
Have We Taken Advantage of the Quarantine to Develop Healthy Habits? A Cross-Sectional Analysis of the Spanish COVID-19 Situation by Gender




Abstract
:1. Introduction
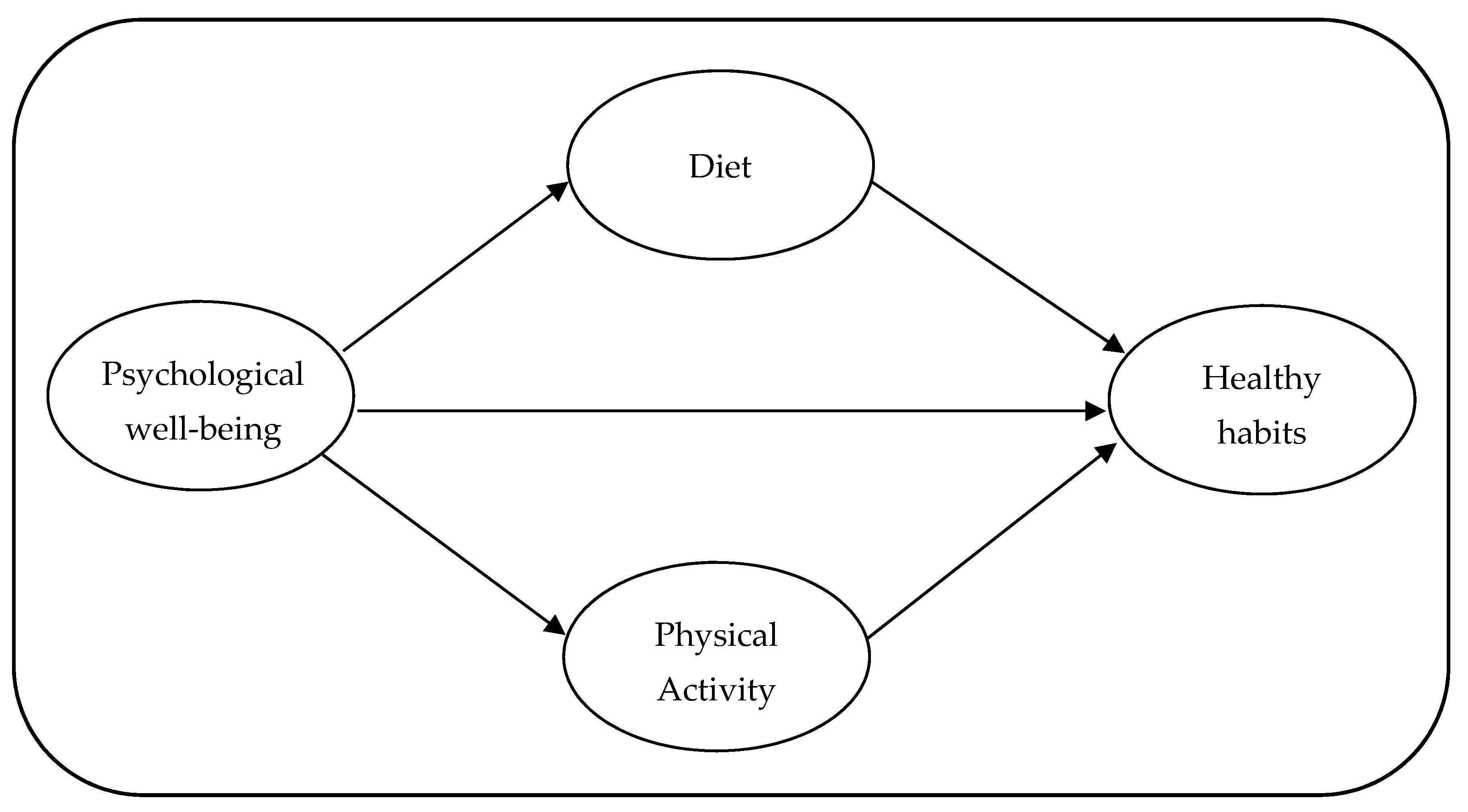
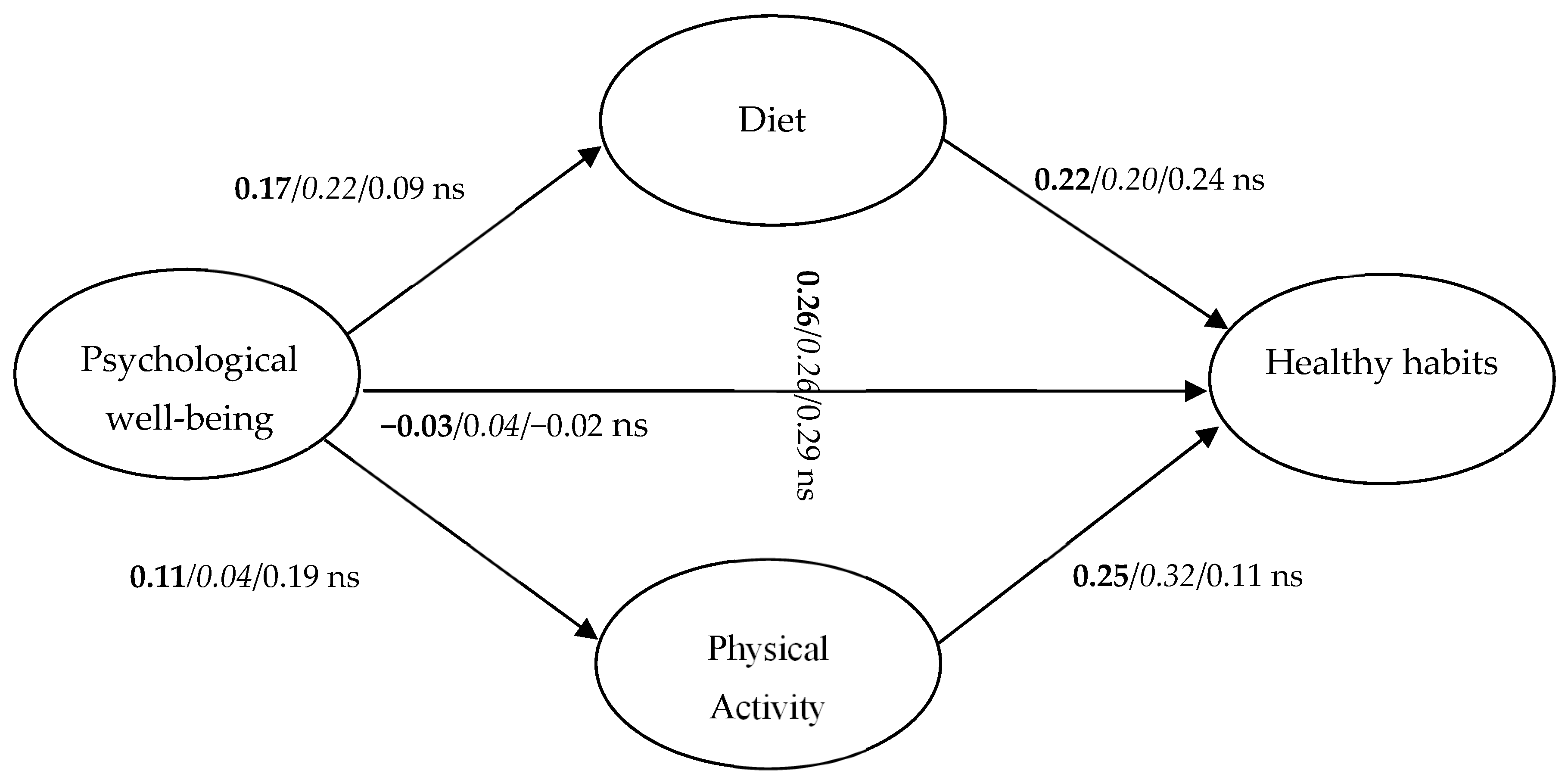
- Objective 1: to verify if the PWB of people, derived from the quarantine situation, relates to healthy habits, and if PA and diet mediate this relationship (see Figure 1).
- Objective 2: to test if there are differences in this model of relationships between women and men.
