
Relationship between Oral Bacterial Count and Postoperative Complications among Patients with Cardiovascular Disease Treated by Surgery: A Retrospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
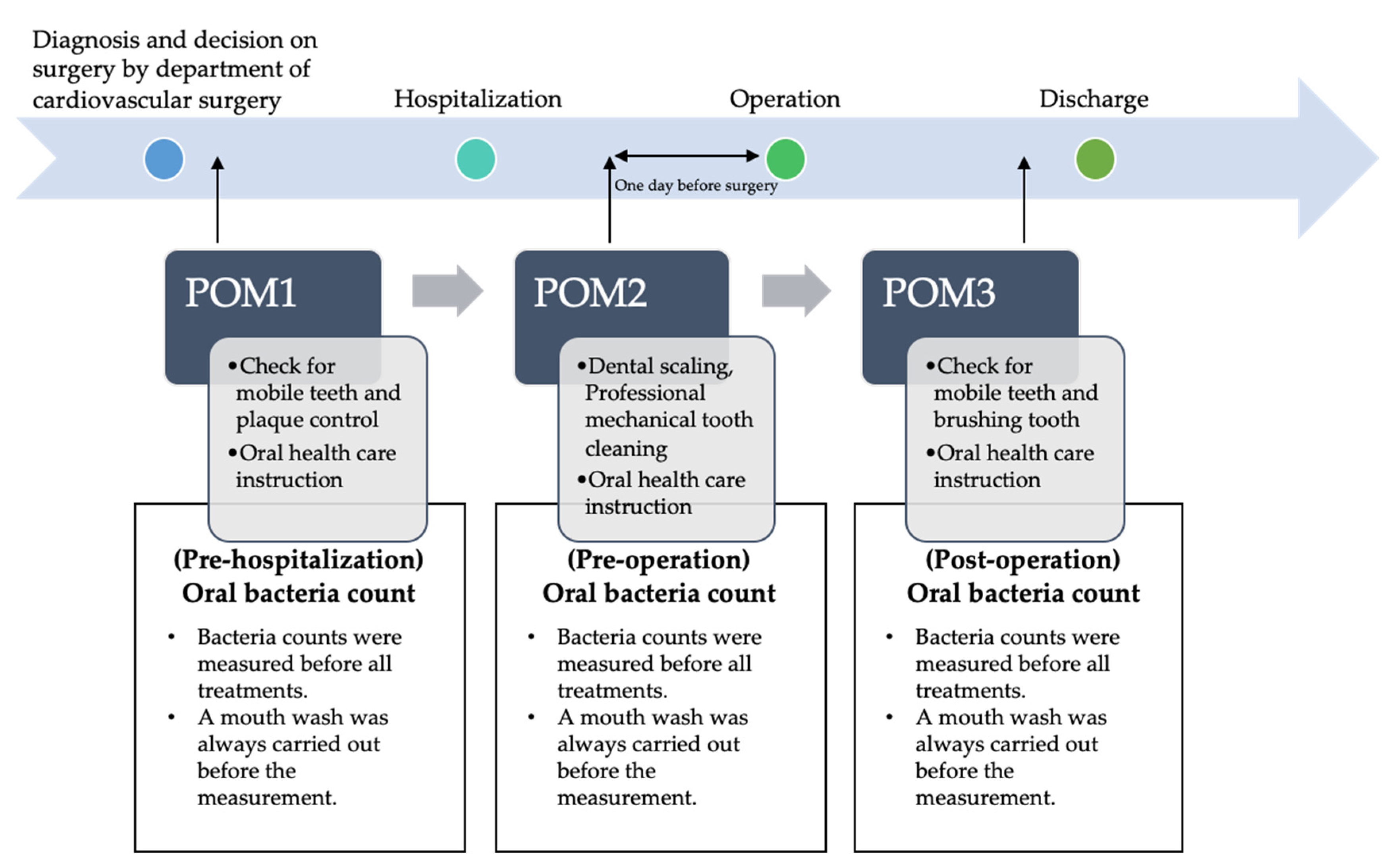
2.1. General Perioperative Oral Management in Kagawa Prefectural Central Hospital
2.2. Recruitment of Research Subjects and Data Collection Methods
2.3. Study Variables
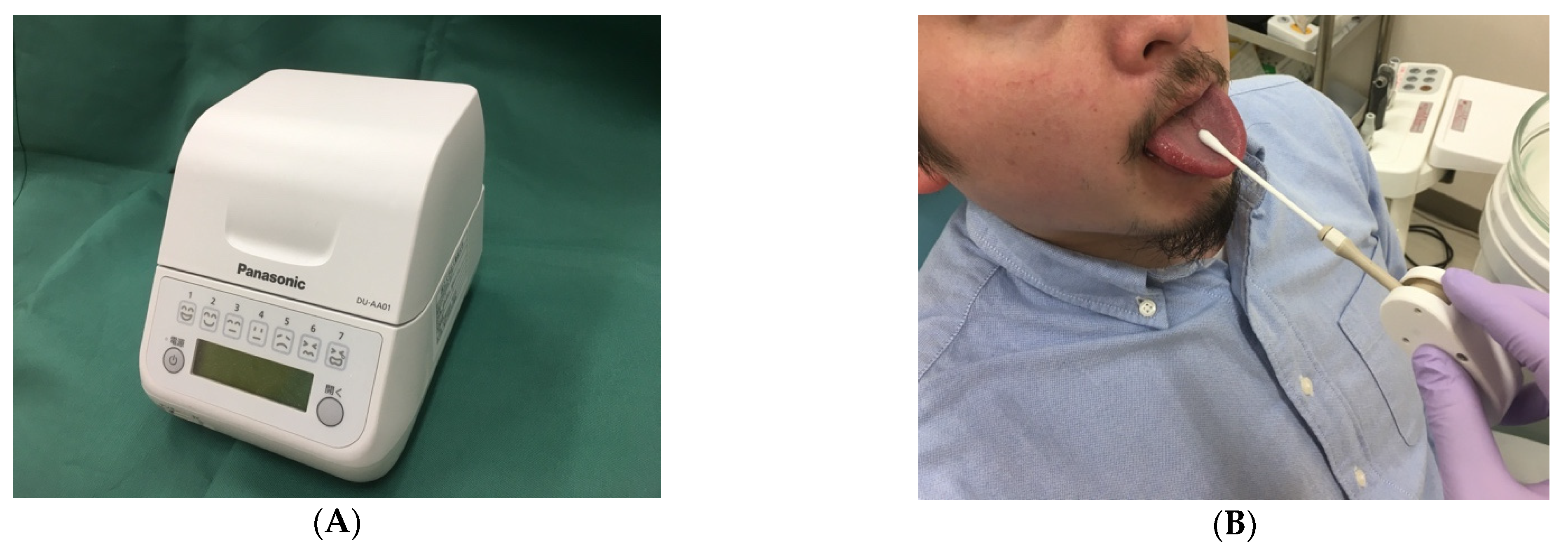
2.4. Oral Bacterial Count
2.5. Study Outcomes
2.6. Statistical Analyses
3. Results
3.1. Patients Characteristic
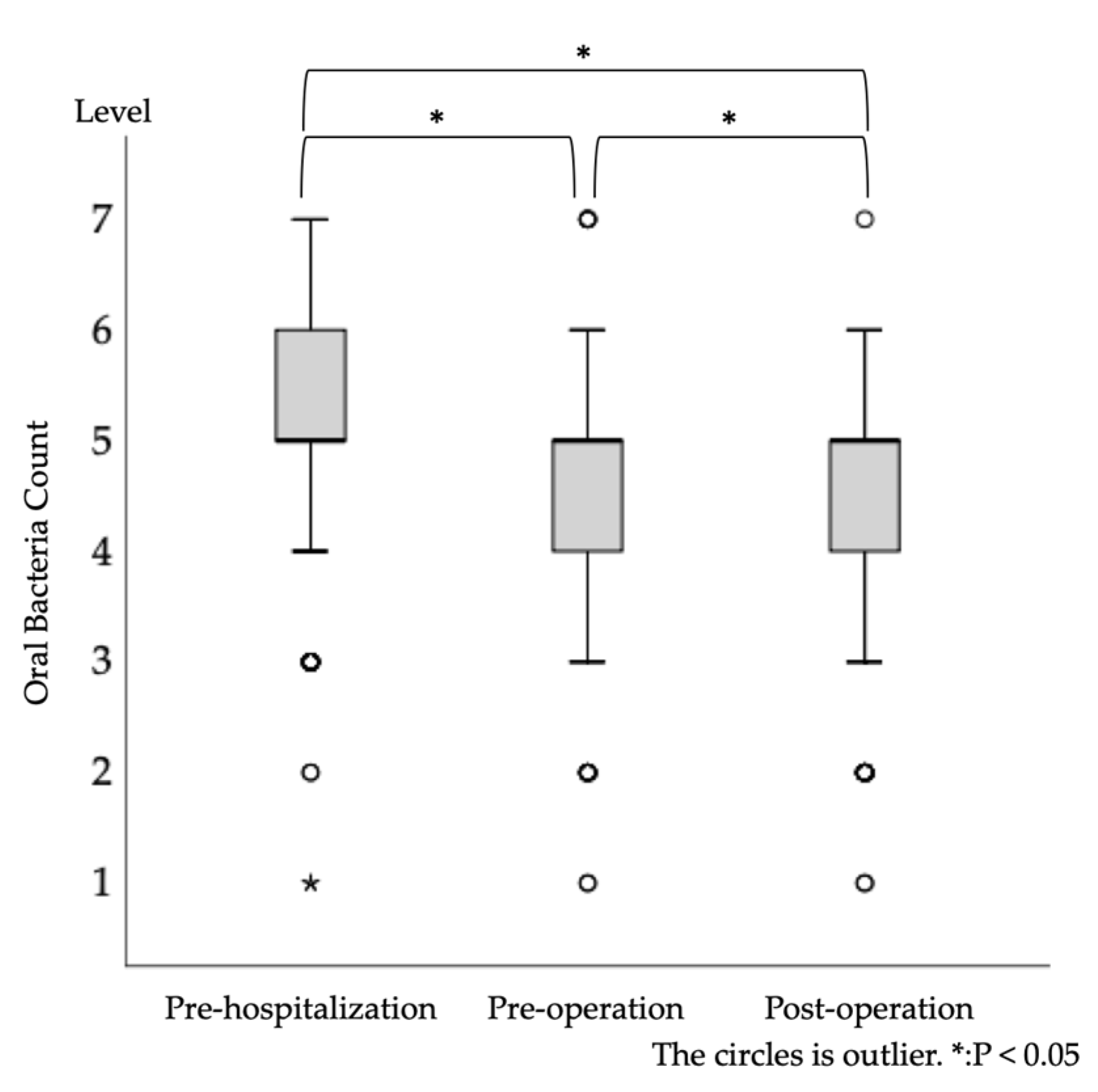
3.2. Longitudinal Change in Oral Bacterial Count
3.3. Number of Patients with Postoperative Complications
3.4. Between-Group Comparison of Baseline Background Factors
3.5. Propensity Score Analysis of the Association between the Development of Postoperative Complications and Oral Bacterial Count
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nakatani, S.; Mitsutake, K.; Hozumi, T.; Yoshikawa, J.; Akiyama, M.; Yoshida, K.; Ishizuka, N.; Nakamura, K.; Taniguchi, Y.; Yoshioka, K.; et al. Current characteristics of infective endocarditis in Japan: An analysis of 848 cases in 2000 and 2001. Circ. J. 2003, 67, 901–905. [Google Scholar] [CrossRef] [Green Version]
- Carinci, F.; Martinelli, M.; Contaldo, M.; Santoro, R.; Pezzetti, F.; Lauritano, D.; Candotto, V.; Mucchi, D.; Palmieri, A.; Tagliabue, A.; et al. Focus on periodontal disease and development of endocarditis. J. Boil. Regul. Homeost. Agents 2018, 32, 143–147. [Google Scholar]
- Nakatani, S.; Ohara, T.; Ashihara, K.; Izumi, C.; Iwanaga, S.; Eishi, K.; Okita, Y.; Daimon, M.; Kimura, T.; Toyoda, K.; et al. JCS 2017 Guideline on Prevention and Treatment of Infective Endocarditis. Circ. J. 2019, 83, 1767–1809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cove, M.E.; Spelman, D.W.; MacLaren, G. Infectious Complications of Cardiac Surgery: A Clinical Review. J. Cardiothorac. Vasc. Anesthesia 2012, 26, 1094–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leishman, S.J.; Do, H.L.; Ford, P.J. Cardiovascular disease and the role of oral bacteria. J. Oral Microbiol. 2010, 2. [Google Scholar] [CrossRef]
