
Knowledge of Antiretroviral Treatment and Associated Factors in HIV-Infected Patients

 ,
,  ,
, 
Abstract
:1. Introduction
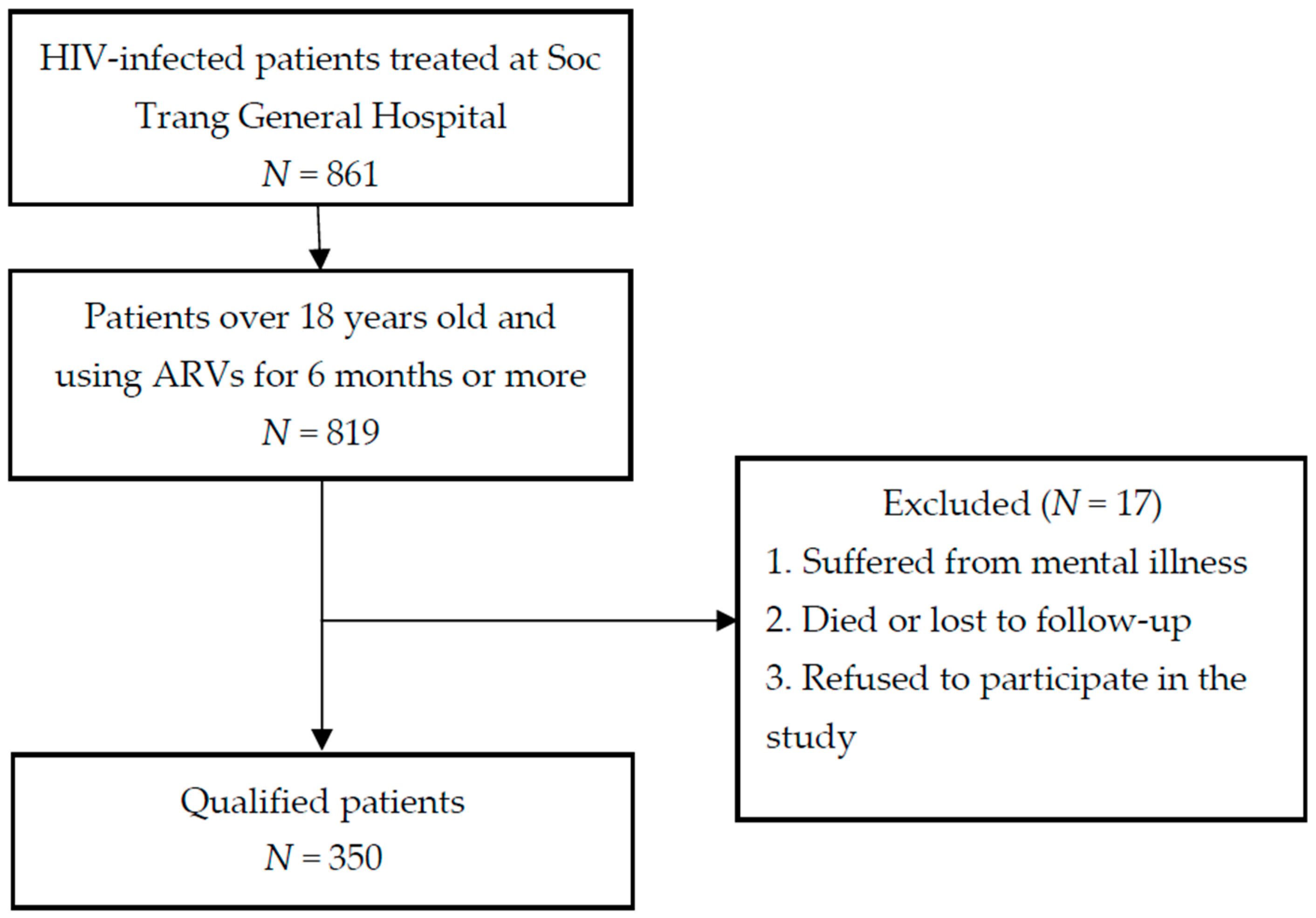
2. Materials and Methods
3. Results
3.1. Demographic Characteristics
3.2. Knowledge of ARV Treatment
3.3. Factors Associated with Knowledge of ARV Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS. UNAIDS Data 2020; Joint United Nation Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland, 2020. [Google Scholar]
- Soc Trang Province AIDS Center. Annual Report of the HIV/AIDS Prevention and Control Program 2020 and Plan for 2021; Soc Trang Province AIDS Center: Soc Trang, Vietnam, 2020.
