5.1. Discussion of Model Results
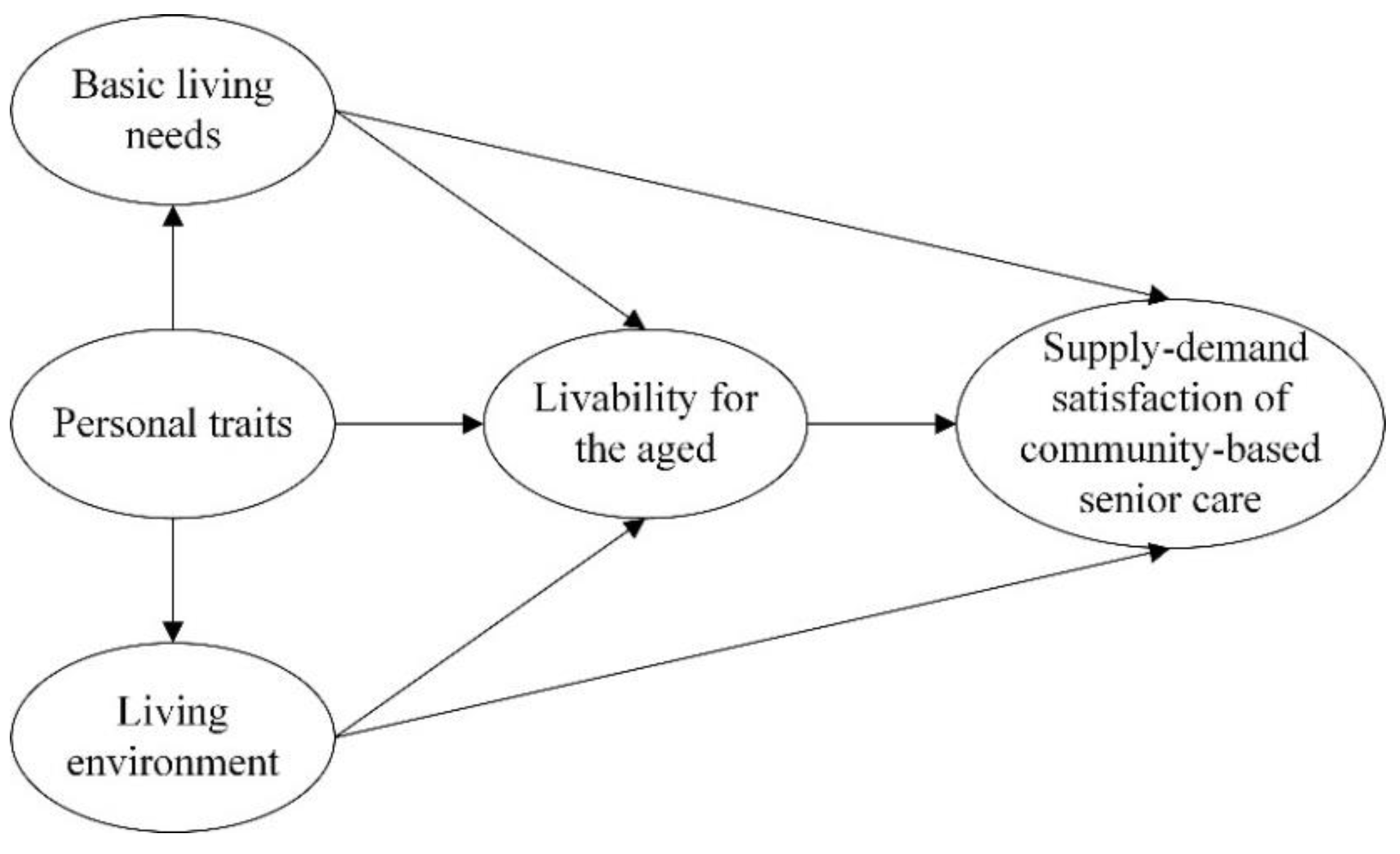
Based on Maslow’s hierarchy of needs theory and customer satisfaction theory, we proposed a model of the SSCSC. With the basis of the elderly’s psychological perceptions and the current situation of community elderly care, an attempt was made to identify the main factors affecting the satisfaction of community senior care. By examining and analyzing the data of the 296 questionnaires collected from seniors over 50 years old or completed by relatives on behalf of seniors according to their actual situation, we obtained the following results.