- Oliveira, F.A.F.; Forte, C.P.F.; Silva, P.G.D.B.; Lopes, C.B.; Montenegro, R.C.; Ândrea, K.C.R.; Sobrinho, C.R.M.R.; Mota, M.; Sousa, F.B.; Alves, A.P.N.N.; et al. Molecular Analysis of Oral Bacteria in Heart Valve of Patients With Cardiovascular Disease by Real-Time Polymerase Chain Reaction. Medicine 2015, 94, e2067. [Google Scholar] [CrossRef] [PubMed]
- Nobuhara, H.; Yanamoto, S.; Funahara, M.; Matsugu, Y.; Hayashida, S.; Soutome, S.; Kawakita, A.; Ikeda, S.; Itamoto, T.; Umeda, M. Effect of perioperative oral management on the prevention of surgical site infection after colorectal cancer surgery: A multicenter retrospective analysis of 698 patients via analysis of covariance using propensity score. Medicine 2018, 97, e12545. [Google Scholar] [CrossRef]
- Nishi, H.; Takahashi, S.; Ohta, K.; Takamoto, M.; Shigeishi, H.; Go, S.; Obayashi, T.; Yoshioka, Y.; Konishi, M.; Shimizu, Y.; et al. Effects of perioperative oral care on postoperative inflammation following heart valve surgery. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Itohara, C.; Matsuda, Y.; Sukegawa-Takahashi, Y.; Sukegawa, S.; Furuki, Y.; Kanno, T. Relationship between Oral Health Status and Postoperative Fever among Patients with Lung Cancer Treated by Surgery: A Retrospective Cohort Study. Health 2020, 8, 405. [Google Scholar] [CrossRef]
- Suzuki, H.; Matsuo, K.; Okamoto, M.; Nakata, H.; Sakamoto, H.; Fujita, M. Perioperative changes in oral bacteria number in patients undergoing cardiac valve surgery. J. Oral Sci. 2019, 61, 526–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okuda, K.; Ishihara, K.; Nakagawa, T.; Hirayama, A.; Inayama, Y.; Okuda, K. Detection of Treponema denticola in atherosclerotic lesions. J. Clin. Microbiol. 2001, 39, 1114–1117. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Deanfield, J. Treatment of Periodontitis and Endothelial Function. N. Engl. J. Med. 2018, 378, 2450. [Google Scholar]
