
Development and Preliminary Validation of LoAD Calc, a Mobile App for Calculating the Maximum Safe Single Dose of Local Anesthetics

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
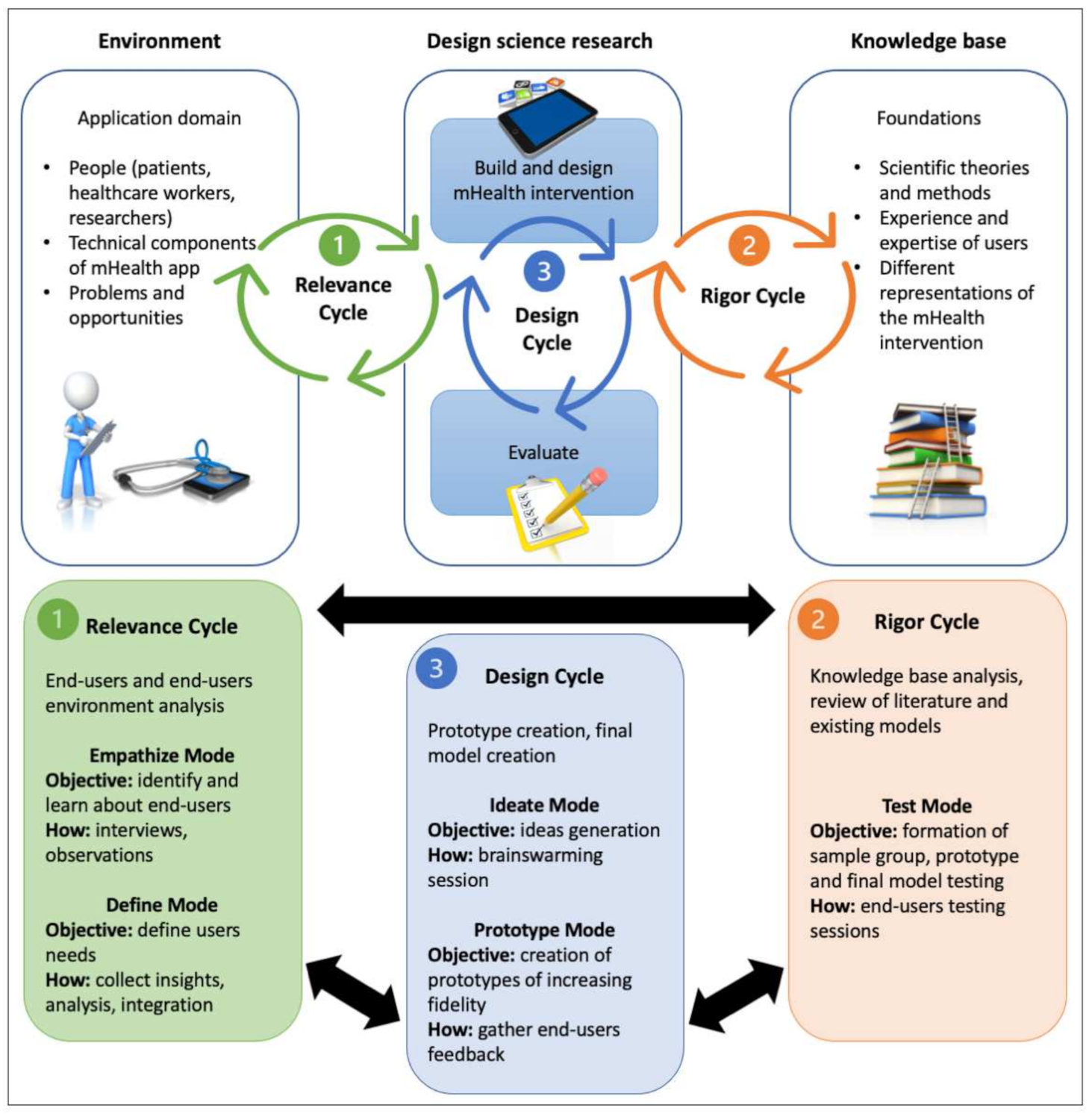
2.1. General Design
2.2. Relevance Cycle
2.2.1. Empathize Mode
2.2.2. Define Mode
2.3. Rigor Cycle
Test Mode
2.4. Design Cycle
2.4.1. Ideate Mode
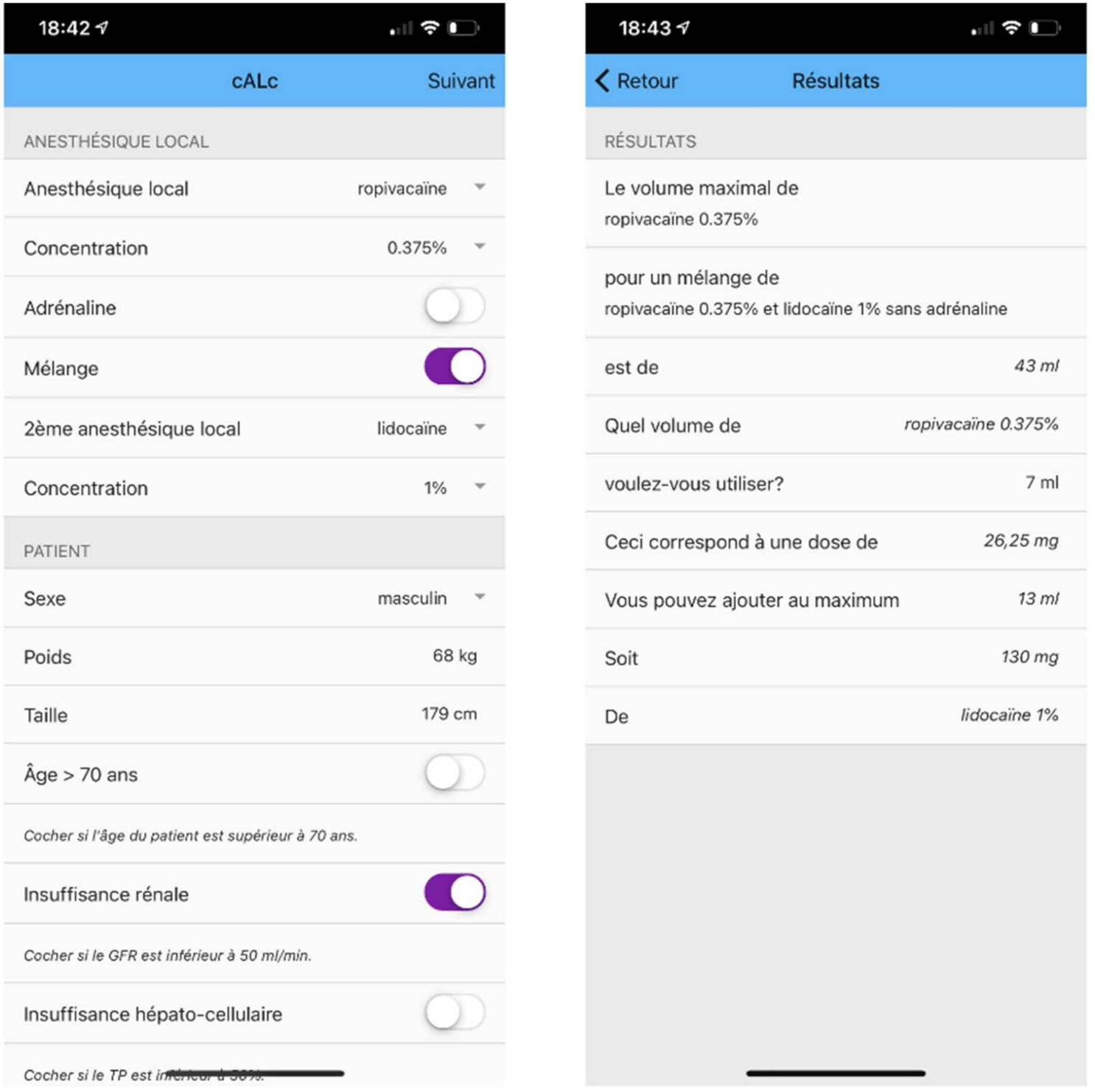
2.4.2. Prototype Mode
3. Results
3.1. Relevance Cycle
3.1.1. Empathize Mode
3.1.2. Define Mode
3.2. Rigor Cycle
Test Mode
3.3. Design Cycle
3.3.1. Ideate Mode
3.3.2. Prototype Mode
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ganzberg, S.; Kramer, K.J. The Use of Local Anesthetic Agents in Medicine. Dent. Clin. N. Am. 2010, 54, 601–610. [Google Scholar] [CrossRef]
- Dickerson, D.M.; Apfelbaum, J.L. Local anesthetic systemic toxicity. Aesthet. Surg. J. 2014, 34, 1111–1119. [Google Scholar] [CrossRef] [Green Version]
- Neal, J.M.; Barrington, M.J.; Fettiplace, M.R.; Gitman, M.; Memtsoudis, S.G.; Mörwald, E.E.; Rubin, D.S.; Weinberg, G. The Third American Society of Regional Anesthesia and Pain Medicine Practice Advisory on Local Anesthetic Systemic Toxicity: Executive Summary 2017. Reg. Anesth. Pain Med. 2018, 43, 113–123. [Google Scholar] [CrossRef] [Green Version]
