
A Validation Study on the Frequency and Natural History of Miscarriages Using the Spanish Primary Care Database BIFAP


Abstract
:1. Introduction
2. Materials and Methods
2.1. Source of Data
2.2. Source Population
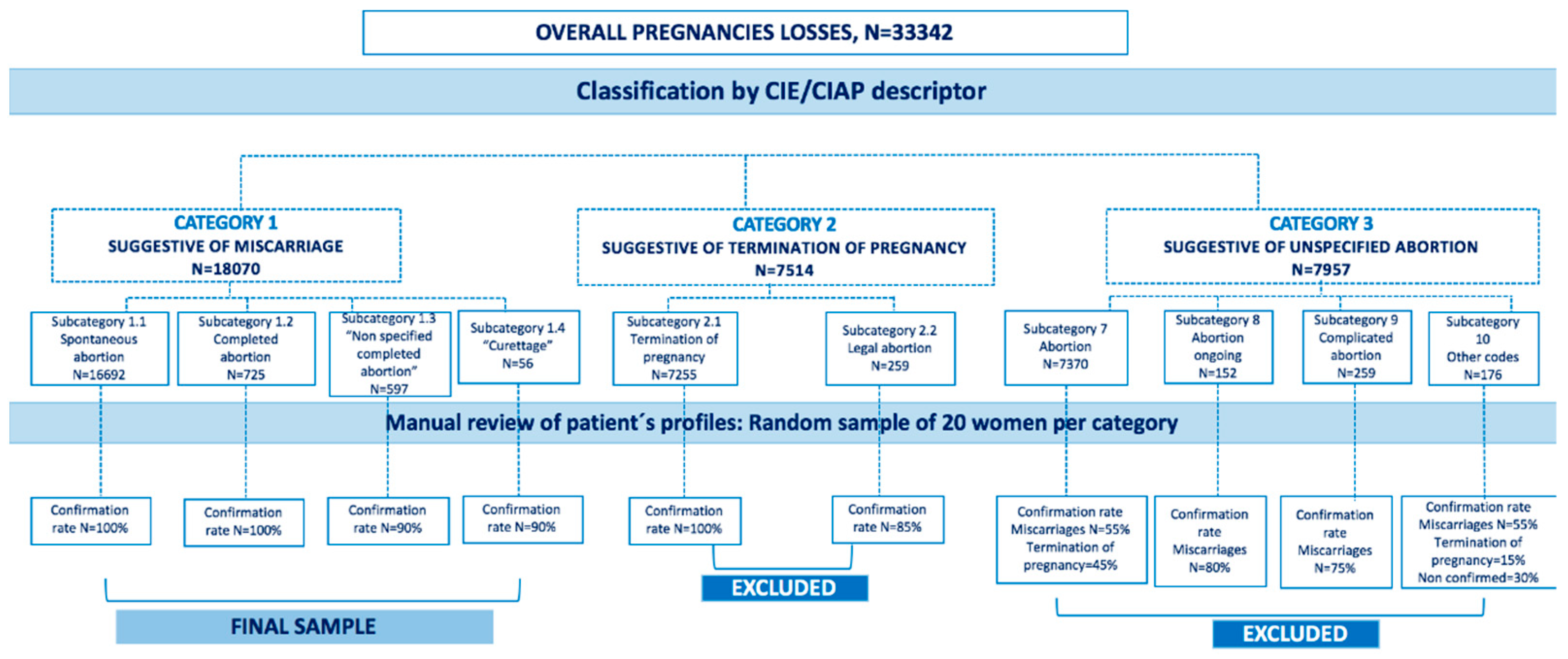
2.3. Separating Miscarriages from All Pregnancy Losses Validation Steps
2.4. Validation of Categories of Pregnancy Losses: Miscarriage, Termination of Pregnancy, and Unspecified Abortion
2.5. Cohort Analysis
- -
- Pregnancy loss (i.e., miscarriage, TOP, and unspecified abortions);
- -
- 154 days (22 weeks) that was the upper limit of the gestational age to consider a pregnancy loss;
- -
- Death.