- Nguyen, D.B.; Do, N.T.; Shiraishi, R.W.; Le, Y.N.; Tran, Q.H.; Nguyen, H.H.; Medland, N.A.; Nguyen, L.T.; Struminger, B.B. Outcomes of Antiretroviral Therapy in Vietnam: Results from a National Evaluation. PLoS ONE 2013, 8, e55750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boateng, D.; Kwapong, G.D.; Agyei-Baffour, P. Knowledge, perception about antiretroviral therapy (ART) and prevention of mother-to-child-transmission (PMTCT) and adherence to ART among HIV positive women in the Ashanti Region, Ghana: A cross-sectional study. BMC Women Health 2013, 13, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruud, K.W.; Srinivas, S.C.; Toverud, E.-L. Knowledge of HIV and its treatment among health care providers in South Africa. Int. J. Clin. Pharm. 2013, 36, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Olowookere, S.A.; Fatiregun, A.A.; Adewole, I.F. Knowledge and attitudes regarding HIV/AIDS and antiretroviral therapy among patients at a Nigerian treatment clinic. J. Infect. Dev. Ctries 2012, 6, 809–816. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.; Thach, A.; Pham, X.; Lam, A.; Nguyen, T.; Duong, C.; Nguyen, L.; Nguyen, T.; Pham, S.; Taxis, K.; et al. Prevalence and Determinants of Medication Adherence among Patients with HIV/AIDS in Southern Vietnam. Infect. Dis. Rep. 2021, 13, 126–135. [Google Scholar] [CrossRef]
- Dagli-Hernandez, C.; Lucchetta, R.C.; De Nadai, T.R.; Galduróz, J.C.F.; Mastroianni, P.D.C. Self-perception of knowledge and adherence reflecting the effectiveness of antiretroviral therapy. Patient Prefer. Adherence 2016, 10, 1787–1793. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, R.; Altice, F.L.; Copenhaver, M.M. HIV-Related Stigma, Motivation to Adhere to Antiretroviral Therapy, and Medication Adherence Among HIV-Positive Methadone-Maintained Patients. JAIDS J. Acquir. Immune Defic. Syndr. 2019, 80, 166–173. [Google Scholar] [CrossRef]
- Altice, F.; Evuarherhe, O.; Shina, S.; Carter, G.; Beaubrun, A.C. Adherence to HIV treatment regimens: Systematic literature review and meta-analysis. Patient Prefer. Adherence 2019, 13, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Azar, P.; Wood, E.; Nguyen, P.; Luma, M.; Montaner, J.; Kerr, T.; Milloy, M.-J. Drug use patterns associated with risk of non-adherence to antiretroviral therapy among HIV-positive illicit drug users in a Canadian setting: A longitudinal analysis. BMC Infect. Dis. 2015, 15, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Soc Trang Province AIDS Center. Annual Report of the HIV/AIDS Prevention and Control Program 2018 and Plan for 2019; Soc Trang Province AIDS Center: Soc Trang, Vietnam, 2019.
