
Effects of Semi-Immersive Virtual Reality-Based Cognitive Training Combined with Locomotor Activity on Cognitive Function and Gait Ability in Community-Dwelling Older Adults

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
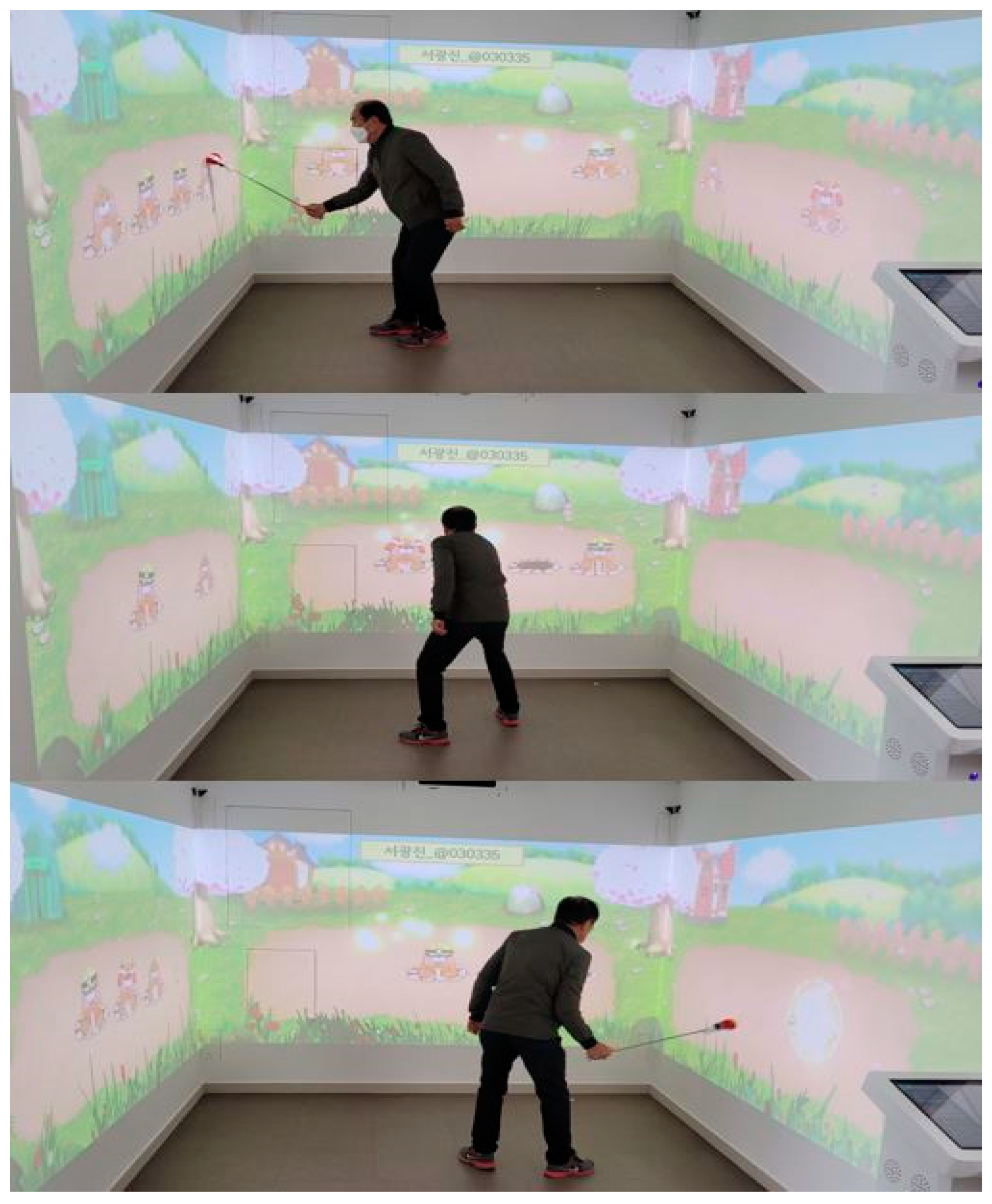
2.2. Study Design and Procedures
2.3. Outcome Measurements
2.4. Statistical Analysis
3. Results
3.1. Subjects’ Characteristics
3.2. Cognitive Function Evaluation
3.3. Gait and Balance Evaluations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Andrews-Hanna, J.R.; Snyder, A.Z.; Vincent, J.L.; Lustig, C.; Head, D.; Raichle, M.E.; Buckner, R.L. Disruption of large-scale brain systems in advanced aging. Neuron 2007, 56, 924–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, N.A.; Lu, T.; Yankner, B.A. Neural mechanisms of ageing and cognitive decline. Nature 2010, 464, 529–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurd, M.D.; Martorell, P.; Delavande, A.; Mullen, K.J.; Langa, K.M. Monetary costs of dementia in the United States. N. Engl. J. Med. 2013, 368, 1326–1334. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.S.; Kim, Y.B.; Kim, H. Discourse Measures to Differentiate Between Mild Cognitive Impairment and Healthy Aging. Front. Aging Neurosci. 2019, 11, 221. [Google Scholar] [CrossRef] [PubMed]
- Fazelzadeh, P.; Hangelbroek, R.W.; Tieland, M.; de Groot, L.C.; Verdijk, L.B.; van Loon, L.J.; Smilde, A.K.; Alves, R.D.; Vervoort, J.; Müller, M.; et al. The Muscle Metabolome Differs between Healthy and Frail Older Adults. J. Proteome Res. 2016, 15, 499–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verghese, J.; LeValley, A.; Hall, C.B.; Katz, M.J.; Ambrose, A.F.; Lipton, R.B. Epidemiology of gait disorders in community-residing older adults. J. Am. Geriatr. Soc. 2006, 54, 255–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [Green Version]
- Liao, Y.Y.; Tseng, H.Y.; Lin, Y.J.; Wang, C.J.; Hsu, W.C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef]
- Zając-Lamparska, L.; Wiłkość-Dębczyńska, M.; Wojciechowski, A.; Podhorecka, M.; Polak-Szabela, A.; Warchoł, Ł.; Kędziora-Kornatowska, K.; Araszkiewicz, A.; Izdebski, P. Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: A pretest-posttest design pilot study. BMC Res. Notes 2019, 12, 776. [Google Scholar] [CrossRef]
- Rendon, A.A.; Lohman, E.B.; Thorpe, D.; Johnson, E.G.; Medina, E.; Bradley, B. The effect of virtual reality gaming on dynamic balance in older adults. Age Ageing 2012, 41, 549–552. [Google Scholar] [CrossRef] [Green Version]
- Holden, M.K. Virtual environments for motor rehabilitation: Review. Cyberpsychol. Behav. 2005, 8, 187–211. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.L.; Rand, D.; Katz, N.; Kizony, R. Video capture virtual reality as a flexible and effective rehabilitation tool. J. Neuroeng. Rehabil. 2004, 1, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rand, D.; Kizony, R.; Weiss, P.T. The Sony PlayStation II EyeToy: Low-cost virtual reality for use in rehabilitation. J. Neurol. Phys. Ther. 2008, 32, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, R.; Maranesi, E.; Riccardi, G.R.; Donna, V.D.; Pelliccioni, P.; Luzi, R.; Lattanzio, F.; Pelliccioni, G. Non-Immersive Virtual Reality for Rehabilitation of the Older People: A Systematic Review into Efficacy and Effectiveness. J. Clin. Med. 2019, 8, 1882. [Google Scholar] [CrossRef] [Green Version]