2.6. Ascertainment of Exposure and Covariates
2.7. Ascertainment of Drug Exposure
2.8. Analysis
3. Results
3.1. Baseline Characteristics
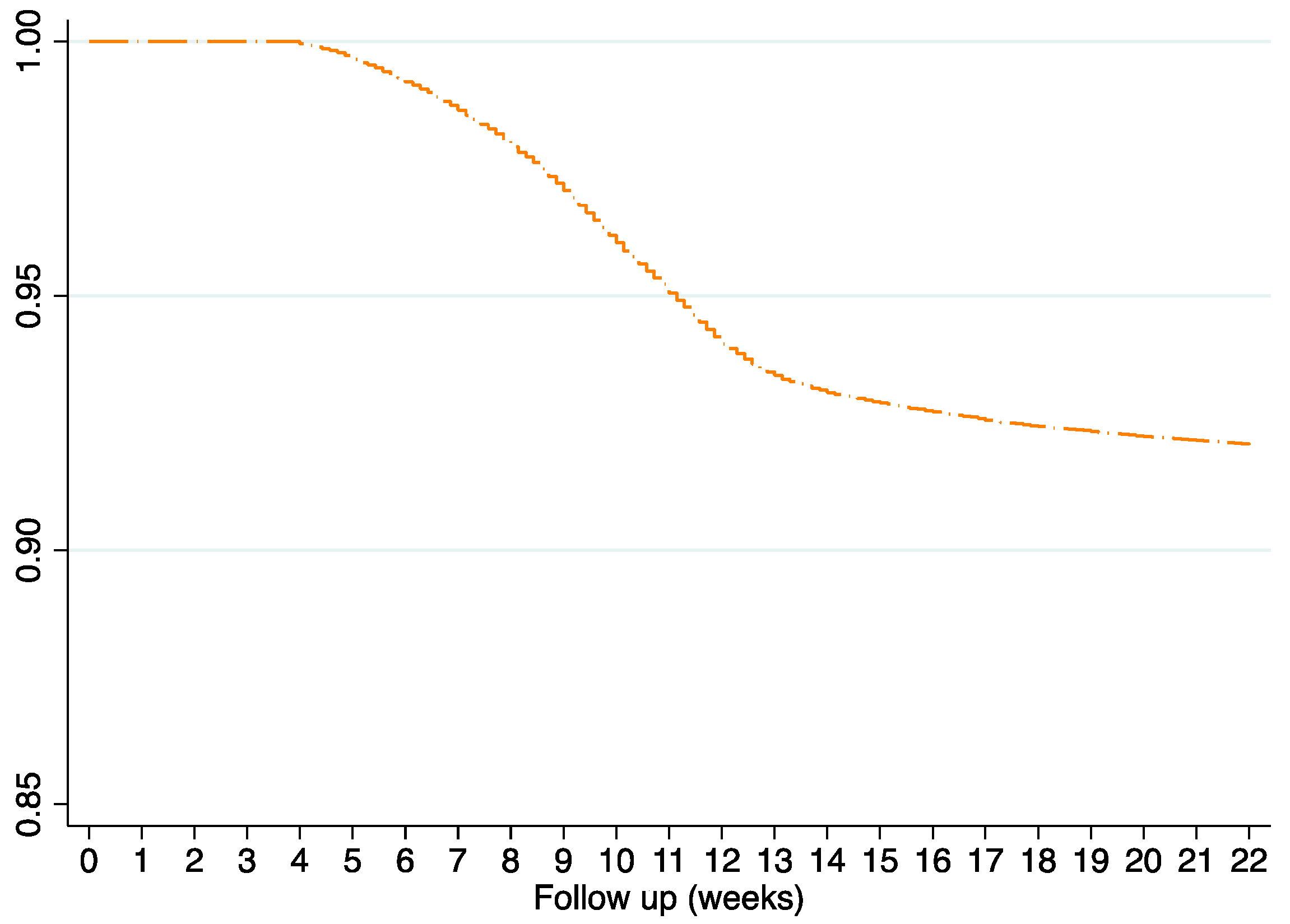
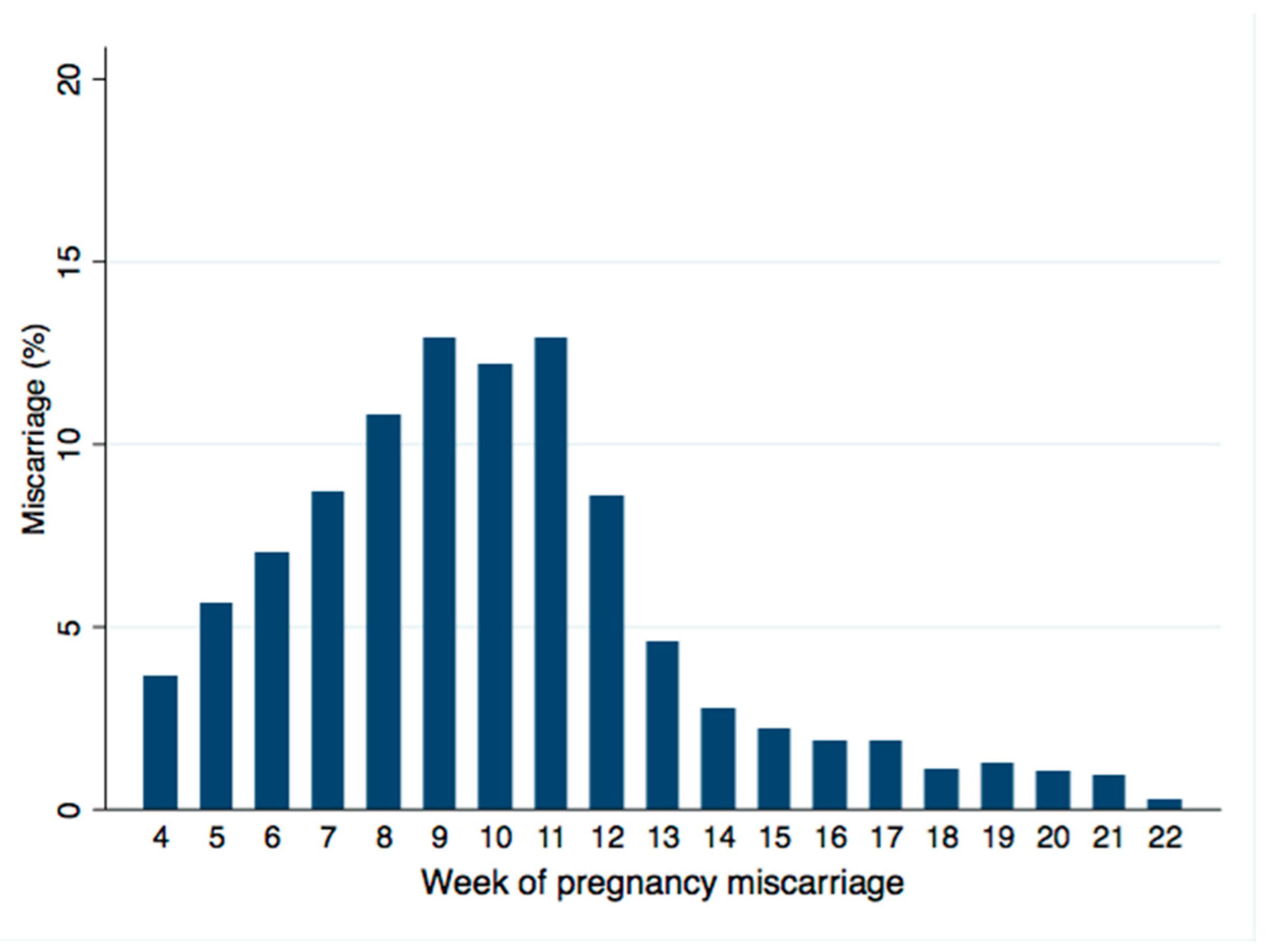
3.2. Overall Incidence of Miscarriage
3.3. Specific Groups Restricted to Women with LMP Date Recorded
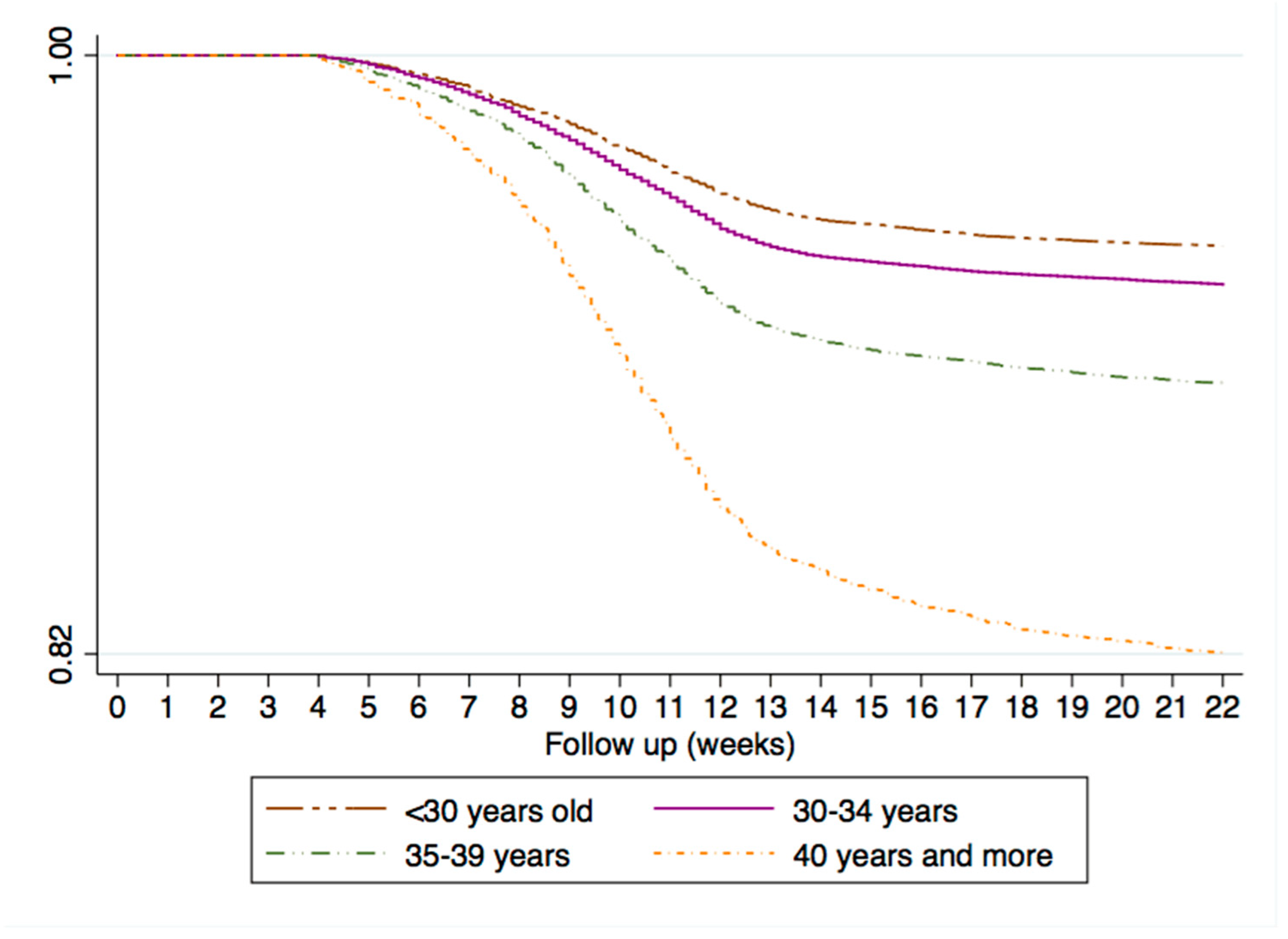
3.4. Predictors for Miscarriages
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poorolajal, J.; Cheraghi, P.; Cheraghi, Z.; Ghahramani, M.; Doosti Irani, A. Predictors of miscarriage: A matched case-control study. Epidemiol. Health 2014, 36, e2014031. [Google Scholar] [CrossRef] [Green Version]
- Magnus, M.C.; Wilcox, A.J.; Morken, N.H.; Weinberg, C.R.; Håberg, S.E. Role of maternal age and pregnancy history in risk of miscarriage: Prospective register based study. BMJ 2019, 364, I869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooke, A.; Mills, T.A.; Lavender, T. Advanced maternal age: Delayed childbearing is rarely a conscious choice a qualitative study of women’s views and experiences. Int. J. Nurs. Stud. 2012, 49, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.P.; Rossetti, E.; Pittini, C.; Cagnacci, A.; Driul, L. Maternal age and the risk of adverse pregnancy outcomes: A retrospective cohort study. BMC Pregnancy Childbirth 2019, 19, 261. [Google Scholar] [CrossRef] [PubMed]
- De la Rochebrochard, E.; Thonneau, P. Paternal age and maternal age are risk factors for miscarriage; results of a multicentre European study. Hum. Reprod. 2002, 17, 1649–1656. [Google Scholar] [CrossRef] [Green Version]
- Radoń-Pokracka, M.; Adrianowicz, B.; Płonka, M.; Danił, P.; Nowak, M.; Huras, H. Evaluation of Pregnancy Outcomes at Advanced Maternal Age. Open Access Maced. J. Med. Sci. 2019, 7, 1951–1956. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, K.; Urayama, K.Y.; Tanigaki, S.; Sago, H.; Sato, S.; Saito, S.; Morisaki, N. Association between very advanced maternal age and adverse pregnancy outcomes: A cross sectional Japanese study. BMC Pregnancy Childbirth 2017, 17, 349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-David, A.; Glasser, S.; Schiff, E.; Zahav, A.S.; Boyko, V.; Lerner-Geva, L. Pregnancy and Birth Outcomes Among Primiparae at Very Advanced Maternal Age: At What Price? Matern. Child Health J. 2016, 20, 833–842. [Google Scholar] [CrossRef]
