
A Systematic Review on Lean Applications’ in Emergency Departments

 , , , , , and
, , , , , and
Abstract
:
1. Introduction
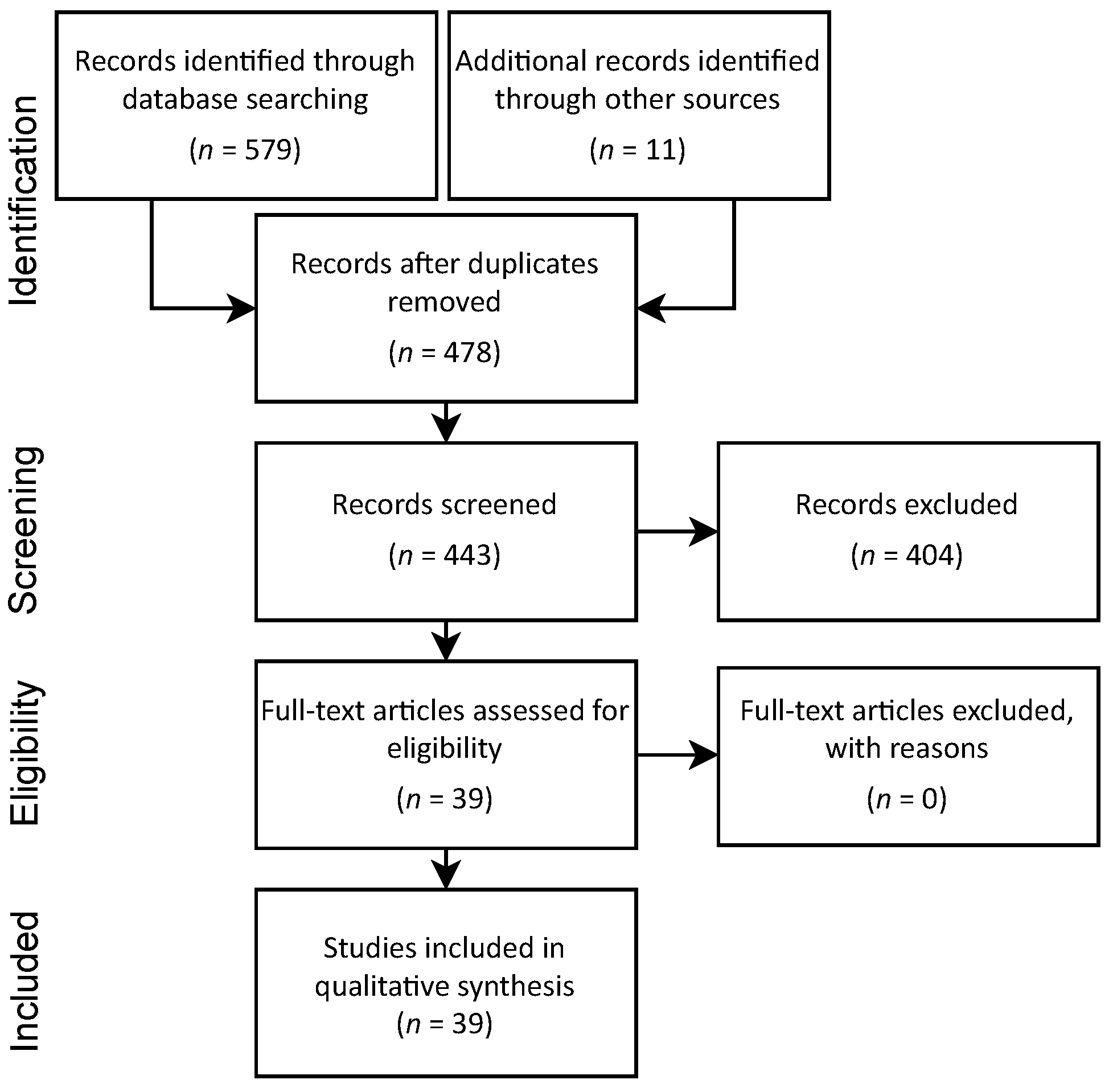
2. Materials and Methods
3. Emergency Department Patient Flow
- Screening: performed by a nursing professional, brief assessment of patient clinical conditions regarding severity to define care priority;
- Medical care: physical examination and interview to understand the main complaint;
- Initial diagnosis: actions based on the primary complaint, oral medication or other modality, and auxiliary services (as needed);
- Intermediate diagnosis: additional service result evaluation and/or medication administration;
- Final diagnosis: hospitalization or medical discharge.