- Gitman, M.; Barrington, M.J. Local Anesthetic Systemic Toxicity: A Review of Recent Case Reports and Registries. Reg. Anesth. Pain Med. 2018, 43, 124–130. [Google Scholar] [CrossRef]
- Rosenberg, P.H.; Veering, B.T.; Urmey, W.F. Maximum recommended doses of local anesthetics: A multifactorial concept. Reg. Anesth. Pain Med. 2004, 29, 564–575. [Google Scholar] [CrossRef]
- Williams, D.J.; Walker, J.D. A nomogram for calculating the maximum dose of local anaesthetic. Anaesthesia 2014, 69, 847–853. [Google Scholar] [CrossRef]
- Baumann, D.; Dibbern, N.; Sehner, S.; Zöllner, C.; Reip, W.; Kubitz, J.C. Validation of a mobile app for reducing errors of administration of medications in an emergency. J. Clin. Monit. Comput. 2019, 33, 531–539. [Google Scholar] [CrossRef]
- Siebert, J.N.; Ehrler, F.; Combescure, C.; Lacroix, L.; Haddad, K.; Sanchez, O.; Gervaix, A.; Lovis, C.; Manzano, S. A Mobile Device App to Reduce Time to Drug Delivery and Medication Errors during Simulated Pediatric Cardiopulmonary Resuscitation: A Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e31. [Google Scholar] [CrossRef]
- Peiffer-Smadja, N.; Poda, A.; Ouedraogo, A.S.; Guiard-Schmid, J.B.; Delory, T.; Le Bel, J.; Bouvet, E.; Lariven, S.; Jeanmougin, P.; Ahmad, R.; et al. Paving the way for the implementation of a decision support system for antibiotic prescribing in primary care in west Africa: Preimplementation and co-design workshop with physicians. J. Med. Internet Res. 2020, 22, e17940. [Google Scholar] [CrossRef]
- Farao, J.; Malila, B.; Conrad, N.; Mutsvangwa, T.; Rangaka, M.X.; Douglas, T.S. A user-centred design framework for mHealth. Schnall, R.; editor. PLoS ONE 2020, 15, e0237910. [Google Scholar] [CrossRef]
- Roberts, J.P.; Fisher, T.R.; Trowbridge, M.J.; Bent, C. A design thinking framework for healthcare management and innovation. Healthcare 2016, 4, 11–14. [Google Scholar] [CrossRef]
- Hevner, A.R. A Three Cycle View of Design Science Research. Scand. J. Inf. Syst. 2007. Available online: https://www.uio.no/studier/emner/jus/afin/FINF4002/v13/hefner-design.pdf (accessed on 10 September 2020).
