
Integrating Quality Tools and Methods to Analyze and Improve a Hospital Sterilization Process



Abstract
:1. Introduction
1.1. Research Motivation
1.2. Literature Overview
1.2.1. Failure Mode and Effects Analysis (FMEA)
1.2.2. Structured Analysis and Design Technique (SADT)
1.2.3. Quality Function Deployment (QFD)
1.3. Objective and Contributions of the Study
2. Materials and Methods
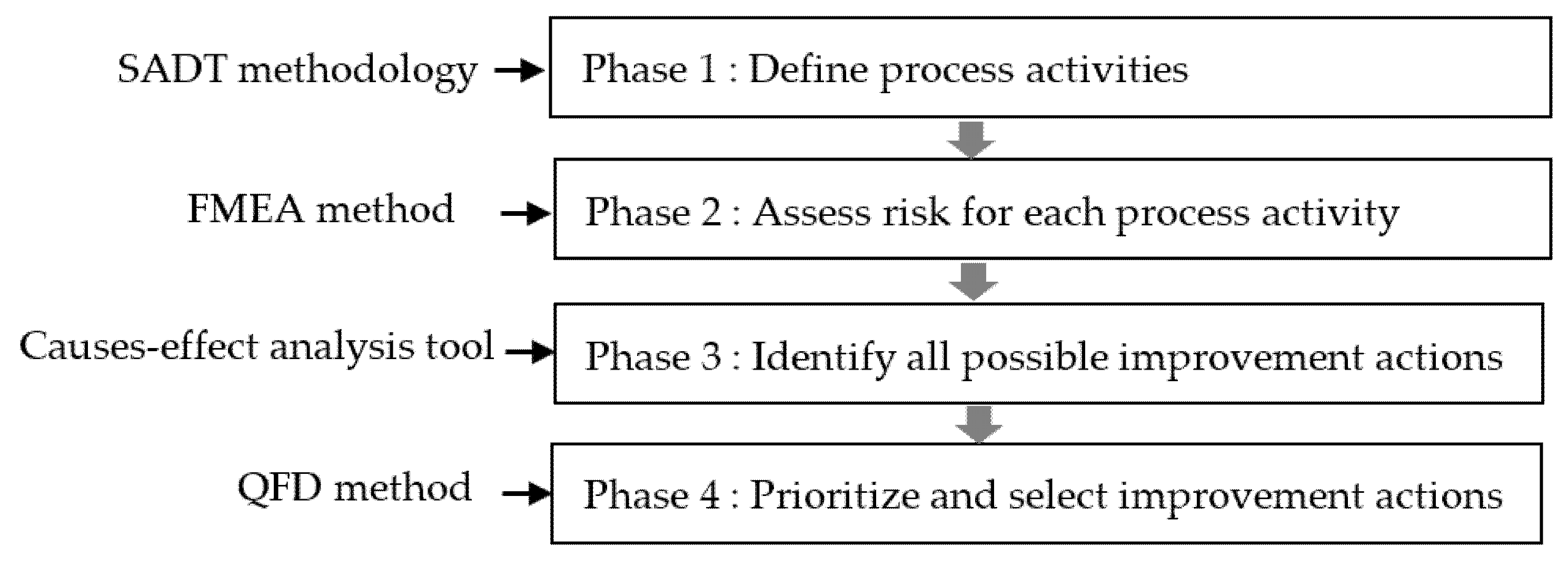
2.1. The Proposed Approach
2.2. The Case Study
3. Results
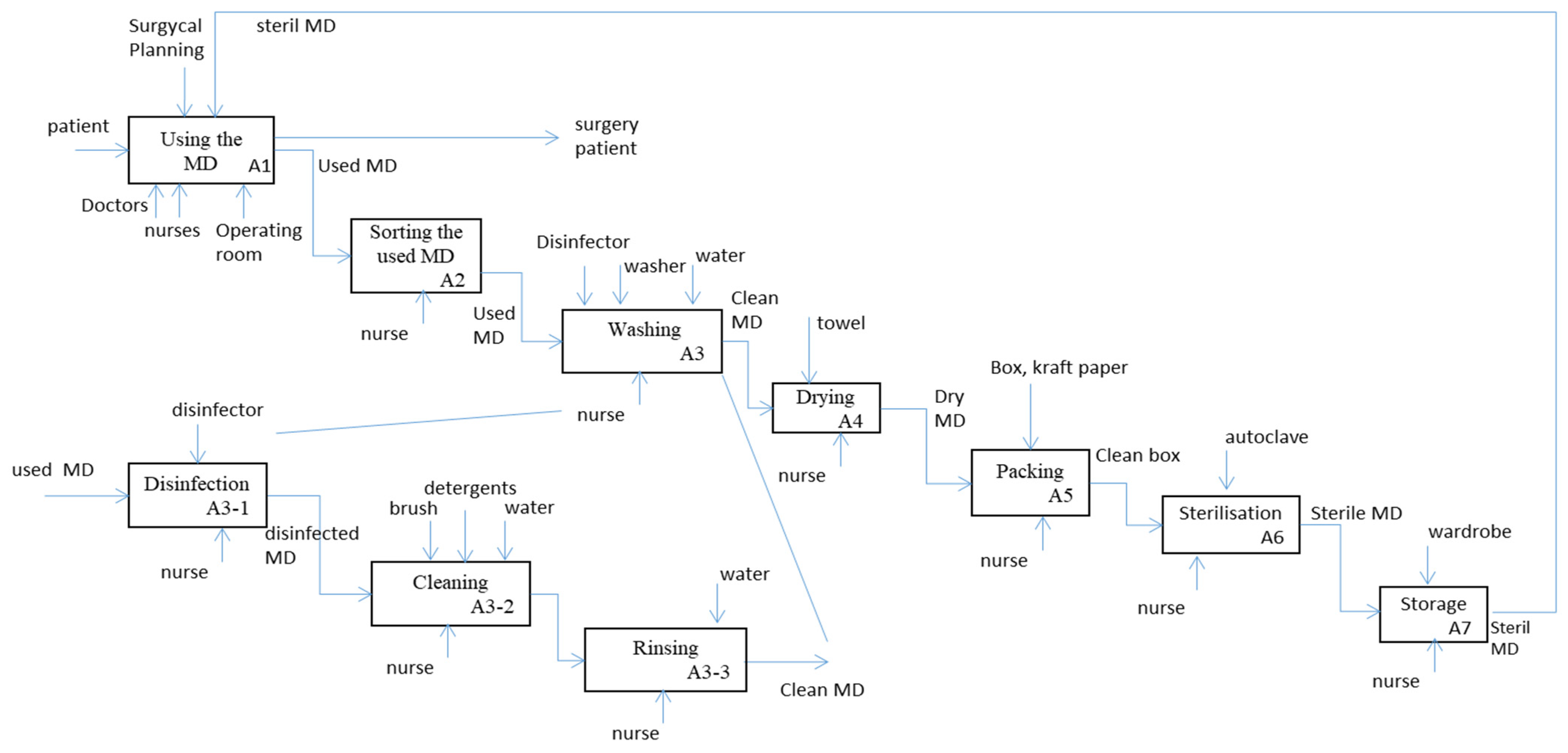
3.1. Phase 1: Define Process Activities
3.2. Phase 2: Assess Risk for Each Process Activity
3.3. Phase 3: Identify All Possible Improvement Actions
3.4. Phase 4: Prioritize the Design Requirements and Improvement Actions
- Identify the customer requirements (what) that represent the sterilization process steps. The sterilization process design was identified through direct observation and interviews with nurses and instrumentalists of the surgical blocks. Items were entered into the house of quality (HOQ) as a voice of the customer (VOC) inputs.