- De Luca, R.; Torrisi, M.; Piccolo, A.; Bonfiglio, G.; Tomasello, P.; Naro, A.; Calabrò, R.S. Improving post-stroke cognitive and behavioral abnormalities by using virtual reality: A case report on a novel use of nirvana. Appl. Neuropsychol. Adult 2018, 25, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; De Luca, R.; Molonia, F.; Porcari, B.; Destro, M.; Casella, C.; Salvati, R.; Bramanti, P.; Calabro, R.S. Cognitive rehabilitation in patients with traumatic brain injury: A narrative review on the emerging use of virtual reality. J. Clin. Neurosci. 2019, 61, 1–4. [Google Scholar] [CrossRef]
- Levac, D.; Glegg, S.; Colquhoun, H.; Miller, P.; Noubary, F. Virtual Reality and Active Videogame-Based Practice, Learning Needs, and Preferences: A Cross-Canada Survey of Physical Therapists and Occupational Therapists. Games Health J. 2017, 6, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef]
- Kang, Y.J.; Ku, J.; Han, K.; Kim, S.I.; Yu, T.W.; Lee, J.H.; Park, C.I. Development and clinical trial of virtual reality-based cognitive assessment in people with stroke: Preliminary study. Cyberpsychol. Behav. 2008, 11, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Luque-Moreno, C.; Ferragut-Garcías, A.; Rodríguez-Blanco, C.; Heredia-Rizo, A.M.; Oliva-Pascual-Vaca, J.; Kiper, P.; Oliva-Pascual-Vaca, Á. A Decade of Progress Using Virtual Reality for Poststroke Lower Extremity Rehabilitation: Systematic Review of the Intervention Methods. Biomed Res. Int. 2015, 2015, 342529. [Google Scholar] [CrossRef] [Green Version]
- Bisson, E.; Contant, B.; Sveistrup, H.; Lajoie, Y. Functional balance and dual-task reaction times in older adults are improved by virtual reality and biofeedback training. Cyberpsychol. Behav. 2007, 10, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Chun, M.H.; Son, Y.R. Effect of virtual reality on cognitive dysfunction in patients with brain tumor. Ann. Rehabil. Med. 2014, 38, 726–733. [Google Scholar] [CrossRef] [Green Version]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 11, Cd008349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, Y.W.; Na, D.L.; Han, S.H. A Validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Mercier, L.; Audet, T.; Hebert, R.; Rochette, A.; Dubois, M.F. Impact of motor, cognitive, and perceptual disorders on ability to perform activities of daily living after stroke. Stroke 2001, 32, 2602–2608. [Google Scholar] [CrossRef] [Green Version]
- Crowe, S.F. The differential contribution of mental tracking, cognitive flexibility, visual search, and motor speed to performance on parts A and B of the Trail Making Test. J. Clin. Psychol. 1998, 54, 585–591. [Google Scholar] [CrossRef]
- Seo, E.H.; Lee, D.Y.; Kim, K.W.; Lee, J.H.; Jhoo, J.H.; Youn, J.C.; Choo, I.H.; Woo, J.I. A normative study of the Trail Making Test in Korean elders. Int. J. Geriatr. Psychiatry 2006, 21, 844–852. [Google Scholar] [CrossRef]
