
Indices of Cardiovascular Health, Body Composition and Aerobic Endurance in Young Women; Differential Effects of Two Endurance-Based Training Modalities


 ,
, 
Abstract
:1. Introduction
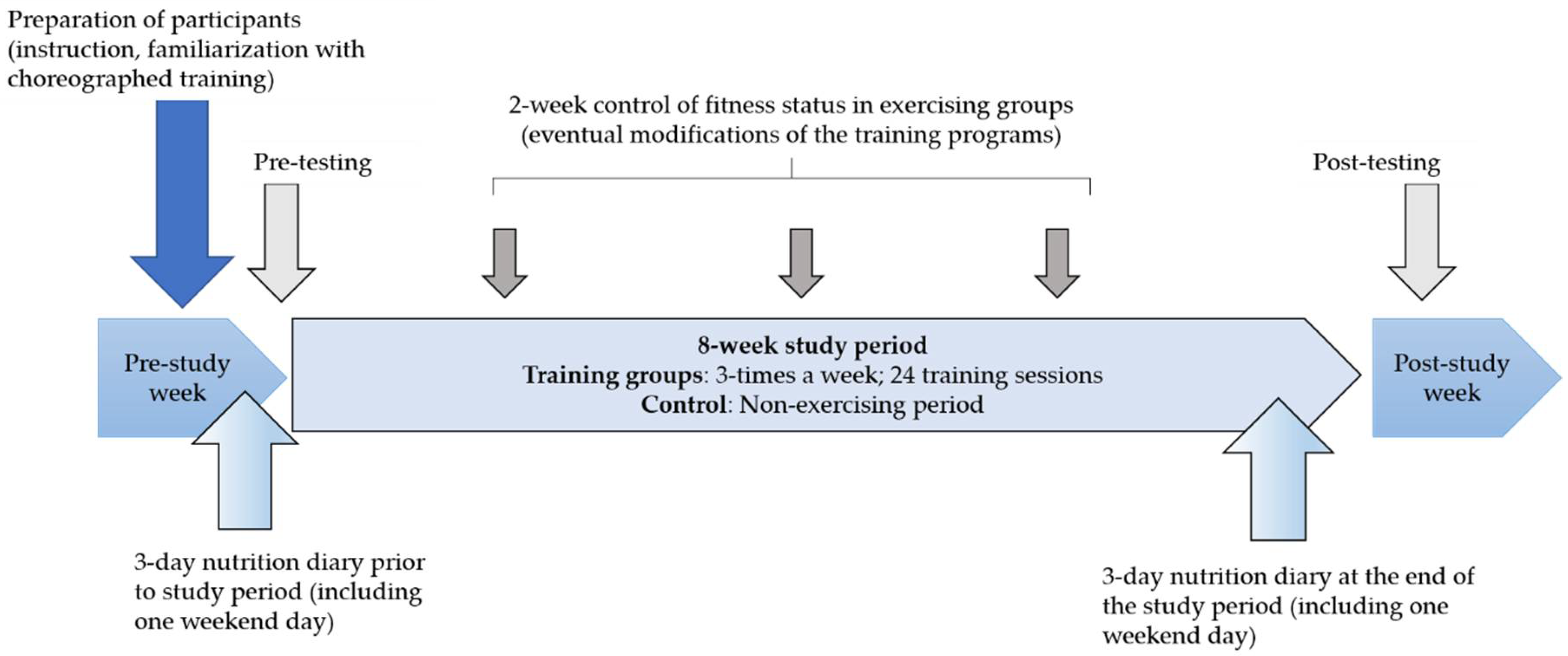
2. Materials and Methods
2.1. Participants
2.2. Testing and Variables
2.3. Physical Exercise Programs
2.4. Statistics
3. Results
4. Discussion
4.1. Endurance Exercise, Lipid Panel, and Plasma Glucose Levels
4.2. Endurance Exercise, Anthropometric/Body-Built Indices and Endurance Capacity
4.3. Differential Effects of Two Types of Endurance Exercise
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lim, H.S.; Yoo, J.J. Association between Health Indicators and Health-Related Quality of Life according to Physical Activity of Older Women. Healthcare 2020, 8, 507. [Google Scholar] [CrossRef] [PubMed]
- Maric, D.; Kvesic, I.; Lujan, I.K.; Bianco, A.; Zenic, N.; Separovic, V.; Terzic, A.; Versic, S.; Sekulic, D. Parental and Familial Factors Influencing Physical Activity Levels in Early Adolescence: A Prospective Study. Healthcare 2020, 8, 532. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E. Updating the evidence that physical activity is good for health: An epidemiological review 2000–2003. J. Sci. Med. Sport 2004, 7, 6–19. [Google Scholar] [CrossRef]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.P.; Church, T.S. The role of exercise and physical activity in weight loss and maintenance. Prog. Cardiovasc. Dis. 2014, 56, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Wieser, H.; Vittadello, F.; Comploj, E.; Stummer, H. Do Health Professionals Sufficiently Address Patients’ Disposition Toward Changing Their Nutritional and Physical Activity Habits? Findings from a Pilot Study among People with Type 2 Diabetes in Northern Italy. Healthcare 2020, 8, 524. [Google Scholar] [CrossRef]
- Sekulic, D.; Maric, D.; Versic, S.; Zevrnja, A.; Terzic, A.; Zenic, N. Familial and Parental Predictors of Physical Activity in Late Adolescence: Prospective Analysis over a Two-Year Period. Healthcare 2021, 9, 132. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Beedie, C.; Jimenez, A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: Review, synthesis and recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mo-suwan, L.; Ekpalakorn, V.; Ruengdarakanon, N. The 4th report on National Health Examination Survey (child health) V. Ekpalakorn Ed. 2008, 2009. [Google Scholar]
- Delgado-Floody, P.; Latorre-Roman, P.; Jerez-Mayorga, D.; Caamano-Navarrete, F.; Garcia-Pinillos, F. Feasibility of incorporating high-intensity interval training into physical education programs to improve body composition and cardiorespiratory capacity of overweight and obese children: A systematic review. J. Exerc. Sci. Fit. 2019, 17, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J.; Grgic, J.; Ogborn, D.; Krieger, J.W. Strength and Hypertrophy Adaptations Between Low- vs. High-Load Resistance Training: A Systematic Review and Meta-analysis. J. Strength Cond. Res. 2017, 31, 3508–3523. [Google Scholar] [CrossRef]
