
The Reciprocal Relationship between Frailty and Depressive Symptoms among Older Adults in Rural China: A Cross-Lag Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Assessment of Frailty
2.3. Assessment of Depressive Symptoms
2.4. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics of Participants in Baseline
3.2. Correlations between Depressive Symptoms and Frailty
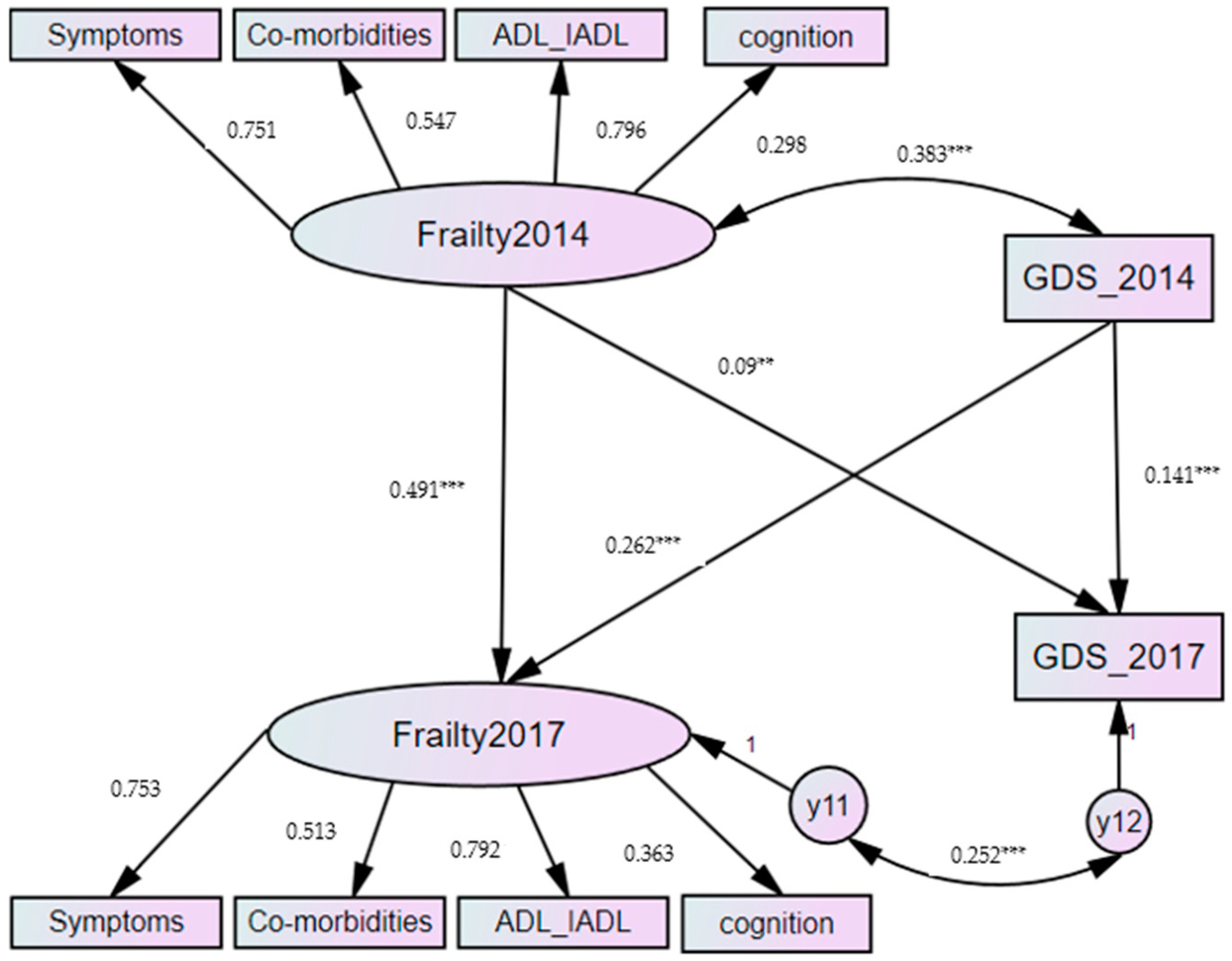
3.3. Two-Wave Cross-Lagged Panel Model
3.4. Gender Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choi, J.; Ahn, A.; Kim, S.; Won, C.W. Global Prevalence of Physical Frailty by Fried’s Criteria in Community-Dwelling Elderly With National Population-Based Surveys. J. Am. Med. Dir. Assoc. 2015, 16, 548–550. [Google Scholar] [CrossRef] [PubMed]
- Hasin, D.S.; Goodwin, R.D.; Stinson, F.S.; Grant, B.F. Epidemiology of Major Depressive Disorder: Results From the National Epidemiologic Survey on Alcoholism and Related Conditions. Arch. Gen. Psychiatry 2005, 10, 1097. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Cawthon, P.M.; Stone, K.L.; Hillier, T.A.; Cauley, J.A.; Hochberg, M.C.; Rodondi, N.; et al. Comparison of 2 Frailty Indexes for Prediction of Falls, Disability, Fractures, and Death in Older Women. Arch. Intern. Med. 2008, 168, 382–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeulen, J.; Neyens, J.C.L.; Van Rossum, E.; Spreeuwenberg, M.D.; De Witte, L.P. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: A systematic review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Hare, D.L.; Toukhsati, S.R.; Johansson, P.; Jaarsma, T. Depression and cardiovascular disease: A clinical review. Eur. Heart J. 2014, 35, 1365–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodda, J.; Walker, Z.; Carter, J. Depression in older adults. BMJ 2011, 343, d5219. [Google Scholar] [CrossRef]
- Buigues, C.; Padilla-Sánchez, C.; Garrido, J.F.; Navarro-Martínez, R.; Ruiz-Ros, V.; Cauli, O. The relationship between depression and frailty syndrome: A systematic review. Aging Ment. Health. 2014, 19, 762–772. [Google Scholar] [CrossRef]
- Vaughan, L.; Corbin, A.L.; Goveas, J.S. Depression and frailty in later life: A systematic review. Clin. Interv. Aging. 2015, 10, 1947. [Google Scholar] [CrossRef] [Green Version]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.-T.; et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Jürschik, P.; Nunin, C.; Botigué, T.; Escobar, M.A.; Lavedán, A.; Viladrosa, M. Prevalence of frailty and factors associated with frailty in the elderly population of Lleida, Spain: The FRALLE survey. Arch. Gerontol. Geriatr. 2012, 55, 625–631. [Google Scholar] [CrossRef]