- Hamada, R.; Nakano, M.; Suehiro, J.; Konishi, K.; Kikutani, T. Development of rapid oral bacteria detection apparatus based on dielectrophoretic impedance measurement method. IET Nanobiotechnol. 2011, 5, 25–31. [Google Scholar] [CrossRef]
- Katayama, H.; Kurokawa, Y.; Nakamura, K.; Ito, H.; Kanemitsu, Y.; Masuda, N.; Tsubosa, Y.; Satoh, T.; Yokomizo, A.; Fukuda, H.; et al. Extended Clavien-Dindo classification of surgical complications: Japan Clinical Oncology Group postoperative complications criteria. Surg. Today 2016, 46, 668–685. [Google Scholar] [CrossRef] [Green Version]
- Finegold, J.A.; Asaria, P.; Francis, D.P. Mortality from ischaemic heart disease by country, region, and age: Statistics from World Health Organisation and United Nations. Int. J. Cardiol. 2013, 168, 934–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yano, K.; Reed, D.M.; McGee, D.L. Ten-year incidence of coronary heart disease in the Honolulu Heart Program. Relationship to biologic and lifestyle characteristics. Am. J. Epidemiol. 1984, 119, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Kiyohara, Y.; Kato, I.; Tanizaki, Y.; Arima, H.; Tanaka, K.; Nakamura, H.; Okubo, K.; Iida, M. Trends in the incidence, mortality, and survival rate of cardiovascular disease in a Japanese community: The Hisayama study. Stroke 2003, 34, 2349–2354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.-Z.; Yuan, Y.-H.; Liu, H.-H.; Li, S.-S.; Zhang, B.-W.; Chen, W.; An, Z.-J.; Chen, S.-Y.; Wu, Y.-Z.; Han, B.; et al. Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral Health 2020, 20, 204. [Google Scholar] [CrossRef]
- Holmlund, A.; Lampa, E.; Lind, L. Poor Response to Periodontal Treatment May Predict Future Cardiovascular Disease. J. Dent. Res. 2017, 96, 768–773. [Google Scholar] [CrossRef]