- Razzouk, R.; Shute, V. What Is Design Thinking and Why Is It Important? Rev. Educ. Res. 2012, 82, 330–348. [Google Scholar] [CrossRef] [Green Version]
- McCaffrey, T. Why You Should Stop Brainstorming. 2014. Available online: https://hbr.org/2014/03/why-you-should-stop-brainstorming (accessed on 27 September 2020).
- MDCalc Local Anesthetic Dosing Calculator. Available online: https://www.mdcalc.com/local-anesthetic-dosing-calculator#next-steps (accessed on 27 September 2020).
- The Podiatry Institute. LA Toxic Dose Calculator. Available online: http://www.podiatryinstitute.com/Local_Anesthetic_Toxic_Dose_Calculator.xls (accessed on 27 September 2020).
- Johns Hopkins Digital. SafeLocal. Available online: https://apps.apple.com/us/app/safelocal/id1440999841 (accessed on 27 September 2020).
- Waldinger, R.; Weinberg, G.; Gitman, M. Local Anesthetic Toxicity in the Geriatric Population. Drugs Aging 2020, 37, 1–9. [Google Scholar] [CrossRef] [PubMed]
- French, J.; Sharp, L.M. Local anaesthetics. Ann. R. Coll. Surg. Engl. 2012, 94, 76–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinakar, P.; Gerner, P. Clinical Applications of Local Anesthetics; Vacanti, C.A., Sikka, P., Urman, R., Segal, B.S., Eds.; Cambridge University Press: Cambridge, UK, 2020; pp. 288–294. [Google Scholar] [CrossRef]
- Wadlund, D.L. Local anesthetic systemic toxicity. AORN J. 2017, 106, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Devine, B.J. Clinical Pharmacy: Case Studies. Drug Intell. Clin. Pharm. 1974, 8, 650–655. [Google Scholar] [CrossRef]
- Abernethy, D.R.; Greenblatt, D.J. Lidocaine disposition in obesity. Am. J. Cardiol. 1984, 53, 1183–1186. [Google Scholar] [CrossRef]
- El-Boghdadly, K.; Chin, K.J. Local anesthetic systemic toxicity: Continuing Professional Development. Can. J. Anesth Can. d’anesthésie 2016, 63, 330–349. [Google Scholar] [CrossRef] [Green Version]
- Munson, E.S.; Paul, W.L.; Embro, W.J. Central-nervous-system toxicity of local anesthetic mixtures in monkeys. Anesthesiology 1977, 46, 179–183. [Google Scholar] [CrossRef]
- Becker, D.E.; Reed, K.L. Local anesthetics: Review of pharmacological considerations. Anesth. Prog. 2012, 59, 90–102. [Google Scholar] [CrossRef] [Green Version]
- Hou, I.-C.; Lan, M.-F.; Shen, S.-H.; Tsai, P.Y.; Chang, K.J.; Tai, H.-C.; Tsai, A.-J.; Chang, P.; Wang, T.-F.; Sheu, S.-J.; et al. The Development of a Mobile Health App for Breast Cancer Self-Management Support in Taiwan: Design Thinking Approach. JMIR mHealth uHealth 2020, 8, e15780. [Google Scholar] [CrossRef] [PubMed]
- Korpershoek, Y.J.G.; Hermsen, S.; Schoonhoven, L.; Schuurmans, M.J.; Trappenburg, J.C.A. User-Centered Design of a Mobile Health Intervention to Enhance Exacerbation-Related Self-Management in Patients with Chronic Obstructive Pulmonary Disease (Copilot): Mixed Methods Study. J. Med. Internet Res. 2020, 22, e15449. [Google Scholar] [CrossRef] [PubMed]
- DeLuke, D.M.; Cannon, D.; Carrico, C.; Byrne, B.E.; Laskin, D.M. Is Maximal Dosage for Local Anesthetics Taught Consistently Across, U.S. Dental Schools? A National Survey. J. Dent. Educ. 2018, 82, 621–624. [Google Scholar] [CrossRef] [PubMed]
- Committee, S.; Society, J. Practical guide for the management of systemic toxicity caused by local anesthetics. J. Anesth. 2019, 33, 1–8. [Google Scholar]
- O’Donnell, B.D.; Iohom, G. An Estimation of the Minimum Effective Anesthetic Volume of 2% Lidocaine in Ultrasound-guided Axillary Brachial Plexus Block. Anesthesiology 2009, 111, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riazi, S.; Carmichael, N.; Awad, I.; Holtby, R.M.; McCartney, C.J.L. Effect of local anaesthetic volume (20 vs. 5 mL) on the efficacy and respiratory consequences of ultrasound-guided interscalene brachial plexus block. Br. J. Anaesth. 2008, 101, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Neal, J.M.; Hsiung, R.L.; Mulroy, M.F.; Halpern, B.B.; Dragnich, A.D.; Slee, A.E. ASRA checklist improves trainee performance during a simulated episode of local anesthetic systemic toxicity. Reg. Anesth. Pain Med. 2012, 37, 8–15. [Google Scholar] [CrossRef]