- Objective 3: to analyze if there are differences in the levels of healthy habits, PA, diet, and PWB depending on gender.
- Objective 4: to test if there are differences in the levels of healthy habits, PA, diet, and PWB depending on living area.
- Objective 5: to assess if there are interaction effects of gender and living area in the levels of healthy habits, PA, diet, and PWB.
2. Materials and Methods
2.1. Participants
2.2. Materials
2.3. Design and Procedure
2.4. Data Analysis
3. Results
3.1. Reliability Analysis
3.2. Descriptive Analysis
3.3. SEM and MLG Analyses
3.4. Gender Comparisons
3.5. Living Area Comparisons
3.6. Interactions between Gender and Living Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GHQ | General Health Questionnaire |
| IPAQ | International Physical Activity Questionnaire |
| MLG | Multi-Group |
| PA | Physical Activity |
| PWB | Psychological wellbeing |
| SEM | Structural Equation Models |
| WHO | World Health Organization |
References
- Sirois, F.M.; Kitner, R.; Hirsch, J.K. Self-Compassion, Affect, and Health-Promoting Behaviors. Health Psychol. 2015, 34, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Lucyk, K.; McLaren, L. Taking Stock of the Social Determinants of Health: A Scoping Review. PLoS ONE 2017, 12, e0177306. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.M. Social Determinants of Health and Related Inequalities: Confusion and Implications. Front. Public Health 2019, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artiga, S.; Hinton, E. Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity; University of California Press: Berkeley, CA, USA, 2018; Volume 13. [Google Scholar]
- WHO|About Social Determinants of Health. Available online: http://www.who.int/social_determinants/sdh_definition/en/ (accessed on 22 June 2020).
- Turner-Musa, J.; Ajayi, O.; Kemp, L. Examining Social Determinants of Health, Stigma, and COVID-19 Disparities. Healthcare 2020, 8, 168. [Google Scholar] [CrossRef]
- Braveman, P. Health Disparities and Health Equity: Concepts and Measurement. Annu. Rev. Public Health 2006, 27, 167–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braveman, P.; Egerter, S.; Williams, D.R. The Social Determinants of Health: Coming of Age. Annu. Rev. Public Health 2011, 32, 381–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmot, M. Social Determinants of Health Inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 22 June 2020).
- Mattioli, A.V.; Ballerini, M. Lifestyle at Time of COVID-19: How Could Quarantine Affect Cardiovascular Risk. Am. J. Lifestyle Med. 2020, 14, 240–242. [Google Scholar] [CrossRef]
- Gensini, G. The Concept of Quarantine in History: From Plague to SARS. J. Infect. 2004, 49, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Lin, E.C.L.; Peng, Y.C.; Hung Tsai, J.C. Lessons Learned from the Anti-SARS Quarantine Experience in a Hospital-Based Fever Screening Station in Taiwan. Am. J. Infect. Control 2010, 38, 302–307. [Google Scholar] [CrossRef]
- Sandín, B.; Valiente, R.M.; García-Escalera, J.; Chorot, P. Impacto psicológico de la pandemia de COVID-19: Efectos negativos y positivos en población española asociados al periodo de confinamiento nacional. RPPC 2020, 25, 1. [Google Scholar] [CrossRef]
- Matias, T.; Dominski, F.H.; Marks, D.F. Human Needs in COVID-19 Isolation. J. Health Psychol. 2020, 25, 871–882. [Google Scholar] [CrossRef] [PubMed]
- Real Decreto 463/2020. Real Decreto 463/2020, Declaración del Estado de Alarma para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19; Ministerio de la Presidencia, Relaciones con las Cortes y Memoria Democrática: Madrid, Spain, 2020; Volume 67, pp. 25390–25400.