- Fillenbaum, G.G.; Hughes, D.C.; Heyman, A.; George, L.K.; Blazer, D.G. Relationship of health and demographic characteristics to Mini-Mental State Examination score among community residents. Psychol. Med. 1988, 18, 719–726. [Google Scholar] [CrossRef]
- Tran, N.D. Study the Adherence of Antiretroviral Therapy and Other Relevant Factors in HIV/AIDS Patients at Can Tho Preventive Health Center, Ninh Kieu District, Can Tho City in 2014. Bachelor’s Thesis, Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam, 2015. [Google Scholar]
- Ngo, V.T.; Tran, T.D.; Nguyen, T.D. Knowledge and practices on adherence to antiretroviral therapy at Nguyen Dinh Chieu Hospital in Ben Tre Province, Vietnam in 2011. J. Pract. Med. 2012, 814, 45–48. [Google Scholar]
- Kipp, W.E.; Alibhai, A.; Saunders, D.; Konde-Lule, J.; Ruhunda, A. Public knowledge and attitudes toward HIV/AIDS and antiretroviral therapy in Kabarole district, western Uganda. AIDS Care 2009, 21, 118–124. [Google Scholar] [CrossRef]
- Molassiotis, A.; Nahas-Lopez, V.; Chung, W.Y.R.; Lam, S.W.C.; Li, C.K.P.; Lau, T.F.J. Factors associated with adherence to antiretroviral medication in HIV-infected patients. Int. J. STD AIDS 2002, 13, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Nachega, J.B.; Lehman, D.A.; Hlatshwayo, D.; Mothopeng, R.; Chaisson, R.E.; Karstaedt, A.S. HIV/AIDS and Antiretroviral Treatment Knowledge, Attitudes, Beliefs, and Practices in HIV-Infected Adults in Soweto, South Africa. JAIDS J. Acquir. Immune Defic. Syndr. 2005, 38, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.G.; Liu, H.; Hays, R.D.; Golin, C.E.; Ye, Z.; Beck, C.K.; Kaplan, A.H.; Wenger, N.S. Knowledge of Antiretroviral Regimen Dosing and Adherence: A Longitudinal Study. Clin. Infect. Dis. 2003, 36, 514–518. [Google Scholar] [CrossRef]
- Potchoo, Y.; Tchamdja, K.; Balogou, A.; Pitche, V.P.; Guissou, I.P.; Kassang, E.K. Knowledge and adherence to antiretroviral therapy among adult people living with HIV/AIDS treated in the health care centers of the association “Espoir Vie Togo” in Togo, West Africa. BMC Clin. Pharmacol. 2010, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Almeida, R.F.D.C.; Vieira, A.P.G.F. Evaluation of HIV/AIDS patients’ knowledge on antiretroviral drugs. Braz. J. Infect. Dis. 2009, 13, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Dowse, R.; Barford, K.; Browne, S. Simple, illustrated medicines information improves ARV knowledge and patient self-efficacy in limited literacy South African HIV patients. AIDS Care 2014, 26, 1400–1406. [Google Scholar] [CrossRef] [Green Version]
- Kasumu, L.O.; Balogun, M.R. Knowledge and attitude towards antiretroviral therapy and adherence pattern of HIV patients in southwest Nigeria. Int. J. Infect. Control 2014, 10, 1–8. [Google Scholar]
- Sangeda, R.Z.; Mosha, F.; Aboud, S.; Kamuhabwa, A.; Chalamilla, G.; Vercauteren, J.; Wijngaerden, E.V.; Lyamuya, E.F.; Vandamme, A.-M. Predictors of non-adherence to antiretroviral therapy at an urban HIV care and treatment center in Tarzania. Drug. Healthc. Patient Saf. 2018, 10, 79–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byabene, A.K.; Fortes-Déguénonvo, L.; Niang, K.; Manga, M.N.; Bulabula, A.N.H.; Nachega, J.B.; Seydi, M. Optimal Antiretroviral Therapy Adherence as Evaluated by CASE Index Score Tool is Associated with Virological Suppression in HIV-Infected Adults in Dakar, Senegal. Trop. Med. Int. Health 2017, 22, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Kranzer, K.; Ford, N. Unstructured treatment interruption of antiretroviral therapy in clinical practice: A systematic review. Trop. Med. Int. Health 2011, 16, 1297–1313. [Google Scholar] [CrossRef] [PubMed]