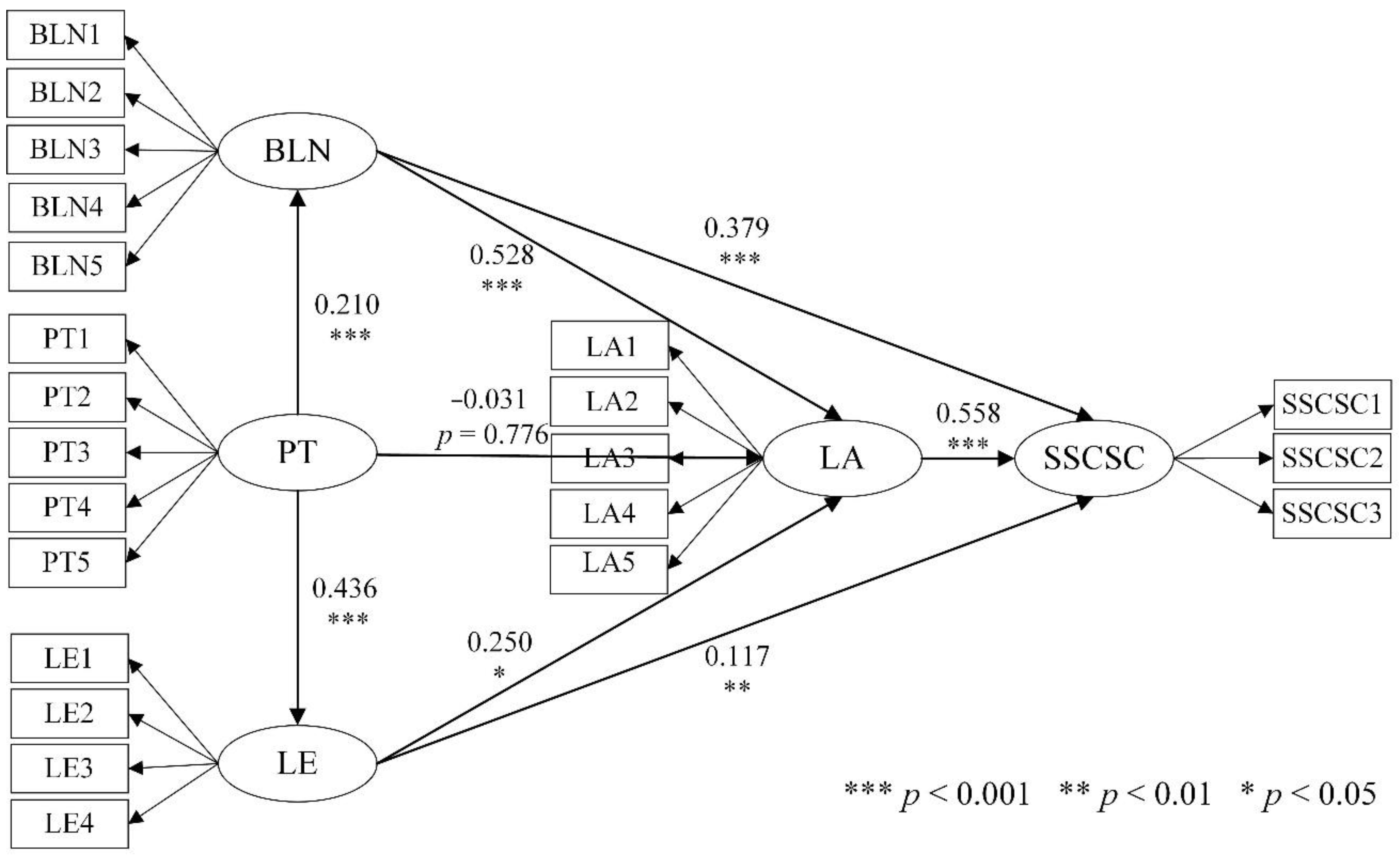
(1) For BLN and LE, as the primary basic factors considered in community-based senior care, both had a more significant effect on SSCSC (BLN→SSCSC: β = 0.379, p < 0.001; LE→SSCSC: β = 0.117, p < 0.005), which supports H1 and H2.