- Stangier, C.; Abel, T.; Mierau, J.; Hollmann, W.; Struder, H.K. Effects of Cycling Versus Running Training on Sprint and Endurance Capacity in Inline Speed Skating. J. Sports Sci. Med. 2016, 15, 41–49. [Google Scholar] [PubMed]
- Myers, J. Exercise and cardiovascular health. Circulation 2003, 107, e2–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khamis, R.Y.; Ammari, T.; Mikhail, G.W. Gender differences in coronary heart disease. Heart 2016, 102, 1142–1149. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.J.; Hong, H.C.; Choi, H.Y.; Yoo, H.J.; Cho, G.J.; Hwang, T.G.; Baik, S.H.; Choi, D.S.; Kim, S.M.; Choi, K.M. Effects of a three-month combined exercise programme on fibroblast growth factor 21 and fetuin-A levels and arterial stiffness in obese women. Clin. Endocrinol. 2011, 75, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Beqa Ahmeti, G.; Idrizovic, K.; Elezi, A.; Zenic, N.; Ostojic, L. Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women. Int. J. Environ. Res. Public Health 2020, 17, 1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhees, L.; Geladas, N.; Hansen, D.; Kouidi, E.; Niebauer, J.; Reiner, Z.; Cornelissen, V.; Adamopoulos, S.; Prescott, E.; Borjesson, M.; et al. Importance of characteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular risk factors: Recommendations from the EACPR. Part II. Eur. J. Prev. Cardiol. 2012, 19, 1005–1033. [Google Scholar] [CrossRef]
- Gotto, A.M., Jr.; Moon, J.E. Management of cardiovascular risk: The importance of meeting lipid targets. Am. J. Cardiol. 2012, 110, 3A–14A. [Google Scholar] [CrossRef] [PubMed]
- Alnasir, F.A.; Masuadi, E.M. The effect of loss of body weight on lipid profile in overweight individuals. Saudi. Med. J. 2006, 27, 687–692. [Google Scholar] [PubMed]
- Hwang, W.J.; Kim, J.A. Developing a Health-Promotion Program Based on the Action Research Paradigm to Reduce Cardiovascular Disease Risk Factors among Blue Collar Workers. Int. J. Environ. Res. Public Health 2019, 16, 4958. [Google Scholar] [CrossRef] [Green Version]
- Ratajczak, M.; Skrypnik, D.; Bogdanski, P.; Madry, E.; Walkowiak, J.; Szulinska, M.; Maciaszek, J.; Kregielska-Narozna, M.; Karolkiewicz, J. Effects of Endurance and Endurance-Strength Training on Endothelial Function in Women with Obesity: A Randomized Trial. Int. J. Environ. Res. Public Health 2019, 16, 4291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barranco-Ruiz, Y.; Ramirez-Velez, R.; Martinez-Amat, A.; Villa-Gonzalez, E. Effect of Two Choreographed Fitness Group-Workouts on the Body Composition, Cardiovascular and Metabolic Health of Sedentary Female Workers. Int. J. Environ. Res. Public Health 2019, 16, 4986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cebula, A.; Tyka, A.K.; Tyka, A.; Palka, T.; Pilch, W.; Luty, L.; Mucha, D. Physiological response and cardiorespiratory adaptation after a 6-week Nordic Walking training targeted at lipid oxidation in a group of post-menopausal women. PloS ONE 2020, 15, e0230917. [Google Scholar] [CrossRef] [Green Version]