- Ranscombe, P. Rural Areas at Risk during COVID-19 Pandemic. Lancet Infect. Dis. 2020, 20, 545. [Google Scholar] [CrossRef]
- De Luca, C.; Tondelli, S.; Åberg, H.E. The Covid-19 Pandemic Effects in Rural Areas. TeMA J. Land Use Mobil. Environ. 2020, 119–132. [Google Scholar] [CrossRef]
- Paul, R.; Arif, A.A.; Adeyemi, O.; Ghosh, S.; Han, D. Progression of COVID-19 From Urban to Rural Areas in the United States: A Spatiotemporal Analysis of Prevalence Rates. J. Rural Health 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with Sleep Problems during Home Confinement Due to the COVID-19 Outbreak: Practical Recommendations from a Task Force of the European CBT-I Academy. J. Sleep Res. 2020, 1–7. [Google Scholar] [CrossRef]
- DiGiovanni, C.; Conley, J.; Chiu, D.; Zaborski, J. Factors Influencing Compliance with Quarantine in Toronto During the 2003 SARS Outbreak. Biosecur. Bioterror. Biodefense Strategy Pract. Sci. 2004, 2, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Maynard, M.S.; Perlman, C.M.; Kirkpatrick, S.I. Food Insecurity and Perceived Anxiety among Adolescents: An Analysis of Data from the 2009–2010 National Health and Nutrition Examination Survey (NHANES). J. Hunger. Environ. Nutr. 2019, 14, 339–351. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely Mental Health Care for the 2019 Novel Coronavirus Outbreak Is Urgently Needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Nestle, M.; Wing, R.; Birch, L.; DiSogra, L.; Drewnowski, A.; Middleton, S.; Sigman-Grant, M.; Sobal, J.; Winston, M.; Economos, C. Behavioral and Social Influences on Food Choice. Nutr. Rev. 2009, 56, 50–64. [Google Scholar] [CrossRef] [Green Version]
- Ellison, N.B.; Lampe, C.; Steinfield, C. FEATURESocial Network Sites and Society: Current Trends and Future Possibilities. Interactions 2009, 16, 6. [Google Scholar] [CrossRef]
- Pouresmaeil, M.; Shahrokhi, A.; Hosseinzadeh, K.; Ziapour, A.; Rahimi, F. Presence in Virtual Social Networks and Health Promoting Behaviors of Medical Students. J. Public Health 2020. [Google Scholar] [CrossRef]
- Cooper, K.H. Aerobics Program for Total Well-Being: Exercise, Diet, and Emotional Balance; Bantam Books: New York, NY, USA, 2013; ISBN 978-0-307-77725-6. [Google Scholar]
- Aidman, E. Cognitive Fitness Framework: Towards Assessing, Training and Augmenting Individual-Difference Factors Underpinning High-Performance Cognition. Front. Hum. Neurosci. 2020, 13, 466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seligman, M.E.P. Positive Health. Appl. Psychol. 2008, 57, 3–18. [Google Scholar] [CrossRef]
- Robinson, P.; Oades, L.; Caputi, P. Conceptualising and Measuring Mental Fitness: A Delphi Study. Int. J. Wellbeing 2015, 5, 53–73. [Google Scholar] [CrossRef]
- Rodríguez, M.Á.; Crespo, I.; Olmedillas, H. Exercising in Times of COVID-19: What Do Experts Recommend Doing within Four Walls? Rev. Española Cardiol. Engl. Ed. 2020, 73, 257. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as Medicine–Evidence for Prescribing Exercise as Therapy in 26 Different Chronic Diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef] [Green Version]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between Physical Exercise and Mental Health in 1·2 Million Individuals in the USA between 2011 and 2015: A Cross-Sectional Study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus Infections and Immune Responses. J. Med. Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, Regional, and National Comparative Risk Assessment of 79 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Lv, M.-R.; Wei, Y.-J.; Sun, L.; Zhang, J.-X.; Zhang, H.-G.; Li, B. Dietary Patterns and Depression Risk: A Meta-Analysis. Psychiatry Res. 2017, 253, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.; Brown, H.; Wrieden, W.; White, M.; Adams, J. Frequency of Eating Home Cooked Meals and Potential Benefits for Diet and Health: Cross-Sectional Analysis of a Population-Based Cohort Study. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 109. [Google Scholar] [CrossRef]