- Huff, C.M.; Silver, M.J.; Ansel, G.M. Percutaneous Endovascular Aortic Aneurysm Repair for Abdominal Aortic Aneurysm. Curr. Cardiol. Rep. 2018, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Stoberock, K.; Kölbel, T.; Atlihan, G.; Debus, E.S.; Tsilimparis, N.; Larena-Avellaneda, A.; Behrendt, C.-A.; Wipper, S. Gender differences in abdominal aortic aneurysm therapy a systematic review. Vasa 2018, 47, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, A.; Sato, T.; Hoshikawa, Y.; Ishida, N.; Tanda, N.; Kawamura, Y.; Kondo, T.; Takahashi, N. Detection and identification of oral anaerobes in intraoperative bronchial fluids of patients with pulmonary carcinoma. Microbiol. Immunol. 2014, 58, 375–381. [Google Scholar] [CrossRef]
- Akutsu, Y.; Matsubara, H.; Okazumi, S.; Shimada, H.; Shuto, K.; Shiratori, T.; Ochiai, T. Impact of preoperative dental plaque culture for predicting postoperative pneumonia in esophageal cancer patients. Dig. Surg. 2008, 25, 93–97. [Google Scholar] [CrossRef]
- Bágyi, K.; Haczku, A.; Márton, I.; Szabó, J.; Gáspár, A.; Andrási, M.; Varga, I.; Tóth, J.; Klekner, A. Role of pathogenic oral flora in postoperative pneumonia following brain surgery. BMC Infect. Dis. 2009, 9, 104. [Google Scholar] [CrossRef] [Green Version]
- Iwamoto, M.; Morikawa, T.; Narita, M.; Shibahara, T.; Katakura, A. Investigation of Surgical Site Infections and Bacteria Detected Following Neck Dissection in Patients with Oral Cancer. Bull. Tokyo Dent. Coll. 2020, 61, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knox, K.W.; Hunter, N. The role of oral bacteria in the pathogenesis of infective endocarditis. Aust. Dent. J. 1991, 36, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Arweiler, N.B.; Marx, V.K.; Laugisch, O.; Sculean, A.; Auschill, T.M. Clinical evaluation of a newly developed chairside test to determine periodontal pathogens. J. Periodontol. 2020, 91, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Chambless, L.E.; Folsom, A.R.; Sharrett, A.; Sorlie, P.; Couper, D.; Szklo, M.; Nieto, F. Coronary heart disease risk prediction in the Atherosclerosis Risk in Communities (ARIC) study. J. Clin. Epidemiol. 2003, 56, 880–890. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Category | N (%) or Median (IQR) |