- Mahajan, A.; Derian, A. Local Anesthetic Toxicit; StatPearls: Treasure Island, CA, USA, 2019. [Google Scholar]
- Schild, S.; Sedlmayr, B.; Schumacher, A.-K.; Sedlmayr, M.; Prokosch, H.-U.; St Pierre, M. German Cognitive Aid Working Group. A Digital Cognitive Aid for Anesthesia to Support Intraoperative Crisis Management: Results of the User-Centered Design Process. JMIR mHealth uHealth 2019, 7, e13226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, J.D.; Williams, N.; Williams, D.J. The accuracy of timed maximum local anaesthetic dose calculations with an electronic calculator, nomogram, and pen and paper. Anaesthesia 2017, 72, 760–764. [Google Scholar] [CrossRef] [Green Version]
- Sagir, A.; Goyal, R. An assessment of the awareness of local anesthetic systemic toxicity among multi-specialty postgraduate residents. J. Anesth. 2015, 29, 299–302. [Google Scholar] [CrossRef]
- Cooper, B.R.; Moll, T.; Griffiths, J.R. Local anaesthetic toxicity: Are we prepared for the consequences in the Emergency Department? Emerg. Med. J. 2010, 27, 599–602. [Google Scholar] [CrossRef] [PubMed]
- Ennezat, P.-V.; Cosgrove, S.; Bouvaist, H.; Maréchaux, S.; Guerbaai, R.-A.; Le Jemtel, T.; Andréjak, M.; Vital-Durand, D. From evidence-based medicine to personalized medicine, with particular emphasis on drug-safety monitoring. Arch. Cardiovasc. Dis. 2017, 110, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Swiss Confederation. Medical Devices Ordinance (MedDO). 2020. Available online: https://www.admin.ch/opc/en/classified-compilation/19995459/202008010000/812.213.pdf (accessed on 10 September 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Open-Ended Questions | Specific Questions |
|---|---|
| In what context do you use local anesthetics? | For what kind of procedures do you use LAs? |
| Which LAs do you routinely use? | |
| Do you use LA mixtures? If yes, do you use ratios other than 1:1? | |
| How do you determine LA1 dosage in your actual practice? | Are there specific rules or tools you know of? |
| Do you use any of these rules or tools? | |
| Do you take patient comorbidities into account? | |
| According to you, are current rules and tools satisfactory? If no, what are the shortcomings you have identified? Is there a solution you would think about? | |
| Do you carry a smartphone while at work? | Is it a personal or professional device? |
| Are any medical apps installed on your device? | |
| If yes, are you comfortable using these apps? | |
| Do you think that a mobile app regarding LA dosage calculation could be useful in your daily practice? If yes, what features would you expect, and which of these features would you consider mandatory? | |
| Is there anything else you would like to add? |
| Tool | Strengths | Weaknesses |
|---|---|---|
| Nomogram [6] | No need for calculation Users are instructed to use IBW 1 for calculation Limitation of body weight entry Limitation of volume for the mixture | Accessibility No dose adaptation based on health conditions and drug interactions |
| MDCalc Local Anesthetic Dosing Calculator (online/app) [15] | Accessibility Limitation of body weight entry | Use of actual body weight for calculation No warning is given if the calculated dose exceeds the maximum safe dose No mixture calculation No dose adaptation based on health conditions and drug interactions |
| The Podiatry Institute’s LA 2 Toxic Dose Calculator (Excel spreadsheet) [16] | Computer-based Volume for 1:1 mixture Maximum volumes indicated | Use of actual body weight for calculation Not easily usable on a smartphone No warning is given if the calculated dose exceeds the maximum safe dose No dose adaptation based on health conditions and drug interactions |