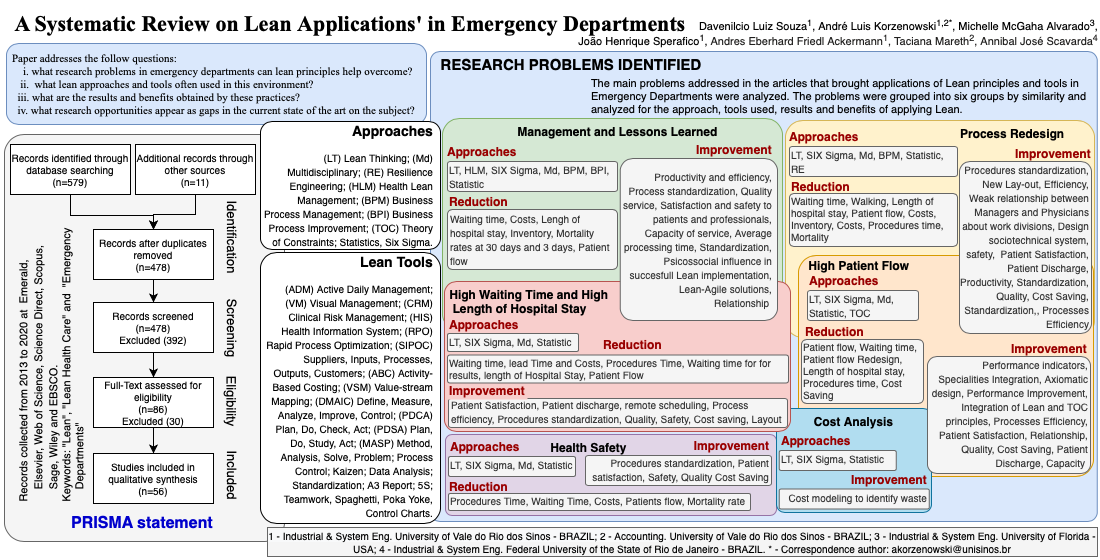
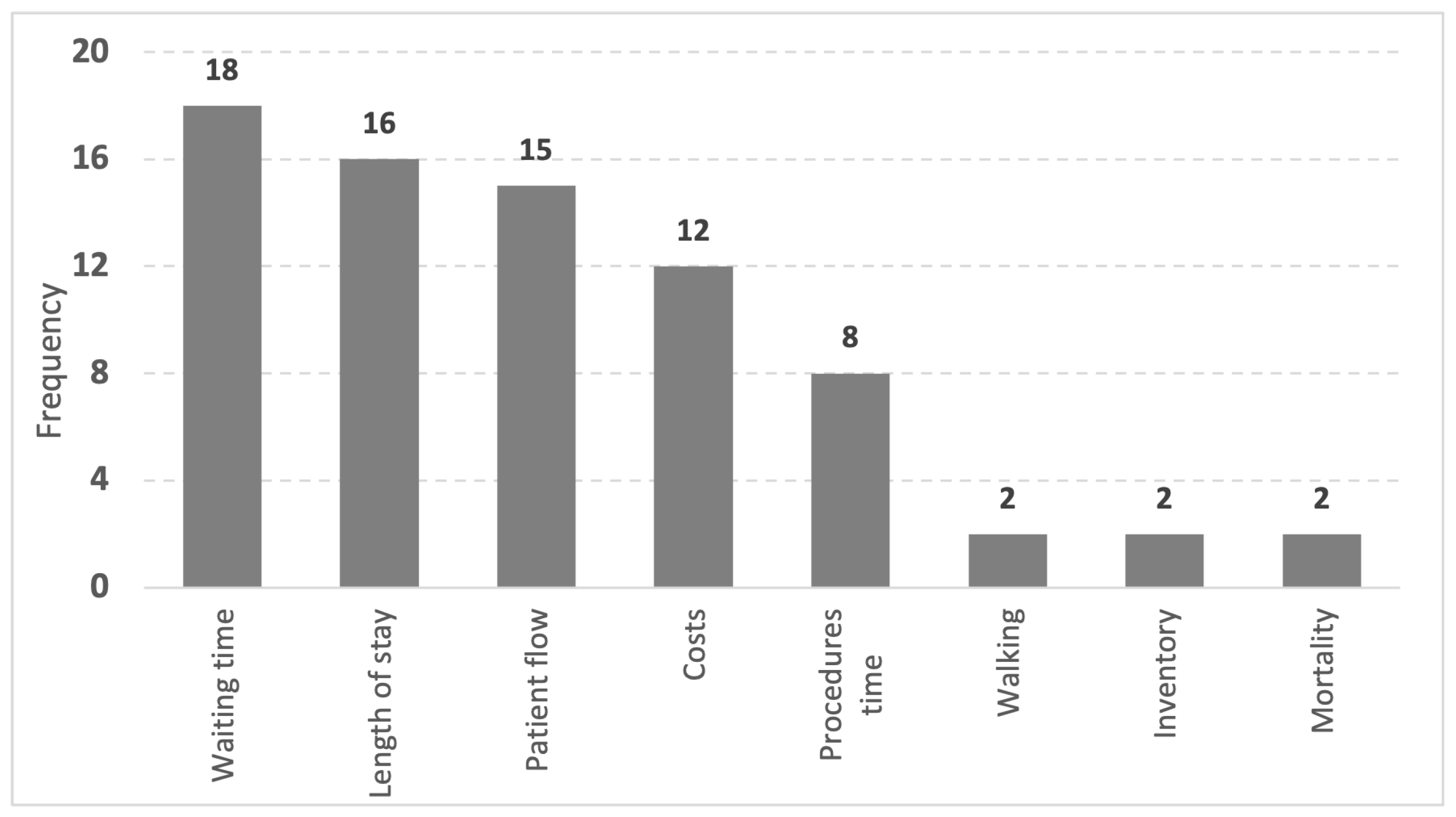
4. Research Problems, Approaches, and Applied Tools
4.1. Management and Lessons Learned
4.2. Process Redesign
4.3. High Waiting Time and High Length of Hospital Stay
4.4. High Patient Flow
4.5. Health Safety
4.6. Cost Analysis
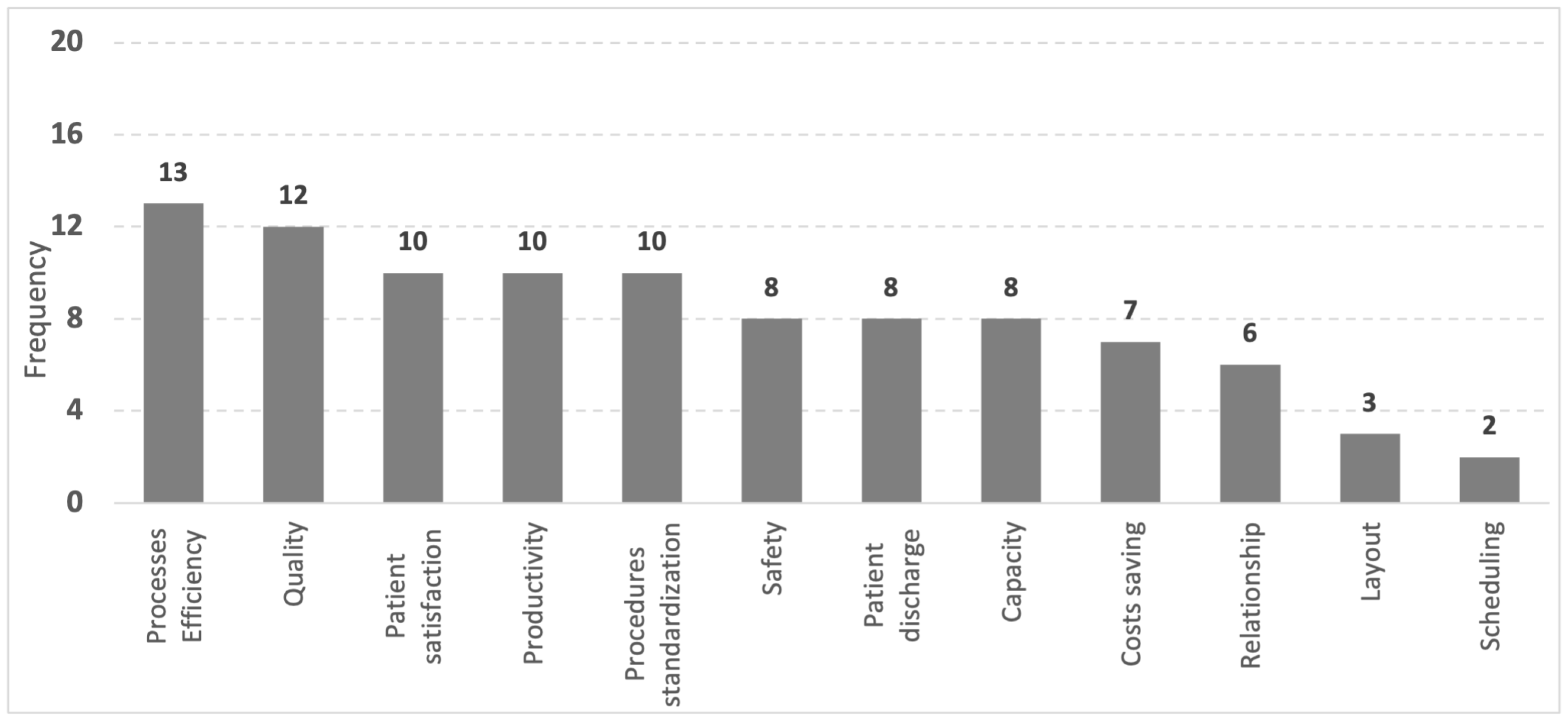
5. Benefits of Lean Application In Emergency Departments
6. Conclusions and Research Opportunities
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yousefi, M.; Ferreira, R. An agent-based simulation combined with technique for improving the performance of an emergency department. Braz. J. Med. Biol. Res. 2017, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schull, M.J.; Slaughter, P.M.; Redelmeier, D.A. Urban emergency department overcrowding: Defining the problem and eliminating misconceptions. Can. J. Emerg. Med. 2002, 4, 76–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Improta, G.; Romano, M.; Di Cicco, M.V.; Ferraro, A.; Borrelli, A.; Verdoliva, C.; Triassi, M.; Cesarelli, M. Lean thinking to improve emergency department throughput at AORN Cardarelli hospital. BMC Health Serv. Res. 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pines, J.M.; Hilton, J.A.; Weber, E.J.; Alkemade, A.J.; Al Shabanah, H.; Anderson, P.D.; Bernhard, M.; Bertini, A.; Gries, A.; Ferrandiz, S.; et al. International perspectives on emergency department crowding. Acad. Emerg. Med. 2011, 18, 1358–1370. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, G.; Konder, M.T.; Machado, C.V.; Alves, C.P.; Alves, R.P. The current scenario of emergency care policies in Brazil. BMC Health Serv. Res. 2013, 13, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verelst, S.; Wouters, P.; Gillet, J.B.; Van den Berghe, G. Emergency department crowding in relation to in-hospital adverse medical events: A large prospective observational cohort study. J. Emerg. Med. 2015, 49, 949–961. [Google Scholar] [CrossRef] [PubMed]
- Daultani, Y.; Chaudhuri, A.; Kumar, S. A decade of lean in healthcare: Current state and future directions. Glob. Bus. Rev. 2015, 16, 1082–1099. [Google Scholar] [CrossRef]
- Paim, J.; Travassos, C.; Almeida, C.; Bahia, L.; Macinko, J. The Brazilian health system: History, advances, and challenges. Lancet 2011, 377, 1778–1797. [Google Scholar] [CrossRef]
- Zhao, Y.; Peng, Q.; Strome, T.; Weldon, E.; Zhang, M.; Chochinov, A. Bottleneck detection for improvement of Emergency Department efficiency. Bus. Process Manag. J. 2015, 21, 564–585. [Google Scholar] [CrossRef]
- White, B.A.; Baron, J.M.; Dighe, A.S.; Camargo, C.A., Jr.; Brown, D.F. Applying Lean methodologies reduces ED laboratory turnaround times. Am. J. Emerg. Med. 2015, 33, 1572–1576. [Google Scholar] [CrossRef] [Green Version]
- Montella, E.; Di Cicco, M.V.; Ferraro, A.; Centobelli, P.; Raiola, E.; Triassi, M.; Improta, G. The application of Lean Six Sigma methodology to reduce the risk of healthcare–associated infections in surgery departments. J. Eval. Clin. Pract. 2017, 23, 530–539. [Google Scholar] [CrossRef]
- Liker, J.K.; Meier, D. O Modelo Toyota-Manual de Aplicação: Um Guia Prático para a Implementação dos 4Ps da Toyota; Bookman Editora: Porto Alegre, Brazil, 2007. [Google Scholar]
- Holweg, M. The genealogy of lean production. J. Oper. Manag. 2007, 25, 420–437. [Google Scholar] [CrossRef]
- Brandao de Souza, L. Trends and approaches in lean healthcare. Leadersh. Health Serv. 2009, 22, 121–139. [Google Scholar] [CrossRef]
- Mazzocato, P.; Holden, R.J.; Brommels, M.; Aronsson, H.; Bäckman, U.; Elg, M.; Thor, J. How does lean work in emergency care? A case study of a lean-inspired intervention at the Astrid Lindgren Children’s hospital, Stockholm, Sweden. BMC Health Serv. Res. 2012, 12, 28. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.K.; Yang, T.; Yang, C.Y.; Chan, F.T. Lean principles and simulation optimization for emergency department layout design. Ind. Manag. Data Syst. 2015, 115, 678–699. [Google Scholar] [CrossRef]