BLN has a significant impact on SSCSC, and this result shows consistency with other related studies on the relationship between BLN and elderly care [
70,
71]. Lengenfelder et al. point out that with age and declining physical function, older adults have varying degrees of decline in self-care and need more care and support from outside [
72]. In his study, Wang notes that older adults have a higher prevalence of chronic diseases and are more susceptible to age-related illnesses [
73]. According to the Country Assessment Report on Ageing and Health in China, published by the World Health Organization in 2018, the accelerated aging of the Chinese population will lead to at least a 40% increase in the disease burden of chronic non-communicable diseases. By 2030, the number of people with one or more chronic diseases in China will more than triple. The demand for health care services among the elderly is much greater than that of the general population. Referring to the findings of Al Ketbi et al., community medical elderly services should intervene in advance to strengthen the prevention of chronic diseases in the elderly, especially those that have a greater impact on their daily lives, and to perform the health care function of community-based senior care [
74]. Increasing physical activity is also an effective means of enhancing physical fitness. With the decline in the locomotor system, strengthening exercise can prevent diseases and enrich the community life of the elderly. If we categorize life and health needs as physical needs, social needs are a collection of psychological needs of the elderly. According to elderly subculture theory, community elderly care institutions are places where elderly people live together having a common activity place and similar age structure, and, subjectively, they can easily form a common area of concern, thus forming a subcultural group with a sense of identity and belonging [
75]. Cultural, sports, and recreational activities are the vehicles for the formation and communication of subcultural groups that can increase a sense of belonging within members of a group, expand one’s social network, and enrich the spiritual life of the elderly. Combined with the characteristics of the psychological changes in the elderly, community care allows the elderly to live in their homes and feel the warmth of family while enjoying the space for community interaction and communication, thus increasing the satisfaction of the elderly.
Compared to BLN, the influence degree of LE on SSCSC was slightly weaker, but it was still significant. Numerous related studies have also focused on the residential needs of older adults [
76,
77]. Li and Li note in their study that the mental accessibility of older adults to spatial places declines with age, and a stable residential environment will help develop familiarity with the surroundings in the brain. In the context of an aging society, the planning and design of urban residential areas must take into account the physiological, psychological, and social characteristics of the elderly, and combine their behavioral trajectories and special needs for outdoor environments, etc. [
78]. The community elderly environment often suffers from a lack of public space, lighting facilities, and a barrier-free design of building entrances and exits, which makes it difficult for the elderly to go out. At the same time, the intersection of pedestrian traffic and vehicular traffic, the discontinuity of sidewalks, the width, slope, road surface materials, and other problems that do not adapt to the gait characteristics of the elderly also cause difficulties for the elderly to walk [
79]. Walking as a widely adopted form of activity among older adults greatly affects their community participation and, thus, satisfaction with community aging. In addition, freedom of movement is important for the physical and mental health of older adults [
80]. A good community environment for leisure interaction and a positive community atmosphere are conducive to increasing older adults’ social participation and improving psychological conditions, thus enhancing satisfaction with community aging.
(2) PT had a significant effect on both BLNs and LE (PT→BLN: β = 0.210, p < 0.001, PT→LE: β = 0.436, p < 0.001), which supports H3 and H4.