- Leung, J.L.; Lee, G.T.; Lam, Y.H.; Chan, R.C.; Wu, J.Y. The use of the Digit Span Test in screening for cognitive impairment in acute medical inpatients. Int. Psychogeriatr. 2011, 23, 1569–1574. [Google Scholar] [CrossRef]
- Watson, M.J. Refining the Ten-metre Walking Test for Use with Neurologically Impaired People. Physiotherapy 2002, 88, 386–397. [Google Scholar] [CrossRef]
- Physiopedia. 10 Metre Walk Test. Available online: https://www.physio-pedia.com/10_Metre_Walk_Test#cite_note-2 (accessed on 26 April 2021).
- Chiong, Y.; Tay, S.S.; Lim, P.A.; Tan, D.M. The effects of toe spreader in people with overactive toe flexors post stroke: A randomized controlled pilot study. Clin. Rehabil. 2013, 27, 90–95. [Google Scholar] [CrossRef]
- Bauer, A.C.M.; Andringa, G. The potential of immersive virtual reality for cognitive training in elderly. Gerontology 2020, 66, 614–623. [Google Scholar] [CrossRef]
- Hwang, J.; Lee, S. The effect of virtual reality program on the cognitive function and balance of the people with mild cognitive impairment. J. Phys. Ther. Sci. 2017, 29, 1283–1286. [Google Scholar] [CrossRef] [Green Version]
- Gamito, P.; Oliveira, J.; Alves, C.; Santos, N.; Coelho, C.; Brito, R. Virtual reality-based cognitive stimulation to improve cognitive functioning in community elderly: A controlled study. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Citri, A.; Malenka, R.C. Synaptic plasticity: Multiple forms, functions, and mechanisms. Neuropsychopharmacology 2007, 33, 18–41. [Google Scholar] [CrossRef] [Green Version]
- Hortsch, M.; Umemori, H. The Sticky Synapse: Cell Adhesion Molecules and Their Role in Synapse Formation and Maintenance; Springer: Dordrecht, The Netherlands, 2009. [Google Scholar]
- Man, D.W.; Chung, J.C.; Lee, G.Y. Evaluation of a virtual reality-based memory training programme for Hong Kong Chinese older adults with questionable dementia: A pilot study. Int. J. Geriatr. Psychiatry 2012, 27, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.N.; Chow, K.Y.; Chan, B.C.; Lam, K.C.; Lee, J.C.; Li, T.H.; Yan, E.W.; Wong, A.T. Usability of a virtual reality environment simulating an automated teller machine for assessing and training persons with acquired brain injury. J. Neuroeng. Rehabil. 2010, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Barcelos, N.; Shah, N.; Cohen, K.; Hogan, M.J.; Mulkerrin, E.; Arciero, P.J.; Cohen, B.D.; Kramer, A.F.; Anderson-Hanley, C. Aerobic and Cognitive Exercise (ACE) Pilot Study for Older Adults: Executive Function Improves with Cognitive Challenge While Exergaming. J. Int. Neuropsychol. Soc. 2015, 21, 768–779. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Stark, J.; Wall, K.M.; VanBrakle, M.; Michel, M.; Maloney, M.; Barcelos, N.; Striegnitz, K.; Cohen, B.D.; Kramer, A.F. The interactive Physical and Cognitive Exercise System (iPACES™): Effects of a 3-month in-home pilot clinical trial for mild cognitive impairment and caregivers. Clin. Interv. Aging 2018, 13, 1565–1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson-Hanley, C.; Barcelos, N.M.; Zimmerman, E.A.; Gillen, R.W.; Dunnam, M.; Cohen, B.D.; Yerokhin, V.; Miller, K.E.; Hayes, D.J.; Arciero, P.J.; et al. The Aerobic and Cognitive Exercise Study (ACES) for Community-Dwelling Older Adults with or At-Risk for Mild Cognitive Impairment (MCI): Neuropsychological, Neurobiological and Neuroimaging Outcomes of a Randomized Clinical Trial. Front. Aging Neurosci. 2018, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- Raichlen, D.A.; Alexander, G.E. Adaptive Capacity: An Evolutionary Neuroscience Model Linking Exercise, Cognition, and Brain Health. Trends Neurosci. 2017, 40, 408–421. [Google Scholar] [CrossRef]