- Moucheraud, C.; Stern, A.F.; Ahearn, C.; Ismail, A.; Nsubuga-Nyombi, T.; Ngonyani, M.M.; Mvungi, J.; Ssensamba, J. Barriers to HIV Treatment Adherence: A Qualitative Study of Discrepancies Between Perceptions of Patients and Health Providers in Tanzania and Uganda. AIDS Patient Care STDs 2019, 33, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Zakher, B.; Blazina, I.; Chou, R. Association between knowledge of HIV-positive status or use of antiretroviral therapy and high-risk transmission behaviors: Systematic review. AIDS Care 2013, 26, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Lolekha, R.; Boon-Yasidhi, V.; Leowsrisook, P.; Naiwatanakul, T.; Durier, Y.; Nuchanard, W.; Tarugsa, J.; Punpanich, W.; Pattanasin, S.; Chokephaibulkit, K. Knowledge, attitudes, and practices regarding antiretroviral management, reproductive health, sexually transmitted infections, and sexual risk behavior among perinatally HIV-infected youth in Thailand. AIDS Care 2015, 27, 618–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoang, D.; Dinh, A.T.; Groce, N.; Sullivan, L.E. Knowledge and Perceptions of HIV-Infected Patients Regarding HIV Transmission and Treatment in Ho Chi Minh City, Vietnam. Asia Pac. J. Public Health 2015, 27, NP746–NP757. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n (%) | General Knowledge of ARV Treatment (≥8 of 9 Answers) | Unadjusted | ||
|---|---|---|---|---|---|
| Yes n (%) | No n (%) | OR (95% CI) | p-Value * | ||
| Age group | |||||
| <35 years | 162 (46.3) | 106 (65.4) | 56 (34.6) | 1.31 | 0.219 |
| ≥35 years | 188 (53.7) | 111 (59.0) | 77 (41.0) | (0.85–2.03) | |
| Gender | |||||
| Male | 220 (62.9) | 139 (63.2) | 81 (36.8) | 1.14 | 0.553 |
| Female | 130 (37.1) | 78 (60.0) | 52 (40.0) | (0.73–1.79) | |
| Distance to clinic offering ARVs | |||||
| <20 km | 108 (30.9) | 70 (64.8) | 38 (35.2) | 1.19 | 0.469 |
| ≥20 km | 242 (69.1) | 147 (60.7) | 95 (39.3) | (0.74–1.91) | |
| Education level | |||||
| Secondary school or more | 206 (58.9) | 151 (73.3) | 55 (26.7) | 3.25 | <0.001 |
| Less than secondary school | 144 (41.1) | 66 (45.8) | 78 (54.2) | (2.07–5.09) | |
| Occupational status | |||||
| Currently employed | 285 (81.4) | 183 (64.2) | 102 (35.8) | 1.64 | 0.074 |
| Unemployed | 65 (18.6) | 34 (52.3) | 31 (47.7) | (0.95–2.82) | |
| Working away from home | |||||
| Yes | 135 (38.6) | 96 (71.1) | 39 (28.9) | 1.91 | 0.005 |
| No | 215 (61.4) | 121 (56.3) | 94 (43.7) | (1.21–3.03) | |
| HIV transmission routes | |||||
| Injecting drugs or mother-to-child contact | 17 (4.9) | 15 (88.2) | 2 (11.8) | 4.86 | 0.022 |
| Sexual intercourse | 333 (95.1) | 202 (60.7) | 131 (39.3) | (1.09–21.62) | |
| Opportunistic infections | |||||
| No | 340 (97.1) | 212 (62.4) | 128 (37.6) | 1.66 | 0.514 * |
| Yes | 10 (2.9) | 5 (50.0) | 5 (50.0) | (0.47–5.83) | |
| Alcohol and tobacco use | |||||
| No | 106 (30.3) | 71 (67.0) | 35 (33.0) | 1.36 | 0.206 |
| Yes | 244 (69.7) | 146 (59.8) | 98 (40.2) | (0.84–2.20) | |
| Presence of tension, anxiety, or stress | |||||
| Yes | 160 (45.7) | 115 (71.9) | 45 (28.1) | 2.21 | <0.001 |
| No | 190 (54.3) | 102 (53.7) | 88 (46.3) | (1.41–3.45) | |
| Patients’ quality of life after treatment | |||||
| Better | 239 (68.3) | 164 (68.6) | 75 (31.4) | 2.39 | <0.001 |
| Normal | 111 (31.7) | 53 (47.7) | 58 (52.3) | (1.51–3.80) | |
| Patients wishing to stop medication after symptoms improved | |||||
| No | 294 (84) | 193 (65.6) | 101 (34.4) | 2.55 | 0.001 |
| Yes | 56 (16) | 24 (42.9) | 32 (57.1) | (1.43–4.56) | |
| Reminder support to take ARVs | |||||