Comparing the path coefficients, the effect of PTs on LE was more significant than the effect on BLNs. One possible explanation is that BLN are a more common and basic need for retirement than LE. At the level of the study where there was more differentiation in PT, the degree of the influence on LE was greater. Du et al. note that advanced aging often implies a higher risk of disability that results in a dichotomy between the increasing need for medical care among the older elderly and the increasing need for spiritual comfort among the younger elderly [
81]. Lai et al. found a statistically significant positive correlation between establishing a friendly living environment and active aging through a categorical survey of 112 elderly people in Malaysia [
82]. Education level, as one of the demographic variables, was also an active factor in studying the demand for elderly services. Eronen et al. investigated active aging among older adults with chronic diseases at different education levels and showed that having a certain level of health literacy was a strong predictor of active aging [
83]. Literacy has different effects on the basic needs and living conditions of older adults; for example, older adults with low literacy may have a higher proportion of need for medical care, cooking, laundry, and talk-and-chat services, while older adults with high literacy have a more urgent need for health care, cultural activities, emotional confessions, and psychological counseling services. Heller and Factor’s study found that the interdependent effects of family support and intergenerational caregiving by family members can lead to better social, health, and economic well-being for older adults. Good family support includes, on the one hand, life care, but more importantly, the environment and climate of interaction in the residential setting [
84]. Family support is closely related to the mental health of older adults, and older adults living alone are prone to depression, anxiety, loneliness, and other negative emotions due to the lack of support and care from their spouses in life and spirit [
85]. Good family support is beneficial to reduce life stress and maintain a sense of well-being. Therefore, when studying SSCSC, we must pay attention to the influence path of PTs on BLN and LE and be concerned about the special needs of elderly people due to the fact of their age, physical quality, and illness so as to realize the refinement of elderly care services.
(3) The effect of PT on LA was not significant, which was lower than expected (PT→LA: β = −0.031, p > 0.05), so H7 was not supported.
Jackson and Garrett’s findings suggest that older adults’ understanding of indicators related to LA, such as accessibility to transit stops and housing conditions, was universal and consistent [
86]. That is, the need for livability and aging appropriateness was universal for older adults of different ages, educational backgrounds, family support situations, and housing situations, which explains why it was less strongly associated with PT. The Report on the Development of China’s Livable Environment for the Elderly (2015), released by The National Working Commission on Aging of China, points out that, “The livable environment for the elderly is a new concept in response to the development of the aging population, and the construction of a safe, convenient and comfortable livable environment for the elderly is standard rather than high-quality mode”. The more common situation is that after retirement, the life type of the elderly gradually changes from work-oriented to leisure-oriented, with less contact with society and a narrower range of activities [
87]. Older adults are more dependent on the community to sustain their health and well-being by continuing to live in the community, maintaining relationships with family and neighbors, and participating in a variety of activities in familiar places and facilities. Due to the changes in physiological and psychological status and lifestyle, the elderly need a safe and comfortable environment for aging in place, a variety of social interaction spaces in the community, and a variety of professional services in the community. The relevant government planning departments should pay attention to the general demands of the elderly to live and age well and support them, improve existing living environments, ensure the elderly truly feel that they have an environment in which to age and live well, realize the function of community livability, and make community life satisfaction more in line with actual demand.
(4) Both BLN and LE had a significant effect on LA (BLN→LA: β = 0.528, p < 0.001, LE→LA: β = 0.250, p < 0.001), which supports H5 and H6.
This view is reinforced by the study by Chiu et al. who suggest that for the elderly, food, clothing, shelter, basic medical care, and a safe and convenient living environment are the basis for quality elderly care [
88]. In other words, BLN and LE were related to the basic needs of senior living, while LA emphasized the quality of senior living with peace and happiness, including the beauty of the senior living environment and the completeness of the number of related facilities. This emphasizes the improvement in the service facility system and the diversification and humanization of the content under the basic framework of health care, culture and entertainment, daily care, and senior living in the community. Gong et al. propose to improve the professionalism of elderly care services through “medical and nursing integration” so that medical and health resources and elderly care resources can complement each other to provide elderly people with adequate supply, reasonable gradients, and various forms of elderly health care services in the process of aging; thus, improving the overall capacity and level of elderly care services [
89]. By exploring the utilization pattern of community elderly facilities, Chang et al. suggest that the functional configuration of elderly facilities should be refined from the perspective of demand to improve the utilization rate of facilities, enhance the safety and comfort of facilities, and improve the efficiency of facility services [
90]. From the abovementioned studies, we can see that a “people-oriented” view to improve the quality and effectiveness of senior care services was fully recognized. The construction and improvement of high-satisfaction community senior care services need to start from the basic needs of senior care and consider the quantity to meet needs but also to provide high-quality community senior care services that are suitable for the elderly.