- Bruderer-Hofstetter, M.; Rausch-Osthoff, A.K.; Meichtry, A.; Münzer, T.; Niedermann, K. Effective multicomponent interventions in comparison to active control and no interventions on physical capacity, cognitive function and instrumental activities of daily living in elderly people with and without mild impaired cognition—A systematic review and network meta-analysis. Ageing Res. Rev. 2018, 45, 1–14. [Google Scholar]
- Doniger, G.M.; Beeri, M.S.; Bahar-Fuchs, A.; Gottlieb, A.; Tkachov, A.; Kenan, H.; Livny, A.; Bahat, Y.; Sharon, H.; Ben-Gal, O.; et al. Virtual reality-based cognitive-motor training for middle-aged adults at high Alzheimer’s disease risk: A randomized controlled trial. Alzheimers Dement. 2018, 4, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of Physical Exercise on Cognitive Functioning and Wellbeing: Biological and Psychological Benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef] [PubMed]
- Luger, A.; Deuster, P.A.; Kyle, S.B.; Gallucci, W.T.; Montgomery, L.C.; Gold, P.W.; Loriaux, D.L.; Chrousos, G.P. Acute hypothalamic-pituitary-adrenal responses to the stress of treadmill exercise. Physiologic adaptations to physical training. N. Engl. J. Med. 1987, 316, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Deutsch, J.E.; Merians, A.S.; Adamovich, S.; Poizner, H.; Burdea, G.C. Development and application of virtual reality technology to improve hand use and gait of individuals post-stroke. Restor. Neurol. Neurosci. 2004, 22, 371–386. [Google Scholar] [PubMed]
- Geiger, R.A.; Allen, J.B.; O’Keefe, J.; Hicks, R.R. Balance and mobility following stroke: Effects of physical therapy interventions with and without biofeedback/forceplate training. Phys. Ther. 2001, 81, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Cikajlo, I.; Rudolf, M.; Goljar, N.; Burger, H.; Matjačić, Z. Telerehabilitation using virtual reality task can improve balance in patients with stroke. Disabil. Rehabil. 2012, 34, 13–18. [Google Scholar] [CrossRef]
- Karahan, A.Y.; Tok, F.; Taşkın, H.; Kuçuksaraç, S.; Başaran, A.; Yıldırım, P. Effects of Exergames on Balance, Functional Mobility, and Quality of Life of Geriatrics Versus Home Exercise Programme: Randomized Controlled Study. Cent. Eur. J. Public Health 2015, 23, S14–S18. [Google Scholar]
- Cromwell, R.L.; Newton, R.A.; Forrest, G. Influence of vision on head stabilization strategies in older adults during walking. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M442–M448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobo, A.M. Efeito de um Treinamento em Ambiente Virtual Sobre o Desempenho da Marcha e Funções Cognitivas em Idosos Saudáveis. 2013. Available online: https://www.teses.usp.br/teses/disponiveis/47/47135/tde-30072013-115907/publico/lobo_corrigida.pdf (accessed on 12 April 2021).
