
Development of the Readiness for Home-Based Palliative Care Scale (RHBPCS) for Primary Family Caregivers



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Setting
2.2. Instrument Development
2.3. Data Analysis
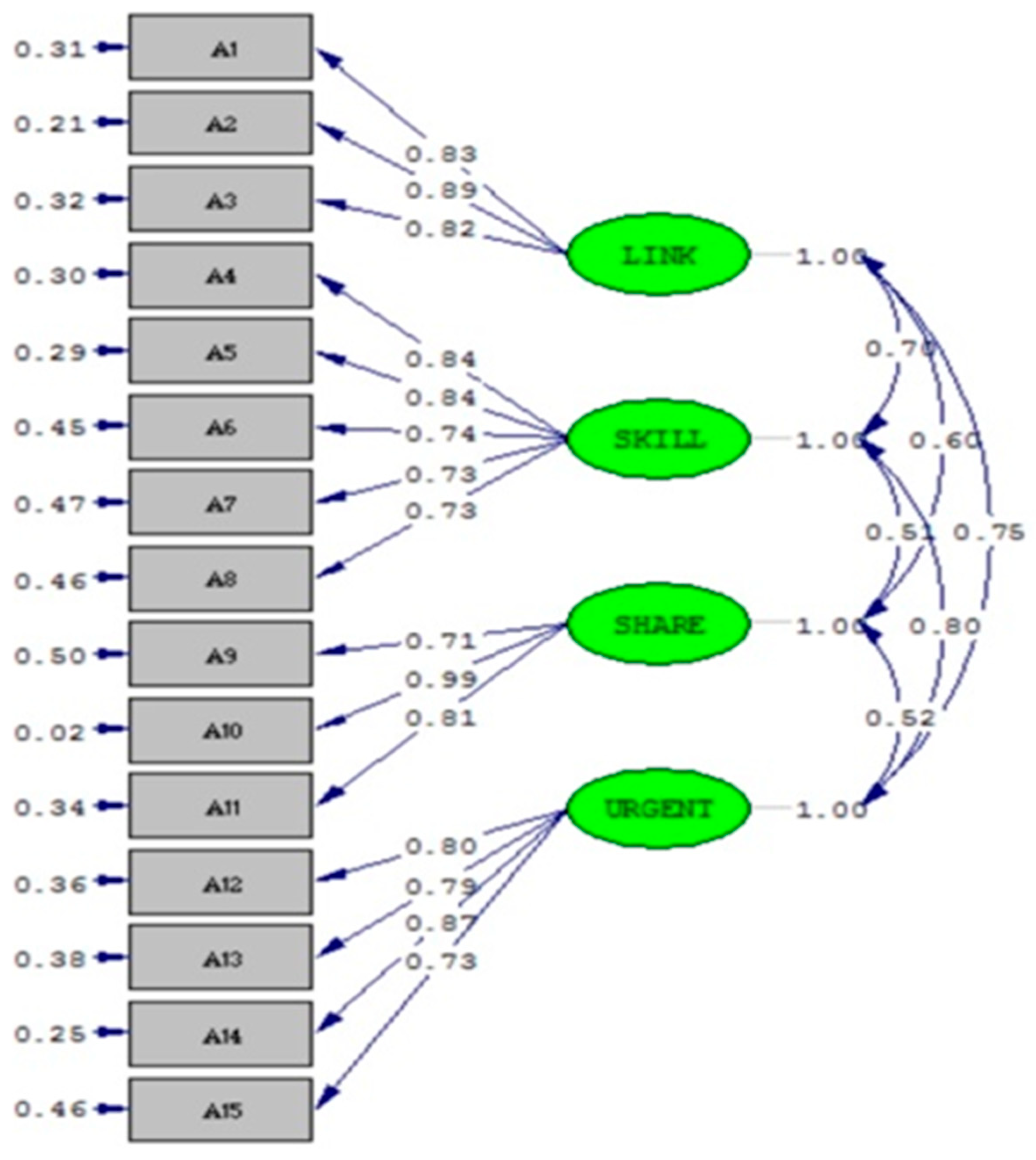
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Subscales and Items | NR | LR | SR | WR | FR |
|---|---|---|---|---|---|
| A. Family maintenance and consensus | |||||
| 1. Me and patient’s families have reached an agreement and have a thorough understanding of patient’s condition and the home-based palliative care. | □ | □ | □ | □ | □ |
| 2. I will follow patient’s wishes, prepare their basal diet and help them with simple exercise. | □ | □ | □ | □ | □ |
| 3.I can maintain a caring, perseverance, patient attitude or have a sense of morality and be spiritual supported. | □ | □ | □ | □ | □ |
| B. Home care skills and hospice preparation | |||||
| 4. I know how to prepare medications for patient. | □ | □ | □ | □ | □ |
| 5. I can use home medical supplies and equipment for the patient. | □ | □ | □ | □ | □ |
| 6. I have nursing skills to take care the patient. | □ | □ | □ | □ | □ |
| 7. I know the traditional culture and all the preparations for home death. | □ | □ | □ | □ | □ |
| 8. I know how to use the caring resources that provided for the home caregiver. | □ | □ | □ | □ | □ |
| C. Arrangements for sharing and rotation | |||||
| 9. I’m fully prepared to arrange the way of rotation. | □ | □ | □ | □ | □ |
| 10.I have time to get enough rest. | □ | □ | □ | □ | □ |
| 11. I am fully prepared for everything in order to take care the patient. | □ | □ | □ | □ | □ |
| D. Timely emergency management and palliative care | |||||
| 12. I know how to manage the patient’s symptoms. | □ | □ | □ | □ | □ |
| 13. I know how to make a contact in case of emergency. | □ | □ | □ | □ | □ |