- Prioritize the CRs using the FMEA rating and a number that reflects the importance of the demand using a one-to-five scale. For sterilization and disinfection activities, which were ranked 1 and 2, respectively, according to FMEA, a weight of 5 was attributed to these activities. For the transport, storage, and RMD sorting activities, the attributed weight was based on the fact that their FMEA ranking ranged between 3 and 5. Finally, the washing and packing activities, which had the lowest FMEA ranking, were attributed a weight of 3. Each activity weight is indicated in the third column of Table 4.
- Determine the categories requiring improvement using indicators that represent the DRs using surveys and exploratory factor analysis. A questionnaire survey was administered to determine the categories requiring improvement based on nurses’ and normative requirements (good pharmaceutical practice).
- To apply the QFD method, the customer should define a relative importance (Wi) of each customer’s requirements (CRi). In our case study, the Wi was defined by healthcare managers for each HSP activity based on the good pharmaceutical practice of the HSP (technical importance), and the risk priority of each HSP activity was defined by the FMEAC analysis. The Wi constitutes the link between FMEA and the QFD method. The RPN calculated by the FMEA for each activity of the process guide and help the decision maker to determine the Wi of each CRi.
- Determine the what–how relationships, which represent the degree to which CRi is met by DRj. These relationships can be evaluated according to a rating scale. In the literature related to QFD [49], many methods and a set of rating scales to facilitate gathering and displaying information are available. A three-point ordinal scale (weak, medium, and strong) can be used to establish relationships between DRj and CRi. This scale considers a further point: the absence of relationship. Ratings obtained with this scale are usually scalarized with numerical series 0, 1, 3, and 9 or 0, 1, 3, and 5 [56]. There is no competition between the rating scales, but the use of one provides an evaluation of the relationships to classify them and then to detect the avenues of HSP improvement. In this study, a 0, 1, 3, 9 rating scale was used. The interrelations are typically defined as strong (9), moderate (3), weak (1), and none (0). In other words, for each activity i, each DRij is estimated using four possibilities: 9, 3, 1, or 0.
- Calculate the individual DRj indices for each DR using Equation (2). The values are shown in the last row of Table 5. For example, using Equation (2), the DR index of the equipment was equal to 4 × 3 + 5 × 0 + 3 × 3 + … 4 × 9 = 165.
- Classify the DRj according to its index value. Derived from the results of the QFD matrix (Table 4), the most important DR for the improvement in the HSP was the management action category, which had an index value of 222. Using the details of the Management category in Table 5, we concluded that the coordination between sterilization service and the block, the average duration of the sterilization process, and the availability of sterile RMDs at a time were the most important factors for improving the current HSP. The second and third most important DRs were personnel category (value of 204) and method category (value of 192). The equipment category (value of 165) was ranked as the fourth important improvement action. Verified by the hospital management, the results were regarded as practical and informative.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CEA | Cause and Effect Analysis |