- Tarín, G.S.; Tarín, G.S. Los Dos Pilares de La Promoción de La Salud Según Hipócrates, Que Hoy Serían Seis. Rev. Asoc. Española Espec. Med. Trab. 2018, 27, 131–132. [Google Scholar]
- Schubert, M.M.; Broom, D.R. Exercise and Diet. In Handbook of Eating and Drinking: Interdisciplinary Perspectives; Meiselman, H.L., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 787–803. ISBN 978-3-030-14504-0. [Google Scholar]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A Nationwide Survey of Psychological Distress among Chinese People in the COVID-19 Epidemic: Implications and Policy Recommendations. Gen. Psychiatr. 2020, 33. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Marco, A.D.; Rossi, A.; Siracusano, A.; Lorenzo, G.D. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health among the General Population in Italy. An N=18147 Web-Based Survey. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.S.; Kubzansky, L.D.; Soo, J.; Boehm, J.K. Maintaining Healthy Behavior: A Prospective Study of Psychological Well-Being and Physical Activity. Ann. Behav. Med. 2017, 51, 337–347. [Google Scholar] [CrossRef]
- Bragina, I.; Voelcker-Rehage, C. The Exercise Effect on Psychological Well-Being in Older Adults—a Systematic Review of Longitudinal Studies. Ger. J. Exerc. Sport Res. 2018, 48, 323–333. [Google Scholar] [CrossRef]
- Boehm, J.K.; Soo, J.; Zevon, E.S.; Chen, Y.; Kim, E.S.; Kubzansky, L.D. Longitudinal Associations between Psychological Well-Being and the Consumption of Fruits and Vegetables. Health Psychol. 2018, 37, 959–967. [Google Scholar] [CrossRef]
- Chida, Y.; Steptoe, A. Positive Psychological Well-Being and Mortality: A Quantitative Review of Prospective Observational Studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef]
- Alcántara, C.; Diaz, S.V.; Cosenzo, L.G.; Loucks, E.B.; Penedo, F.J.; Williams, N.J. Social Determinants as Moderators of the Effectiveness of Health Behavior Change Interventions: Scientific Gaps and Opportunities. Health Psychol. Rev. 2020, 14, 132–144. [Google Scholar] [CrossRef] [PubMed]
- Alaminos, A.; Castejón, J.L. Elaboración, Análisis e Interpretación de Encuestas, Cuestionarios y Escalas de Opinión; Marfil: Alcoy, España, 2006; ISBN 84-268-1267-8. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roman-Viñas, B.; Serra-Majem, L.; Hagströmer, M.; Ribas-Barba, L.; Sjöström, M.; Segura-Cardona, R. International Physical Activity Questionnaire: Reliability and Validity in a Spanish Population. Eur. J. Sport Sci. 2010, 10, 297–304. [Google Scholar] [CrossRef]
- Bauman, A.; Bull, F.; Chey, T.; Craig, C.L.; Ainsworth, B.E.; Sallis, J.F.; Bowles, H.R.; Hagstromer, M.; Sjostrom, M.; Pratt, M.; et al. The International Prevalence Study on Physical Activity: Results from 20 Countries. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 21. [Google Scholar] [CrossRef]
- Goldberg, D.; Williams, P. A User’s Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- Rocha, K.B.; Pérez, K.; Rodríguez-Sanz, M.; Borrell, C.; Jordi, E. Obiols Propiedades psicométricas y valores normativos del General Health Questionnaire (GHQ-12) en población general española. Int. J. Clin. Health Psychol. 2011, 11, 125–139. [Google Scholar]
- Sánchez-López, M.P.; Dresch, V. The 12-Item General Health Questionnaire (GHQ-12): Relibability, External Validity and Factor Structure in the Spanish Population. Psicothema 2008, 20, 839–843. [Google Scholar]
- Claes, R.; Fraccaroli, F. The General Health Questionnaire (GHQ-12): Factorial Invariance in Different Language Versions. Boll. Psicol. Appl. 2002, 237, 25–35. [Google Scholar]
- Cuéllar-Flores, I.; Sánchez-López, M.P.; Limiñana-Gras, R.M.; Colodro-Conde, L. The GHQ-12 for the Assessment of Psychological Distress of Family Caregivers. Behav. Med. 2014, 40, 65–70. [Google Scholar] [CrossRef]
- Nilsson, K.W.; Leppert, J.; Simonsson, B.; Starrin, B. Sense of Coherence and Psychological Well-Being: Improvement with Age. J. Epidemiol. Community Health 2010, 64, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Sociedad Española De Nutrición Comunitaria. Available online: https://www.nutricioncomunitaria.org/es/noticia/guia-de-alimentacion-saludablesenc (accessed on 17 June 2020).