- Almeida, N.K.O.; Almeida, R.M.V.R.; Pedreira, C.E. Adverse perinatal outcomes for advanced maternal age: A cross-sectional study of Brazilian births. J. Pediatr. 2015, 91, 493–498. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Tanbo, T.; Åbyholm, T.; Henriksen, T. The impact of advanced maternal age and parity on obstetric and perinatal outcomes in singleton gestations. Arch. Gynecol. Obstet. 2011, 284, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Woolner, A.M.F.; Raja, E.A.; Bhattacharya, S.; Danielian, P.; Bhattacharya, S. Inherited susceptibility to miscarriage: A nested case-control study of 31,565 women from an intergenerational cohort. Am. J. Obstet. Gynecol. 2020, 222, 168.e1–168.e8. [Google Scholar] [CrossRef] [PubMed]
- Feodor Nilsson, S.; Andersen, P.K.; Strandberg-Larsen, K.; Nybo Andersen, A.M. Risk factors fot miscarriage from a prevention perspective: A nationwide follow up study. BJOG 2014, 121, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S. Modifiable risk factors for miscarriage identified. Evid. Based Nurs. 2015, 18, 72. [Google Scholar] [CrossRef]
- Bu, Z.; Hu, L.; Su, Y.; Guo, Y.; Zhai, J.; Sun, Y.P. Factors related to early spontaneous miscarriage during IVF/ICSI treatment: An analysis of 21,485 clinical pregnancies. Reprod. Biomed. Online 2020, 40, 201–206. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, R.; Hart, R.J. Pregnancy-related outcomes for women with polycystic ovary syndrome. Womens Health 2017, 13, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Combs, C.A.; Kitzmiller, J.L. Spontaneous abortion and congenital malformations in diabetes. Baillieres Clin. Obstet. Gynaecol. 1991, 5, 315–331. [Google Scholar] [CrossRef]
- McGrogan, A.; Snowball, J.; de Vries, C.S. Pregnancy losses in women with Type 1 or Type 2 diabetes in the UK: An investigation using primary care records. Diabet. Med. 2014, 31, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Lohse, S.R.; Farkas, D.K.; Lohse, N.; Skouby, S.O.; Nielsen, F.E.; Lash, T.L.; Ehrenstein, V. Validation of spontaneous abortion diagnoses in the Danish National Registry of Patients. Clin. Epidemiol. 2010, 2, 247–250. [Google Scholar] [CrossRef] [Green Version]
- Quinley, K.E.; Falck, A.; Kallan, M.J.; Datner, E.M.; Carr, B.G.; Schreiber, C.A. Validation of ICD-9 Codes for Stable Miscarriage in the Emergency Department. W. J. Emerg. Med. 2015, 16, 551–556. [Google Scholar] [CrossRef] [Green Version]
- Maciá-Martínez, M.A.; Gil, M.; Huerta, C.; Martín-Merino, E.; Álvarez, A.; Bryant, V.; Montero, D.; BIFAP Team. Base de Datos para la Investigación Farmacoepidemiológica en Atención Primaria (BIFAP): A data resource for pharmacoepidemiology in Spain. Pharmacoepidemiol. Drug Saf. 2020, 29, 1236–1245. [Google Scholar] [CrossRef]