| CR | Customer Requirement |
| CRi | Customer Requirement of activity i |
| QFD | Quality Function Deployment |
| D | Detection |
| DR | Design Requirement |
| DRij | Score of Design Requirement j for activity i |
| FMEA | Failure Modes and Effects Analysis |
| HOQ | House of Quality |
| HSP | Hospital Sterilization Process |
| ICAM | Integrated Computer-Aided Manufacturing |
| IDEF0 | ICAM Definition for Function Modeling |
| RPN | Risk Priority Number |
| O | Occurrence |
| RMD | Reusable Medical Devices |
| S | Severity |
| SADT | Structured Analysis and Design Technique |
| TQM | Total Quality Management |
| VOC | Voice of the Customer |
| Wi | Importance Weight of Activity i |
References
- Zhang, L.; Liu, R.; Jiang, S.; Luo, G.; Liu, H.-C. Identification of Key Performance Indicators for Hospital Management Using an Extended Hesitant Linguistic DEMATEL Approach. Healthcare 2020, 8, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrouzi, F.; Ma’aram, A. Identification and ranking of specific balanced scorecard performance measures for hospitals: A case study of private hospitals in the Klang Valley area, Malaysia. Int. J. Health Plan. Manag. 2019, 34, 1364–1376. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, B.; Rowan, N. Terminal sterilization of medical devices using vaporized hydrogen peroxide: A review of current methods and emerging opportunities. J. Appl. Microbiol. 2019, 127, 1403–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Klundert, J.; Muls, P.; Schadd, M. Optimizing sterilization logistics in hospitals. Health Care Manag. Sci. 2008, 11, 23–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlgaard, J.J.; Pettersen, J.; Dahlgaard-Park, S.M. Quality and lean health care: A system for assessing and improving the health of healthcare organisations. Total Qual. Manag. Bus. Excell. 2011, 22, 673–689. [Google Scholar] [CrossRef]
- Øvretveit, J. Total quality management in European healthcare. Int. J. Health Care Qual. Assur. 2000, 13, 74–80. [Google Scholar] [CrossRef]
- Komashie, A.; Mousavi, A.; Gore, J. Quality management in healthcare and industry: A comparative review and emerging themes. J. Manag. Hist. 2007, 13, 359–370. [Google Scholar] [CrossRef]
- Rutala, W.A.; Gergen, M.F.; Weber, D.J. Comparative evaluation of the sporicidal activity of new low-temperature sterilization technologies: Ethylene oxide, 2 plasma sterilization systems, and liquid peracetic acid. Am. J. Infect. Control 1998, 26, 393–398. [Google Scholar] [CrossRef]
- Rutala, W.; Gergen, M.; Weber, D. Impact of an Oil-Based Lubricant on the Effectiveness of the Sterilization Processes. Infect. Control Hosp. Epidemiol. 2008, 29, 69–72. [Google Scholar] [CrossRef]
- Nilsen, E.V. Managing Equipment and Instrument in the Operating Room. AORN J. 2005, 81, 349–358. [Google Scholar] [CrossRef]
- Ahmadi, E.; Masel, D.T.; Metcalf, A.Y.; Schuller, K. Inventory management of surgical supplies and sterile instruments in hospitals: A literature review. Health Syst. (Basingstoke) 2018, 8, 134–151. [Google Scholar] [CrossRef] [PubMed]
- Fineman, S.J.; Kapadia, A.S. An analysis of the logistics of supplying and processing sterilized items in hospitals. Comput. Oper. Res. 1978, 5, 47–54. [Google Scholar] [CrossRef]
- Johnson, D. A roadmap to optimizing sterile processing workflow. Health Care Purch. News 2005, 29, 30–34. [Google Scholar]