- Chin, W.W. How to Write Up and Report PLS Analyses. In Handbook of Partial Least Squares: Concepts, Methods and Applications; Esposito Vinzi, V., Chin, W.W., Henseler, J., Wang, H., Eds.; Springer Handbooks of Computational Statistics; Springer: Berlin/Heidelberg, Germany, 2010; pp. 655–690. ISBN 978-3-540-32827-8. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Bentler, P.M.; Yuan, K.-H. Structural Equation Modeling with Small Samples: Test Statistics. Multivar. Behav. Res. 1999, 34, 181–197. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Iverson, R.D.; Maguire, C. The Relationship between Job and Life Satisfaction: Evidence from a Remote Mining Community. Hum. Relat. 2000. [Google Scholar] [CrossRef]
- Terry, M.L.; Leary, M.R.; Mehta, S.; Henderson, K. Self-Compassionate Reactions to Health Threats. Pers. Soc. Psychol. Bull. 2013, 39, 911–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunne, S.; Sheffield, D.; Chilcot, J. Brief Report: Self-Compassion, Physical Health and the Mediating Role of Health-Promoting Behaviours. J. Health Psychol. 2018, 23, 993–999. [Google Scholar] [CrossRef] [Green Version]
- Ridder, D.D.; de Wit, J.; Adriaanse, M.A. Making Plans for Healthy Diet: The Role of Motivation and Action Orientation. Eur. J. Soc. Psychol. 2009, 39, 622–630. [Google Scholar] [CrossRef]
- Carrero, I.; Vilà, I.; Redondo, R. What Makes Implementation Intention Interventions Effective for Promoting Healthy Eating Behaviours? A Meta-Regression. Appetite 2019, 140, 239–247. [Google Scholar] [CrossRef]
- Algarni, A.S.A.; Alqahtani, W.S.S.; Alotaibi, F.S.A.; Asiri, A.M.; Mutheeb, A.; Alwadie, A.M.F.; Alkhidhran, S.S.S.; Asiri, A.M.B.; Al-mosa, W.H.; Shehata, F.; et al. Gender Differences in Habits for a Healthy Lifestyle among Medical Students, Saudi Arabia. Indo Am. J. Pharm. Sci. 2019, 7, 636–642. [Google Scholar]
- Hagstromer, M.; Ainsworth, B.E.; Oja, P.; Sjostrom, M. Comparison of a Subjective and an Objective Measure of Physical Activity in a Population Sample. J. Phys. Act. Health 2010, 7, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Procter-Gray, E.; Olendzki, B.; Kane, K.; Churchill, L.; Hayes, R.B.; Aguirre, A.; Kang, H.; Li, W.; Health Statistics and Geography Lab, Division of Preventive and Behavioral Medicine, Department of Medicine, University of Massachusetts Medical School, Worcester, MA 01655, USA. Comparison of Dietary Quality Assessment Using Food Frequency Questionnaire and 24-Hour-Recalls in Older Men and Women. AIMS Public Health 2017, 4, 326–346. [Google Scholar] [CrossRef] [PubMed]
- Kiefer, I.; Rathmanner, T.; Kunze, M. Eating and Dieting Differences in Men and Women. J. Men’s Health Gend. 2005, 2, 194–201. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Lipovetsky, G. La Tercera Mujer-Lipovetsky, Gilles; Anagrama: Barcelona, Spain, 2006; ISBN 978-84-339-0573-4. [Google Scholar]
- Sok, S.; Pal, K.; Tuot, S.; Yi, R.; Chhoun, P.; Yi, S. Health Behaviors among Male and Female University Students in Cambodia: A Cross-Sectional Survey. J. Environ. Public Health 2020, 2020, 6740236. [Google Scholar] [CrossRef]