- Feng, L.; Nyunt, M.S.; Feng, L.; Yap, K.B.; Ng, T.P. Frailty predicts new and persistent depressive symptoms among community-dwelling older adults: Findings from Singapore longitudinal aging study. J. Am. Med. Dir. Assoc. 2014, 15, 76-e7. [Google Scholar] [CrossRef] [PubMed]
- Arts, M.H.; Collard, R.M.; Comijs, H.C.; Zuidersma, M.; de Rooij, S.E.; Naarding, P.; Voshaar, R.C. Physical frailty and cognitive functioning in depressed older adults: Findings from the NESDO study. J. Am. Med. Dir. Assoc. 2016, 17, 36–43. [Google Scholar] [CrossRef]
- De Albuquerque Sousa, A.C.; Dias, R.C.; Maciel, Á.C.; Guerra, R.O. Frailty syndrome and associated factors in community-dwelling elderly in Northeast Brazil. Arch. Gerontol. Geriatr. 2012, 54, e95–e101. [Google Scholar] [CrossRef] [PubMed]
- Pegorari, M.S.; Tavares, D.M. Factors associated with the frailty syndrome in elderly individuals living in the urban area. Rev. Lat. Am. Enferm. 2014, 22, 874–882. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.W.; Jang, I.Y.; Lee, Y.S.; Lee, C.K.; Cho, E.I.; Kang, W.Y.; Chae, J.H.; Lee, E.J.; Kim, D.H. Prevalence of frailty and aging-related health conditions in older Koreans in rural communities: A cross-sectional analysis of the aging study of Pyeongchang rural area. J. Korean Med. Sci. 2016, 31, 345. [Google Scholar] [CrossRef]
- Katz, I.R. Depression and frailty: The need for multidisciplinary research. Am. J. Geriatr. Psychiatry 2004, 12, 1–5. [Google Scholar] [CrossRef]
- Rui, M.D.; Veronese, N.; Trevisan, C.; Carraro, S.; Sergi, G. Changes in frailty status and risk of depression: Results from the pro.v.a. longitudinal study. Am. J. Geriatr. Psychiatry 2016, 25, 190–197. [Google Scholar] [CrossRef]
- Veronese, N.; Solmi, M.; Maggi, S.; Noale, M.; Sergi, G.; Manzato, E.; Prina, A.M.; Fornaro, M.; Carvalho, A.F.; Stubbs, B. Frailty and incident depression in community—dwelling older people: Results from the ELSA study. Int. J. Geriatr. Psychiatry 2017, 32, e141–e149. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.J.; Rutherford, B.R.; Yaffe, K.; Tandler, J.M.; Ray, J.L.; Pott, E.; Chung, S.; Roose, S.P. The depressed frail phenotype: The clinical manifestation of increased biological aging—sciencedirect. Am. J. Geriatr. Psychiatry 2016, 24, 1084–1094. [Google Scholar] [CrossRef] [Green Version]