- Chovanec, L.; Gropel, P. Effects of 8-week endurance and resistance training programmes on cardiovascular stress responses, life stress and coping. J. Sports Sci. 2020, 38, 1699–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.H.; Jeong, M.K.; Park, H.; Park, S.K. Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension. Int. J. Environ. Res. Public Health 2021, 18, 2935. [Google Scholar] [CrossRef]
- Strachan, S.M.; Perras, M.G.; Brawley, L.R.; Spink, K.S. Exercise in challenging times: The predictive utility of identity, self-efficacy, and past exercise. Sport Exercise Perform. Psychol. 2016, 5, 247. [Google Scholar] [CrossRef]
- Condello, G.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Simon, C.; Ciarapica, D.; Coppinger, T.; et al. Behavioral determinants of physical activity across the life course: A "DEterminants of DIet and Physical ACtivity" (DEDIPAC) umbrella systematic literature review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- Cortis, C.; Puggina, A.; Pesce, C.; Aleksovska, K.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Simon, C.; Ciarapica, D.; et al. Psychological determinants of physical activity across the life course: A "DEterminants of DIet and Physical ACtivity" (DEDIPAC) umbrella systematic literature review. PloS ONE 2017, 12, e0182709. [Google Scholar] [CrossRef]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef] [Green Version]
- Jackson, A.S.; Pollock, M.L. Generalized equations for predicting body density of men. Br. J. Nutr. 1978, 40, 497–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; de Ridder, H. International Society for the Advancement of Kinantropometry. Int. Stand. Anthr. Assessment. Aust. Low. Hutt New Zeal. Int. Soc. Adv. Kinanthropometry 2001, 1, 57–72. [Google Scholar]
- Warnick, G.R.; Knopp, R.H.; Fitzpatrick, V.; Branson, L. Estimating low-density lipoprotein cholesterol by the Friedewald equation is adequate for classifying patients on the basis of nationally recommended cutpoints. Clin. Chem. 1990, 36, 15–19. [Google Scholar] [CrossRef] [PubMed]
- McSwegin, P.J.; Plowman, S.A.; Wolff, G.M.; Guttenberg, G.L. The validity of a one-mile walk test for high school age individuals. Meas. Phys. Educ. Exerc. Sci. 1998, 2, 47–63. [Google Scholar] [CrossRef]
- Sekulić, D.; Rausavljević, N.; Zenić, N. Changes in motor and morphological measures of young women induced by the HI-LO and Step aerobic dance programs. Kinesiology 2003, 35, 48–58. [Google Scholar]
- Jeukendrup, A.; Hesselink, M.; Kuipers, H.; Keizer, H. The Conconi test. Inter. J. Sports Med. 1997, 18, 393–394. [Google Scholar] [CrossRef]
- Murray, C.J.; Lauer, J.A.; Hutubessy, R.C.; Niessen, L.; Tomijima, N.; Rodgers, A.; Lawes, C.M.; Evans, D.B. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: A global and regional analysis on reduction of cardiovascular-disease risk. Lancet 2003, 361, 717–725. [Google Scholar] [CrossRef]
- Duarte-Clíments, G.; Mauricio, T.F.; Gómez-Salgado, J.; Moreira, R.P.; Romero-Martín, M.; Sánchez-Gómez, M.B. Assessment of Cardiovascular Risk Factors in Young Adults through the Nursing Diagnosis: A Cross-Sectional Study among International University Students. Healthcare 2021, 9, 91. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Vander Hoorn, S.; Murray, C.J.; Group, C.R.A.C. Selected major risk factors and global and regional burden of disease. The Lancet 2002, 360, 1347–1360. [Google Scholar] [CrossRef]