- Mao, H.-Y.; Hsu, H.-C.; Lee, S.-D. Gender Differences in Related Influential Factors of Regular Exercise Behavior among People in Taiwan in 2007: A Cross-Sectional Study. PLoS ONE 2020, 15, e0228191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, T.; Tanisawa, K.; Kawakami, R.; Usui, C.; Ishii, K.; Suzuki, K.; Sakamoto, S.; Muraoka, I.; Oka, K.; Higuchi, M. Micronutrient Intake Adequacy in Men and Women with a Healthy Japanese Dietary Pattern. Nutrients 2019, 12, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shernoff, E.S.; Mehta, T.G.; Atkins, M.S.; Torf, R.; Spencer, J. A Qualitative Study of the Sources and Impact of Stress Among Urban Teachers. Sch. Ment. Health 2011, 3, 59–69. [Google Scholar] [CrossRef]
- Von Bothmer, M.I.K.; Fridlund, B. Gender Differences in Health Habits and in Motivation for a Healthy Lifestyle among Swedish University Students. Nurs. Health Sci. 2005, 7, 107–118. [Google Scholar] [CrossRef]
- Jayachandran, S. The Roots of Gender Inequality in Developing Countries. Annu. Rev. Econ. 2015, 7, 63–88. [Google Scholar] [CrossRef]
- Palomino Moral, P.A.; Grande Gascón, M.L.; Linares Abad, M. La salud y sus determinantes sociales. Desigualdades y exclusión en la sociedad del siglo XXI. Rev. Int. Sociol. 2014, 72, 45–70. [Google Scholar] [CrossRef] [Green Version]
- Olson, J.L.; March, S.; Clough, B.; Biddle, S.J.H.; Ireland, M. Not Quite City and Not Quite Rural: Active Lifestyle Beliefs in Peri-Urban Australians. Health Promot. J. Aust. 2019, 30, 72–84. [Google Scholar] [CrossRef]
- Sygit, K.M.; Sygit, M.; Wojtyla-Buciora, P.; Lubiniec, O.; Stelmach, W.; Krakowiak, J. Physical Activity as an Important Element in Organizing and Managing the Lifestyle of Populations in Urban and Rural Environments. Ann. Agric. Environ. Med. 2019, 26, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Nepomuceno, B.B.; Cardoso, A.A.V.; Ximenes, V.M.; Barros, J.P.P.; Leite, J.F. Mental Health, Well-Being, and Poverty: A Study in Urban and Rural Communities in Northeastern Brazil. J. Prev. Interv. Community 2016, 44, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Eckert, K.A.; Taylor, A.W.; Tucker, G.R.; Wilkinson, D.D. How Does Mental Health Status Relate to Accessibility and Remoteness? Med. J. Aust. 2004, 181, 540–543. [Google Scholar] [CrossRef]
- Easterlin, R.A.; Angelescu, L.; Zweig, J.S. The Impact of Modern Economic Growth on Urban–Rural Differences in Subjective Well-Being. World Dev. 2011, 39, 2187–2198. [Google Scholar] [CrossRef]
- Conway, J.M. Method variance and method bias in industrial and organizational psychology. In Handbook of Research Methods in Industrial and Organizational Psychology; Jonh wiley & Sons, Inc.: Malden, NJ, USA, 2008; pp. 344–365. ISBN 978-0-470-75657-7. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common Method Biases in Behavioral Research: A Critical Review of the Literature and Recommended Remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Li, L.; Gan, Y.; Wang, C.; Jiang, H.; Cao, S.; Lu, Z. Sedentary Behaviors and Risk of Depression: A Meta-Analysis of Prospective Studies. Transl. Psychiatry 2020, 10, 26. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Women | Men | ||
