
Ultrasound-Guided Anterior Mediastinotomy: A Feasible Tool for Critical Lymphoma Patients

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
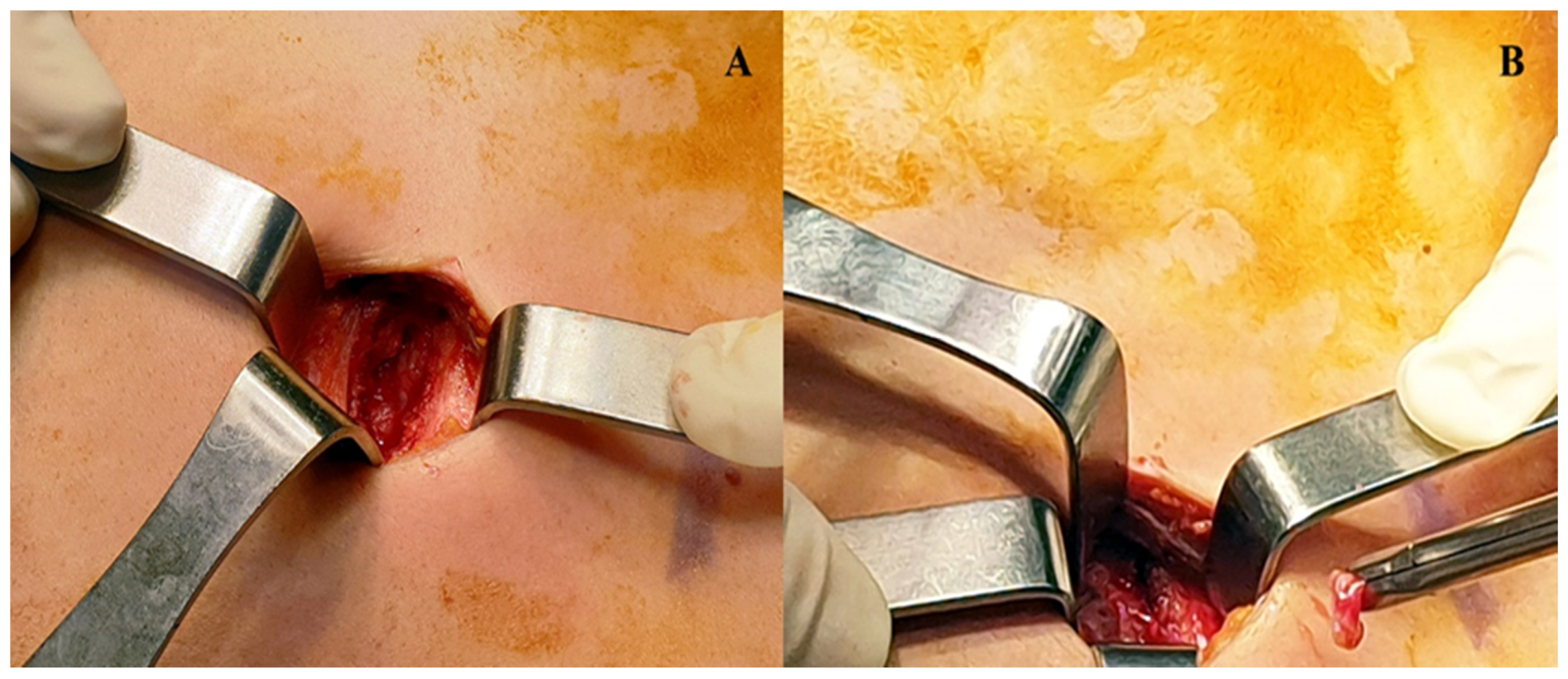
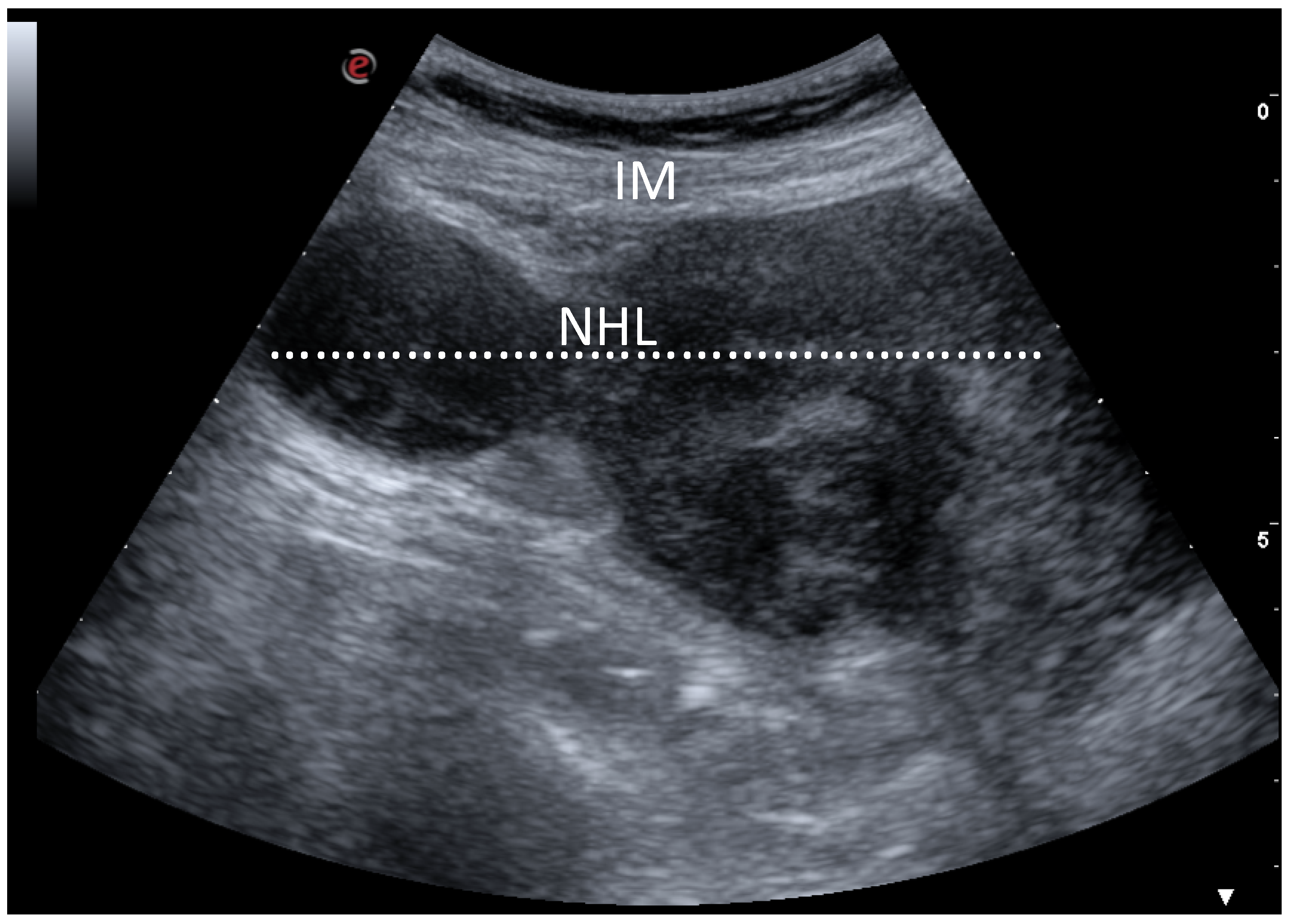
Ultrasonography and Surgical Procedure
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McNeill, T.M.; Chamberlain, J.M. Diagnostic Anterior Mediastinotomy. Ann. Thorac. Surg. 1966, 2, 532–539. [Google Scholar] [CrossRef]
- Dreyling, M.; Campo, E.; Hermine, O.; Jerkeman, M.; Le Gouill, S.; Rule, S.; Shpilberg, O.; Walewski, J.; Ladetto, M. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv62–iv71. [Google Scholar] [CrossRef]
- Duwe, B.V.; Sterman, D.H.; Musani, A.I. Tumors of the mediastinum. Chest 2005, 128, 2893–2909. [Google Scholar] [CrossRef]
- Carter, B.W.; Marom, E.M.; Detterbeck, F.C. Approaching the patient with an anterior mediastinal mass: A guide for clinicians. J. Thorac. Oncol. 2014, 9, S102–S109. [Google Scholar] [CrossRef] [Green Version]
- Plönes, T.; Mardanzai, K.; Gafencu, D.; Viehof, J.; Hager, T.; Theegarten, D.; Dührsen, U.; Darwiche, K.; Taube, C.; Aigner, C. Cytology Versus Histology in the Primary Diagnosis of Lymphoma Located in the Mediastinum. Ann. Thorac. Surg. 2019, 108, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Sica, A.; Santagata, M.; Sagnelli, C.; Rambaldi, P.; Franco, R.; Creta, M.; Vitiello, P.; Caccavale, S.; Tammaro, V.; Sagnelli, E.; et al. Primary Extra-Nodal DLBCL of Glands: Our Experiences outside Guidelines of Treatment. Healthcare 2021, 9, 286. [Google Scholar] [CrossRef] [PubMed]
- Sica, A.; Sagnelli, C.; Vitiello, P.; Franco, R.; Argenziano, G.; Ciccozzi, M.; Sagnelli, E.; Ronchi, A. Rescue therapy of refractory DLBCL BCL2 with venetoclax: Case report. Chemotherapy 2020, 1–5. [Google Scholar] [CrossRef]
- Sica, A.; Sagnelli, C.; Casale, B.; Svanera, G.; Creta, M.; Calogero, A.; Franco, R.; Sagnelli, E.; Ronchi, A. How Fear of COVID-19 Can Affect Treatment Choices for Anaplastic Large Cell Lymphomas ALK+ Therapy: A Case Report. Healthcare 2021, 9, 135. [Google Scholar] [CrossRef]