- Ulhassan, W.; Westerlund, H.; Thor, J.; Sandahl, C.; von Thiele Schwarz, U. Does Lean implementation interact with group functioning? J. Health Organ. Manag. 2014, 28, 196–213. [Google Scholar] [CrossRef]
- Moraros, J.; Lemstra, M.; Nwankwo, C. Lean interventions in healthcare: Do they actually work? A systematic literature review. Int. J. Qual. Health Care 2016, 28, 150–165. [Google Scholar] [CrossRef] [Green Version]
- Bucci, S.; De Belvis, A.; Marventano, S.; De Leva, A.; Tanzariello, M.; Specchia, M.L.; Ricciardi, W.; Franceschi, F. Emergency department crowding and hospital bed shortage: Is lean a smart answer? A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 4209–4219. [Google Scholar]
- Improta, G.; Cesarelli, M.; Montuori, P.; Santillo, L.C.; Triassi, M. Reducing the risk of healthcare-associated infections through Lean Six Sigma: The case of the medicine areas at the Federico II University Hospital in Naples (Italy). J. Eval. Clin. Pract. 2018, 24, 338–346. [Google Scholar] [CrossRef] [Green Version]
- Ortíz-Barrios, M.A.; Alfaro-Saíz, J.J. Methodological approaches to support process improvement in emergency departments: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 2664. [Google Scholar] [CrossRef] [PubMed]
- Ponsiglione, A.M.; Ricciardi, C.; Improta, G.; Orabona, G.D.; Sorrentino, A.; Amato, F.; Romano, M. A Six Sigma DMAIC methodology as a support tool for Health Technology Assessment of two antibiotics. Math. Biosci. Eng. 2021, 18, 3469–3490. [Google Scholar] [CrossRef]
- Rowley, J.; Slack, F. Conducting a literature review. Manag. Res. News 2004, 27, 31–39. [Google Scholar] [CrossRef]
- Cant, R.P.; Cooper, S.J. Simulation-based learning in nurse education: Systematic review. J. Adv. Nurs. 2010, 66, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Mareth, T.; Thomé, A.M.T.; Scavarda, L.F.; Oliveira, F.L.C. Technical efficiency in dairy farms: Research framework, literature classification and research agenda. Int. J. Prod. Perform. Manag. 2017, 66, 380–404. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Weintraub, I. The impact of alternative presses on scientific communication. Int. J. Grey Lit. 2000, 1, 54–59. [Google Scholar] [CrossRef]
- Eidelwein, F.; Antunes Júnior, J.A.V.; Piran, F.S.; de Lima Nunes, F. Conceptual precision in production engineering: A theoretical approach. Rev. ESPACIOS 2016, 37, 6. [Google Scholar]
- Yarmohammadian, M.H.; Rezaei, F.; Haghshenas, A.; Tavakoli, N. Overcrowding in emergency departments: A review of strategies to decrease future challenges. J. Res. Med. Sci. 2017, 22. [Google Scholar] [CrossRef]
- Magalhães, A.L.P.; Erdmann, A.L.; Silva, E.L.D.; Santos, J.L.G.D. Lean thinking in health and nursing: An integrative literature review. Rev. Lat. Am. Enferm. 2016, 24. [Google Scholar] [CrossRef] [Green Version]
- Mazzocato, P.; Stenfors-Hayes, T.; von Thiele Schwarz, U.; Hasson, H.; Nyström, M.E. Kaizen practice in healthcare: A qualitative analysis of hospital employees’ suggestions for improvement. BMJ Open 2016, 6, e012256. [Google Scholar] [CrossRef] [Green Version]
- Crema, M.; Verbano, C. Mapping lean experiences and emerging connections with clinical risk management in Italian context. Bus. Process Manag. J. 2015, 21, 1091–1116. [Google Scholar] [CrossRef]
- Timmons, S.; Coffey, F.; Vezyridis, P. Implementing lean methods in the Emergency Department: The role of professions and professional status. J. Health Organ. Manag. 2014, 28, 214–228. [Google Scholar] [CrossRef]
- Mogini, V.; Campanella, P.; Moraca, E.; Makishti, O.; Ricciardi, W.; Specchia, M. Improving quality and efficiency in healthcare. The Lean Thinking strategy. Eur. J. Public Health 2017, 27. [Google Scholar] [CrossRef] [Green Version]