- Gobernanza del Acceso a los Datos de BIFAP Agencia Española de Medicamentos y Productos Sanitarios (n.d.). 28 January 2021. Available online: http://bifap.aemps.es/docs/Gobernanza_acceso_datos_BIFAP_v1_Junio2017.pdf (accessed on 4 January 2021).
- World Organization of Family Doctors (WONCA) International Classification Committee. International Classification of Primary Care (ICPC), 2nd ed; Oxford Medical Publications; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Ministerio de Sanidad, Servicios Sociales e Igualdad, Dirección General de Salud Pública, Calidad e Innovación, Subdirección General de Información Sanitaria e Innovación (n.d.). Edición Electrónica de la CIE-9- MC. Clasificación Internacional de EnferMedades 9a Revisión, Modificación Cínica. 28 January 2021. Available online: https://eciemaps.mscbs.gob.es/ecieMaps/browser/index_9_mc.html (accessed on 4 January 2021).
- WHO Collaborating Centre for Drug Statistics Methodology (n.d) ATC/DDD Index. 28 January 2021. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 4 January 2021).
- Gil, M.; Rodríguez-Miguel, A.; Montoya-Catalá, H.; González-González, R.; Álvarez-Gutiérrez, A.; Rodríguez-Martín, S.; García-Rodríguez, L.A.; de Abajo, F.J. Validation study of colorectal cancer diagnosis in the Spanish primary care database, BIFAP. Pharmacoepidemiol. Drug Saf. 2019, 28, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Cea-Soriano, L.; García Rodríguez, L.A.; Fernández Cantero, O.; Hernández-Díaz, S. Challenges of using primary care electronic medical records in the UK to study medications in pregnancy. Pharmacoepidemiol. Drug Saf. 2013, 22, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Sanchez Ortiz, S.; Llorente García, A.; Astasio, P.; Huerta, C.; Cea Soriano, L. An algorithm to identify pregnancies in BIFAP Primary Care database in Spain: Results from a cohort of 155 419 pregnancies. Pharmacoepidemiol. Drug Saf. 2020, 29, 57–68. [Google Scholar] [CrossRef]
- Wilcox, A.J.; Weinberg, C.R.; O’Connor, J.F.; Baird, D.D.; Schlatterer, J.P.; Canfield, R.E.; Armstrong, E.G.; Nisula, B.C. Incidence of early loss of pregnancy. N. Engl. J. Med. 1988, 319, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Almeida, N.D.; Basso, O.; Abrahamowicz, M.; Gagnon, R.; Tamblyn, R. Risk of Miscarriage in Women Receiving Antidepressants in Early Pregnancy, Correcting for Induced Abortions. Epidemiology 2016, 27, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Rossen, L.M.; Ahrens, K.A.; Branum, A.M. Trends in Risk of Pregnancy Loss Among US Women, 1990–2011. Paediatr. Perinat. Epidemiol. 2018, 32, 19–29. [Google Scholar] [CrossRef]