(5) LA had a significant effect on SSCSC (LA→SSCSC: β = 0.558, p < 0.001), which supports H8.
Currently, there are structural changes in the elderly population, and the number of people who are willing and able to lead a high quality of life in old age is gradually increasing, and the conditions, perceptions, and lifestyles of the elderly are quietly changing. The path coefficient also shows that LA was the most critical variable affecting SSCSC. In reality, the demands of the elderly for senior living was mainly reflected in two ways: one was to meet the physiological needs, mainly referring to meeting the characteristics of the elderly activities and behavior, such as adequate facilities which are easy to operate and reasonable space layout; the second is to meet the psychological needs of the elderly, which make they feel a sense of security, comfort as well as respect and care in the space. This is supported by a study by Carmody et al., who suggest that community care should further promote the level of geriatric care practice by improving the level of care and enhancing aging appropriateness [
91]. Integrating research in landscape, environmental behavior, psychology, and medicine, Rajagopalan et al. suggest that natural landscapes have the effect of reducing stress, relieving emotions, preventing hidden illnesses, and restoring health [
92]. Related studies have also shown a positive correlation between the amount of green space in the living environment and health [
93]. In other words, the beauty of community environment affects both the physical health and psychological health of the elderly thus affecting satisfaction. At the same time, community aging cannot be achieved without the support of the government and the community. The development of a complete social security system, the provision of pension and health insurance policies as well as the specification requirements for community aging, etc., these aspects of support determine, to some extent, the quality of institutions, thus directly or indirectly affecting the perceptions of elderly people towards community aging [
94]. With sufficient government support, a sound social security system, and reasonable pension levels, the elderly have enough ability to cope with illness and pay for their old-age expenses. In the face of standardized and professional community elderly care services, the elderly can enjoy more comprehensive and complete care, so the willingness and satisfaction of community elderly care increases.
5.2. Suggestions
Based on the above findings, this study makes the following recommendations to improve the supply–demand satisfaction of community-based senior care.
(1) Based on the basic living needs of the elderly, establish a community elderly service system that meets needs.
How to accurately grasp the needs of the elderly is an important basis for improving community elderly care services. Focused on the basic needs of the elderly for daily care and health, community elderly care service personnel should provide “warm” services with “love, patience and care” according to the special characteristics of the service recipients while improving the professionalism of nursing care, making seniors feel at home in community care. Actively promoting the development of medical and elderly care integration and exploring new models of cooperation between medical institutions and senior care institutions is an important issue in the construction of the current senior care service system. Communities can establish partnerships with professional medical institutions to build a health care service structure consisting of multidisciplinary teams. Adhering to a people-oriented ideology, medical services should be provided closely around the needs of the elderly, and appropriate health care plans should also be developed for them through daily diagnosis and comprehensive assessments. The beneficial exploration in the field of health care integration helps to further improve the satisfaction of community elderly care. The community can also improve the interpersonal relationships of the elderly, actively eliminate possible negative emotions in aging, improve the mental health of the elderly, and create a harmonious, mutually supportive and positive atmosphere by organizing highly participatory and interactive senior activities and cultural and recreational programs. In addition, the spiritual life of the elderly can be enriched by inviting volunteer services into the community and other forms to actively intervene and reduce their loneliness and improve their satisfaction with community aging. The government and the community should establish a senior care service system that meets the needs of the elderly based on the actual community senior care, with the supply side as the guide. Consider the quantitative allocation of senior care services, especially the supply of health care services, while focusing on the safety needs of the elderly, to improve the allocation of senior care resources and avoid the phenomenon of mismatch between supply and demand.
(2) Pay attention to the heterogeneous needs of individuals and provide differentiated and refined elderly care services.