- Grau-Pellicer, M.; Chamarro-Lusar, A.; Medina-Casanovas, J.; Serdà Ferrer, B.C. Walking speed as a predictor of community mobility and quality of life after stroke. Top. Stroke Rehabil. 2019, 26, 349–350. [Google Scholar] [CrossRef]


{kind=link}
| Experimental Group (n = 9) | Control Group (n = 9) | |
|---|---|---|
| Number of subject | 9 | 9 |
| Gender (man/woman) | 4:5 | 5:4 |
| Age (year) | 70.1 ± 3.9 | 69.2 ± 4.1 |
| Educational level | ||
| Uneducated | 1 | 1 |
| Elementary school | 2 | 2 |
| Middle School | 4 | 4 |
| High school | 1 | 1 |
| University | 1 | 1 |
| Experimental Group | Control Group | Between Groups p-Values | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Before Treatment | After Treatment | Mean Difference | p-Value | Before Treatment | After Treatment | Mean Difference | p-Value | ||
| K-MMSE | 25.90 (1.79) | 27.00 (2.30) | 1.10 (2.13) | 0.131 | 25.90 (0.99) | 26.60 (1.07) | 0.70 (0.82) | 0.055 | 0.393 |
| TMT-A | 57.54 (19.31) | 49.36 (11.18) | −8.18 (13.84) † | 0.012 * | 56.40 (11.45) | 58.00 (12.65) | 1.60 (5.05) | 0.357 | 0.045 † |
| TMT-B | 204.70 (65.48) | 207.60 (48.00) | 2.90 (59.92) | 0.721 | 204.50 (44.01) | 200.60 (36.52) | −3.90 (12.71) | 0.359 | 0.791 |
| DST-Forward | 3.90 (1.28) | 4.50 (1.50) | 0.60 (1.17) | 0.131 | 3.70 (0.67) | 3.70 (0.94) | 0.00 (0.66) | 1.000 | 0.274 |
| DST-Backward | 2.50 (0.70) | 3.00 (0.66) | 0.50 (0.52) | 0.025 * | 2.60 (0.51) | 2.70 (0.67) | 0.10 (0.56) | 0.564 | 0.012 † |
| TUG | 7.27 (2.81) | 7.78 (1.57) | 0.51 (2.64) | 0.445 | 8.23 (1.15) | 8.14 (0.85) | −0.09 (0.66) | 0.506 | 0.705 |
| 10MWT | 7.98 (1.97) | 6.27 (0.77) | −1.71 (1.92) | 0.028 * | 8.57 (1.12) | 8.00 (0.87) | −0.57 (1.15) | 0.086 | 0.001 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, N.-K.; Choi, J.-B.; Choi, D.-K.; Park, J.-M.; Hong, C.-W.; Park, J.-S.; Yoon, T.-H. Effects of Semi-Immersive Virtual Reality-Based Cognitive Training Combined with Locomotor Activity on Cognitive Function and Gait Ability in Community-Dwelling Older Adults. Healthcare 2021, 9, 814. https://doi.org/10.3390/healthcare9070814
Hwang N-K, Choi J-B, Choi D-K, Park J-M, Hong C-W, Park J-S, Yoon T-H. Effects of Semi-Immersive Virtual Reality-Based Cognitive Training Combined with Locomotor Activity on Cognitive Function and Gait Ability in Community-Dwelling Older Adults. Healthcare. 2021; 9(7):814. https://doi.org/10.3390/healthcare9070814
Chicago/Turabian StyleHwang, Na-Kyoung, Jong-Bae Choi, Dae-Kil Choi, Jae-Min Park, Chang-Wan Hong, Ji-Su Park, and Tae-Hyung Yoon. 2021. "Effects of Semi-Immersive Virtual Reality-Based Cognitive Training Combined with Locomotor Activity on Cognitive Function and Gait Ability in Community-Dwelling Older Adults" Healthcare 9, no. 7: 814. https://doi.org/10.3390/healthcare9070814