|---|---|---|
| Age | 76.0 (69.0–81.0) | |
| Sex | Male | 301 (64.0) |
| Female | 169 (36.0) | |
| Body mass index | 21.9 (19.6–24.6) | |
| Performance status | 0 | 438 (93.2) |
| 1 | 12 (2.6) | |
| 2 | 13 (2.8) | |
| 3 | 4 (0.9) | |
| 4 | 3 (0.6) | |
| Brinkman Index | 0.0 (0.0–800.0) | |
| Cardiovascular disease | Angina | 42 (8.9) |
| Myocardial infarction | 7 (1.5) | |
| Aortic aneurysm | 162 (34.5) | |
| Aortic dissection | 3 (0.6) | |
| Valvular disease | 212 (45.1) | |
| Cardiomyopathy | 1 (0.2) | |
| Atrial septal defect | 4 (0.9) | |
| Heart tumor | 5 (1.1) | |
| Heart failure | 2 (0.4) | |
| Arrhythmia | 6 (1.3) | |
| Arteriosclerosis obliterans | 4 (0.9) | |
| Popliteal aneurysm | 2 (0.4) | |
| Iliac artery aneurysm | 12 (2.6) | |
| Myocarditis | 1 (0.2) | |
| Internal carotid artery stenosis | 1 (0.2) | |
| Aortic dilation | 2 (0.4) | |
| Ventricular aneurysm | 1 (0.2) | |
| Rurish syndrome | 1 (0.2) | |
| Cardiogenic cerebral embolism | 1 (0.2) | |
| Infective endocarditis | 1 (0.2) | |
| Medical history | Diabetes mellitus | 104 (22.1) |
| Cerebrovascular disease | 61 (13.0) | |
| Cancer | 85 (18.1) | |
| Dementia | 8 (1.7) | |
| Rheumatoid | 6 (1.3) | |
| Number of teeth | 17.0 (5.0–25.0) | |
| Denture | Yes | 233 (49.6) |
| Home dentist | Yes | 359 (76.4) |
| Oral bacterial count at pre-hospitalization | (106 CFU/mL) | 26.8 (14.2–47.1) |
| Level | 5.0 (5.0–6.0) | |
| Oral bacterial count at preoperation | (106 CFU/mL) | 15.8 (7.4–31.2) |
| Level | 5.0 (4.0–5.0) | |
| Oral bacterial count at postoperation | (106 CFU/mL) | 13.2 (6.4–23.5) |
| Level | 5.0 (4.0–5.0) | |
| Operation time | (minutes) | 305.5 (204.8–382.0) |
| White blood cell count at preoperation | 103/μL | 6.0 (4.9–7.3) |
| Serum albumin value at preoperation | g/dL | 4.0 (3.6–4.3) |
| Hospital duration | Day | 17.0 (14.0–23.0) |
| Type of Complication | N (%) |
|---|---|
| Pericardial fluid storage | 21 (42.9) |
| Postoperative pneumonia | 13 (26.5) |
| Surgical site infection | 9 (18.4) |
| Mediastinitis | 2 (4.1) |