- Sica, A.; De Rimini, M.L.; Sagnelli, C.; Casale, B.; Spada, A.; Reginelli, A.; Amarelli, C.; Maiello, C.; Belfiore, M.P.; Massimiliano, C.; et al. Post Heart Transplantation Lymphoproliferative Diseases (PLDs) and the diagnostic role of [18f] FDG- PET/CT. Minerva Med. 2020. [Google Scholar] [CrossRef]
- Sica, A.; Vitiello, P.; Caccavale, S.; Sagnelli, C.; Calogero, A.; Doraro, C.A.; Pastore, F.; Ciardiello, F.; Argenziano, G.; Reginelli, A.; et al. PrimaryCutaneous DLBCL Non-GCB Type: Challenges of a Rare Case. Open Med. 2020, 15, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Sica, A.; Casale, B.; Sagnelli, C.; Di Dato, M.T.; Buonavolontà, P.; Salzano, A.M.; Sagnelli, E.; Famiglietti, V.; Saracco, E.; Tammaro, D.; et al. All-in-One Spinal Cord Stimulation in Lymphoproliferative Diseases. Front Neurol. 2020, 11, 550554. [Google Scholar] [CrossRef]
- Ronchi, A.; Zito Marino, F.; Vitiello, P.; Caccavale, S.; Argenziano, G.; Crisci, S.; Franco, R.; Sica, A. A case of primarycutaneous B-celllymphoma with immature features in an old man. Diffuse Large B-cell Lymhpoma with immature features or B-cell Lymhpoblastic Lymphoma? J. Cutan. Pathol. 2020. [Google Scholar] [CrossRef]
- Visco, C.; Di Rocco, A.; Evangelista, A.; Quaglia, F.M.; Tisi, M.C.; Morello, L.; Zilioli, V.R.; Rusconi, C.; Hohaus, S.; Sciarra, R.; et al. Outcomes in first relapsed-refractory younger patients with mantle cell lymphoma: Results from the MANTLE-FIRST study. Leukemia 2021. [Google Scholar] [CrossRef] [Green Version]
- Pirsaharkhiz, N.; Comolli, K.; Fujiwara, W.; Stasiewicz, S.; Boyer, J.M.; Begin, E.V.; Rubinstein, A.J.; Henderson, H.R.; Lazar, J.F.; Watson, T.J.; et al. Utility of erectorspinaeplaneblock in thoracic surgery. J. Cardiothorac. Surg. 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Cascone, R.; Sica, A.; Sagnelli, C.; Carlucci, A.; Calogero, A.; Santini, M.; Fiorelli, A. Endoscopic Treatment and Pulmonary Rehabilitation for Management of Lung Abscess in Elderly Lymphoma Patients. Int. J. Environ. Res. Public Health 2020, 17, 997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armitage, J.O.; Gascoyne, R.D.; Lunning, M.A.; Cavalli, F. Non-Hodgkin lymphoma. Lancet 2017, 390, 298–310. [Google Scholar] [CrossRef]