- Adolfsson, A.; Larsson, P.G. Cumulative incidence of previous spontaneous abortion in Sweden in 1983-2003: A register study. Acta Obstet. Gynecol. Scand. 2006, 85, 741–747. [Google Scholar] [CrossRef]
- Hemminki, E.; Forssas, E. Epidemiology of miscarriage and its relation to other reproductive events in Finland. Am. J. Obstet. Gynecol. 1999, 181, 396–401. [Google Scholar] [CrossRef]
- Marinescu, I.P.; Foarfă, M.C.; Pîrlog, M.C.; Turculean, A. Prenatal depression and stress—Risk factors for placental pathology and spontaneous abortion. Rom. J. Morphol. Embryol. 2014, 55, 1155–1160. [Google Scholar]
- Oppong, S.A.; Torto, M.; Beyuo, T. Risk factors and pregnancy outcome in women aged over 40 years at Korle-Bu Teaching Hospital in Accra, Ghana. Int. J. Gynaecol. Obstet. 2019. [CrossRef]
- De Viti, D.; Malvasi, A.; Busardò, F.; Beck, R.; Zaami, S.; Marinelli, E. Cardiovascular Outcomes in Advanced Maternal Age Delivering Women. Clinical Review and Medico-Legal Issues. Medicina 2019, 55, 658. [Google Scholar]
- Luke, B.; Brown, M.B. Elevated risks of pregnancy complications and adverse outcomes with increasing maternal age. Hum. Reprod. 2007, 22, 1264–1272. [Google Scholar] [CrossRef] [Green Version]
- Laopaiboon, M.; Lumbiganon, P.; Intarut, N.; Mori, R.; Ganchimeg, T.; Vogel, J.P.; Souza, J.P.; Gülmezoglu, A. M WHO Multicountry Survey on Maternal Newborn Health Research Networ. Advanced maternal age and pregnancy outcomes: A multicountry assessment. BJOG 2014, 121, 49–56. [Google Scholar] [PubMed] [Green Version]
- Dietl, A.; Cupisti, S.; Beckmann, M.W.; Schwab, M.; Zollner, U. Pregnancy and obstetrical outcomes in women over 40 years of age. Geburtshilfe Frauenheilkd 2015, 75, 827–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abalos, E.; Duley, L.; Steyn, D.W.; Gialdini, C. Antihypertensive drug therapy for mild to moderate hypertension during pregnancy. Cochrane Database Syst. Rev. 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Cea-Soriano, L.; García-Rodríguez, L.A.; Brodovicz, K.G.; Masso Gonzalez, E.; Bartels, D.B.; Hernández-Díaz, S. Safety of non-insulin glucose-lowering drugs in pregnant women with pre-gestational diabetes: A cohort study. Diabetes Obes. Metab. 2018, 20, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Cuneo, B.F.; Kaizer, A.M.; Clur, S.A.; Swan, H.; Herberg, U.; Winbo, A.; Rydberg, A.; Haugaa, K.; Etheridge, S.; Ackerman, M.J.; et al. Mothers with long QT syndrome are at increased risk for fetal death: Findings from a multicenter international study. Am. J. Obstet. Gynecol. 2020, 222, 263.e1–263.e11. [Google Scholar] [CrossRef]