| SafeLocal mobile app by Johns Hopkins Digital [17] | Accessibility Mixture calculation Maximum dosage is adapted according to certain relevant comorbidities | Use of actual body weight for calculation No limitation of value entries (i.e., no maximum body weight defined) No warning is given if the calculated dose exceeds the maximum safe dose |
| Dosage Element | Knowledge Classification | Commentary | Inclusion(Y 1/N 2) | App Rules |
|---|---|---|---|---|
| Dose limit for a single LA 3 | Known [18,19,20] | Slight variations of maximum LA dosage. Choice of safer (lower) dosage. | Y | Levobupivacaine: 2 mg/kg (max 150 mg/dose) Lidocaine: 3 mg/kg (max 300 mg/dose) Ropivacaine: 3 mg/kg (max 225 mg/dose) |
| Influence of epinephrine on dose limit | Known [18,19,20] | Slight variations of maximum LA dosage in the presence of epinephrine. Choice of safer (lower) dosage. | Y | Levobupivacaine: 3 mg/kg (max 150 mg/dose) Lidocaine: 7 mg/kg (max 400 mg/dose) Ropivacaine: 3 mg/kg (max 225 mg/dose) |
| Influence of other adjuvants | Unknown | Some supposed effects, but unclear if maximum LA dose should be adapted. | N | None |
| Influence of injection site | Unknown [5,21] | Better and faster absorption if the injection site is well perfused, but no algorithm defined yet to adapt maximum LA dose calculation. | N | None |
| Determination of Calculation Weight | Unclear [6,22,23] | Exact formula and limits for LA dose calculation are not clearly defined. | Y | 1. Calculation of BMI 4; 2. Calculation of IBW 5 (Devine Formula); 3. Application of the following algorithm to define CW 6:
|
| Dose adaptation depending on health conditions/drugs | Unclear [5,24] | Some uncomplete indications in the literature, especially after repeated administration. | Y | Conditions:
If two or more conditions are present, the calculator reduces the total maximum dose by 30%. |
| Calculation rule for LA mixtures | Unclear [19,25] | General rule for calculation of LA mixtures. Unclear if there could be a synergistic effect. | Y | The app performs the following steps: 1. Calculation of maximum safe volume for first LA; 2. The user enters which volume of first LA is to be used (0–maximum volume); 3. Calculation of corresponding maximum dose of first LA and determination of the percentage of total maximum dose; 4. Calculation of maximum dose of second LA-based on remaining percentage of total maximum dose; 5. Calculation of maximum volume of second LA. |
| Time-dependent maximum dosage | Unclear [26] | Should be adaptable from known data, but too many parameters considered unknown or unclear to be included at this stage. | N | None |
| Concept | Goal | Solution |
|---|---|---|
| Dependent dropdown menus for concentration selection | Force selection of correct concentration for a given LA 1. Avoid unusual mixtures and inattention errors. | Only usual concentrations for chosen LA shown in the dependent dropdown. Dependent dropdown resets if LA is changed. |
| Conditional appearance of 2nd set of dropdown menus | Avoid unnecessary information on the screen. | Second set of dropdowns not visible if mixture toggle button is “on”. |
| Limited selection of 2nd LA | Avoid performing an unnecessary mixture calculation. Avoid invalid data input. | Error message displayed when both selected LAs are identical, and calculation is impossible. |
| Mandatory unique sex selection | Force sex selection. Avoid error in IBW 2 calculation. | If sex is not selected, an error message stays on the screen and calculation is impossible Only one selection is possible (male or female) |
| Number-only character-limited input fields for height and weight | Avoid calculation error Avoid invalid data input. | Input field and contextual keyboard-only allow numbers to be entered. Input limitation of maximum three characters. |