- Ronchi, A.; Caputo, A.; Pagliuca, F.; Montella, M.; Marino, F.Z.; Zeppa, P.; Franco, R.; Cozzolino, I. Lymphonode fine need leaspirationcytology (FNAC) in paediatric patients: Why not? Diagnostic accuracy of FNAC in a series of heterogeneous paediatric lymphadenopathies. Pathol. Res. Pract. 2021, 217. [Google Scholar] [CrossRef]
- Sud, A.; Thomsen, H.; Law, P.J.; Försti, A.; Filho, M.I.D.S.; Holroyd, A.; Broderic, K.P.; Orlando, G.; Lenive, O.; Wright, L.; et al. Genome-wide association study of classical Hodgkin lymphoma identifies key regulators of disease susceptibility. Nat. Commun. 2017, 8, 1892. [Google Scholar] [CrossRef] [Green Version]
- Aoki, T.; Chong, L.C.; Takata, K.; Milne, K.; Hav, M.; Colombo, A.; Chavez, E.A.; Nissen, M.; Wang, X.; Miyata-Takata, T.; et al. Single-Cell Transcriptome Analysis Reveals Disease-Defining T-cell Subsets in the Tumor Microenvironment of Classic Hodgkin Lymphoma. Cancer Discov. 2020, 10, 406–421. [Google Scholar] [CrossRef] [Green Version]
- Sica, A.; Vitiello, P.; Ronchi, A.; Casale, B.; Calogero, A.; Sagnelli, E.; Costa Nachtigal, G.; Troiani, T.; Franco, R.; Argenziano, G.; et al. Primary Cutaneous Anaplastic Large Cell Lymphoma (pcALCL) in elderly, the importance of a sport activity training. Int. J. Environ. Res. Public Health 2020, 17, 839. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; Min, Q.; Wang, J.Y. B Cell Lymphoma. Adv. Exp. Med. Biol. 2020, 1254, 161–181. [Google Scholar]
- Petroianu, A.; Alberti, L.R.; Orsi, V.L.; Viana, F.C.T.; Moura, C.B. Etiopathogenic, epidemiologic and clinical-therapeutic comparison of Non-Hodgkin’s Lymphoma and Kaposi’s Sarcoma. Arq. Bras. Cir. Dig. 2020, 33, e1521. [Google Scholar] [CrossRef] [PubMed]