| 14. I am preparing and I know how to manage the signs of death. | □ | □ | □ | □ | □ |
| 15. I can discussed with the patient about his/her state of an illness and last words. | □ | □ | □ | □ | □ |
References
- World Health Organization. Density of Hospice Centres (per 100,000 Population). Available online: http://apps.who.int/gho/data/node.wrapper.imr?x-id=5131 (accessed on 17 May 2021).
- World Health Organization. Media Centre-Palliative Care. Available online: http://www.who.int/mediacentre/factsheets/fs402/en/ (accessed on 17 May 2021).
- Currow, D.C.; Agar, M.R.; Phillips, J.L. Role of Hospice Care at the End of Life for People With Cancer. J. Clin. Oncol. 2020, 38, 937–943. [Google Scholar] [CrossRef] [PubMed]
- National Hospice and Palliative Care Organization. Hospice & Palliative Care: Hospice Care. Available online: https://www.nhpco.org/nhpco-edge-1 (accessed on 17 May 2021).
- National Hospice and Palliative Care Organization. Learn about End-of-Life Care. Available online: https://www.nhpco.org/learn-about-end-life-care (accessed on 17 May 2021).
- National Hospice and Palliative Care Organization. Angela Hospice Home Care, Inc. (Angela Hospice Care Center). Available online: https://www.nhpco.org/content/angela-hos-pice-home-care-inc-angela-hospice-care-center (accessed on 17 May 2021).
- National Hospice and Palliative Care Organization. Hospice Care. 2021. Available online: https://www.nhpco.org/about/hospice-care (accessed on 17 May 2021).
- Dugdale, D.C., III. Hospice Care. Available online: https://medlineplus.gov/ency/patientinstructions/000467.htm. (accessed on 17 May 2021).
- Worldwide Hospice Palliative Care Alliance. Hospice and Palliative Care Worldwide. Available online: http://www.thewhpca.org/get-informed/hospice-and-palliative-care-worldwide (accessed on 17 May 2021).