| Self-remind | 293 (83.7) | 193 (65.9) | 100 (34.1) | 2.65 | 0.001 |
| Spouses, parents, siblings | 57 (16.3) | 24 (42.1) | 33 (57.9) | (1.49–4.73) | |
| Self-evaluated adherence | |||||
| High adherence | 282 (80.6) | 194 (68.8) | 88 (31.2) | 4.31 | <0.001 |
| Medium and low adherence | 68 (19.4) | 23 (33.8) | 45 (66.2) | (2.46–7.57) | |
| Question | Frequency (n = 350) | Percentage (%) |
|---|---|---|
| 1. What are antiretroviral drugs? | ||
| Antivirals (correct) | 320 | 91.4 |
| Antibiotics/do not know | 30 | 8.6 |
| 2. How many types of drugs are in the ARV combinations? | ||
| Triple ARVs or more (correct) | 251 | 71.7 |
| Do not know | 99 | 28.3 |
| 3. How long does treatment last? | ||
| Lifelong (correct) | 341 | 97.4 |
| Other duration/do not know | 9 | 2.6 |
| 4. How does one take ARVs correctly? | ||
| Once daily (q.24.h) or twice daily (q.12.h) (correct) | 343 | 98.0 |
| Do not know | 7 | 2.0 |
| 5. What are the side-effects of taking ARVs? | ||
| Rash, headache/dizziness, nausea/vomiting, diarrhea, stomachache, anemia, hepato-renal toxicity, etc. (correct) | 334 | 95.4 |
| Do not know | 16 | 4.6 |
| 6. How to manage the side-effects of taking ARVs? | ||
| Consult with physicians (correct) | 320 | 91.4 |
| Self-manage/do not know | 30 | 8.6 |
| 7. How to manage after missing medication? | ||
| Take it as soon as you remember (correct) | 311 | 88.9 |
| Skip the missed dose/do not know | 39 | 11.1 |
| 8. How to calculate the next doses? | ||
| Take the next dose 4 h after taking the missed dose (for the twice-daily regimen) or 12 h (for the once-daily regimen) (correct) | 328 | 93.7 |
| Do not know | 22 | 6.3 |
| 9. What is treatment adherence? | ||
| Take the right medicine, right dose, at the right time, in the right way, and re-examine on time (correct) | 338 | 96.6 |
| Do not know | 12 | 3.4 |
| General knowledge of ARV treatment (≥ 8 of 9 scores) | 217 | 62.0 |
| Mean score (SD): 8.2 (1.4) | ||
| Covariate | Adjusted | |
|---|---|---|
| OR (95% CI) | p-Value | |
| Education level | ||
| Secondary school or more | 2.54 (1.56–4.13) | <0.001 |
| Less than secondary school | ||
| Working away from home | ||
| Yes | 1.91 (1.14–3.18) | 0.013 |
| No | ||
| HIV transmission routes | ||
| Injecting drugs or mother-to-child contact | 6.65 (1.29–34.07) | 0.023 |
| Sexual intercourse | ||
| Patients with tension, anxiety, or stress | ||
| Yes | 2.04 (1.24–3.34) | 0.005 |
| No | ||
| Reminder support to take ARVs | ||
| Self-remind | 2.12 (1.1–4.06) | 0.024 |
| Spouses, parents, siblings | ||
| Self-evaluated adherence | ||
| High adherence | 4.06 (2.17–7.57) | <0.001 |
| Medium and low adherence | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Nguyen, L.; Nguyen, T.N.P.; Thach, A.N.; Lam, A.N.; Lam, D.Q.; Duong, C.X.; Pham, S.T.; Nguyen, T.H.; Perwitasari, D.A.; Taxis, K.; et al. Knowledge of Antiretroviral Treatment and Associated Factors in HIV-Infected Patients. Healthcare 2021, 9, 483. https://doi.org/10.3390/healthcare9040483
Van Nguyen L, Nguyen TNP, Thach AN, Lam AN, Lam DQ, Duong CX, Pham ST, Nguyen TH, Perwitasari DA, Taxis K, et al. Knowledge of Antiretroviral Treatment and Associated Factors in HIV-Infected Patients. Healthcare. 2021; 9(4):483. https://doi.org/10.3390/healthcare9040483
Chicago/Turabian StyleVan Nguyen, Lam, Thao N. P. Nguyen, Anh N. Thach, Anh N. Lam, Duc Q. Lam, Chu X. Duong, Suol T. Pham, Thao H. Nguyen, Dyah A. Perwitasari, Katja Taxis, and et al. 2021. "Knowledge of Antiretroviral Treatment and Associated Factors in HIV-Infected Patients" Healthcare 9, no. 4: 483. https://doi.org/10.3390/healthcare9040483