- Gerrard, M.; Waxman, I.M.; Sposto, R.; Auperin, A.; Perkins, S.L.; Goldman, S.; Harrison, L.; Pinkerton, R.; McCarthy, K.; Raphael, M.; et al. French-American-British/Lymphome Malins de Burkit 96 (FAB/LMB 96) International Study Committee. Outcome and pathologic classification of children and adolescents with mediastinal large B-cell lymphoma treated with FAB/LMB96 mature B-NHL therapy. Blood 2013, 121, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Bennani, N.N.; Feldman, A.L. Lymphoma classification update: B-cell non-Hodgkin lymphomas. Expert Rev. Hematol. 2017, 10, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Mugnaini, E.N.; Ghosh, N. Lymphoma. Prim. Care 2016, 43, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, E.S. Diagnosis and classification of lymphoma: Impact of technical advances. Semin. Hematol. 2019, 56, 30–36. [Google Scholar] [CrossRef]
- Jiang, M.; Bennani, N.N.; Feldman, A.L. Lymphoma classification update: T-cell lymphomas, Hodgkin lymphomas, and histiocytic/dendritic cell neoplasms. Expert Rev. Hematol. 2017, 10, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Swerdlow, S.H.; Cook, J.R. As the world turns, evolving lymphoma classifications-past, present and future. Hum. Pathol. 2020, 95, 55–77. [Google Scholar] [CrossRef]
- Lynch, R.C.; Gratzinger, D.; Advani, R.H. Clinical Impact of the 2016 Update to the WHO Lymphoma Classification. Curr. Treat. Options Oncol. 2017, 18, 45. [Google Scholar] [CrossRef]
- Sica, A.; Sagnelli, C.; Papa, A.; Ciccozzi, M.; Sagnelli, E.; Calogero, A.; Martinelli, E.; Casale, B. An Anecdotal Case Report of Chronic Lymphatic Leukemia with del (11q) Treated with Ibrutinib: Artificial Nourishment and Physical Activity Program. Int. J. Environ. Res. Public Health 2020, 17, 1929. [Google Scholar] [CrossRef] [Green Version]
- Ferry, J.A. Scientific Advances and the Evolution of Diagnosis, Subclassification and Treatment of Lymphoma. Arch. Med. Res. 2020, 51, 749–764. [Google Scholar] [CrossRef]
- Capece, M.; Creta, M.; Calogero, A.; La Rocca, R.; Napolitano, L.; Barone, B.; Sica, A.; Fusco, F.; Santangelo, M.; Dodaro, C.; et al. Does physical activity regulate prostate carcinogenesis and prostate canceroutcomes? A narrative review. Int. J. Environ. Res. Public Health 2020, 17, 1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankland, K.R.; Armitage, J.O.; Ancock, B.W. Non-Hodgkin lymphoma. Lancet 2012, 380, 848–857. [Google Scholar] [CrossRef]