- McIlfatrick, S.; Doherty, L.C.; Murphy, M.; Dixon, L.; Donnelly, P.; McDonald, K.; Fitzsimons, D. ‘The importance of planning for the future’: Burden and unmet needs of caregivers’ in advanced heart failure: A mixed methods study. Palliat. Med. 2017, 32, 881–890. [Google Scholar] [CrossRef]
- Morey, T.; Scott, M.; Saunders, S.; Varenbut, J.; Howard, M.; Tanuseputro, P.; Webber, C.; Killackey, T.; Wentlandt, K.; Zimmermann, C.; et al. Transitioning From Hospital to Palliative Care at Home: Patient and Caregiver Perceptions of Continuity of Care. J. Pain Symptom Manag. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hampton, M.M.; Newcomb, P. Self-efficacy and Stress Among Informal Caregivers of Individuals at End of Life. J. Hosp. Palliat. Nurs. 2018, 20, 471–477. [Google Scholar] [CrossRef]
- Jack, B.A.; Mitchell, T.K.; Cope, L.C.; O’Brien, M.R. Supporting older people with cancer and life-limiting conditions dying at home: A qualitative study of patient and family caregiver experiences of Hospice at Home care. J. Adv. Nurs. 2016, 72, 2162–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.-P.; Huang, S.-J.; Tsao, L.-I. The Life Experiences Among Primary Family Caregivers of Home-Based Palliative Care. Am. J. Hosp. Palliat. Med. 2020, 37, 816–822. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Ding, L.; Velicer, W.F.; Harlow, L.L. Effects of estimation methods, number of indicators per factor, and improper solutions on structural equation modeling fit indices. Struct. Equ. Model. A Multidiscip. J. 1995, 2, 119–143. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 2nd ed.; Prentice-Hall: Upper Saddle River, NJ, USA, 2000. [Google Scholar]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 5th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Hoyle, R.H. The structural equation modeling approach: Basic concepts and fundamental issues. In Structural Equation Modeling: Concepts, Issues, and Applications; Hoyle, R.H., Ed.; Sage Publications, Inc: London, UK, 1995; pp. 1–15. [Google Scholar]
- Waltz, C.F.; Strickland, O.L.; Lenz, E.R.; Satyshur, R.D.; Stone, K.S.; Frazier, S.K.; Ryan-Wenger, N.A.; Antol, S.; Scisney-Matlock, M.; Hupcey, J.E.; et al. Measurement in Nursing and Health Research, 5th ed.; Springer Publishing Company: New York, NY, USA, 2016. [Google Scholar]
- Allende-Pérez, S.; González, P.; Peña-Nieves, A.; Herrera-Gómez, Á.; Verástegui, E. End-of-Life Admission to the Emergency Department: Experience of Mexico’s National Cancer Institute of a Developing Country. Am. J. Hosp. Palliat. Med. 2020, 37, 881–884. [Google Scholar] [CrossRef]
- Hudson, P. Positive aspects and challenges associated with caring for a dying relative at home. Int. J. Palliat. Nurs. 2004, 10, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Stajduhar, K.I.; Martin, W.L.; Barwich, D.; Fyles, G. Factors Influencing Family Caregivers’ Ability to Cope With Providing End-of-Life Cancer Care at Home. Cancer Nurs. 2008, 31, 77–85. [Google Scholar] [CrossRef]
- Given, B.; Sherwood, P.R.; Given, C.W. What Knowledge And Skills Do Caregivers Need? J. Soc. Work. Educ. 2008, 44, 115–123. [Google Scholar] [CrossRef]
- Soroka, J.T.; Froggatt, K.; Morris, S. Family Caregivers’ Confidence Caring for Relatives in Hospice Care at Home: An Exploratory Qualitative Study. Am. J. Hosp. Palliat. Med. 2018, 35, 1540–1546. [Google Scholar] [CrossRef]
- Farquhar, M.; Penfold, C.; Benson, J.; Lovick, R.; Mahadeva, R.; Howson, S.; Burkin, J.; Booth, S.; Gilligan, D.; Todd, C.; et al. Six key topics informal carers of patients with breathlessness in advanced disease want to learn about and why: MRC phase I study to inform an educational intervention. PLoS ONE 2017, 12, e0177081. [Google Scholar] [CrossRef] [Green Version]
- Glass, A.P.; Chen, L.-K.; Hwang, E.; Ono, Y.; Nahapetyan, L. A Cross-Cultural Comparison of Hospice Development in Japan, South Korea, and Taiwan. J. Cross-Cult. Gerontol. 2010, 25, 1–19. [Google Scholar] [CrossRef]