- Rotteau, L.; Webster, F.; Salkeld, E.; Hellings, C.; Guttmann, A.; Vermeulen, M.J.; Bell, R.S.; Zwarenstein, M.; Rowe, B.H.; Nigam, A.; et al. Ontario’s emergency department process improvement program: The experience of implementation. Acad. Emerg. Med. 2015, 22, 720–729. [Google Scholar] [CrossRef]
- Toussaint, J.S.; Berry, L.L. The promise of Lean in health care. Mayo Clin. Proc. 2013, 88, 74–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sankoff, J.; Taub, J.; Mintzer, D. Accomplishing much in a short time: Use of a rapid improvement event to redesign the assessment and treatment of patients with alcohol withdrawal. Am. J. Med. Qual. 2013, 28, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Dyas, S.R. PRACTITIONER APPLICATION: Using Time-Driven Activity-Based Costing to Model the Costs of Various Process Improvement Strategies in Acute Pain Management. J. Healthc. Manag. 2018, 63, e86–e87. [Google Scholar] [CrossRef]
- Ulhassan, W.; von Thiele Schwarz, U.; Thor, J.; Westerlund, H. Interactions between lean management and the psychosocial work environment in a hospital setting–a multi-method study. BMC Health Serv. Res. 2014, 14, 480. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, G.S.A.; Silva, U.R.; Costa, A.L.; Pádua, S.I.D.D.D. The promotion of BPM and lean in the health sector: Main results. Bus. Process Manag. J. 2016, 24, 400–424. [Google Scholar] [CrossRef]
- Alnajem, M.; Garza-Reyes, J.A.; Antony, J. Lean readiness within emergency departments: A conceptual framework. Benchmarking Int. J. 2019, 26, 1874–1904. [Google Scholar] [CrossRef]
- Olsson, O.; Aronsson, H. Managing a variable acute patient flow–categorising the strategies. Supply Chain Manag. Int. J. 2015, 20, 113–127. [Google Scholar] [CrossRef]
- Efe, B.; Efe, Ö.F. An application of value analysis for lean healthcare management in an emergency department. Int. J. Comput. Intell. Syst. 2016, 9, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Swanson, C. Reorganizing a Resuscitation Room Using Six Sigma (6S) Principles. J. Emerg. Nurs. 2014, 40, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Breen, L.M.; Trepp, R.; Gavin, N. Lean Process Improvement in the Emergency Department. Emerg. Med. Clin. 2020, 38, 633–646. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.S.; Rasid, M.F.; Salim, W.I. Using modified triage system to improve emergency department efficacy: A successful Lean implementation. Int. J. Healthc. Manag. 2019, 14, 419–423. [Google Scholar] [CrossRef]
- Sloan, T.; Fitzgerald, A.; Hayes, K.J.; Radnor, Z.; Robinson, S.; Sohal, A. Lean in healthcare–history and recent developments. J. Health Organ. Manag. 2014, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, K.J.; Reed, N.; Fitzgerald, A.; Watt, V. Applying lean flows in pathology laboratory remodelling. J. Health Organ. Manag. 2014, 28, 229–246. [Google Scholar] [CrossRef] [Green Version]
- Swartz, J.; Davis, D.; Graban, M. Lean hospital (ist) s. Hosp. Med. Clin. 2015, 4, 581–593. [Google Scholar] [CrossRef]
- Balfour, M.E.; Tanner, K.; Jurica, P.J.; Llewellyn, D.; Williamson, R.G.; Carson, C.A. Using Lean to rapidly and sustainably transform a behavioral health crisis program: Impact on throughput and safety. Jt. Commission J. Qual. Patient Saf. 2017, 43, 275–283. [Google Scholar] [CrossRef] [Green Version]
- Narayanamurthy, G.; Gurumurthy, A.; Subramanian, N.; Moser, R. Assessing the readiness to implement lean in healthcare institutions: A case study. Int. J. Prod. Econ. 2018, 197, 123–142. [Google Scholar] [CrossRef] [Green Version]
- Vashi, A.A.; Sheikhi, F.H.; Nashton, L.A.; Ellman, J.; Rajagopal, P.; Asch, S.M. Applying lean principles to reduce wait times in a VA emergency department. Military Med. 2019, 184, e169–e178. [Google Scholar] [CrossRef] [Green Version]
- Leggat, S.G.; Gough, R.; Bartram, T.; Stanton, P.; Bamber, G.J.; Ballardie, R.; Sohal, A. Process redesign for time-based emergency admission targets. J. Health Organ. Manag. 2016, 30, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Alowad, A.; Samaranayake, P.; Ahsan, K.; Alidrisi, H.; Karim, A. Enhancing patient flow in emergency department (ED) using lean strategies—An integrated voice of customer and voice of process perspective. Bus. Process Manag. J. 2020, 27, 75–105. [Google Scholar] [CrossRef]