- Piña-Oviedo, S.; Moran, C.A. Primary Mediastinal Nodal and Extranodal Non-Hodgkin Lymphomas: Current Concepts, Historical Evolution, and Useful Diagnostic Approach: Part 1. Adv. Anat. Pathol. 2019, 26, 346–370. [Google Scholar] [CrossRef] [PubMed]
- Petranovic, M.; Gilman, M.D.; Muniappan, A.; Hasserjian, R.P.; Digumarthy, S.R.; Muse, V.V.; Sharma, A.; Shepard, J.A.O.; Wu, C.C. Diagnostic yield of CT-guided percutaneous transthoracic needle biopsy for diagnosis of anterior mediastinal masses. Am. J. Roentgenol. 2015, 205, 774–779. [Google Scholar] [CrossRef]
- Iguchi, T.; Hiraki, T.; Matsui, Y.; Fujiwara, H.; Sakurai, J.; Masaoka, Y.; Uka, M.; Tanaka, T.; Gobara, H.; Kanazawa, S. CT fluoroscopy-guided core needle biopsy of anterior mediastinal masses. Diagn. Interv. Imaging 2018, 99, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Seaberg, K.; Wallace, M.J.; Madoff, D.C.; Morello, F.A.; Ahrar, K.; Murthy, R.; Hicks, M. EImaging-guided percutaneous biopsy of mediastinal lesions: Different approaches and anatomic considerations. Radiographic 2005, 25, 763–786. [Google Scholar] [CrossRef] [Green Version]
- Tacconi, F.; Rogliani, P.; Cristino, B.; Gilardi, F.; Palombi, L.; Pompeo, E. Minimalist video-assisted thoracic surgery biopsy of mediastinal tumors. J. Thorac. Dis. 2016, 8, 3704–3710. [Google Scholar] [CrossRef] [Green Version]
- Erdös, G.; Tzanova, I. Perioperative anaesthetic management of mediastinal mass in adults. Eur. J. Anaesthesiol. 2009, 26, 627–632. [Google Scholar] [CrossRef]
- Galvez, C.; Galiana, M.; Corcoles, J.M.; Lirio, F.; Sesma, J.; Bolufer, S. Current anesthesiological approach to mediastinal surgery. J. Vis. Surg. 2018, 4, 146. [Google Scholar] [CrossRef]
- Li, W.W.L.; Van Boven, W.P.; Annema, J.T.; Eberl, S.; Klomp, H.M.; de Mol, B.A.J.M. Management of large mediastinal masses: Surgical and anesthesiological considerations. J. Thorac. Dis. 2016, 8, E175–E184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sica, A.; Casale, B.; Sagnelli, C.; Di Dato, M.T.; Rispoli, M.; Santagata, M. Chronic Chest Pain Control after Trans-Thoracic Biopsy in Mediastinal Lymphomas. Healthcare 2021, 9, 589. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery after Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardio Thorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | |
