultation: min | 6.9 ± 95.0 [1–35] | 6.9 ± 94.7 [1–50] | 0.538 § |
| Consultation details: multiple answer | |||
| Having COVID-19-related symptoms | 285 (83.1) | 400 (87.7) | 0.064 * |
| Having contacts with returnees from abroad | 24 (7.0) | 16 (3.5) | 0.025 * |
| Having contacts with COVID-19 patients | 27 (7.9) | 34 (7.5) | 0.827 * |
| Visiting a clinic | 25 (7.3) | 39 (8.6) | 0.515 * |
| Undergoing PCR testing | 38 (11.1) | 54 (11.8) | 0.738 * |
| Going to work or school | 20 (5.8) | 21 (4.6) | 0.437 * |
| Other consultations | 48 (14.0) | 51 (11.2) | 0.233 * |
| Recommendations of PHNs for the consultations: multiple answer | |||
| Recommendation of primary care doctor visit | 224 (65.3) | 316 (69.3) | 0.233 * |
| Recommendations for self-care: adequate rest and hydration | 55 (16.0) | 68 (14.9) | 0.663 * |
| Self-health monitoring | 92 (26.8) | 119 (26.1) | 0.818 * |
| Provision of information on infection prevention measures | 36 (10.5) | 48 (10.5) | 0.989 * |
| Provision of COVID-19 information | 32 (9.3) | 33 (7.2) | 0.284 * |
| Provision of information on clinics and PCR testing | 22 (6.4) | 24 (5.3) | 0.489 * |
| Coordination of clinic visits and PCR testing | 10 (2.9) | 21 (4.6) | 0.221 * |
| Other recommendations | 4 (1.2) | 4 (0.9) | 0.685 * |
| Recommendations of PHNs for Each Consultation | Consultation Details from Community People | ||||||
|---|---|---|---|---|---|---|---|
| Having COVID-19-Related Symptoms (n = 809) | Having Contacts with Returnees from Abroad (n = 42) | Having Contacts with COVID-19 Patients (n = 79) | Visiting a Clinic (n = 73) | Undergoing PCR Testing (n = 187) | Going to Work or School (n = 53) | Other Consultations (n = 188) | |
| Recommendation of primary care doctor visit | 623 (77.0) | 27 (64.3) | 28 (35.4) | 52 (71.2) | 137 (73.3) | 11 (20.8) | 24 (12.8) |
| Recommendations for self-care: adequate rest and hydration | 122 (15.1) | 5 (11.9) | 8 (10.1) | 3 (4.1) | 9 (4.8) | 3 (5.7) | 8 (4.3) |
| Self-health monitoring | 183 (22.6) | 15 (35.7) | 24 (30.4) | 6 (8.2) | 17 (9.1) | 22 (41.5) | 29 (15.4) |
| Provision of information on infection prevention measures | 67 (8.3) | 3 (7.1) | 18 (22.8) | 5 (6.8) | 7 (3.7) | 9 (17.0) | 53 (28.2) |
| Provision of COVID-19-related information | 30 (3.7) | 4 (9.5) | 17 (21.5) | 6 (8.2) | 10 (5.3) | 14 (26.4) | 85 (45.2) |
| Provision of information on clinics and PCR testing | 32 (4.0) | 0 (0.0) | 3 (3.8) | 8 (11.0) | 29 (15.5) | 4 (7.5) | 26 (13.8) |
| Coordination of clinic visits and PCR testing | 119 (14.7) | 2 (4.8) | 10 (12.7) | 7 (9.6) | 91 (48.7) | 1 (1.9) | 4 (2.1) |
| Other recommendations | 8 (1.0) | 0 (0.0) | 0 (0.0) | 1 (1.4) | 2 (1.1) | 0 (0.0) | 16 (8.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumikawa, Y.; Honda, C.; Yoshioka-Maeda, K.; Yamamoto-Mitani, N. Characteristics of COVID-19-Related Free Telephone Consultations by Public Health Nurses in Japan: A Retrospective Study. Healthcare 2021, 9, 1022. https://doi.org/10.3390/healthcare9081022
Sumikawa Y, Honda C, Yoshioka-Maeda K, Yamamoto-Mitani N. Characteristics of COVID-19-Related Free Telephone Consultations by Public Health Nurses in Japan: A Retrospective Study. Healthcare. 2021; 9(8):1022. https://doi.org/10.3390/healthcare9081022
Chicago/Turabian StyleSumikawa, Yuka, Chikako Honda, Kyoko Yoshioka-Maeda, and Noriko Yamamoto-Mitani. 2021. "Characteristics of COVID-19-Related Free Telephone Consultations by Public Health Nurses in Japan: A Retrospective Study" Healthcare 9, no. 8: 1022. https://doi.org/10.3390/healthcare9081022