| Seroma | 1 (2.0) |
| Postoperative infective endocarditis | 1 (2.0) |
| Lung torsion | 1 (2.0) |
| Pericardial effusion | 1 (2.0) |
| Variables | Category | N (%) or Median (IQR) | p-Value | |
|---|---|---|---|---|
| Non-Complication (N = 421) | Complication (N = 49) | |||
| Age | 76.0 (69.0–81.0) | 73.0 (68.0–78.0) | 0.11 a | |
| Sex | Male | 263 (62.5) | 38 (77.6) | 0.04 b,* |
| Female | 158 (37.5) | 11 (22.4) | ||
| Body mass index | 22.0 (19.8–24.5) | 21.2 (18.5–24.9) | 0.25 a | |
| Performance status | 0 | 391 (92.9) | 47 (95.9) | 0.44 a |
| 1 | 12 (2.9) | 0 (0) | ||
| 2 | 12 (2.9) | 1 (2.0) | ||
| 3 | 3 (0.7) | 1 (2.0) | ||
| 4 | 3 (0.7) | 0 (0) | ||
| Brinkman Index | 0.0 (0.0–770.0) | 450.0 (0.0–900.0) | 0.05 a | |
| Cardiovascular disease | Angina | 40 (9.5) | 2 (4.1) | – |
| Myocardial infarction | 6 (1.4) | 1 (2.0) | ||
| Aortic aneurysm | 145 (34.4) | 17 (34.7) | ||
| Aortic dissection | 3 (0.7) | 0 (0) | ||
| Valvular disease | 190 (45.1) | 22 (44.9) | ||
| Cardiomyopathy | 1 (0.2) | 0 (0) | ||
| Atrial septal defect | 4 (1.0) | 0 (0) | ||
| Heart tumor | 4 (1.0) | 1 (2.0) | ||
| Heart failure | 1 (0.2) | 1 (2.0) | ||
| Arrhythmia | 6 (1.4) | 0 (0) | ||
| Arteriosclerosis obliterans | 4 (1.0) | 0 (0) | ||
| Popliteal aneurysm | 1 (0.2) | 1 (2.0) | ||
| Iliac artery aneurysm | 12 (2.9) | 0 (0) | ||
| Myocarditis | 0 (0) | 1 (2.0) | ||
| Internal carotid artery stenosis | 1 (0.2) | 0 (0) | ||
| Aortic dilation | 2 (0.5) | 0 (0) | ||
| Ventricular aneurysm | 0 (0) | 1 (2.0) | ||
| Rurish syndrome | 1 (0.2) | 0 (0) | ||
| Cardiogenic cerebral embolism | 0 (0) | 1 (2.0) | ||
| Infective endocarditis | 0 (0) | 1 (2.0) | ||
| Medical history | Diabetes mellitus | 92 (21.9) | 12 (24.5) | 0.72 b |
| Cerebrovascular disease | 50 (11.9) | 11 (22.4) | 0.04 b,* | |
| Cancer | 73 (17.3) | 12 (24.5) | 0.24 b | |
| Dementia | 7 (1.7) | 1 (2.0) | 0.59 b | |
| Rheumatoid | 6 (1.4) | 0 (0) | 1.00 b | |
| Number of teeth | 17.0 (6.0–25.0) | 17.0 (2.0–26.0) | 0.91 a | |
| Denture | Yes | 207 (49.2) | 26 (53.1) | 0.65 b |