- Ma, H.; Shieh, K.-J. Cholesterol and human health. J. Am. Sci. 2006, 2, 46–50. [Google Scholar]
- Leaf, D.A. The effect of physical exercise on reverse cholesterol transport. Metabolism 2003, 52, 950–957. [Google Scholar] [CrossRef]
- Dunn, A.L.; Marcus, B.H.; Kampert, J.B.; Garcia, M.E.; Kohl, H.W., III; Blair, S.N. Reduction in cardiovascular disease risk factors: 6-month results from ProjectActive. Prev. Med. 1997, 26, 883–892. [Google Scholar] [CrossRef] [PubMed]
- LeMura, L.M.; von Duvillard, S.P.; Andreacci, J.; Klebez, J.M.; Chelland, S.A.; Russo, J. Lipid and lipoprotein profiles, cardiovascular fitness, body composition, and diet during and after resistance, aerobic and combination training in young women. Eur. J. Appl. Physiol. 2000, 82, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Kostrzewa-Nowak, D.; Nowak, R.; Jastrzębski, Z.; Zarębska, A.; Bichowska, M.; Drobnik-Kozakiewicz, I.; Radzimińsk, Ł.; Leońska-Duniec, A.; Ficek, K.; Cięszczyk, P. Effect of 12-week-long aerobic training programme on body composition, aerobic capacity, complete blood count and blood lipid profile among young women. Biochem. Med. 2015, 25, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Kondric, M.; Sekulic, D.; Uljevic, O.; Gabrilo, G.; Zvan, M. Sport nutrition and doping in tennis: An analysis of athletes’ attitudes and knowledge. J. Sports Sci. Med. 2013, 12, 290–297. [Google Scholar]
- Conn, V.S.; Koopman, R.J.; Ruppar, T.M.; Phillips, L.J.; Mehr, D.R.; Hafdahl, A.R. Insulin sensitivity following exercise interventions: Systematic review and meta-analysis of outcomes among healthy adults. J. Prim. Care Community Health 2014, 5, 211–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coggan, A.R. Plasma glucose metabolism during exercise in humans. Sports Med. 1991, 11, 102–124. [Google Scholar] [CrossRef] [PubMed]
- Holloszy, J.O.; Kohrt, W.M.; Hansen, P.A. The regulation of carbohydrate and fat metabolism during and after exercise. Front. Biosci. 1998, 3, D1011–D1027. [Google Scholar] [CrossRef] [PubMed]
- Röhling, M.; Herder, C.; Stemper, T.; Müssig, K. Influence of acute and chronic exercise on glucose uptake. J. Diabetes Res. 2016, 2016, 2868652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derouich, M.; Boutayeb, A. The effect of physical exercise on the dynamics of glucose and insulin. J. Biomech. 2002, 35, 911–917. [Google Scholar] [CrossRef]
- Kondo, T.; Kobayashi, I.; Murakami, M. Effect of exercise on circulating adipokine levels in obese young women. Endocr. J. 2006, 53, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Ostrowski, K.; Rohde, T.; Zacho, M.; Asp, S.; Pedersen, B. Evidence that interleukin-6 is produced in human skeletal muscle during prolonged running. J. Physiol. 1998, 508, 949–953. [Google Scholar] [CrossRef]