- Lee, Y.S.; Akhileswaran, R.; Ong, E.H.; Wah, W.; Hui, D.; Ng, S.H.; Koh, G. Clinical and Socio-Demographic Predictors of Home Hos-pice Patients Dying at Home: A Retrospective Analysis of Hospice Care Association’s Database in Singapore. J. Pain Symptom Manag. 2017, 53, 1035–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobb, E.A.; Bindley, K.; Sanderson, C.; MacLeod, R.; Mowll, J. Navigating the path to care and death at home—it is not always smooth: A qualitative examination of the experiences of bereaved family caregivers in palliative care. J. Psychosoc. Oncol. Res. Pract. 2019, 1, e3. [Google Scholar] [CrossRef]
- Schumacher, K.; Beck, C.A.; Marren, J.M. Family Caregivers: Caring for older adults, working with their families. Am. J. Nurs. 2006, 106, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Oechsle, K.; Ullrich, A.; Marx, G.; Benze, G.; Heine, J.; Dickel, L.-M.; Zhang, Y.; Wowretzko, F.; Wendt, K.N.; Nauck, F.; et al. Psychological burden in family caregivers of patients with advanced cancer at initiation of specialist inpatient palliative care. BMC Palliat. Care 2019, 18, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Shepperd, S.; Gonçalves-Bradley, D.C.; Straus, S.E.; Wee, B. Hospital at home: Home-based end-of-life care. Cochrane Database Syst. Rev. 2021, 3, CD009231. [Google Scholar] [PubMed]
- Bradshaw, A.; Santarelli, M.; Mulderrig, M.; Khamis, A.; Sartain, K.; Boland, J.W.; Bennett, M.I.; Johnson, M.; Pearson, M.; Murtagh, F.E.M. Implementing person-centred outcome measures in palliative care: An exploratory qualitative study using Normalisation Process Theory to understand processes and context. Palliat. Med. 2021, 35, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Ewing, G.; Grande, G.; on behalf of the National Association for Hospice at Home. Development of a Carer Support Needs Assessment Tool (CSNAT) for end-of-life care practice at home: A qualitative study. Palliat. Med. 2012, 27, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Ewing, G.; Brundle, C.; Payne, S.; Grande, G. The Carer Support Needs Assessment Tool (CSNAT) for Use in Palliative and End-of-life Care at Home: A Validation Study. J. Pain Symptom Manag. 2013, 46, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Seow, H.; Bainbridge, D. A Review of the Essential Components of Quality Palliative Care in the Home. J. Palliat. Med. 2018, 21, 37–44. [Google Scholar] [CrossRef]

| Variable | n | (%) |
|---|---|---|
| Sex | ||
| Male | 33 | (32.0) |
| Female | 70 | (68.0) |
| Age | ||
| Under 50 years | 18 | (17.5) |
| 51–60 years | 31 | (30.1) |
| 61–70 years | 39 | (7.9) |
| 71–80 years | 9 | (8.7) |
| Above 81 yrs | 6 | (5.8) |
| Education | ||
| Under elementary school | 14 | (13.6) |
| Junior high school | 7 | (6.8) |
| High school | 25 | (24.3) |
| Some college or associate degree | 57 | (55.3) |
| Married status | ||
| Unmarried | 20 | (19.4) |
| Married | 75 | (72.8) |
| Divorced | 2 | (1.9) |
| Widowed | 6 | (5.8) |
| Religion | ||
| Taoism | 31 | (30.1) |
| Buddhism | 39 | (37.9) |
| Christianity | 9 | (8.7) |
| Others | 7 | (6.8) |
| None | 17 | (16.5) |
| Occupation | ||
| Retiree | 37 | (35.9) |
| Homemaker | 26 | (25.2) |
| Public sector | 6 | (5.8) |
| Business | 13 | (12.6) |
| Service industry | 17 | (16.5) |
| Others | 1 | (1.0) |
| None | 3 | (2.9) |
| Caregiver relationship | ||
| Couple | 23 | (22.3) |
| Son or daughter | 58 | (56.3) |
| Daughter-in-law | 13 | (12.6) |
| Other relatives | 9 | (8.8) |
| Care time | ||
| <1 year | 23 | (22.3) |
| 1–3 year | 34 | (33.0) |
| ≥3 year | 46 | (44.7) |
| Couple | 24 | (23.3) |
| Son or daughter | 14 | (13.6) |
| Other relatives | 38 | (36.9) |
| None | 27 | (26.2) |
| Chronic disease | ||
| Yes | 45 | (43.7) |
| No | 58 | (56.3) |
| Patient diagnosis | ||
| Cancer | 36 | (35.0) |
| None-cancer | 67 | (65.0) |
| Sub-Scale | Number of Items | Cronbach’s α |
|---|---|---|
| Family maintenance and consensus | 3 | 0.859 |