- Johnson, D. Achieving LEAN sterile Processing. Health Care Purch. News 2011, 35, 46–50. [Google Scholar]
- Reymondon, F.; Pellet, B.; Marcon, E. Optimization of hospital sterilization costs proposing new grouping choices of medical devices into packages. Int. J. Prod. Econ. 2008, 112, 326–335. [Google Scholar] [CrossRef]
- Ozturk, O.; Begen, M.A.; Zaric, G.S. A branch and bound based heuristic for makespan minimization of washing operations in hospital sterilization services. Eur. J. Oper. Res. 2014, 239, 214–226. [Google Scholar] [CrossRef]
- Di Mascolo, M.; Gouin, A. A generic simulation model to assess the performance of sterilization services in health establishments. Health Care Manag. Sci. 2013, 16, 45–61. [Google Scholar] [CrossRef]
- Hachicha, W.; Benaissa, M.; Almalki, H.; Kammoum, A. A Simulation Study to organize a Hospital Sterilization-Process of Maternity-Service. Int. J. Eng. Res. Technol. 2019, 8, 140–146. [Google Scholar]
- Weinstein, R.A.; Linkin, D.R.; Sausman, C.; Santos, L.; Lyons, C.; Fox, C.; Aumiller, L.; Esterhai, J.; Pittman, B.; Lautenbach, E. Applicability of Healthcare Failure Mode and Effects Analysis to Healthcare Epidemiology: Evaluation of the Sterilization and Use of Surgical Instruments. Clin. Infect. Dis. 2005, 41, 1014–1019. [Google Scholar] [CrossRef] [Green Version]
- Figliatto, F.S.; Anzanello, M.J.; Tonetto, L.M.; Shneider, D.S.S.; Magalhaes, M.; Maria, A. Lean-healthcare approach to reduce costs in a sterilization plant based on surgical tray rationalization. Prod. Plan. Control 2020, 31, 483–495. [Google Scholar] [CrossRef]
- Harikumar, P.; Saleeshya, P.G. Integrating FMEA, QFD and Lean for Risk management in hospitals. IOP Conf. Ser. Mater. Sci. Eng. 2019, 577, 012040. [Google Scholar] [CrossRef] [Green Version]
- Altuntas, S.; Kansu, S. An innovative and integrated approach based on SERVQUAL, QFD and FMEA for service quality improvement: A case study. Kybernetes 2019, 49, 2419–2453. [Google Scholar] [CrossRef]
- Pourmadadkar, M.; Beheshtinia, M.A.; Ghods, K. An integrated approach for healthcare services risk assessment and quality enhancement. Int. J. Qual. Reliab. Manag. 2019, 37, 1183–1208. [Google Scholar] [CrossRef]
- Carnut, L.; Narvai, P.C.A. Meta-summarization of Qualitative Findings about Health Systems Performance Evaluation Models: Conceptual Problems and Comparability Limitations. Inq. J. Health Care Organ. Provis. Financ. 2020, 57, 1–19. [Google Scholar] [CrossRef]
- Nicolaou, N.; Kentas, G. Total Quality Management Implementation Failure Reasons in Healthcare Sector. J. Health Sci. 2017, 5, 110–113. [Google Scholar] [CrossRef] [Green Version]
- Alfalah, T.F. Total Quality Management Tools: Are they Necessary for Improving Service Quality and Customer Satisfaction? Int. Rev. Manag. Mark. 2017, 7, 121–125. [Google Scholar]
- Ashley, L.; Armitage, G.; Neary, M.; Hollingsworth, G. A practical guide to failure mode and effects analysis in health care: Making the most of the team and its meetings. Jt. Comm. J. Qual. Patient Saf. 2008, 36, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Serrou, D.; Abouabdellah, A.; Mharzi, H. Proposed an approach for measuring the performance of hospital logistics systems by integrating quality, safety and environment. Int. J. Sci. Eng. Technol. 2015, 4, 24–27. [Google Scholar]
- Meyrieux, C.; Garcia, R.; Pourel, N.; Mège, A.; Bodez, V. Analyse des risques a priori du processus de prise en charge des patients en radiothérapie: Exemple d’utilisation de la méthode AMDEC. Cancer/Radiothérapie 2012, 16, 613–618. [Google Scholar] [CrossRef]