- Rosso, C.B.; Saurin, T.A. The joint use of resilience engineering and lean production for work system design: A study in healthcare. Appl. Ergon. 2018, 71, 45–56. [Google Scholar] [CrossRef]
- Kane, M.; Chui, K.; Rimicci, J.; Callagy, P.; Hereford, J.; Shen, S.; Norris, R.; Pickham, D. Lean manufacturing improves emergency department throughput and patient satisfaction. J. Nurs. Adm. 2015, 45, 429–434. [Google Scholar] [CrossRef]
- Chiarini, A. Waste savings in patient transportation inside large hospitals using lean thinking tools and logistic solutions. Leadersh. Health Serv. 2013, 26, 356–367. [Google Scholar] [CrossRef]
- Lisiecka-Biełanowicz, M.; Lisiecka, K. Lean Healthcare in Hospital Emergency Department. Case Study. Zeszyty Naukowe. Organizacja i Zarządzanie/Politechnika Śląska 2020, 123–133. [Google Scholar] [CrossRef]
- Allaudeen, N.; Vashi, A.; Breckenridge, J.S.; Haji-Sheikhi, F.; Wagner, S.; Posley, K.A.; Asch, S.M. Using lean management to reduce emergency department length of stay for medicine admissions. Qual. Manag. Health Care 2017, 26, 91–96. [Google Scholar] [CrossRef]
- Sanders, J.H.; Karr, T. Improving ED specimen TAT using lean six sigma. Int. J. Health Care Qual. Assurance 2015, 28, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, M.J.; Stukel, T.A.; Guttmann, A.; Rowe, B.H.; Zwarenstein, M.; Golden, B.; Nigam, A.; Anderson, G.; Bell, R.S.; Schull, M.J.; et al. Evaluation of an emergency department lean process improvement program to reduce length of stay. Ann. Emerg. Med. 2014, 64, 427–438. [Google Scholar] [CrossRef] [Green Version]
- White, B.A.; Chang, Y.; Grabowski, B.G.; Brown, D.F. Using lean-based systems engineering to increase capacity in the emergency department. West. J. Emerg. Med. 2014, 15, 770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, G.T.; Campos, A.T.; de Lima Magacho, A.; Segismondi, L.C.; Vilela, F.F.; de Queiroz, J.A.; Montevechi, J.A.B. Lean thinking by integrating with discrete event simulation and design of experiments: An emergency department expansion. PeerJ Comput. Sci. 2020, 6, e284. [Google Scholar] [CrossRef]
- Furterer, S.L. Applying Lean Six Sigma methods to reduce length of stay in a hospital’s emergency department. Qual. Eng. 2018, 30, 389–404. [Google Scholar] [CrossRef]
- Uspal, N.G.; Rutman, L.E.; Kodish, I.; Moore, A.; Migita, R.T. Use of a Dedicated, Non–Physician-led Mental Health Team to Reduce Pediatric Emergency Department Lengths of Stay. Acad. Emerg. Med. 2016, 23, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.C.; Ramos, M.; Paixão, C. A lean case study in an oncological hospital: Implementation of a telephone triage system in the emergency service. Risk Manag. Healthc. Policy 2014, 7, 1. [Google Scholar]
- Patey, C.; Norman, P.; Araee, M.; Asghari, S.; Heeley, T.; Boyd, S.; Hurley, O.; Aubrey-Bassler, K. SurgeCon: Priming a community emergency department for patient flow management. West. J. Emerg. Med. 2019, 20, 654. [Google Scholar] [CrossRef] [Green Version]
- Ker, J.I.; Wang, Y.; Hajli, N. Examining the impact of health information systems on healthcare service improvement: The case of reducing in patient-flow delays in a US hospital. Technol. Forecast. Soc. Chang. 2018, 127, 188–198. [Google Scholar] [CrossRef] [Green Version]
- Shakoor, M.; Qureshi, M.R.; Jaber, S. Applying Management Principles of Lean Manufacturing for Enhancing Efficiency and Effectiveness of Emergency Department Rooms. Jordan J. Mech. Ind. Eng. 2019, 13, 291–299. [Google Scholar]
- Wiler, J.L.; Bookman, K.; Birznieks, D.B.; Leeret, R.; Koehler, A.; Planck, S.; Zane, R. Rapid Process Optimization: A Novel Process Improvement Methodology to Innovate Health Care Delivery. Am. J. Med. Qual. 2017, 32, 172–177. [Google Scholar] [CrossRef]