- Silverstein, B.; Edwards, T.; Gamma, A.; Ajdacic-Gross, V.; Rossler, W.; Angst, J. The role played by depression associated with somatic symptomatology in accounting for the gender difference in the prevalence of depression. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 48, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Smit, E.; Xue, Q.-L.; Odden, M.C. Prevalence and Correlates of Frailty Among Community-Dwelling Chinese Older Adults: The China Health and Retirement Longitudinal Study. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2018, 73, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Wang, Y.; Zhang, Y.; Chu, X.; Wang, Z.; Qian, D.; Chen, F.; Xu, J.; Li, S.; Jin, L.; et al. Cohort profile: The Rugao Longevity and Ageing Study (RuLAS). Int. J. Epidemiol. 2015, 45, 1064–1073. [Google Scholar] [CrossRef] [Green Version]
- Rockwood, K.; Mitnitski, A. Frailty in Relation to the Accumulation of Deficits. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Wang, Q.; Zhi, T.; Zhu, Y.; Wang, Y.; Wang, Z.; Shi, J.; Xie, X.; Chu, X.; Wang, X.; et al. Frailty index and its relation to falls and overnight hospitalizations in elderly Chinese people: A population-based study. J. Nutr. Heal. Aging 2016, 20, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric depression scale (GDS) recent evidence and development of a shorter version. Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Rogosa, D. A critique of cross-lagged correlation. Psychol. Bull. 1980, 88, 245. [Google Scholar] [CrossRef]
- Hamaker, E.L.; Kuiper, R.M.; Grasman, R.P. A critique of the cross-lagged panel model. Psychol. Methods 2015, 20, 102. [Google Scholar] [CrossRef]
- Collard, R.M.; Comijs, H.C.; Naarding, P.; Penninx, B.W.; Milaneschi, Y.; Ferrucci, L.; Voshaar, R.C. Frailty as a predictor of the incidence and course of depressed mood. J. Am. Med Dir. Assoc. 2015, 16, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Paulson, D.; Lichtenberg, P.A. Vascular depression: An early warning sign of frailty. Aging Ment. Health. 2013, 17, 85–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann, R.; Schmidt, F.M.; Sander, C.; Hegerl, U. Heart Rate Variability as Indicator of Clinical State in Depression. Front. Psychiatry 2019, 9, 735. [Google Scholar] [CrossRef] [Green Version]
- Ottenbacher, K.J.; Graham, J.E.; Al Snih, S.; Raji, M.; Samper-Ternent, R.; Ostir, G.V.; Markides, K.S. Mexican Americans and frailty: Findings from the Hispanic established populations epidemiologic studies of the elderly. Am. J. Public Health. 2009, 99, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Westbury, L.; Cooper, C. Social isolation and loneliness as risk factors for the progression of frailty: The English Longitudinal Study of Ageing. Age Ageing 2018, 47, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohman, M.; Dumenci, L.; Mezuk, B. Sex Differences in the Construct Overlap of Frailty and Depression: Evidence from the Health and Retirement Study. J. Am. Geriatr. Soc. 2014, 62, 500–505. [Google Scholar] [CrossRef] [Green Version]