- Lim, S.; Choi, S.H.; Jeong, I.-K.; Kim, J.H.; Moon, M.K.; Park, K.S.; Lee, H.K.; Kim, Y.-B.; Jang, H.C. Insulin-sensitizing effects of exercise on adiponectin and retinol-binding protein-4 concentrations in young and middle-aged women. J. Clin. Endocrinol. Metabol. 2008, 93, 2263–2268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ürimäe, J.; Hofmann, P.; Jürimäe, T.; Mäestu, J.; Purge, P.; Wonisch, M.; Pokan, R.; Von Duvillard, S. Plasma adiponectin response to sculling exercise at individual anaerobic threshold in college level male rowers. Int. J. Sports Med. 2006, 27, 272–277. [Google Scholar]
- Williams, C.B.; Zelt, J.G.; Castellani, L.N.; Little, J.P.; Jung, M.E.; Wright, D.C.; Tschakovsky, M.E.; Gurd, B.J. Changes in mechanisms proposed to mediate fat loss following an acute bout of high-intensity interval and endurance exercise. Appl. Physiol. Nutr. Metab. 2013, 38, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Poehlman, E.T.; Dvorak, R.V.; DeNino, W.F.; Brochu, M.; Ades, P.A. Effects of resistance training and endurance training on insulin sensitivity in nonobese, young women: A controlled randomized trial. J. Clin. Endocrinol. Metab. 2000, 85, 2463–2468. [Google Scholar] [CrossRef] [PubMed]
- Sillanpää, E.; Laaksonen, D.E.; Häkkinen, A.; Karavirta, L.; Jensen, B.; Kraemer, W.J.; Nyman, K.; Häkkinen, K. Body composition, fitness, and metabolic health during strength and endurance training and their combination in middle-aged and older women. Eur. J. Appl. Physiol. 2009, 106, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Ingjer, F. Effects of endurance training on muscle fibre ATP-ase activity, capillary supply and mitochondrial content in man. J. Physiol. 1979, 294, 419–432. [Google Scholar] [CrossRef] [PubMed]
- Midgley, A.W.; McNaughton, L.R.; Wilkinson, M. Is there an optimal training intensity for enhancing the maximal oxygen uptake of distance runners? Sports Med. 2006, 36, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.B.; Araújo, C.G.S. Effects of aerobic training on heart rate. Rev. Bras. Med. Esporte 2003, 9, 113–120. [Google Scholar] [CrossRef]
- Wakayoshi, K.; Yoshida, T.; Ikuta, Y.; Mutoh, Y.; Miyashita, M. Adaptations to six months of aerobic swim training. Int. J Sports Med. 1993, 14, 368–372. [Google Scholar] [CrossRef]
- Saltin, B.; Rowell, L.B. Functional adaptations to physical activity and inactivity. Fed. Proc. 1980, 39, 1506–1513. [Google Scholar]
- Gronwald, T.; Torpel, A.; Herold, F.; Budde, H. Perspective of Dose and Response for Individualized Physical Exercise and Training Prescription. J. Funct. Morphol. Kinesiol. 2020, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.; Bassey, E. Postexercise heart rates and pulse palpation as a means of determining exercising intensity in an aerobic dance class. Br. J.Sports Med. 1996, 30, 48–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, C.; Anholm, J.D.; Bok, D.; Boullosa, D.; Condello, G.; Cortis, C.; Fusco, A.; Jaime, S.J.; de Koning, J.J.; Lucia, A.; et al. Generalized Approach to Translating Exercise Tests and Prescribing Exercise. J. Funct. Morphol. Kinesiol. 2020, 5, 63. [Google Scholar] [CrossRef] [PubMed]
- Hausken, K.; Dyrstad, S.M. Heart Rate, Accelerometer Measurements, Experience and Rating of Perceived Exertion in Zumba, Interval Running, Spinning, and Pyramid Running. J. Exerc. Physiol. Online 2013, 16. [Google Scholar]