| Value limitations for height and weight | Avoid invalid data input. | Minimum and maximum values setting for the input fields, if a value outside limits error message is displayed and calculation is impossible. |
| Scrolling screen | Facilitate main page design and navigation | User can scroll the whole screen to see all the fields. |
| Reset button | Facilitate voiding of the form for new calculation. | Reset button to void all fields Refocus on top of the form page on pressing. |
| Conditional calculation | Avoid calculation errors. | Calculation only possible when all fields are filled, and no error message is displayed. |
| Conditional navigation to results pages | Avoid specific unnecessary tasks Allow better adaptation of results page depending on type of calculation (simple or mixture). | Navigation to a different results page, depending on the state of the mixture toggle button |
| Conditional display of 2nd part of mixture results | Avoid unnecessary information on the screen. | If no volume of first LA is entered, the proposed volume of second LA is not displayed. |
| Value limitation for chosen volume of 1st LA | Avoid display of invalid data. Avert miscomprehension for the user. | Entered volume must be between 0 and maximum allowed volume (displayed on-screen); if not, an error message is displayed. |
| Rounding of clinically usable values | Avert miscomprehension for the user Increase safety. | All given volumes are floored to inferior integer. |
| Problem | Explanation | Correction |
|---|---|---|
| Misplacement of the “Calculate” button | Users found it was more logical to have the “Reset” button on the left and the “Calculate” button on the right. | Exchange of buttons placement. |
| Keyboard remained visible after entering data in the number field | This issue was found unpractical by users as the keyboard covers part of the screen. | Ability to make the keyboard disappear by defocusing. |
| Data disappeared when pressing “back” button from the results page | Users found it would be more convenient to keep the data already entered when pressing the “Back” button on the results page as it allows to modify only chosen parameters. | Data in the form are still visible when pressing the “Back” button from the results page; If the “Reset” button is pressed on the results page, it brings the user back to a blank form. |
| Calculation weight and LA 1 maximum dosage (mg/kg) unknown | Users wanted these two parameters to be indicated so that they could better understand and redo the calculations. | Calculation weight and LA maximum dosage in mg/kg were made visible on the results pages. |
| Too much information under the “Drugs” checkbox | Users found that the whole list of drugs decreasing LA metabolism was too long and difficult to read. Moreover, this list could slightly differ depending on the chosen LA. | Information button icon added under the checkbox. On pressing, it shows a list of relevant drugs decreasing LA metabolism for the chosen LA. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suppan, M.; Beckmann, T.S.; Gercekci, C.; Sigrist, T.; Savoldelli, G.L.; Fournier, R.; Samer, C.F. Development and Preliminary Validation of LoAD Calc, a Mobile App for Calculating the Maximum Safe Single Dose of Local Anesthetics. Healthcare 2021, 9, 799. https://doi.org/10.3390/healthcare9070799
Suppan M, Beckmann TS, Gercekci C, Sigrist T, Savoldelli GL, Fournier R, Samer CF. Development and Preliminary Validation of LoAD Calc, a Mobile App for Calculating the Maximum Safe Single Dose of Local Anesthetics. Healthcare. 2021; 9(7):799. https://doi.org/10.3390/healthcare9070799
Chicago/Turabian StyleSuppan, Mélanie, Tal Sarah Beckmann, Cenan Gercekci, Thérèse Sigrist, Georges Louis Savoldelli, Roxane Fournier, and Caroline Flora Samer. 2021. "Development and Preliminary Validation of LoAD Calc, a Mobile App for Calculating the Maximum Safe Single Dose of Local Anesthetics" Healthcare 9, no. 7: 799. https://doi.org/10.3390/healthcare9070799