- Verbano, C.; Crema, M. Applying lean management to reduce radiology turnaround times for emergency department. Int. J. Health Plan. Manag. 2019, 34, e1711–e1722. [Google Scholar] [CrossRef]
- Van der Linden, M.C.; van der Linden, N.N. The impact of a multimodal intervention on emergency department crowding and patient flow. Int. J. Emerg. Med. 2019, 12, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Arcidiacono, G.; Matt, D.T.; Rauch, E. Axiomatic design of a framework for the comprehensive optimization of patient flows in hospitals. J. Healthc. Eng. 2017, 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassanain, M. An Overview of the Performance Improvement Initiatives by the Ministry of Health in the Kingdom of Saudi Arabia. INQUIRY J. Health Care Organ. Provis. Financ. 2017, 54, 0046958017707872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, A.; Hunter, K.; Cunningham, K.; Williams, J.; O’Shea, H.; Rooney, P.; Hickey, F. STEPS: Lean thinking, theory of constraints and identifying bottlenecks in an emergency department. Irish Med. J. 2013, 106, 105–107. [Google Scholar]
- Fall, D.D. Earning Your “Gait Belt” in Lean: “Stopping the Line” through a Staffing Response Team. Nurse Leader 2016, 14, 343–349. [Google Scholar] [CrossRef]
- Burström, L.; Letterstål, A.; Engström, M.L.; Berglund, A.; Enlund, M. The patient safety culture as perceived by staff at two different emergency departments before and after introducing a flow-oriented working model with team triage and lean principles: A repeated cross-sectional study. BMC Health Serv. Res. 2014, 14, 296. [Google Scholar] [CrossRef] [Green Version]
- Maliszewski, B.; Whalen, M.; Lindauer, C.; Williams, K.; Gardner, H.; Baptiste, D.L. Quality Improvement in the Emergency Department: A Project to Reduce Door-to-Electrocardiography Times for Patients Presenting with Chest Pain. J. Emerg. Nurs. 2020, 46, 497–504. [Google Scholar] [CrossRef]
- Dyas, S.R.; Greenfield, E.; Messimer, S.; Thotakura, S.; Gholston, S.; Doughty, T.; Hays, M.; Ivey, R.; Spalding, J.; Phillips, R. Process-improvement cost model for the emergency department. J. Healthc. Manag. 2015, 60, 442–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polosa, R.; Spinicci, M.; Prisco, D. “COVID-19: Diagnosis, management and prognosis”: A new topical collection of Internal and Emergency Medicine. Intern. Emerg. Med. 2020, 15, 747–750. [Google Scholar] [CrossRef]
- Meschi, T.; Rossi, S.; Volpi, A.; Ferrari, C.; Sverzellati, N.; Brianti, E.; Fabi, M.; Nouvenne, A.; Ticinesi, A. Reorganization of a large academic hospital to face COVID-19 outbreak: The model of Parma, Emilia-Romagna region, Italy. Eur. J. Clin. Investig. 2020, 50, e13250. [Google Scholar] [CrossRef]
- Patey, C.; Asghari, S.; Norman, P.; Hurley, O. Redesign of a rural emergency department to prepare for the COVID-19 pandemic. CMAJ 2020, 192, E518–E520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russi, C.S.; Heaton, H.A.; Demaerschalk, B.M. Emergency medicine telehealth for COVID-19: Minimize front-line provider exposure and conserve personal protective equipment. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2020; Volume 95, pp. 2065–2068. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Classification | Frequency |
|---|---|---|
| Methodological Approaches | Qualitative | 33 |
| Qualitative/Quantitative | 19 | |
| Quantitative | 4 | |
| Type of Study | Theoretical-Empirical | 32 |
| Empirical | 20 | |
| Theoretical | 4 | |
| Research Method | Case Study | 37 |
| Literature Review | 11 | |
| Survey | 5 | |
| Modeling | 3 |
| Research Problem | Authors | Approach | Tools and Methods |
|---|---|---|---|
| [30,31,32] | LT, HLM | Process Control; Kaizen; PDSA; CRM | |
| [33] | LT, Six Sigma | DMAIC | |
| [18,34] | LT, Statistic | Data Analysis; Standardization | |
| [35,36] | LT, Md | Teamwork; Standardization; VSM; PDSA; VM | |