| Home dentist | Yes | 316 (75.1) | 43 (87.8) | 0.05 b |
| Oral bacterial count at pre-hospitalization | Level | 5.0 (5.0–6.0) | 5.0 (5.0–6.0) | 0.65 a |
| Oral bacterial count at preoperation | Level | 5.0 (4.0–5.0) | 5.0 (4.0–6.0) | 0.28 a |
| Oral bacterial count at postoperation | Level | 5.0 (4.0–5.0) | 5.0 (4.0–5.0) | 0.08 a |
| Operation time | (minutes) | 297.0 (196.0–368.0) | 379.0 (311.0–467.0) | <0.01 a,* |
| White blood cell count at preoperation | 103/μL | 6.0 (4.9–7.4) | 6.0 (4.9–7.2) | 0.95 a |
| Serum albumin value at preoperation | g/dL | 4.0 (3.6–4.3) | 4.0 (3.5–4.3) | 1.00 a |
| Explanatory Variable | Odds Ratio (CI) | p‒Values | |
|---|---|---|---|
| Oral bacterial count at pre-hospitalization | Level | 0.90 (0.69–1.17) | 0.43 |
| Oral bacterial count at preoperation | Level | 1.14 (0.84–1.56) | 0.40 |
| Oral bacterial count at postoperation | Level | 1.26 (1.00–1.60) | 0.05 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osako, R.; Matsuda, Y.; Itohara, C.; Sukegawa-Takahashi, Y.; Sukegawa, S.; Okuma, S.; Furuki, Y.; Kanno, T. Relationship between Oral Bacterial Count and Postoperative Complications among Patients with Cardiovascular Disease Treated by Surgery: A Retrospective Cohort Study. Healthcare 2021, 9, 850. https://doi.org/10.3390/healthcare9070850
Osako R, Matsuda Y, Itohara C, Sukegawa-Takahashi Y, Sukegawa S, Okuma S, Furuki Y, Kanno T. Relationship between Oral Bacterial Count and Postoperative Complications among Patients with Cardiovascular Disease Treated by Surgery: A Retrospective Cohort Study. Healthcare. 2021; 9(7):850. https://doi.org/10.3390/healthcare9070850
Chicago/Turabian StyleOsako, Rie, Yuhei Matsuda, Chieko Itohara, Yuka Sukegawa-Takahashi, Shintaro Sukegawa, Satoe Okuma, Yoshihiko Furuki, and Takahiro Kanno. 2021. "Relationship between Oral Bacterial Count and Postoperative Complications among Patients with Cardiovascular Disease Treated by Surgery: A Retrospective Cohort Study" Healthcare 9, no. 7: 850. https://doi.org/10.3390/healthcare9070850