- González, G.; Vives, A. Work Status, Financial Stress, Family Problems, and Gender Differences in the Prevalence of Depression in Chile. Ann. Work. Expo. Health 2019, 63, 359–370. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N (%) | Mean (SD) | |
|---|---|---|
| Age | 75.1 (3.802) | |
| 70–74 | 695 (50.5) | |
| 75–79 | 466(33.9) | |
| 80–84 | 215 (15.6) | |
| Gender | ||
| Male | 622 (45.2) | |
| Female | 754 (54.8) | |
| Marital status at baseline | ||
| Currently Married | 930 (68.2) | |
| Others | 434 (31.8) | |
| Educational level at baseline | ||
| Illiterate | 735 (54.4) | |
| Literate | 617 (45.6) | |
| Occupation | ||
| Farmer | 1225 (90.4) | |
| Others | 130 (9.6) | |
| Frailty Index | ||
| ≤0.1 | 193 (14.0) | |
| 0.1–0.21 | 716 (52.0) | |
| >0.21 | 467 (33.9) |
| Indicators | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Depression 2014 | 2.46 | 2.278 | 1.000 | |||||||||
| 2. Symptoms 2014 | 4.102 | 1.773 | 0.344 *** | 1.000 | ||||||||
| 3. Co-morbidities 2014 | 1.340 | 1.097 | 0.148 *** | 0.277 *** | 1.000 | |||||||
| 4. ADL_IADL 2014 | 1.506 | 2.106 | 0.309 *** | 0.331 *** | 0.205 *** | 1.000 | ||||||
| 5. Cognitive function 2014 | 0.50 | 0.247 | 0.575 *** | 0.177 *** | 0.114 *** | 0.174 *** | 1.000 | |||||
| 6 Depression 2017 | 2.00 | 2.302 | 0.141 *** | 0.084 *** | 0.057 * | 0.059 * | 0.086 ** | 1.000 | ||||
| 7. Symptoms 2017 | 3.902 | 1.703 | 0.256 *** | 0.390 *** | 0.166 *** | 0.223 *** | 0.150 *** | 0.315 *** | 1.000 | |||
| 8. Co-morbidities 2017 | 1.344 | 1.125 | 0.163 *** | 0.219 *** | 0.423 *** | 0.126 *** | 0.108 *** | 0.123 *** | 0.318 *** | 1.000 | ||
| 9. ADL_IADL 2017 | 1.690 | 2.104 | 0.161 *** | 0.211 *** | 0.105 *** | 0.433 *** | 0.054 | 0.196 *** | 0.318 *** | 0.151 *** | 1.000 | |
| 10. Cognitive function 2017 | 0.54 | 0.251 | 0.135 *** | 0.129 *** | 0.049 | 0.035 | 0.094 *** | 0.392 *** | 0.287 *** | 0.118 | 0.204 *** | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Shen, K. The Reciprocal Relationship between Frailty and Depressive Symptoms among Older Adults in Rural China: A Cross-Lag Analysis. Healthcare 2021, 9, 593. https://doi.org/10.3390/healthcare9050593
Wang X, Shen K. The Reciprocal Relationship between Frailty and Depressive Symptoms among Older Adults in Rural China: A Cross-Lag Analysis. Healthcare. 2021; 9(5):593. https://doi.org/10.3390/healthcare9050593
Chicago/Turabian StyleWang, Xuehui, and Kaijun Shen. 2021. "The Reciprocal Relationship between Frailty and Depressive Symptoms among Older Adults in Rural China: A Cross-Lag Analysis" Healthcare 9, no. 5: 593. https://doi.org/10.3390/healthcare9050593