- Stryuk, R.I.; Burns, C.A.; Filippov, M.P.; Brytkova, Y.V.; Borisov, I.V.; Barkova, E.L.; Gomova, T.A.; Kozina, E.A.; Nagirnyak, O.A. Cardiovascular disease and associated comorbid conditions as determinants of adverse perinatal outcomes in pregnancy—An analysis of the results of the register of pregnant BEREG. Ter. Arkh. 2018, 90, 9–16. [Google Scholar] [CrossRef]
- Kelly, R.; Holzman, C.; Senagore, P.; Wang, J.; Tian, Y.; Rahbar, M.H.; Chung, H. Placental vascular pathology findings and pathways to preterm delivery. Am. J. Epidemiol. 2009, 170, 148–158. [Google Scholar] [CrossRef]
- Richardson, J.L.; Martin, F.; Dunstan, H.; Greenall, A.; Stephens, S.; Yates, L.M.; Thomas, S.H. Pregnancy outcomes following maternal venlafaxine use: A prospective observational comparative cohort study. Reprod. Toxicol. 2019, 84, 108–113. [Google Scholar] [CrossRef]
- Blotière, P.O.; Weill, A.; Dalichampt, M.; Billionnet, C.; Mezzarobba, M.; Raguideau, F.; Dray-Spira, R.; Zureik, M.; Coste, J.; Alla, F. Development of an algorithm to identify pregnancy episodes and related outcomes in health care claims databases: An application to antiepileptic drug use in 4.9 million pregnant women in France. Pharmacoepidemiol. Drug Saf. 2018, 27, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Charlton, R.A.; Cunnington, M.C.; de Vries, C.S.; Weil, J.G. Data resources for investigating drug exposure during pregnancy and associated outcomes: The General Practice Research Database (GPRD) as an alternative to pregnancy registries. Drug Saf. 2008, 31, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Toh, S.; Mitchell, A.A.; Werler, M.M.; Hernández-Díaz, S. Sensitivity and specificity of computerized algorithms to classify gestational periods in the absence of information on date of conception. Am. J. Epidemiol. 2008, 167, 633–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Women with Miscarriage | Remaining Pregnant Women | ||||||
|---|---|---|---|---|---|---|---|---|
| LMP Date Recorded N = 7827 | LMP Date Imputed N = 10,243 | LMP Date Recorded N = 93,480 | LMP Date Imputed N = 43,869 | |||||
| N | % | N | % | N | % | N | % | |
| Age | ||||||||
| <30 years | 1731 | 22.1 | 2161 | 21.1 | 29,051 | 31.1 | 12,845 | 29.3 |
| 30–34 years | 2685 | 34.3 | 3265 | 31.9 | 36,744 | 39.3 | 15,655 | 35.7 |
| 35–39 years | 2462 | 31.5 | 3204 | 31.3 | 23,072 | 24.7 | 11,986 | 27.3 |
| ≥40 years | 949 | 12.1 | 1613 | 15.7 | 4613 | 4.9 | 3383 | 7.7 |
| Obesity | 612 | 7.8 | 735 | 7.2 | 6540 | 7.0 | 2549 | 5.8 |
| Smoke | 683 | 8.7 | 982 | 9.6 | 7160 | 7.7 | 3267 | 7.4 |