| Management and Lessons Learned | [37] | LT, Md, Six Sigma | Kaizen; DMAIC; A3; PDCA; Teamwork |
| [38] | LT, Md, Six Sigma, Statistic | VSM; DMAIC; Kaizen; Control Chart; Teamwork | |
| [39] | LT, Statistic, Md | Teamwork; MASP; VM; 5S; Data Analysis | |
| [40] | LT, Md, BPM | Service; Teamwork | |
| [17,41] | LT, Psycho-social | Service; VSM; Teamwork; Standardization | |
| [42] | LT, BPI | VSM; Lean-Agile | |
| [43] | LT | VSM; Teamwork; Data Analysis; VM | |
| [44,45] | LT, Six Sigma | Kaizen; DMAIC; Teamwork; VM; 5S; Standardization | |
| [16,46] | LT, Statistic | VSM; WIP; Simulation; Data Analysis | |
| Process Redesign | [47,48,49,50,51,52] | LT, Md | VSM; Kaizen; Teamwork; Spaghetti; Standardization |
| [53] | LT, Md, Six Sigma | VSM; DMAIC; Teamwork; | |
| [21,54] | LT, Statistic, Six Sigma, BPM | VSM; PDCA; Data Analysis; PDSA; VM; Standardization | |
| [55] | LT, Md, RE | VSM; Kaizen; Teamwork; PDCA | |
| [56,57,58] | LT | VSM; 5S; Kaizen; Spaghetti; ADM; Check Sheet; Standardization | |
| [59] | LT, Md | Teamwork; VM; Standardization | |
| High Waiting Time and High Length of Hospital Stay | [60] | LT, Six Sigma | VSM; DMAIC; PDCA; Kaizen; 5S; Poka Yoke; VM |
| [10,61,62,63] | LT, Statistic | VSM; Kaizen; Data Analysis; Cohort; Standardization | |
| [64] | LT, Statistic, Six Sigma | VSM; Kaizen; DMAIC; PDCA | |
| [65,66,67] | LT, Statistic, Md | VSM; Control Chart; Teamwork; ADM; Data Analysis | |
| [68,69] | LT | Kaizen; HIS; Teamwork; VSM; Data Analysis; Standardization | |
| [19] | LT, Md | VSM; Teamwork; Standardization | |
| [70,71] | LT, Md, Six Sigma | DMAIC; RPO; 5S; PDSA; Teamwork | |
| High Patient Flow | [72] | LT, Statistic | Teamwork; Data Analysis |
| [73] | LT, Six Sigma, Md, Statistic | VSM; DMAIC; Teamwork; Data Analysis; Design Axiomatic | |
| [74] | LT, Six Sigma | VSM; DMAIC; VM | |
| [75] | LT, TOC | VSM; Steps of TOC | |
| [76] | LT, Md, Six Sigma | VSM, DMAIC, VM, Teamwork, PDCA | |
| Health Safety | [77] | LT, Statistic, Md | PDSA; Teamwork; Data Analysis |
| [78] | LT, Md, Statistic, Six Sigma | Data Analysis; Standardization; Teamwork | |
| Cost Analysis | [79] | LT, Statistic, Six Sigma | VSM; DMAIC; Spaghetti; SIPOC; ABC |
| Research Problem | Results/Benefits | |
|---|---|---|
| Management and Lessons Learned | Reduction | Waiting time, costs, Length of hospital stay [30,31,32]; Waiting time, Inventory, Mortality rates at 30 days and 3 days [18,34]; Waiting time %, Costs % [35,36]; Length of hospital stay from 3.6 days to 2.6 days [37]; Waiting time, Costs, Length of hospital stay [40]; Waiting time, Patient flow [41]. |
| Improvement | Productivity +68%, efficiency, Process standardization, Quality service, Satisfaction and safety to patients and professionals, Improvement suggestions given by 72% of the employees [30,31,32,33]; The Lean implementations suggest new studies [18,34]; Capacity of service +10% [35,36]; Savings of U$ 2 million per year [37]; Average processing time Scanner from 113 min to 58 min [38]; Significant results in wards I and II and not significant in ED, Differences in teams performances [39]; Productivity, Efficiency, Quality, Satisfaction and safety to patients and professionals, Standardization [40]; Psico-ssocial influence in successful Lean implementation [17]; Lean-Agile solutions [42]; Processes Efficiency, Procedures Standardization, Relationship [41]. | |
| Process Redesign | Reduction | Waiting time from 78 to 38 min [16]; Walking km = 8 work days/year [47,48,49,51]; Waiting time from 34.7 to 22.1 min, Length of hospital stay from 163.2 to 146.3 min [52]; Waiting time %, Patient flow, Length of hospital stay from 8.7 to 6.4 h, Costs [21]; Length of hospital stay, Patient flow [46]; Costs, Length of hospital stay, Patient flow, Walking [45]; Waiting time, Length of hospital stay, Patient flow, Inventory [43]; Waiting time, Costs, Patient flow, Procedure times, Mortality [54]; Waiting time, Patient flow [50]. |