| Home care skills and hospice preparation | 5 | 0.879 |
| Arrangements for sharing and rotation | 3 | 0.875 |
| Timely emergency management and palliative care | 4 | 0.860 |
| Total scale of the RHBPCS | 15 | 0.928 |
| Items | t-Value | p-Value |
|---|---|---|
| 1. Me and patient’s families have reached an agreement and have a thorough understanding of patient’s condition and the home-based palliative care. | 3.959 | <0.001 |
| 2. I’m fully prepared to arrange the way of rotation. | 3.034 | 0.004 |
| 3.I have time to get enough rest. | 5.014 | 0.000 |
| 4. I know how to manage the patient’s symptoms. | 3.813 | <0.001 |
| 5. I know how to prepare medications for patient. | 2.540 | 0.014 |
| 6. I know how to make a contact in case of emergency. | 2.553 | 0.014 |
| 7. I can use home medical supplies and equipment for the patient. | 2.780 | 0.007 |
| 8. I have nursing skills to take care the patient. | 3.545 | 0.001 |
| 9. I will follow patient’s wishes, prepare their basal diet and help them with simple exercise. | 2.553 | 0.014 |
| 10. I know the traditional culture and all the preparations for home death. | 4.076 | <0.001 |
| 11. I am preparing and I know how to manage the signs of death. | 4.666 | <0.001 |
| 12. I can discussed with the patient about his/her state of an illness and last words. | 5.284 | <0.001 |
| 13. I am fully prepared for everything in order to take care the patient. | 3.576 | 0.001 |
| 14.I can maintain a caring, perseverance, patient attitude or have a sense of morality and be spiritual supported. | 3.545 | 0.001 |
| 15.I know how to use the caring resources that provided for the home caregiver. | 3.667 | 0.001 |
| Items | Item Deleted Cronbach’s α | Item-Total Correlation |
|---|---|---|
| 1. Me and patient’s families have reached an agreement and have a thorough understanding of patient’s condition and the home-based palliative care. | 0.902 | 0.696 *** |
| 2. I’m fully prepared to arrange the way of rotation. | 0.909 | 0.522 *** |
| 3. I have time to get enough rest. | 0.904 | 0.660 *** |
| 4. I know how to manage the patient’s symptoms. | 0.902 | 0.688 *** |
| 5. I know how to prepare medications for patient. | 0.900 | 0.744 *** |
| 6. I know how to make a contact in case of emergency. | 0.904 | 0.660 *** |
| 7. I can use home medical supplies and equipment for the patient. | 0.901 | 0.740 *** |
| 8. I have nursing skills to take care the patient. | 0.903 | 0.671 ** |
| 9. I will follow patient’s wishes, prepare their basal diet and help them with simple exercise. | 0.901 | 0.752 *** |
| 10. I know the traditional culture and all the preparations for home death. | 0.904 | 0.680 *** |
| 11. I am preparing and I know how to manage the signs of death. | 0.900 | 0.753 *** |
| 12. I can discussed with the patient about his/her state of an illness and last words. | 0.905 | 0.678 *** |
| 13. I am fully prepared for everything in order to take care the patient. | 0.907 | 0.551 *** |
| 14.I can maintain a caring, perseverance, patient attitude or have a sense of morality and be spiritual supported. | 0.902 | 0.704 *** |
| 15.I know how to use the caring resources that provided for the home caregiver. | 0.905 | 0.605 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, M.-P.; Tsao, L.-I.; Huang, S.-J.; Liu, C.-Y. Development of the Readiness for Home-Based Palliative Care Scale (RHBPCS) for Primary Family Caregivers. Healthcare 2021, 9, 608. https://doi.org/10.3390/healthcare9050608
Wu M-P, Tsao L-I, Huang S-J, Liu C-Y. Development of the Readiness for Home-Based Palliative Care Scale (RHBPCS) for Primary Family Caregivers. Healthcare. 2021; 9(5):608. https://doi.org/10.3390/healthcare9050608
Chicago/Turabian StyleWu, Meng-Ping, Lee-Ing Tsao, Sheng-Jean Huang, and Chieh-Yu Liu. 2021. "Development of the Readiness for Home-Based Palliative Care Scale (RHBPCS) for Primary Family Caregivers" Healthcare 9, no. 5: 608. https://doi.org/10.3390/healthcare9050608