- Cagliano, A.C.; Grimaldi, S.; Rafele, C.A. systemic methodology for risk management in healthcare sector. Saf. Sci. 2011, 49, 695–708. [Google Scholar] [CrossRef] [Green Version]
- Crane, J.; Crane, F.G. Preventing medication errors in hospitals through a systems approach and technological innovation: A prescription for 2010. Hosp. Top. 2006, 84, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, N.; Mondal, S. Development of a predictive maintenance model using modified FMEA approach. IUP J. Oper. Manag. 2014, 13, 7–16. [Google Scholar]
- Abbasgholizadeh Rahimi, S.; Jamshidi, A.; Ait-Kadi, D.; Ruiz, A. Using fuzzy cost-based FMEA, GRA and profitability theory for minimizing failures at a healthcare diagnosis service. Qual. Reliab. Eng. Int. 2015, 31, 601–615. [Google Scholar] [CrossRef]
- Yousefinezhadi, T.; Nobari, F.A.J.; Goodari, F.B.; Arab, M. A case study on improving intensive care unit (ICU) services reliability: By using process failure mode and effects analysis (PFMEA). Glob. J. Health Sci. 2016, 8, 207. [Google Scholar] [CrossRef]
- Day, S.; Dalto, J.; Fox, J.; Allen, A.; Ilstrup, S. Utilization of failure mode effects analysis in trauma patient registration. Qual. Manag. Healthc. 2007, 16, 342–348. [Google Scholar] [CrossRef]
- Capunzo, M.; Cavallo, P.; Boccia, G.; Brunetti, L.; Pizzuti, S. A FMEA clinical laboratory case study: How to make problems and improvements measurable. Clin. Leadersh. Manag. Rev. 2004, 18, 37–41. [Google Scholar] [PubMed]
- Chiozza, M.L.; Ponzetti, C. FMEA: A model for reducing medical errors. Clin. Chim. Acta 2009, 404, 75–78. [Google Scholar] [CrossRef]
- Najafpour, Z.; Hasoumi, M.; Behzadi, F.; Mohamadi, E.; Jafary, M.; Saeedi, M. Preventing blood transfusion failures: FMEA, an effective assessment method. BMC Health Serv. Res. 2017, 17, 453. [Google Scholar] [CrossRef] [Green Version]
- Malfará, M.; Pernassi, M.; Aragon, D.; Carlotti, A. Impact of the clinical pharmacist interventions on prevention of pharmacotherapy related problems in the paediatric intensive care unit. Int. J. Clin. Pharm. 2018, 40, 513–519. [Google Scholar] [CrossRef]
- Mirdamadi, S. Système D’aide à la Décision Pour la Génération des Processus D’inspection par la Fédération des Expertises Métier. Ph.D. Thesis, Arts et Métiers ParisTech, Paris, France, 2014. [Google Scholar]
- Liu, H.C.; Chen, X.Q.; Duan, C.Y.; Wang, Y.M. Failure mode and effect analysis using multi-criteria decision making methods: A systematic literature review. Comput. Ind. Eng. 2019, 135, 881–897. [Google Scholar] [CrossRef]
- Lakhoua, M.N.; Salem, B.; El Amraoui, L. Augmenting SADT with Respect to Timing Constraints, Formalization and Dependability Evaluation. Int. J. Sci. Eng. Res. 2016, 7, 446–451. [Google Scholar]
- Mutic, S.; Brame, R.S.; Oddiraju, S.; Michalski, J.M.; Wu, B. System mapping of complex healthcare processes using IDEF0: A radiotherapy example. Int. J. Collab. Enterp. 2010, 1, 316–331. [Google Scholar] [CrossRef]
- Funk, K.H., II; Bauer, J.D.; Doolen, T.L.; Telasha, D.; Nicolalde, R.J.; Reeber, M.; Long, M. Use of modeling to identify vulnerabilities to human error in laparoscopy. J. Minim. Invasive Gynecol. 2010, 17, 311–320. [Google Scholar] [CrossRef]
- Abo-Hamad, W.; Arisha, A. Simulation-based framework to improve patient experience in an emergency department. Eur. J. Oper. Res. 2013, 224, 154–166. [Google Scholar] [CrossRef] [Green Version]