| Improvement | Procedures standardization [44]; New Lay-out, Efficiency from 54.8% to 88.5% [16]; Processes [47,48,49,51]; Weak relationship between Managers and Physicians about work divisions [53]; Framework, Design social-technical system, efficiency, safer place [55]; Relationship, Layout, Patient Discharge from 161.8 to 156.6 min [52]; Patient Satisfaction, Patient Discharge [21]; Processes Efficiency, Productivity [46]; Patient Satisfaction, Efficiency, Productivity, Standardization, Quality, Cost Saving, Patient Discharge, Capacity [45]; Patient Satisfaction, Efficiency, Productivity, Safety, Quality, Cost Saving [43]; Patient Satisfaction, Processes Efficiency, Productivity, Procedures Standardization, Relationship, Safety, Quality, Cost Saving, Discharge, Layout, Capacity [54]; Patient Satisfaction, Processes Efficiency, safety, Quality, Patient Discharge, Capacity from 25 to 34 patients [50]. | |
| High Waiting Time and High Length of Hospital Stay | Reduction | Waiting time, Lead time and costs [56,57]; Time exam execution %, Waiting time for results [60]; Length of hospital stay % [64]; Procedure times [65,66]; Length of hospital stay from 199.4 to 134.4 min [67]; Procedure times from 104.3 to 42.2 min [67]; Waiting time [58]; Waiting time, Costs, Length of hospital stay, Patient flow, Procedure times [63]; Length of hospital stay from 8.7 to 6.4 h = 26.4% [59]. |
| Improvement | Patient satisfaction [56,57]; +40% of patient discharge in 1 h [10,61,62]; Patient satisfaction from 24% to 90% [64]; Remote scheduling [65,66]; Patient satisfaction, Capacity 25.7%, Processes Efficiency [67]; Processes Efficiency, Procedures Standardization, Quality, Patient Discharge [58]; Patient Satisfaction, Efficiency, Procedures Standardization, Safety, Quality, Cost Saving, Patient Discharge, Scheduling, Layout, Capacity [63]; Procedures Standardization [59]. | |
| High Patient Flow | Reduction | Patient flow, Costs [68]; Waiting time, Patient flow Redesign [70]; Patient flow [73]; Waiting time, Patient flow [75]; Waiting time, Patient flow [71]; Length of hospital stay from 167 to 154 min, Patient flow, Procedure times [72]; Waiting time, Costs, Length of hospital stay [69]; Length of hospital stay, Cost Saving [19]. |
| Improvement | Performance indicators, Specialities Integration [70]; Axiomatic design according Lean Health Care [73]; Performance Improvement Unit (PIU) weak integration between teams and managers [74]; Integration of Lean and TOC principles [75]; Processes Efficiency, Patient Satisfaction, Relationship, Quality [71]; Quality [72]; Processes Efficiency, Quality, Cost Saving, Patient Discharge, Capacity [69]; Productivity, Patient Satisfaction, Capacity [19]. | |
| Health Safety | Reduction | Procedure times from 17 to 7 min, Waiting time, Costs, Patient flow, Mortality [78]. |
| Improvement | Procedures standardization [76]; Patient satisfaction [77]; Procedures Standardization, Safety, Quality, Cost Saving [78]. | |
| Cost Analysis | Improvement | Cost model creation make easier to identify waste in expenses [79]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souza, D.L.; Korzenowski, A.L.; Alvarado, M.M.; Sperafico, J.H.; Ackermann, A.E.F.; Mareth, T.; Scavarda, A.J. A Systematic Review on Lean Applications’ in Emergency Departments. Healthcare 2021, 9, 763. https://doi.org/10.3390/healthcare9060763
Souza DL, Korzenowski AL, Alvarado MM, Sperafico JH, Ackermann AEF, Mareth T, Scavarda AJ. A Systematic Review on Lean Applications’ in Emergency Departments. Healthcare. 2021; 9(6):763. https://doi.org/10.3390/healthcare9060763
Chicago/Turabian StyleSouza, Davenilcio Luiz, André Luis Korzenowski, Michelle McGaha Alvarado, João Henrique Sperafico, Andres Eberhard Friedl Ackermann, Taciana Mareth, and Annibal José Scavarda. 2021. "A Systematic Review on Lean Applications’ in Emergency Departments" Healthcare 9, no. 6: 763. https://doi.org/10.3390/healthcare9060763