- Doma, K.; Deakin, G.B. The effects of strength training and endurance training order on running economy and performance. Appl. Physiol. Nutr. Metab. 2013, 38, 651–656. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Measurement | Group | Interaction | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F Test | p | η2 | F Test | p | η2 | F test | p | η2 | |
| BM | 426.1 | 0.001 | 0.88 | 0.26 | 0’.77 | 0.01 | 85.1 | 0.001 | 0.75 |
| BMI | 178.04 | 0.001 | 0.76 | 0.74 | 0.48 | 0.03 | 68.29 | 0.001 | 0.71 |
| BF | 112.1 | 0.001 | 0.66 | 2.43 | 0.09 | 0.08 | 28.93 | 0.001 | 0.5 |
| END | 534.52 | 0.001 | 0.9 | 5.41 | 0.01 | 0.16 | 128.39 | 0.001 | 0.81 |
| PG | 47.49 | 0.001 | 0.45 | 47.49 | 0.001 | 0.45 | 7.48 | 0.01 | 0.2 |
| TC | 137.05 | 0.001 | 0.7 | 1.45 | 0.23 | 0.04 | 25.5 | 0.001 | 0.47 |
| HDL | 151.39 | 0.001 | 0.73 | 3.36 | 0.03 | 0.12 | 41.09 | 0.001 | 0.59 |
| LDL | 205.59 | 0.001 | 0.78 | 2.63 | 0.08 | 0.08 | 31.11 | 0.001 | 0.52 |
| TG | 700.96 | 0.001 | 0.92 | 7.97 | 0.001 | 0.22 | 67.57 | 0.001 | 0.7 |
| C (n = 19) | CAT (n = 19) | TEE (n = 20) | ||||
|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | Pre-Test | Post-Test | |
| BM (kg) | 65.38 ± 8.32 | 64.79 ± 9.1 * | 67.88 ± 5.86 | 59.91 ± 5.87 * | 67.35 ± 8.39 | 59.38 ± 8.56 * |
| BMI (kg/m2) | 23.77 ± 2.71 | 24.2 ± 2.49 | 24.45 ± 2.49 | 21.58 ± 2.32 * | 25.11 ± 2.69 | 22.09 ± 2.79 * |
| BF (%) | 33.94 ± 6.06 | 34.02 ± 6.22 | 34.77 ± 5.79 | 26.15 ± 5.41 * | 36.43 ± 5.43 | 27.14 ± 4.04 * |
| END (mL/O2) | 27.08 ± 2.26 | 28.17 ± 2.29 * | 17.49 ± 1.53 | 29.76 ± 1.57 * | 26.31 ± 1.58 | 32.62 ± 1.68 *, C, CAT |
| PG (mmol/L) | 5.04 ± 0.55 | 4.94 ± 0.36 | 4.94 ± 0.48 | 4.52 ± 0.41 * | 4.89 ± 0.54 | 4.25 ± 0.6 *, C, CAT |
| TC (mmol/L) | 4.67 ± 0.57 | 4.52 ± 0.54 | 4.75 ± 0.47 | 4.03 ± 0.53 * | 4.94 ± 0.56 | 3.77 ± 0.47 *, C, CAT |
| HDL (mmol/L) | 1.6 ± 0.23 | 1.6 ± 0.26 | 1.63 ± 0.15 | 1.23 ± 0.16 * | 1.74 ± 0.27 | 1.25 ± 0.18 *, C, CAT |
| LDL (mmol/L) | 3.18 ± 0.6 | 2.99 ± 0.49 | 3.25 ± 0.47 | 2.44 ± 0.41 *, C | 3.36 ± 0.43 | 2.21 ± 0.46 *, C, CAT |
| TG (mmol/L) | 1.2 ± 0.22 | 1.02 ± 0.22 * | 1.2 ± 0.17 | 0.57 ± 0.12 *, C | 1.18 ± 0.23 | 0.72 ± 0.16 *, C, CAT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Idrizovic, K.; Ahmeti, G.B.; Sekulic, D.; Zevrnja, A.; Ostojic, L.; Versic, S.; Zenic, N. Indices of Cardiovascular Health, Body Composition and Aerobic Endurance in Young Women; Differential Effects of Two Endurance-Based Training Modalities. Healthcare 2021, 9, 449. https://doi.org/10.3390/healthcare9040449
Idrizovic K, Ahmeti GB, Sekulic D, Zevrnja A, Ostojic L, Versic S, Zenic N. Indices of Cardiovascular Health, Body Composition and Aerobic Endurance in Young Women; Differential Effects of Two Endurance-Based Training Modalities. Healthcare. 2021; 9(4):449. https://doi.org/10.3390/healthcare9040449
Chicago/Turabian StyleIdrizovic, Kemal, Gentiana Beqa Ahmeti, Damir Sekulic, Ante Zevrnja, Ljerka Ostojic, Sime Versic, and Natasa Zenic. 2021. "Indices of Cardiovascular Health, Body Composition and Aerobic Endurance in Young Women; Differential Effects of Two Endurance-Based Training Modalities" Healthcare 9, no. 4: 449. https://doi.org/10.3390/healthcare9040449