|---|---|
| Number of patients | 13 |
| Age, years (M ± SD) | 55.69 ± 19.11 |
| Male sex, N° (%) | 8 (61.5) |
| Comorbidity, N° (%): | |
| COPD | 6 (46.2) |
| Cardiac | 6 (46.2) |
| Diabetes mellitus | 5 (38.5) |
| Functional tests (M ± SD) | |
| FEV1 | 81.07 ± 11.25 |
| 6 mwt (m) | 370.76 ± 72.27 |
| EF | 48.84 ± 9.38 |
| Variables | p Value | |
|---|---|---|
| Operative time | 33.46 ± 6.21 | <0.0001 |
| (M ± SD) | ||
| VAS (M ± SD) | ||
| After surgery | 2.92 ± 1.11 | <0.0001 |
| 12 h | 2.69 ± 0.48 | <0.0001 |
| 24 h | 3.15 ± 0.30 | <0.0001 |
| Length of stay | 1.38 ± 0.50 | <0.0001 |
| Technique | Pros | Cons |
|---|---|---|
| CT guided or US—FNAB |
| Sample insufficient for a definitive diagnosis |
| CT or US guided Core-needle biopsy |
|
|
| VATS biopsy |
|
|
| Standard mediastinotomy (Chamberlain technique) |
|
|
| Present technique (US associated with anterior mediastinotomy) |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cascone, R.; Carlucci, A.; Messina, G.; Noro, A.; Bove, M.; Natale, G.; Sagnelli, C.; Opromolla, G.; Martone, M.; Santoriello, C.; et al. Ultrasound-Guided Anterior Mediastinotomy: A Feasible Tool for Critical Lymphoma Patients. Healthcare 2021, 9, 770. https://doi.org/10.3390/healthcare9060770
Cascone R, Carlucci A, Messina G, Noro A, Bove M, Natale G, Sagnelli C, Opromolla G, Martone M, Santoriello C, et al. Ultrasound-Guided Anterior Mediastinotomy: A Feasible Tool for Critical Lymphoma Patients. Healthcare. 2021; 9(6):770. https://doi.org/10.3390/healthcare9060770
Chicago/Turabian StyleCascone, Roberto, Annalisa Carlucci, Gaetana Messina, Antonio Noro, Mary Bove, Giovanni Natale, Caterina Sagnelli, Giorgia Opromolla, Mario Martone, Carlo Santoriello, and et al. 2021. "Ultrasound-Guided Anterior Mediastinotomy: A Feasible Tool for Critical Lymphoma Patients" Healthcare 9, no. 6: 770. https://doi.org/10.3390/healthcare9060770