| Anemia | 50 | 0.6 | 51 | 0.5 | 414 | 0.4 | 171 | 0.4 |
| Anxiety | 1472 | 18.8 | 1766 | 17.2 | 16,132 | 17.3 | 6581 | 15.0 |
| Asthma | 398 | 5.1 | 525 | 5.1 | 4648 | 5.0 | 2082 | 4.7 |
| Depression | 745 | 9.5 | 978 | 9.5 | 7271 | 7.8 | 3329 | 7.6 |
| Diabetes | 66 | 0.8 | 114 | 1.1 | 562 | 0.6 | 311 | 0.7 |
| Epilepsy | 48 | 0.6 | 65 | 0.6 | 549 | 0.6 | 289 | 0.7 |
| Hypercholesterolemia | 318 | 4.1 | 449 | 4.4 | 3516 | 3.8 | 1438 | 3.3 |
| Hypertension | 123 | 1.6 | 153 | 1.5 | 951 | 1.0 | 493 | 1.1 |
| Hypothyroidism | 612 | 7.8 | 643 | 6.3 | 6057 | 6.5 | 2248 | 5.1 |
| Irritable Bowel Syndrome | 160 | 2.0 | 199 | 1.9 | 1719 | 1.8 | 712 | 1.6 |
| Migraine | 534 | 6.8 | 689 | 6.7 | 5770 | 6.2 | 2434 | 5.5 |
| Multiple Sclerosis | 10 | 0.1 | 12 | 0.1 | 153 | 0.2 | 64 | 0.1 |
| Psychiatric antecedents * | 110 | 1.4 | 151 | 1.5 | 1031 | 1.1 | 528 | 1.2 |
| Metabolic antecedents φ | 167 | 2.1 | 168 | 1.6 | 1599 | 1.7 | 574 | 1.3 |
| Acid suppressant | 406 | 5.2 | 552 | 5.4 | 4397 | 4.7 | 1890 | 4.3 |
| Antibiotics | 947 | 12.1 | 1205 | 11.8 | 10,746 | 11.5 | 4607 | 10.5 |
| Antiepileptics | 55 | 0.7 | 93 | 0.9 | 576 | 0.6 | 337 | 0.8 |
| Antihistamines | 379 | 4.8 | 437 | 4.3 | 4242 | 4.5 | 1687 | 3.8 |
| Antihypertensives | 89 | 1.1 | 121 | 1.2 | 518 | 0.6 | 327 | 0.7 |
| Antimigraine drugs | 66 | 0.8 | 79 | 0.8 | 604 | 0.6 | 239 | 0.5 |
| Benzodiazepines | 416 | 5.3 | 549 | 5.4 | 3880 | 4.2 | 1909 | 4.4 |
| Codeine | 74 | 0.9 | 101 | 1.0 | 883 | 0.9 | 430 | 1.0 |
| Folic Acid | 744 | 9.5 | 624 | 6.1 | 8302 | 8.9 | 2227 | 5.1 |
| Oral Corticosteroids | 181 | 2.3 | 277 | 2.7 | 2305 | 2.5 | 995 | 2.3 |
| Respiratory drugs | 504 | 6.4 | 564 | 5.5 | 5649 | 6.0 | 2195 | 5.0 |
| SSRIs | 179 | 2.3 | 255 | 2.5 | 1597 | 1.7 | 885 | 2.0 |
| Thyroid hormone | 212 | 2.7 | 208 | 2.0 | 1798 | 1.9 | 610 | 1.4 |
| All drugs except vit/minerals | 3900 | 49.8 | 4513 | 44.1 | 43,300 | 46.3 | 16,800 | 38.3 |
| D and X category | 471 | 6.0 | 611 | 6.0 | 4210 | 4.5 | 2097 | 4.8 |
| Women with Miscarriages N = 7827 | Women w/o Miscarriages N = 93,480 | HR (95% CI) ϕ | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Age | |||||
| <30 years | 1731 | 22.1 | 29,051 | 31.1 | 1 (-) |
| 30–34 years | 2685 | 34.3 | 36,744 | 39.3 | 1.21 (1.14–1.28) |
| 35–39 years | 2462 | 31.5 | 23,072 | 24.7 | 1.76 (1.65–1.87) |
| >40 years | 949 | 12.1 | 4613 | 4.9 | 3.34 (3.08–3.62) |
| GP Visits | |||||
| 0–1 | 1388 | 17.7 | 20,438 | 21.9 | 1 (-) |
| 2–4 | 2312 | 29.5 | 27,627 | 29.6 | 1.23 (1.15–1.31) |
| 5–9 | 2478 | 31.7 | 28,620 | 30.6 | 1.27 (1.19–1.36) |
| >10 | 1649 | 21.1 | 16,795 | 18.0 | 1.45 (1.35–1.56) |