- Bevilacqua, M.; Mazzuto, G.; Paciarotti, C. A combined IDEF0 and FMEA approach to healthcare management reengineering. Int. J. Procure. Manag. 2015, 8, 25–43. [Google Scholar] [CrossRef]
- Rihar, L.; Kušar, J. Implementing Concurrent Engineering and QFD Method to Achieve Realization of Sustainable Project. Sustainability 2021, 13, 1091. [Google Scholar] [CrossRef]
- Tanık, M. Improving “order handling” process by using QFD and FMEA methodologies: A case study. Int. J. Qual. Reliab. Manag. 2010, 27, 404–423. [Google Scholar] [CrossRef]
- Gremyr, I.; Raharjo, H. Quality function deployment in healthcare: A literature review and case study. Int. J. Health Care Qual. Assur. 2013, 26, 135–146. [Google Scholar] [CrossRef]
- Carnevalli, J.A.; Miguel, P.C. Review, analysis and classification of the literature on QFD—Types of research, difficulties and benefits. Int. J. Prod. Econ. 2008, 114, 737–754. [Google Scholar] [CrossRef]
- Said, M.; Yunus, R.; Palutturi, S. Increasing Inpatient Service Quality of Using Quality Function Deployment Method in Nene Mallomo Hospital of Sidrap Regency, Indonesia. Indian J. Public Health Res. Dev. 2018, 9, 287–291. [Google Scholar]
- Debata, B.R.; Patnaik, B.; Mahapatra, S.S.; Sreekumar. An integrated approach for service quality improvement in medical tourism: An Indian perspective. Int. J. Serv. Oper. Manag. 2012, 13, 119–145. [Google Scholar] [CrossRef]
- Stamatis, D.H. Essentials for the Improvement of Healthcare Using Lean & Six Sigma; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Dai, W.; Maropoulos, P.G.; Cheung, W.M.; Tang, X. Decision-making in product quality based on failure knowledge. Int. J. Prod. Lifecycle Manag. 2011, 5, 143–163. [Google Scholar] [CrossRef]
- Chan, L.K.; Wu, M.L. Quality function deployment: A literature review. Eur. J. Oper. Res. 2002, 143, 463–497. [Google Scholar] [CrossRef]
- Franceschini, F.; Rupil, A. Rating scales and prioritization in QFD. Int. J. Qual. Reliab. Manag. 1999, 16, 85–97. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Value | Occurrence (O) | Severity (S) | Detectability (D) |
|---|---|---|---|
| 1 | Less than once a year | No harm, no increased | Observable |
| 2 | Less than once a month | Non-permanent minor harm or increased length of stay | Effective detection |
| 3 | Less than once a week | Non-permanent major harm or permanent minor harm | Low detection |
| 4 | Less than once a day | Permanent major harm | Rare detection |
| 5 | Once a day or more | Death | Cannot detect |
| Occurrence/Severity | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 5 | 5 Un-wanted | 10 Un-wanted | 15 Un-acceptable | 20 Un-acceptable | 25 Un-acceptable |
| 4 | 4 Acceptable | 8 Un-wanted | 12 Un-wanted | 16 Un-acceptable | 20 Un-acceptable |
| 3 | 3 Acceptable | 6 Acceptable | 9 Un-wanted | 12 Un-wanted | 15 Un-acceptable |
| 2 | 2 Wanted | 4 Acceptable | 6 Acceptable | 8 Un-wanted | 10 Un-wanted |
| 1 | 1 Wanted | 2 Wanted | 3 Acceptable | 4 Acceptable | 5 Un-wanted |
| Activity | Failure Mode | Effect | Cause | S | O | D | RPN |
|---|---|---|---|---|---|---|---|
| Reception and sorting soiled medical devices | Queue of soiled RMDs | Damage to the RMDs | Nurses are busy | 4 | 4 | 1 | 16 |
| Disinfection | Decontamination time is not respected | Medical dispositive was poorly disinfected | Staff are not trained | 5 | 5 | 1 | 25 |
| Washing | Security measures are not followed | Risk of nurse’s infection | Lack of personnel safety tools | 4 | 4 | 1 | 16 |
| Drying | Lack of a special drying tool | Medical device poorly dried | Using a towel to dry the medical device | 3 | 5 | 1 | 15 |