|---|---|---|---|
| Unemployed | Count | 127 | 46 |
| Expected count (%) | 116.9 (12.5) | 56.1 (9.4) | |
| Adjusted residual | 1.7 | −1.7 | |
| ERTE | Count | 127 | 55 |
| Expected count (%) | 122.9 (12.5) | 59.1 (11.2) | |
| Adjusted residual | 0.7 | −0.7 | |
| Face-to-face work | Count | 89 | 57 |
| Expected count (%) | 98.6 (8.7) | 47.4 (11.7) | |
| Adjusted residual | −18 | 1.8 | |
| Online work | Count | 333 | 162 |
| Expected count (%) | 334.4 (22.1) | 160.6 (10.7) | |
| Adjusted residual | −0.2 | 0.2 | |
| Face-to-face and online work | Count | 40 | 43 |
| Expected count (%) | 56.1 (2.7) | 26.9 (2.9) | |
| Adjusted residual | −3.9 | 3.9 | |
| Study | Count | 274 | 112 |
| Expected count (%) | 260.7 (18.2) | 125.3 (7.4) | |
| Adjusted residual | 1.7 | −1.7 | |
| Another situation | Count | 28 | 14 |
| Expected count (%) | 28.4 (1.9) | 13.6 (0.9) | |
| Adjusted residual | −0.1 | 0.1 |
| Variable | M ± SD | Correlations | |||
|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | ||
| 1. Healthy habits | 2.36 ± 1.67 | 1 | 0.12 ** | 0.13 ** | 0.02 |
| 2. PA | 1864.80 ± 2918.31 | - | 1 | 0.13 ** | 0.08 ** |
| 3. Diet | 10.02 ± 5.51 | - | - | 1 | 0.14 ** |
| 4. PWB | 2.84 ± 5.79 | - | - | - | 1 |
| Variables | Women | Men | F | p | ŋ2partial | ||
|---|---|---|---|---|---|---|---|
| n (%) | M ± SD | n (%) | M ± SD | ||||
| Healthy habits | 974 (67.6) | 2.51 ± 1.7 | 466 (32.4) | 2.1 ± 1.61 | 15.26 | 0.0001 | 0.011 |
| PA | 974 (67.6) | 1758.58 ± 2365.02 | 466 (32.4) | 2038.23 ± 2753.05 | 4.75 | 0.03 | 0.003 |
| Diet | 974 (67.6) | 10.12 ± 5.16 | 466 (32.4) | 9.7 ± 5.16 | 0.76 | 0.38 | 0.001 |
| PWB | 974 (67.6) | 2.78 ± 0.59 | 466 (32.4) | 2.95 ± 0.53 | 12.06 | 0.001 | 0.008 |
| Variables | Urban Area | Rural Area | F | p | ŋ2partial | ||
|---|---|---|---|---|---|---|---|
| n (%) | M ± SD | n (%) | M ± SD | ||||
| Healthy habits | 1222 (84.8) | 2.38 ± 1.7 | 218 (15.2) | 2.37 ± 1.68 | 0.90 | 0.34 | 0.001 |
| PA | 1222 (84.8) | 1798.22 ± 2437.58 | 218 (15.2) | 2134.18 ± 2811.65 | 4.91 | 0.03 | 0.003 |
| Diet | 1222 (84.8) | 10.01 ± 5.19 | 218 (15.2) | 9.81 ± 5.04 | 0.26 | 0.61 | 0.0001 |
| PWB | 1222 (84.8) | 2.86 ± 0.57 | 218 (15.2) | 2.7 ± 0.59 | 8.61 | 0.003 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corbí, M.; Del Líbano, M.; Alonso-Centeno, A.; Gutiérrez-García, A. Have We Taken Advantage of the Quarantine to Develop Healthy Habits? A Cross-Sectional Analysis of the Spanish COVID-19 Situation by Gender. Healthcare 2021, 9, 844. https://doi.org/10.3390/healthcare9070844
Corbí M, Del Líbano M, Alonso-Centeno A, Gutiérrez-García A. Have We Taken Advantage of the Quarantine to Develop Healthy Habits? A Cross-Sectional Analysis of the Spanish COVID-19 Situation by Gender. Healthcare. 2021; 9(7):844. https://doi.org/10.3390/healthcare9070844
Chicago/Turabian StyleCorbí, Miguel, Mario Del Líbano, Almudena Alonso-Centeno, and Aida Gutiérrez-García. 2021. "Have We Taken Advantage of the Quarantine to Develop Healthy Habits? A Cross-Sectional Analysis of the Spanish COVID-19 Situation by Gender" Healthcare 9, no. 7: 844. https://doi.org/10.3390/healthcare9070844