Community elderly care should closely follow the actual situation, widely understand and further filter and screen needs, and summarize the general rules of different types of elderly people. Most of the needs of the elderly at the same age are homogeneous, which is consistent with the threat of physical decline and health risks. However, elderly people have different heterogeneous needs due to the fact of their different family support, education levels, and personality preferences. Therefore, for general needs, it is necessary to provide a wide range of services based on the improvement of service suitability and refinement. At the same time, we need to take into account the heterogeneous needs of the elderly and provide segmented services. For example, for empty nesters and elderly people with insufficient family support, more attention should be paid to the guarantee of life care and spiritual comfort services. For younger elderly people, the community should provide abundant recreational activities as much as possible, while for the older elderly people, the community should increase the number of care services provided and improve the professionalism of care. The government can commission relevant third parties to conduct comprehensive research on the needs of the elderly and grasp the current situation related to the different types of elderly people. In addition, interviews or questionnaires can be conducted with the elderly in the community to obtain the actual needs of the elderly in the role of service providers. At the same time, information technology can be used to establish an information database for the elderly and create an effective file to record specific information about senior care services. Communities can conduct data analyses on these needs through the database and dynamically track senior satisfaction to assess service quality. Through the stages of pre-service research, in-service inquiry and post-service feedback, the community can dynamically manage the service quality of elderly care, pay attention to the effective subjective perceptions of the elderly in the process of using the service, establish an information feedback mechanism and service problem solutions, and improve the sustainability of the service operation.
(3) Integrate the layout of community public space and improve the community elderly care environment.
The unevenness of the current external living space of the environment of aging communities limits the diversified needs of the elderly, and the previous study found that there were generally problems such as small-scale public spaces, poor openness, and incomplete facilities with a lack of barrier-free environments in current community elderly service spaces. The construction of community public space should be re-integrated and laid out to enhance community livability and the level of the age-friendly living environment. Since elderly people have limited acting ability, a small activity range, and fixed activity location, multi-level public spaces should be planned according to the activity circle of elderly people to facilitate different outdoor activities such as walking, resting, chatting, and playing chess. For different types of aging communities, the community environment should also be differently configured and improved. For example, for aging communities with dense buildings and severe aging facilities, small public green areas can be built using open spaces between houses to improve the greening level of the community. Public passages and public spaces should be renovated for barrier-free facilities. For aging communities with a good community environment and public green space, on the one hand, the greening configuration and maintenance level of public green space can be improved, on the other hand, the openness of public green space can be improved by supporting the construction of leisure and fitness facilities and increasing outdoor activity space. For new elderly residential areas, they should not only ensure the land space of the community public green space, but also support the community square, small garden, and other public space. At the same time, the design of walking paths, squares, public green areas and public facilities should be fully implemented in the design of a barrier-free walking environment. All parts of the community elderly environment facilities should be interrelated and interact with each other to form an organic whole, to give full play to its role as the basic unit of elderly services and improve the overall level of satisfaction of the community elderly.
(4) Realize substantial community livability and aging-friendly transformation.
At present, most elderly people still live in old communities, and research shows that the lack of “quantity” and “quality” of community public facilities and public spaces, such as elderly care, education, and culture, restrict the development of community elderly care services. Therefore, the transformation of this old space is an important measure to complete the improvement in community elderly care patterns. As China has paid more attention to the stock planning in recent years, more renovations have been made to the existing communities in urban areas, but more focus is paid on the energy-saving renovations and pipeline improvements in old neighborhoods, lacking systematic sorting and in-depth research on the physiological and psychological needs of the elderly, which cannot create a spatial environment truly suitable for the elderly to live and work. Therefore, we should pay attention to the quality of the current community elderly service facilities and the creation of the community environment for the elderly. For example, with the help of “Internet Plus”, a new community management model can be established to create a wise, safe, and efficient intelligent community for the elderly. It provides health management, remote care, catering reservation, online elderly assistance, and emergency assistance services for the elderly. It improves management efficiency, achieves remote monitoring and real-time responses, keeps track of the physical and mental health of the elderly, learns about sudden diseases and takes preventive measures as early as possible. Through wireless network and cloud monitoring, the community can monitor the elderly’s outdoor activities and provide timely assistance in case of sudden falls and other conditions. The elderly can also enjoy medical and shopping services without having to leave home, which is convenient and fast.. It is important to emphasize that age-friendly renovation should start from meeting the needs of the elderly, paying special attention to the psychological needs, and be realized through universal design principles.. This will make community-based care an important part of pension system reform as a complementary pension structure system.






{kind=link}
{kind=link}
{kind=link}