| Packaging | Queue of packaged, clean medical devices | Late delivery of the RMDs | Insufficient sterilization equipment | 3 | 4 | 1 | 12 |
| Sterilization | Lack of control | Service is badly organized and does not meet pharmaceutical standards | No sterilization activity manager | 5 | 5 | 1 | 25 |
| Heterogeneous load of the autoclave | Some medical devices are poorly sterilized | Lack of awareness and control | 5 | 4 | 1 | 20 | |
| Autoclaves frequently out of order | Disruption of activities and surgical schedule | Equipment amortized and absence of preventive maintenance | 4 | 4 | 1 | 16 | |
| Overload of the autoclave | Boxes are wet and badly sterilized | Lack of autoclave baskets | 5 | 4 | 1 | 20 | |
| Storage | Sterile RMDs poorly stored | Medical device risk due to no longer being sterilized | Absence of adequate storage sites | 4 | 5 | 1 | 20 |
| Transport | Poor transport of the RMDs | Damage to the boxes | Lack of transport trolleys | 5 | 5 | 1 | 25 |
| What: CRi | FMEA Ranking | Wi | How: DRj | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Equipment | Material | Method | Environment | Personnel | Measure | Management | |||
| RMD sorting | 5 | 4 | 3 | 0 | 9 | 0 | 3 | 0 | 9 |
| Disinfection | 2 | 5 | 0 | 9 | 9 | 9 | 9 | 0 | 9 |
| Washing | 6 | 3 | 3 | 3 | 3 | 9 | 9 | 3 | 9 |
| Packing | 7 | 3 | 9 | 0 | 3 | 9 | 9 | 3 | 9 |
| Sterilization | 1 | 5 | 9 | 3 | 9 | 9 | 9 | 9 | 3 |
| Storage | 4 | 4 | 9 | 0 | 3 | 0 | 3 | 3 | 9 |
| Transport | 3 | 4 | 9 | 0 | 9 | 0 | 9 | 9 | |
| DRj index | 165 | 69 | 192 | 144 | 204 | 75 | 222 | ||
| Priority level | 4 | 7 | 3 | 5 | 2 | 6 | 1 | ||
| Category | Items |
|---|---|
| Equipment (Machine) | The quality of the containers of the RMD (Clubs) |
| The tools used for packaging such as bags, etc.) | |
| RMD transport boxes (trucks) | |
| Material | The quality of the disinfector product |
| The quality of water used for washing | |
| The quality of water used for the autoclaves | |
| Method | The condition of the soiled medical devices carriage |
| The condition of the clean medical devices carried to the autoclave | |
| The condition of the sterile medical devices carried to the block | |
| Environment | A location reserved for washing and conditioning |
| A location reserved for sterilization | |
| Personnel (Man) | Staff qualification for the washing activity |
| Staff distribution in the washing and conditioning step | |
| Staff distribution in the sterilization step | |
| Measure | Control of the box type before loading the autoclave |
| Control of the box quantity loaded in the autoclave | |
| Control after the sterilization step | |
| Management | Sterilization service and block coordination |
| Average duration of the sterilization process | |
| The availability of RMDs at a given time |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kammoun, A.; Hachicha, W.; Aljuaid, A.M. Integrating Quality Tools and Methods to Analyze and Improve a Hospital Sterilization Process. Healthcare 2021, 9, 544. https://doi.org/10.3390/healthcare9050544
Kammoun A, Hachicha W, Aljuaid AM. Integrating Quality Tools and Methods to Analyze and Improve a Hospital Sterilization Process. Healthcare. 2021; 9(5):544. https://doi.org/10.3390/healthcare9050544
Chicago/Turabian StyleKammoun, Amira, Wafik Hachicha, and Awad M. Aljuaid. 2021. "Integrating Quality Tools and Methods to Analyze and Improve a Hospital Sterilization Process" Healthcare 9, no. 5: 544. https://doi.org/10.3390/healthcare9050544