| Smoking | 683 | 8.7 | 7160 | 7.7 | 1.07 (0.91–1.25) |
| Anxiety | 1472 | 18.8 | 16,132 | 17.3 | 1.06 (1.00–1.12) |
| Cardiopathy | 5 | 0.1 | 15 | 0.0 | 3.58 (1.49–8.60) |
| Depression | 745 | 9.5 | 7271 | 7.8 | 1.12 (1.04–1.21 |
| Epilepsy | 48 | 0.6 | 549 | 0.6 | 1.00 (0.75–1.33) |
| Hypertension | 123 | 1.6 | 951 | 1.0 | 1.19 (1.00–1.43) |
| Hypothyroidism | 612 | 7.8 | 6057 | 6.5 | 1.09 (1.00–1.18) |
| Irritable Bowel Syndrome | 160 | 2.0 | 1719 | 1.8 | 1.04 (0.89–1.22) |
| Migraine | 534 | 6.8 | 5770 | 6.2 | 1.08 (0.99–1.18) |
| Metabolic conditions * | 1092 | 14.0 | 11,557 | 12.4 | 1.05 (0.98–1.11) |
| Psychiatric conditions φ | 110 | 1.4 | 1031 | 1.1 | 0.90 (0.74–1.09) |
| Antibiotics | 947 | 12.1 | 10,746 | 11.5 | 0.99 (0.92–1.06) |
| Acid Suppressants | 406 | 5.2 | 4397 | 4.7 | 0.99 (0.89–1.10) |
| Benzodiazepines | 416 | 5.3 | 3880 | 4.2 | 1.13 (1.02–1.25) |
| Antihypertensives | 89 | 1.1 | 518 | 0.6 | 1.49 (1.21–1.84) |
| ARBs | 30 | 0.4 | 204 | 0.2 | 1.21 (0.85–1.74) |
| ACEI | 9 | 0.1 | 50 | 0.1 | 1.37 (0.71–2.64) |
| Calcium channel blockers | 11 | 0.1 | 53 | 0.1 | 1.78 (0.99–3.22) |
| B-Blocking agents | 40 | 0.5 | 181 | 0.2 | 2.07 (1.52–2.83) |
| Diuretics | 19 | 0.2 | 96 | 0.1 | 1.59 (1.01–2.49) |
| SSRI | 179 | 2.3 | 1597 | 1.7 | 1.15 (0.99–1.34) |
| Antimigraine drugs | 66 | 0.8 | 604 | 0.6 | 1.17 (0.92–1.49) |
| Folic Acid | 744 | 9.5 | 8302 | 8.9 | 1.02 (0.94–1.10) |
| Antiepileptics | 55 | 0.7 | 576 | 0.6 | 1.02 (0.79–1.22) |
| Thyroid Hormones | 212 | 2.7 | 1798 | 1.9 | 1.15 (1.01–1.33) |
| D X category | 471 | 6.0 | 4210 | 4.5 | 1.17 (1.07–1.29) |
| All drugs (exc vit and min) | 3900 | 49.8 | 43,302 | 46.3 | 1.03 (0.98–1.08) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez Ortiz, S.; Huerta, C.; Llorente-García, A.; Ortega, P.; Astasio, P.; Cea-Soriano, L. A Validation Study on the Frequency and Natural History of Miscarriages Using the Spanish Primary Care Database BIFAP. Healthcare 2021, 9, 596. https://doi.org/10.3390/healthcare9050596
Sanchez Ortiz S, Huerta C, Llorente-García A, Ortega P, Astasio P, Cea-Soriano L. A Validation Study on the Frequency and Natural History of Miscarriages Using the Spanish Primary Care Database BIFAP. Healthcare. 2021; 9(5):596. https://doi.org/10.3390/healthcare9050596
Chicago/Turabian StyleSanchez Ortiz, Sara, Consuelo Huerta, Ana Llorente-García, Paloma Ortega, Paloma Astasio, and Lucía Cea-Soriano. 2021. "A Validation Study on the Frequency and Natural History of Miscarriages Using the Spanish Primary Care Database BIFAP" Healthcare 9, no. 5: 596. https://doi.org/10.3390/healthcare9050596